Assessing and Treating Cognitive Impairments in Schizophrenia: Current and Future
Chun-Yuan Lina,b,c Guochuan E. Tsaid and Hsien-Yuan Lanea, e
a Institute of Clinical Medical Science, Medical College, China Medical University, Taichung, Taiwan
b Department of Psychiatry, Changhua Hospital, Changhua, Taiwan c National Changhua University of Education, Changhua, Taiwan
d Department of Psychiatry, Harbor-UCLA Medical Center
e Department of Psychiatry, China Medical University Hospital, Taichung, Taiwan
** Correspondence:
Hsien-Yuan Lane, MD, PhD
Institute of Clinical Medical Science, Medical College, China Medical University, Taichung, Taiwan
No.91 Hsueh-Shih Road, Taichung 404, Taiwan E-mail: [email protected]
Tel: +886-4-22053366 # 7620
Guochuan E. Tsai and Hsien-Yuan Lane contributed equally as corresponding authors.
Abstract
Schizophrenia is a serious neuropsychiatric disease characterized by positive symptoms, negative symptoms and cognitive impairments. Evidences have showed that cognitive impairments sustain in every clinical stage, relate with the liability, may predict functional outcome in schizophrenia and could be the core symptom of
schizophrenia. The treatment of cognitive impairments in schizophrenia could
alleviate the burden of the illness and has become the subject of intensive research.In this review, we synthesize current advances of assessing strategies, pharmacological and non-pharmacological treatments of cognitive impairments in schizophrenia. According to the registered records of ClinicalTrials.gov, the most widely studied of these are neurochemical mechanisms related with the dopamine metabolism,
glutamate metabolism , γ-aminobutyric acid (GABA) metabolism, serotonin metabolism, acetylcholine metabolism , and oxytocin. Despite preclinical data for putative pro-cognitive drugs, their clinical benefits for schizophrenia patients have been limited. The small sample sizes and the short treatment duration could be related with the suboptimal results. Evidences supported the short-term benefits of cognitive remediation therapy on cognitive domains with small to moderate effects; however, the small sample sizes and the characteristics of subjects limited the generalization of the positive results and long-term functional outcome is not clear. Combination therapy is promising, by integrating pro-cognitive agents and cognitive rehabilitation programs or combining two kinds of pro-cognitive agents via different mechanisms. Future studies should investigate the pro-cognitive drugs’ long-term efficacy, rebound deterioration in psychosis/cognition following discontinuation, and related biomarkers of functional outcome.
Introduction
Schizophrenia is one of the most serious neuropsychiatric diseases in the world, influencing 1% of the global population. The symptom complexes of disease liability in schizophrenia are positive symptoms (delusions and hallucinations), negative symptoms (anhedonia, asociality, and amotivation) and cognitive impairments
(memory, attention, and executive dysfunction). Most people with schizophrenia cope with symptoms throughout their lives and often rely on others for help. The families and society are also affected by schizophrenia, and the direct and indirect costs of schizophrenia are great. In this review, we synthesize current advances of assessing strategies, pharmacological and non-pharmacological treatments of cognitive impairments in schizophrenia. Articles were identified through a literature search in MEDLINE. The search covered the period from January 1990 to February 2012. The keywords were “schizophrenia” (in title) combined with “cognitive” (in title/abstract) and the additional filters were “journal article, full text available, humans, and
English language”. The search produced 4081 articles and 2257 were excluded after title examination. Then, the following criteria guided the inclusion of studies in the review if: (1) the sample consisted of schizophrenia patients according to a recognized criterion-based diagnostic system such as DSM or ICD; (2) for clinical trials: the study used standardized and reliable clinical scales and cognitive tasks; (3) the study was published in a peer-reviewed journal. Finally, 191 publications were enrolled for the authors to review.
Significant cognitive impairment including working memory, attention, visual memory, executive function and social cognition were observed in the subjects of prodromal psychosis. Prior to onset of psychosis, cognitive dysfunction is evident in pre-schizophrenia subjects during childhood and importantly, the cognitive
impairments are associated with the vulnerability to psychosis among the unaffected high-risk subjects . In the early course of schizophrenia, cognitive impairment is present in the drug naïve patients and even in those patients with intact intellectual function. Moreover, cognitive functioning is independently correlated with the post-onset relapses of first-episode psychoses. In the chronic stage of schizophrenia, cognition does not consequentially improve following relief from acute psychotic episode. Impaired cognitive function is associated with social and adaptive
functioning in geriatric schizophrenia patients, particularly for those with long illness duration. More so than other dimensions, cognitive impairment is thought to be the core manifestation of schizophrenia for the pervasive persistence at each course of the illness and the predictive utility for the daily functioning of patients.
The relationships between positive, negative and mood symptoms and cognitive symptoms have been equivocal in both cross-sectional and longitudinal studies . A recent meta-analytic review of 58 cross-sectional studies enrolling 5,009 individuals (94% with schizophrenia, 3% with schizoaffective disorder, and 3% with other psychotic disorders; mean age and mean illness duration ranged from 19.1 to 51.9 years and 4.8 to 28.9 years, respectively) showed that negative and disorganized dimensions were significantly but modestly associated with cognitive deficits. In contrast, positive and depressive symptom dimensions did not show any relationship with any neuropsychological domain.
related with improvements in positive symptoms but not in negative symptoms over 6 months. Improvement in positive symptoms but not negative symptoms was
associated with improvements in cognitive domains of executive function , spatial memory, concentration/speed , and global cognition in a study in 42 schizophrenia patients during their first 4-5 years of illness duration, however improved negative symptoms but not psychotic or disorganized symptoms were related with improved verbal cognition in another 5-year follow-up cohort of fifty-four first-episode and recent-onset schizophrenia patients . For chronic schizophrenia (illness duration of 13.9-20.5 years), change in positive or negative symptoms was not related to change in cognition longitudinally . Different characteristics of patients may contribute to the conflicting results of the relationship between changes in symptoms and cognitive functioning in schizophrenia.
Collectively, negative symptoms may be associated with the levels of cognitive deficits and a poor cognitive outcome but the correlation between negative symptoms and change in cognition was reduced longitudinally. Moreover, cognitive impairment in schizophrenia is not merely side effects of medication or disease chronicity but a prominent and stable domain throughout the course of schizophrenia, even as positive symptoms fluctuate. It sustains in every clinical stage, relates with the liability, and may predict functional outcome in schizophrenia .
Assessment tests of cognitive impairments in schizophrenia
Among patients with schizophrenia, cognitive impairments have been identified in almost every measurable cognitive ability domain, from basic to higher order cognition. It has been suggested that cognitive impairments may represent the candidate endophenotypes in the search for genes conferring risk for schizophrenia . Therefore, it is important to establish a more refined description of cognitive
impairments by using neuropsychological measures.
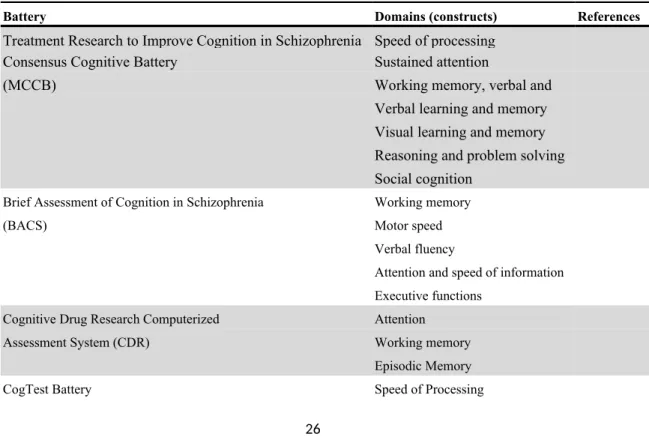
Various batteries have been introduced to assess the cognitive deficits of
schizophrenia patients (Table 1), such as Treatment Research to Improve Cognition in Schizophrenia Consensus Cognitive Battery (MCCB), the Brief Assessment of Cognition in Schizophrenia (BACS), Cognitive Drug Research computerized
assessment system (CDR), CogTest Battery, and Cambridge Neuropsychological Test Automated Battery (CANTAB). To develop efficient tool with brief administration and scoring time, portability, repeatability, and availability for the design of clinical trials of drugs for cognitive impairment in schizophrenia, Treatment Research to Improve Cognition in Schizophrenia (MATRICS) initiative facilitated the
development of MCCB. The creation of MCCB is an important step because well-defined measures have been chosen to comprise cognitive domains that best
characterized schizophrenia. MCCB includes 7 domains: (1) speed of processing (2) sustained attention (3) working memory, verbal and nonverbal (4) verbal learning and memory (5) visual learning and memory (6) reasoning and problem solving, and (7) social cognition.
The 1st to 6th domains were defined as neurocognition, the processes of linking and appraising information, while the 7th domain of social cognition, measured by Mayer–Salovey–Caruso Emotional Intelligence Test Version 2.0 (MSCEIT V2.0), was defined the mental operations underlying social interactions such as the
perception, interpretation, and generation of responses to the intentions and behaviors of others. Neurocognition and social cognition are related, but different constructs. Research on social cognition in schizophrenia has focused on 4 domains: perceiving emotions, using emotions to facilitate thought, understanding emotions, and managing emotions in self and others. Cumulative data showed that social cognition may
mediate the relationship between neurocognition and functional outcomes. MATRICS defined social cognition and neurocognition as an integral whole of cognitive function in schizophrenia and the managing emotions component was selected for its relatively stronger relationship to functional status.
The MCCB has become the standard assessment tool for assessing cognitive dysfunction in schizophrenia, however the predominant population in the studies has been older, chronic, and mainly male schizophrenia patients, further endeavors to recruit larger and diverse samples and to ensure versions with the cross-cultural adaptability for different countries are necessary.
Biomarkers reflecting on cognitive impairments
At present, the diagnosis of schizophrenia relies on descriptive behavioral and symptomatic information, and specific biomarker is lacking. Establishing biomarkers those reflect on cognitive impairment, a primary role in the pathophysiology of schizophrenia, with sensitivity, specificity and availability deserves further investigation.
Genetics modalities
Susceptibility genes may increase risk for schizophrenia through baneful effects on
cognitive processes. Several genes those regulate neural development, dystrobrevin-binding protein 1 (DTNBP1) gene, catechol-O-methyltransferase (COMT) gene ,brain derived neurotrophic factor (BDNF) gene, Disrupted in schizophrenia 1 (DISC1) gene, and D-amino acid oxidase activator gene (DAOA, G72) have garnered as potential contributors to impaired cognition in schizophrenia. The majority of these studies measured schizophrenia patients’ cognitive domains, and genotyped the patients for specific SNPs and then investigated the associations of alleles with either general or specific cognitive measures. For examples, schizophrenia patients who
carried the DTNBP1 haplotype showed significantly greater P1 of the visual evoked potential (VEP) deficit than patients who were non-carriers ; higher loading of the
COMT 158 Met allele was associated with better neurocognitive performance among
patients with chronic schizophrenia while while the Val allele is associated with impaired working memory and general cognitive decline ;the Met allele at the val66met polymorphism in the BDNF gene was associated with impaired working memory performance and visuospatial dysfunction ; and DISC1 genotype was related to rapid visual search and verbal working memory in schizophrenia. Although the studies are beset with small sample sizes, heterogeneous ethnic origin, and
unequivocal cognitive test methods so that consistent and specific effect of genotypes on cognitive impairment in schizophrenia remain variable, genetics modalities
provided promising evidence that variation in particular genes could affect neural development and function and further explained the heterogeneity of cognitive impairments in patients with schizophrenia.
Neuroimaging modalities
Neuroimaging assessments, including morphometric neuroimaging and functional neuroimaging, have played a prominent role in the quest to identify the brain systems responsible for cognitive dysfunction in schizophrenia. Whereas morphometric neuroimaging assessments such as computer tomography (CT) and magnetic resonance imaging (MRI) allow for detailed visualization of the brain structure, functional neuroimaging assessments, such as positron emission
tomography (PET), functional magnetic resonance imaging (fMRI), and magnetic resonance spectroscopy (MRS) further investigators to evaluate both brain structure and activity in the brain more closely. For examples, meta-analysis of diffusion-tensor imaging (DTI) studies identified fractional anisotropy reductions of left frontal
lobe and temporal lobe in schizophrenia and supported that in addition to gray matter deficits, disruption of white matter integrity may be affected in schizophrenia and findings from resting-state fMRI have supported that schizophrenia patients and their healthy first-degree relatives have impaired connectivity from DLPFC to its
coordinated regions including the bilateral caudate, left middle/inferior frontal gyrus, left precentral gyrus, and right cerebellum.
The study of cognitive impairments with neuroimaging tools may be potential biomarkers of schizophrenia by identifying the neurophysiologic connections of cognitive impairments. There are evidences that linked impairments of key cognitive domains to brain dysfunction including working memory and episodic memory with hypofrontality, executive function with deficits in dorsolateral prefrontal cortex (DLPFC) , anterior cingulate cortex (ACC) and mediodorsal nucleus of the thalamus and poorer verbal working memory performance with decreased white matter
integrity between prefrontal and parietal cortices . Moreover, Subramaniam et al demonstrated that cognitive training generalized to an untrained higher-order
operation and produced a significant improvement in its correlation of fMRI activity in patients with schizophrenia, suggesting that neuroimaging tools could be used as the outcome measurement s for pro-cognitive agents or programs. To date, the quality of neuroimaging has dramatically increased so investigators are able to evaluate neurodevelopmental abnormalities and neurodegenerative changes in the brain by combining structural and functional measures. Therefore, the capacity to test the relationship of cognitive symptoms and brain abnormalities (including both structure and dynamics) in schizophrenia is promising.For examples, MRS providing chemical composition, neurotransmitter levels, and neuronal integrity in living tissue is
in schizophrenia; the majority of brain image studies on cognitive deficits are to approach the connections of activity/volume in a brain region of interest (ROI) during cognitive tasks in schizophrenia patients and healthy controls respectively. However, there is a considerable inconsistency caused by heterogeneous subjects across studies and methodological differences in various cognitive tasks, image processing and quality assurance protocols. Besides unifying image operations and cognitive tasks during image survey, further studies will need to identify more homogeneous subject groups and follow patients longitudinally throughout the illness stages to understand the role of neurophysiologic disturbances and further, to develop specific imaging biomarkers for aligned use in trials of cognitive dysfunction in schizophrenia.
Peripheral modalities
Blood is the safe and maybe the most available route to develop biomarker of schizophrenia. For the examples of excitatory amino acids (EAA), Hashimoto et al reported that serum levels of D-serine and the ratio of D-serine to total serine in patients with schizophrenia are significantly decreased in schizophrenia patients than in healthy subjects. Decreased plasma glycine levels, lower glycine/serine ratio and higher homocysteine levels were found in schizophrenia patients than in comparison subjects . Higher serum level of D-serine was associated with more symptom
improvements of positive, negative and cognitive symptoms in a D-serine add-on treatment for schizophrenia patients. Another example is brain-derived neurotrophic factor (BDNF), in a 50 hours computerized auditory training that enrolled chronic schizophrenia patients and matched healthy comparison subjects, serum BDNF levels were significantly increased in schizophrenia subjects after neurocognitive training, and the authors suggested that serum BDNF levels may serve as a peripheral
suggested that EAA levels (D- serine level and glycine level) and BDNF levels may be promising convenient peripheral markers for schizophrenia and changes of the levels may reflect the improvement of the clinical and cognitive symptoms.
Pharmacotherapy based on biological aspects of cognitive impairment in schizophrenia
A number of diverse etiological hypotheses including neurodevelopmental, neurodegenerative, immunological, inflammatory, infectious and metabolic pathophysiological mechanisms for schizophrenia have been proposed.Evidences show that schizophrenia is a polygenic disorder in which the multiple susceptibility genes act together with environmental stressors in increasing vulnerability. Many of the susceptibility genes identified for schizophrenia are responsible for regulating neuronal connectivity and synaptogenesis that are associated with learning and memory indicating pathophysiology of cognitive impairments could be the important etiology of schizophrenia. Although improving cognitive function is crucial, the effect of present psychotherapeutic medication, typical and atypical antipsychotics, for cognitive impairments in schizophrenia is controversial .
Cognition is a highly complex CNS function depends upon interconnectivity of multiple CNS systems.Whereas models of the pathophysiology of schizophrenia per se emphasize excessive signaling in subcortical dopamine (DA) pathways, the accumulating research supported a link between schizophrenia and functional and anatomical dysconnectivity that lead structural changes of association fibers at the cellular level and aberrant control of synaptic plasticity at the synaptic level. Besides dopamine pathway, a diverse palette of neurotransmitters, such as glutamate, gamma-aminobutyric acid (GABA), and acetylcholine influence cognitive performance. These neurochemical systems constitute a large, heterogeneous set of potential targets
for novel therapeutic agents to remediate cognition in schizophrenia.
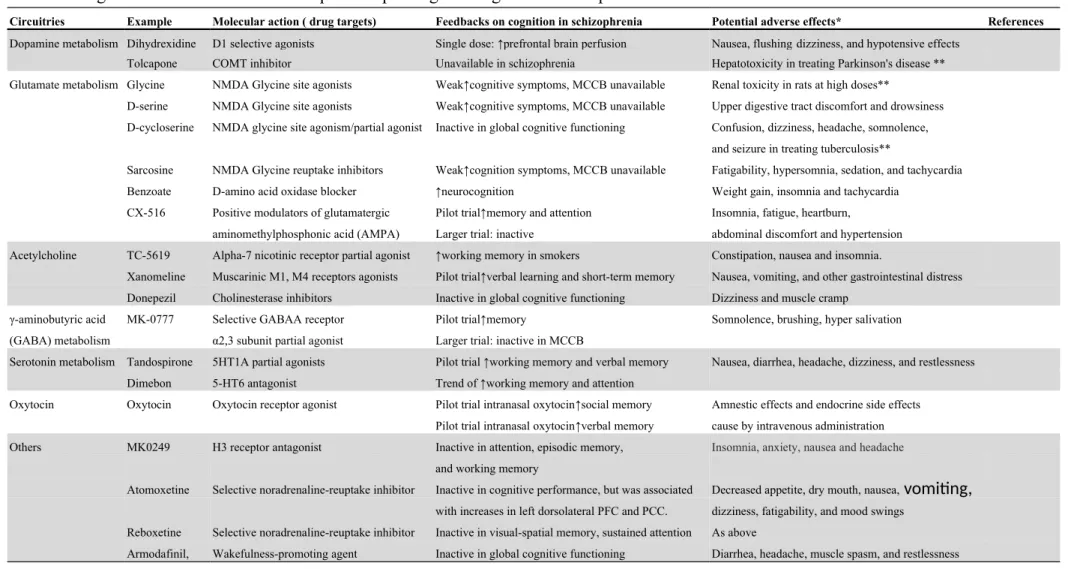
Many strategies for developing pro-cognitive agents in schizophrenia have been proposed and the recently popular approaches are on putative agents that may directly or indirectly enhance neuroplasticity. These include research on pro-cognitive agents those enhance neurotransmission (e.g., cholinesterase inhibitors), stimulate or inhibit brain receptors (e.g., NMDA receptor glycine site agonists).According to the
registered records of ClinicalTrials.gov , the most widely studied of these are neurochemical mechanisms related with the dopamine metabolism, glutamate metabolism , GABA metabolism, serotonin metabolism, acetylcholine metabolism , and oxytocin (Table 2).
Dopamine targets
Dopamine D1 receptor agonists
Davis et al provided a mechanism to propose that schizophrenia is characterized by frontal hypodopaminergia resulting in striatal hyperdopaminergia. While exposure to dopamine D2 receptor agonists induces psychotic symptoms and that conventional antipsychotic drugs block subcortical D2 receptors, a deficit in cortical dopamine transmission at D1 receptors may be associated with cognitive impairments of executive function and working memory in schizophrenia. Dopamine D1 receptor agonists/partial agonists have been putative targets for cognition enhancement for the localization of D1 receptors in prefrontal cortex (PFC) profoundly may be associated with higher cognitive function. PFC regulation behavior, thought, and working memory and dopamine depletion may induce PFC cognitive impairment in animals . Impairments of working memory and executive functioning domains have been linked with decreased PFC dopamine signaling.A single subcutaneous dose of dihydrexidine,
a D1 selective agonists, was safe and increased prefrontal brain perfusion in patients with schizophrenia in a pilot study. However, there are some flaws need to be
overcome: D1 receptor agonists have not been shown to exert any cognitive improvement in human, chronic treatment with a D1 agonist may lead to down-regulation of D1 receptors and may exacerbate cognitive dysfunction, and direct-acting D1agonists on peripheral D1 receptors could lead to hypotensive effects.
Catechol-O-methyltransferase inhibitor
Catechol-O-methyltransferase (COMT) methylates catecholamines and COMT may be important for the breakdown of PFC dopamine levels, particularly during performance of PFC-dependent tasks. Given the role of indirect dopamine-activating regulation, the use of COMT inhibitors is another tractable therapeutic target for cognitive impairments in schizophrenia. For examples, cognitive performance was improved following inhibition of COMT with tolcapone, a COMT antagonist, in rat. Clinical trials have been conducted to test the effects of COMT inhibition on
cognition in schizophrenia. Notably, tolcapone increased prepulse inhibition (PPI) and
improved performance in working memory tasks only in the COMT Val158Met G/G
group of healthy male subject suggesting that the efficacy may be in condition of special pharmacogenetic background.
Glutaminergic targets
Glutamate is the most important excitatory amino acid in central nervous system among mammalian animals, and affects the exercise and emotion function. There is evidence supporting that deficient glutamatergic functioning is associated with full-scale symptoms in schizophrenia. Moreover, many of susceptibility genes for schizophrenia regulate synaptogenesis at glutamate synapses and glutamate neurotransmission.
NMDA receptor antagonist
Agents acting at the glutamate system were the most frequently studied class of pro-cognitive drugs since enhanced glutamate release from presynaptic neurons and
activation of postsynaptic N-methyl-D-aspartate (NMDA) receptors assist long-term potentiation (LTP) induction which is critical for strengthening synaptic plasticity and facilitating learning. NMDA receptor is the most fine-defined glutamate receptor, could modulate synaptic plasticity, memory, and cognition and the dysfunction of NMDA receptor might cause the lost of neuroplasticity and cognition impairments. NMDA receptor antagonists could not only cause positive, negative, and cognitive symptoms of schizophrenia in healthy subjects but also deteriorate positive and negative symptoms in schizophrenic patients. The important role played by NMDA receptors in both the pathophysiology of schizophrenia and neuronal plasticity suggest that enhancement of NMDA receptor function may cope with the cognitive
impairments in schizophrenia. NMDA receptor channels could be functioned through glutamate and glycine sites and excitotoxicity could be prevented while the glycine sites of NMDA receptor are enhanced . These treatments safely facilitate NMDA receptor function with agonists of the NMDA receptor-associated glycine site included: D-serine, glycine, D-alanine, D-cycloserine.
GlyT-I glycine transporter I (GlyT-1) inhibitor
Besides the action of agonists, NMDA receptor function also can be safely enhanced indirectly with Glycine transporter I (GlyT-1) inhibitor. GlyT-1 inhibitor is importnat in the process of NMDA glutamatergic neurotransmission; the glycine supply to synapse could be incresed through sarcosine by blocking the reuptake of glycine. GlyT-1inhibitor has been one of the most promising approaches for pro-cognitve agents via enhancing NMDA receptor function. For example, sarcosine, an endogenous GlyT-1 inhibitor, alone or combined with other antipsychotics could improve schizophrenia patients’ positive, negative, and cognitive symptoms while comparing with placebo. Another exapmle is bitopertin, which is currently in a
number of phase III clinical trials comparing its effect on the symptoms of
schizophrenia with placebo. From previous research aimed on schizophrenia patients, it was suggested that D-Serine, glycine, and sarcosine might modify part of cognitive function. However, study on the efficacy of these NMDA enhancers for cognitive impairments in schizophrenia using comprehensive tool such as MCCB is limited. Since glutamate metabolism , especially NMDA receptor paly an important role in plasticity and memory, further approaches of cognitive enhancements associated with NMDA receptors are needed.
DAAO (D-amino acid oxidase) inhibitor
Another hopeful agent for treating schizophrenia is D-amino acid oxidase
(DAAO) inhibitor. DAAO, presents in mammals’ liver, kindney and brain, is the main metabolic enzyme that decreases the effect of amino acids, like serine and D-alanine. When the activity of DAAO is restrained, the metabolism of D-amino acids could be retarded so the additional way to reinforce NMDA receptor is to restrain the activity of DAAO . A randomized double blind trial has showed that DAAO inhibitor modified cognitive function in chronic schizophrenia patients , supporting the safety and pro-cognitive potential of DAAO inhibitor.Since this is the first positive result among NMDA receptor- related clinical trials using MCCB, further studies should be encouraged.
AMPA-receptor-positive modulation
The other indirect enhancement of NMDA receptor is activating glutamatergic α-amino-3-hydroxy-5-methyl-4-isoxazolepropionic acid (AMPA) receptor. Postsynaptic AMPA receptors provide the primary depolarization to activate NMDA receptors, while NMDA receptors are required for cooperation of AMPA receptors to process synaptic plasticity. Therefore, activation of AMPA receptors to enhance glutamatergic
transmission may be important for learning and memory. However, AMPA receptors rapidly desensitize after activation. To avoid desensitization of AMPA receptors, ampakines, allosteric potentiators of AMPA receptors function, are managed as treatments for enhancing cognition in schizophrenia. The use of ampakines were found to inhibit receptor deactivation and potentiate LTP and improve performance of memory tasks in rodents.In a 4-weeks clinical trial of 21 schizophrenia patients on clozapine, coadministration of the ampakine CX-516 yielded significant
improvements in memory and attention, however, in a larger trial of 105
schizophrenia patients on atypical antipsychotics, CX-516 augmentation was well tolerated but not show clear beneficial effects. Suboptimal does and short half-life of CX-516 and short trial duration may contribute to the inconsistent findings.
Ampakines are heterogeneous with different potency, half-life and pharmacodynamic effects, thus, besides CX-516, other AMPA-receptor-positive modulation is still a highly active area of research.
Cholinergic targets
Acetylcholine is a critical mediator of learning and memory and degeneration of the cholinergic neurons has been recognized as a part of the pathophysiology of Alzheimer’s disease (AD). Cholinergic approach has been the main therapy for cognitive decline in AD. In schizophrenia patients, anticholinergic drugs are usually prescribed to patients taking antipsychotics to control extrapyramidal symptoms induced by antipsychotic medication. Serum anticholinergic activity in schizophrenia patients showed a significant association with impaired cognitive performance and was significantly associated with a lowered response to cognitive training.Taken together, cholinergic targets have been widely introduced to treat cognitive impairment in schizophrenia.
Nicotinic acetylcholine receptors
Agonists at nicotinic acetylcholine receptors increase in cholinergic activity and may thereby benefit attention capacity, the variable of cognitive performance.
Nicotinic acetylcholine receptors (nAChR) and G-protein coupled muscarinic receptors are the two receptor classes of acetylcholine. The two nAChR subtypes, heteropentameric α4β2nAChRs and homopentameric α7nAChRs, are highly localized within brain regions associated with mediating cognitive function, have received
much attention. The drugs targeting α4β2nAChR and α7nAChRshave been tested for
the role in cognitive dysfunction but the results of nAChR agonists/partial agonists on cognition enhancement in patients with schizophrenia were mixed. Potential benefits for cognitive impairments and negative symptoms of α7nAChRs (TC-5619) for in schizophrenia was reported recently . Of note, in line with studies regarding cognitive improvements after nicotine administration in patients with schizophrenia, the results of TC-5619 on the working memory improvement were statistically significant smokers with schizophrenia. Other ongoing trials may help to elucidate the
uniqueness of nicotinic agonist treatments for schizophrenia patients who are regular cigarette smokers.
Muscarinic acetylcholine receptors
Muscarinic acetylcholine receptors (mAChR) are classified into five subtypes (M1 to M5) based on intracellular signaling pathways. The M1 mAChR, M4 mAChR, and M2 mAChR expressed within the CNS predominantly and involved in regulating the effects of Ach. M1 mAChR received much attention as a potential drug target to improve learning and memory. Unfortunately, it is difficult to develop selective agents for the different muscarinic receptor subtypes. No mAChR agonist, however, has undergone successful clinical development, except a 4-week small pilot study,
schizophrenia subjects treated with xanomeline, a muscarinic agonist with relative functional in vitro selectivity for the M1 and M4 receptor, showed improvements in measures of verbal learning and short-term memory function.
Acetylcholinesterase inhibitors (AChEIs)
Acetylcholinesterase is the enzyme responsible for metabolizing acetylcholine in the synaptic cleft. Inhibition of the enzyme via acetylcholinesterase inhibitors
(AChEIs) delays the breakdown of acetylcholine and elevates cholinergic
transmission. AChEIs including donepezil, rivastigmine and galantamine (a relative lower potency AChEI with allosteric nicotinic receptor modulation properties) have become the first line pharmacotherapy for mild to moderate AD though the treatment effects on daily living activities and behavior are partially. Potential benefits of AChEIs adjunctive therapy in cognitive impairments in schizophrenia was supposed, however, there is weak clinical evidence that AChEIs benefit for schizophrenia in randomized, placebo-controlled studies .
γ-aminobutyric acid (GABA) targets
GABA is the main inhibitory neurotransmitter and GABA receptors are the principal inhibitory neurotransmitter receptors in human CNS. Frontocortical GABA interneurons and pyramidal cells integrate inputs from modulators controlling
cognitive function, including monoamines, acetylcholine and glutamate. GABA type A (GABAA ) receptors modulate emotions, cognition, and muscle tone and are targets of clinically used drugs, such as anxiolytics, sedatives, and hypnotics. A disturbance in cortical GABAA receptor signaling connected with schizophrenia was reported and it has been proposed that full positive allosteric modulators of α2, α3 or α5 subunit subtype that are unrelated to the current uses of benzodiazepines may provide
therapeutic potential for the defect cognition in schizophrenia. MK-0777, a relatively selective agonist at the GABAAα2 subtype, induced reversal of ketamine-induced
working memory impairments by the GABAA alpha2/3 agonism in primates and improvement of prefrontal-mediated delayed memory in schizophrenia in a small sample size trial. In contrast with the promising preliminary data, it was recently reported that MK-0777 did not have an improvement in cognition of schizophrenia subjects in a large, multi-site, randomized clinical trial and the authors suggested that a more potent partial agonist with greater intrinsic activity at the GABAA α2 site might be needed for cognitive enhancement in schizophrenia .
Serotonergic targets
5-hydroxytryptamine (Serotonin, 5-HT) transporters are widely distributed in the brain areas linked to memory such as the hippocampus, frontal cortex and
striatum. Serotonin acts through several 5-HT receptors in the brain to modulate dopaminergic neurotransmission and the ultimate effect of 5-HT/DA interactions has been posited as the main feature of atypical antipsychotics such as clozapine and benefit to negative and cognitive deficits. 5-HT1A receptor agonists, 5-HT2C receptor agonists, 5-HT6 receptor antagonists and 5-HT7 receptor ligands may contribute to beneficial effects on schizophrenia including negative cognitive symptoms . It is also noteworthy that some selective 5-HT2A receptor antagonists blocked the cognition-damage effects (prepulse inhibition) of NMDA receptor antagonist in rats so that 5-HT2A antagonistic actions may normalizing NMDA receptor function and thereby improve cognition in schizophrenia. In addition, 5-HT4 receptor agonists and 5-HT6 receptor antagonists have shown enhancing cholinergic transmission and 5-HT6 receptor antagonism also have shown enhancing neurotransmission at glutamatergic neurons.
Taken together, studies suggest an intimate association between 5-HT receptors and dopamine, acetylcholine and glutamine systems and imply that the modulation of
serotonin neurotransmission may prove value in the treatment of disorders involving glutamatergic /dopamine /cholinergic dysfunction such as schizophrenia. However the preclinical and clinical literatures are mixed regarding whether 5-HT agonists or antagonists enhance cognition. Among the limited clinical feedbacks, a study of 6 weeks administration of tandospirone, a 5-HT1A partial agonist, augmented with typical antipsychotic drugs enhanced verbal memory in 26 outpatients with schizophrenia but a risk for exacerbating positive symptoms of 5-HT agonist in schizophrenia was a concern. To date, no compound aimed at 5-HT receptors solely benefits cognitive function in schizophrenia patients. Moreover, many approved atypical antipsychotics have 5-HT2A antagonist and 5-HT1A partial agonist actions, it is unlikely that atypical antipsychotics have powerful efficacy of improving cognition in schizophrenia. These results demonstrate that additional clinical studies are needed.
Oxytocin and others
Oxytocin is released from the posterior pituitary in response to sexual
stimulation, uterine dilatation, nursing, and, in some situations, stress. Animal studies connected oxytocin with social recognition, pair bonding, and parental behavior while human studies associated oxytocin with facial emotion perception, trust, and coping with stress. Oxytocin may play important role in social behavior and emotion regulation in humans and dopaminergic or glutamatergic systems appear to mediate these effects.There have been growing trials on oxytocin in neuropsychiatric disorders in recent 5 years. Single-dose infusion of oxytocin showed improvements in affective speech comprehension in autistic spectrum disorders, 2 weeks of intranasal oxytocin administration may improve social cognition in schizophrenia. Moreover, 3 weeks of twice-daily intranasal oxytocin adjunctive to standard antipsychotic medications
caused reductions on the Positive and Negative Symptom Scale and Clinical Global Impression-Improvement Scale in schizophrenia subjects may support that oxytocin exhibits antipsychotic properties. However, the sample size was very small and the trial duration was brief in these studies. An important concern is that amnesic effects have been reported in humans treated with oxytocin, although better verbal memory performance with 3 weeks adjunctive intranasal oxytocin in schizophrenia subjects was reported recently. Further comprehensive studies about the impact of oxytocin on both social cognition and neurocognition in schizophrenia are needed.
Histamine H3 receptor antagonist , dopamine and noradrenaline-reuptake transporter inhibitors, selective noradrenaline-reuptake inhibitor, wakefulness-promoting agent have been also introduced as pro-cognitive agents in schizophrenia, however, robust positive effect has not been reported yet.
We identified 59 published clinical trials on pro-cognitive drugs in schizophrenia patients through the Pubmed website from January 1990 to February 2012 using the terms ‘‘schizophrenia and dopamine agonists ’’, ‘‘schizophrenia and COMT ’’, ‘‘schizophrenia and glutamate’’, ‘‘schizophrenia and acetylcholine’’, ‘‘schizophrenia and γ-aminobutyric acid ’’, ‘‘schizophrenia and serotonin ’’, ‘‘schizophrenia and oxytocin ’’, ‘‘schizophrenia and histamine’’, ‘‘schizophrenia and norepinephrine’’, and ‘‘schizophrenia and stimulant’’. Positive results of modest to moderate degrees of diverse cognitive improvement in 31 researches were reported, while negative results were reported in 28studies (Supplemental Figure). Although the trend of bias of more positive results on publications of newer experimental agents is unapparent, it should be noted that according to the analysis of completed clinical trials of potential pro-cognitive drugs in schizophrenia by Keefe et al, suboptimal statistical power is a critical methodological issues. Therefore ongoing efforts should be made to increase
the probability of identifying pro-cognitive treatments in schizophrenia.
Non-pharmacological cognitive remediation therapy
Various psychosocial cognitive rehabilitation and enhancement programs ( also often referred to as cognitive remediation therapy), that provide computerized exercises, therapist-guided instruction, and group discussions to link training exercises to everyday life have been introduced to remediate the cognitive
impairments in schizophrenia. The benefit of cognitive remediation therapy was built upon repetitive training to enhance neuroplasticity of the brain and supported by the improved performance of neuropsychological test and the accompanied neuroimaging change and biological change. Meta-analytic reviews supported the short-term
benefits of cognitive remediation therapy on cognitive domains with small to moderate effect, and limited longitudinal studies showed improvements in several cognitive domains endured at 6-12 months. In addition, higher dose and more broad-spectrum training programs may be necessary to drive enduring gains of cognitive remediation therapy. It should be noted that the small sample sizes and the
characteristics of subjects (mostly male patients, narrowed age distribution in mid-thirties, and requests of low symptom severity and educational levels of enrolling for trials) limited the generalization of the positive results and it is not yet clear whether or not cognitive remediation therapy results in improved long-term functional
outcome. The duration and intensity/dose, and programs/strategies of cognitive remediation therapy have been variable across studies since there has been rapid multiplication of new and adapted cognitive remediation approaches. Long-term maintenance of cognitive effects, the effectiveness of transferring to real-world functional competence and the ideal duration/dose of cognitive rehabilitation
programs remain unclear. Nevertheless,the effectiveness of cognitive remediation is providing opportunity for improving everyday functioning of schizophrenia patients.
It is interesting that cognitive remediation therapy that provided more
comprehensive integration with neurocognitive and psychosocial rehabilitation that included coaching strategies and adjunctive social rehabilitation showed greater effects on functioning , so there is a need to understand mediators and moderators of the synergic benefit. Social cognition may impact the functional outcome of
independent living skills because intact social skills are vital for negotiating good interpersonal interactions in real world. Neurocognitive impairments may have an deleterious effect on social cognition and thereby social cognition mediated
neurocognition and functional outcome. Programs implant social skill training may be a way to enhance the efficacy of cognitive remediation therapy programs or even pro-cognitive agents.
Combination therapy
Augmentation of antipsychotics with combining of pro-cognitive agents and cognitive rehabilitation programs would be expected to maximize the benefits of cognitive improvement. Although the first study of combined pharmacotherapy (D-serine) and cognitive remediation therapy reported that while cognitive retraining resulted in a significant improvement in verbal working memory, D-Serine or the combination of D-Serine and cognitive retraining did not show any significant effect on the global cognitive improvement in schizophrenia subjects. Since the safety and tolerability were good in the combination therapy, future studies using higher doses of D-serine or other pro-cognitive agents, along with the newer cognitive remediation strategies has been encouraged. Another promising strategy is to combine with two kinds of pro-cognitive agents via different mechanisms; however the safety and
tolerability should be investigated carefully.
Conclusions
Despite preclinical bench data, there has been limited positive clinical feedback for current putative pro-cognitive drugs target in humans. Add-on, placebo-controlled, double-blind design was predominant across the completed trials those tended to have a small sample size (the majority was less than 50 subjects), to have a shorter study duration (ranged from 2-24 weeks, 8 weeks was in the majority), to be an add-on trial, and use a single cognitive outcome measure. There has been limited robust effect on cognitive improvement so far for current pro-cognitive agents. The possible
methodological reasons, the limited sample sizes and the short treatment duration, could be related with the suboptimal results of little changes in cognitive scores. Moreover, to obtain robust and consistent effects, studies of pro-cognitive agents in schizophrenia conducted in subjects who are younger, at an earlier stage of illness, or have less severe cognitive impairments are necessary. Besides pharmacotherapy, the benefit of cognitive remediation therapy is promising, however, the generalization of the positive results has been limited and the variable programs across studies need further integration. Combination therapy, by integrating pro-cognitive agents and cognitive rehabilitation programs or combining two kinds of pro-cognitive agents via different mechanisms is hopeful if safety and tolerability will be investigated
carefully.
Given the broad pattern of cognitive impairments, from attention and working memory to social cognition in schizophrenia, the efficacy on a single dimension, such as working memory, would not suffice to predict the effect on overall cognitive improvement. Therefore, the lately ongoing trials with adequate sample size, with comprehensive outcome measurement to meet adopted standards for cognitive
assessments and longer duration may be promising for investigating enhancement of cognition with positive results in schizophrenia. Furthermore, more future studies should be intensively focused on investigating the long-term efficacy, identity of multinational sites, the rebound deterioration in psychosis/cognition following the discontinuation, and co-outcomes of related biomarkers and daily functioning improvement.
References
Table 1. Batteries of assessing the cognitive impairments in schizophrenia
Battery Domains (constructs) References
Treatment Research to Improve Cognition in Schizophrenia Speed of processing
Consensus Cognitive Battery Sustained attention
(MCCB) Working memory, verbal and
Verbal learning and memory
Visual learning and memory
Reasoning and problem solving
Social cognition
Brief Assessment of Cognition in Schizophrenia Working memory
(BACS) Motor speed
Verbal fluency
Attention and speed of information Executive functions Cognitive Drug Research Computerized Attention
Assessment System (CDR) Working memory
Episodic Memory
Selective and Sustained Attention Working Memory Declarative Memory Executive Function Set Shifting Conflict Functions
Language and Spatial Skills Motor Speed and Laterality
Social Cognition
Cambridge Neuropsychological Test Visual memory Automated Battery (CANTAB) Attention and reaction time
Verbal memory
Decision making and response
Executive function
Emotion recognition
Table 2. Targets and clinical feedbacks for putative pro-cognitive agents in schizophrenia
Circuitries Example Molecular action ( drug targets) Feedbacks on cognition in schizophrenia Potential adverse effects* References
Dopamine metabolism Dihydrexidine D1 selective agonists Single dose: ↑prefrontal brain perfusion Nausea, flushingdizziness, and hypotensive effects Tolcapone COMT inhibitor Unavailable in schizophrenia Hepatotoxicity in treating Parkinson's disease ** Glutamate metabolism Glycine NMDA Glycine site agonists Weak↑cognitive symptoms, MCCB unavailable Renal toxicity in rats at high doses**
D-serine NMDA Glycine site agonists Weak↑cognitive symptoms, MCCB unavailable Upper digestive tract discomfort and drowsiness D-cycloserine NMDA glycine site agonism/partial agonist Inactive in global cognitive functioning Confusion, dizziness, headache, somnolence,
and seizure in treating tuberculosis**
Sarcosine NMDA Glycine reuptake inhibitors Weak↑cognition symptoms, MCCB unavailable Fatigability, hypersomnia, sedation, and tachycardia Benzoate D-amino acid oxidase blocker ↑neurocognition Weight gain, insomnia and tachycardia
CX-516 Positive modulators of glutamatergic Pilot trial↑memory and attention Insomnia, fatigue, heartburn, aminomethylphosphonic acid (AMPA) Larger trial: inactive abdominal discomfort and hypertension Acetylcholine TC-5619 Alpha-7 nicotinic receptor partial agonist ↑working memory in smokers Constipation, nausea and insomnia.
Xanomeline Muscarinic M1, M4 receptors agonists Pilot trial↑verbal learning and short-term memory Nausea, vomiting, and other gastrointestinal distress Donepezil Cholinesterase inhibitors Inactive in global cognitive functioning Dizziness and muscle cramp
γ-aminobutyric acid MK-0777 Selective GABAA receptor Pilot trial↑memory Somnolence, brushing, hyper salivation (GABA) metabolism α2,3 subunit partial agonist Larger trial: inactive in MCCB
Serotonin metabolism Tandospirone 5HT1A partial agonists Pilot trial ↑working memory and verbal memory Nausea, diarrhea, headache, dizziness, and restlessness Dimebon 5-HT6 antagonist Trend of ↑working memory and attention
Oxytocin Oxytocin Oxytocin receptor agonist Pilot trial intranasal oxytocin↑social memory Amnestic effects and endocrine side effects Pilot trial intranasal oxytocin↑verbal memory cause by intravenous administration
Others MK0249 H3 receptor antagonist Inactive in attention, episodic memory, Insomnia, anxiety, nausea and headache
and working memory
Atomoxetine Selective noradrenaline-reuptake inhibitor Inactive in cognitive performance, but was associated Decreased appetite, dry mouth, nausea, vomiting, with increases in left dorsolateral PFC and PCC. dizziness, fatigability, and mood swings
Reboxetine Selective noradrenaline-reuptake inhibitor Inactive in visual-spatial memory, sustained attention As above
Armodafinil, Wakefulness-promoting agent Inactive in global cognitive functioning Diarrhea, headache, muscle spasm, and restlessness
* No dropout was due to severe adverse effect in current available clinical trials. **No detrimental changes in clinical laboratory parameters in clinical trials.
Abbreviations:
COMT: Catechol-O-methyltransferase ; NMDA: N-methyl-D-aspartate
MCCB: Treatment Research to Improve Cognition in Schizophrenia Consensus Cognitive Battery DLPFC: dorsolateral prefrontal cortex PCC: posterior cingulate cortex
Supplemental Figure
Ratios of positive and negative results of clinical trials focused on pro-cognitive effect in schizophrenia, by different circuitries.
Abbreviations:
GABA: γ-aminobutyric acid
Legend of supplemental figure
59 published clinical trials with cognitive improvement as the primary or secondary outcome of schizophrenia subjects through searches of the Pubmed website using the terms ‘‘schizophrenia and dopamine agonists ’’, ‘‘schizophrenia and COMT ’’, ‘‘schizophrenia and glutamate’’, ‘‘schizophrenia and acetylcholine’’, ‘‘schizophrenia and γ-aminobutyric acid ’’, ‘‘schizophrenia and serotonin ’’, ‘‘schizophrenia and oxytocin ’’, ‘‘schizophrenia and histamine’’, ‘‘schizophrenia and norepinephrine’’, and ‘‘schizophrenia and stimulant’’ were identified from January 1990 to February 2012. Positive results of modest to moderate degrees of cognitive improvement in 31 researches were reported, while negative