Is Zolpidem Associated with Increased Risk of
Fractures in the Elderly with Sleep Disorders?
A Nationwide Case Cross-Over Study in
Taiwan
Yih-Jing Tang
1,2☯, Shinn-Ying Ho
3,4☯, Fang-Ying Chu
4, Hung-An Chen
4, Yun-Ju Yin
4,
Hua-Chin Lee
4, William Cheng-Chung Chu
5, Hui-Wen Yeh
4,6,7, Wei-Shan Chiang
7,8,
Chia-Lun Yeh
4, Hui-Ling Huang
3,4*, Nian-Sheng Tzeng
8,9*
1 Department of Family Medicine, Center for Geriatrics and Gerontology, Taichung Veterans General Hospital, Taichung, Taiwan, 2 School of Medicine, Chung Shan Medical University, Taichung, Taiwan, 3 Institute of Bioinformatics and Systems Biology, National Chiao Tung University, Hsinchu, Taiwan, 4 Department of Biological Science and Technology, National Chiao Tung University, Hsinchu, Taiwan, 5 Department of Computer Science, Tunghai University, Taichung, Taiwan, 6 Department of Nursing, Tri-Service General Hospital, School of Nursing, National Defense Medical Center, Taipei, Taiwan, 7 Institute and Department of Mathematics, National Tamkang University, New Taipei City, Taiwan, 8 Department of Psychiatry, Tri-Service General Hospital, School of Medicine, National Defense Medical Center, Taipei, Taiwan, 9 Student Counseling Center, National Defense Medical Center, Taipei, Taiwan
☯ These authors contributed equally to this work.
*hlhuang@mail.nctu.edu.tw(HLH);pierrens@mail.ndmctsgh.edu.tw(NST)
Abstract
Background
We conducted a study using a case-crossover design to clarify the risk of acute effects of
zolpidem and benzodiazepine on all-sites of fractures in the elderly.
Design of study
Case-crossover design.
Methods and Materials
Elderly enrollees (n = 6010) in Taiwan
’s National Health Insurance Research Database with
zolpidem or benzodiazepine use were analyzed for the risk of developing fractures.
Results
After adjusting for medications such as antipsychotics, antidepressants, and diuretics, or
comorbidities such as hypertension, osteoarthritis, osteoporosis, rheumatoid arthritis and
depression, neither zolpidem nor benzodiazepine was found to be associated with
increased risk in all-sites fractures. Subjects without depression were found to have an
increased risk of fractures. Diazepam is the only benzodiazepine with increased risk of
OPEN ACCESS
Citation: Tang Y-J, Ho S-Y, Chu F-Y, Chen H-A, Yin Y-J, Lee H-C, et al. (2015) Is Zolpidem Associated with Increased Risk of Fractures in the Elderly with Sleep Disorders? A Nationwide Case Cross-Over Study in Taiwan. PLoS ONE 10(12): e0146030. doi:10.1371/journal.pone.0146030
Editor: Uwe Rudolph, McLean Hospital/ Harvard Medical School, UNITED STATES
Received: April 17, 2015 Accepted: December 12, 2015 Published: December 30, 2015
Copyright: © 2015 Tang et al. This is an open access article distributed under the terms of the
Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Data Availability Statement: Data are available from the Longitudinal Health Insurance Database (LHID) published by Taiwan National Health Insurance (NHI) Bureau. Due to legal restrictions imposed by the government of Taiwan in relation to the“Personal Information Protection Act”, data cannot be made publicly available. Requests for data can be sent as a formal proposal to the NHIRD (http://nhird.nhri.org.tw/ index1.php).
Funding: This work was supported by grant number Tri-Service-General-Hospital (TSGH)-C103-019. This work was also funded by Ministry of Science and
fractures after adjusting for medications and comorbidities. Hip and spine were particular
sites for increased fracture risk, but following adjustment for comorbidities, the associations
were found to be insignificant.
Conclusion
Neither zolpidem nor benzodiazepine was associated with increased risk of all-site fractures
in this case cross-over study after adjusting for medications or comorbidities in elderly
indi-viduals with insomnia. Clinicians should balance the benefits and risks for prescribing
zolpi-dem or benzodiazepine in the elderly accordingly.
Introduction
Fractures are a significant and growing health problem for elderly individual, and are
associ-ated with increased morbidity and mortality [
1
–
3
]. Though the absolute incidence of fractures
in the elderly has decreased in recent years, the resulting economic burden and mortality have
increased [
1
,
4
,
5
]. In France, a 5-year (2000
–2004) analysis of 2,625,743 death certificates
showed a 2.2% incidence of fractures, resulting in a crude number of deaths associated with
fractures of 57,753, while the number associated with osteoporotic fractures was 46,849 (1.85%
and 1.78% of all deaths, respectively) [
2
]. Fractures also impose high medical costs during and
even after surgical treatment; in the United States, costs for pelvic, hip and tibia fractures
accrue in the second year following injury ($5,121, $3,930, and $3,828, respectively) [
6
].
Previous studies have shown that hypertension [
7
], osteoarthritis and osteoporosis [
8
],
dia-betes mellitus, depression, hyperlipidemias, heart failure, dementia and cardiovascular disease
[
9
–
11
] are associated with increased risk of fractures in the elderly. Vitamin D deficiency is
also a known risk factor for fractures [
12
,
13
]. Aging and the ensuing reduction in physical
activity, could also contribute to fractures [
13
]. Falling injuries may contribute to pelvic [
14
,
15
], hip [
16
] and other fractures in the elderly [
17
].
In previous studies, zolpidem [
18
–
21
] and benzodiazepine (BDZ) [
22
,
23
] were reported to
be associated with increased risk of elderly hip or non-vertebral fractures. Few studies
exam-ined the association between hypnotics and non-hip fractures. Furthermore, a case-crossover
study design might be more suitable to clarify the acute or short-term effects on risk in all-sites
fractures in the elderly associated with zolpidem [
24
,
25
], since the hangover effects or complex
sleep behaviors associated with these drugs (e.g., zolpidem-related somnambulism) usually do
not persist for more than a day [
26
–
30
].
This study used the Taiwan National Health Insurance Research Database (NHIRD) to
determine the association of zolpidem or BZDs and all-sites of fractures in the elderly from
2000 to 2010. As of June 2009, Taiwan’s National Health Insurance (NHI) Program covered
22,928,190 people, exceeding 99% of the population. The NHI also has contracts with 97% of
medical providers in Taiwan [
31
]. The NHI uses diagnostic coding in accordance with the
International Classification of Diseases, 9th Revision, Clinical Modification (ICD-9-CM)
diag-nostic criteria [
32
]. Each fracture diagnosis is made by board-certified orthopedic surgeons.
The Bureau of National Health Insurance randomly reviews the charts of 1 per 100 ambulatory
and 1 per 20 in-patient claim cases to verify diagnosis accuracy [
33
].
Technology of Taiwan under the contract number MOSTE-009-117- and MOST -103-2221-E-009-141-, and "Center for Bioinformatics Research of Aiming for the Top University Program" of the National Chiao Tung University and Ministry of Education, Taiwan, R.O.C. for the project 103W962. This work was also supported in part by the UST-UCSD International Center of Excellence in Advanced Bioengineering sponsored by the Taiwan Ministry of Science and Technology I-RiCE Program under Grant Number: MOST-103-2911-I-009-101-. The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
Competing Interests: The authors have declared that no competing interests exist.
Materials and Methods
Data Sources
This research was based on a population-base cohort study. The data were taken from the
Lon-gitudinal Health Insurance Database (LHID) for 2005 published by the NHI Bureau. Taiwan
’s
NHI was launched in March 1995 [
34
] and covered from over 25 million Taiwanese. It also
represented approximately 98% of the Taiwanese [
35
] who lived in Taiwan for more than four
months.
The longitudinal database is a subset of the NHIDatabase consisting of 1 million samples
from Taiwanese covered by the NHI in 2005 [
36
]. It contains patient medical records for
in-patient, out-in-patient, and ambulatory care. Each sample is enrolled in the LHID with codes for
diagnoses, surgical operations, dental services, prescription drugs, medical institutions,
physi-cians, and registration data, all based on the International Classification of Disease, 9th
revi-sion, Clinical Modification (ICD-9-CM) [
37
].
Study Subjects
The present study tracked patients over the age of 65 who were using zolpidem or BDZs. In
addition, the study also discussed patients diagnosed with sleep disorders (ICD-9-CM codes
307.41–307.49 and 780.50–780.89) and their impact on fractures. The index date was defined
as the date on which subjects were diagnosed with fractures by ICD-9-CM codes for fractures
of the hip (820), humerus (812), forearm (813), wrist (814), spine (805, 806), and any other
sites (800
–829). Patients who had been previously diagnosed with fractures before the index
date were excluded. For patients, who had suffered a stroke and were paralyzed for a period of
time, it was impossible to measure the extent of paralysis and the recovery time. Therefore, we
excluded subjects with a stroke diagnosis. Regarding diseases, such as dizziness and locomotor
problems, it could not be confirmed whether the patient was paralyzed or not. Consequently,
we did not take these diseases into account. All study subjects had used hypnotics within six
months prior to the index date.
Data Collection of Study Subject Characteristics
Comorbidities or coexisting medications that might interact with the risk of fractures were
adjusted for. The confounding factors with potential to change between case and control
groups were adjusted in our analysis based on Chen, et al. [
38
]. These confounding factors
included comorbidities and coexisting medications and were identified by outpatient data. In
this study, comorbidities were defined as experiencing the following medical conditions within
one year prior to the index date in each control and hazard period: Hypertension,
osteoarthri-tis, osteoporosis, diabetes mellitus, dementia, rheumatoid arthriosteoarthri-tis, heart failure, Parkinson
’s
disease, non-stroke cerebrovascular diseases, chronic obstructive pulmonary disease (COPD),
benign prostate hyperplasia (BPH), hyperlipidemias, gout, hypothyroidism, anemia, and
depression. Medications including antidepressants, diuretics and antipsychotics were also
adjusted for.
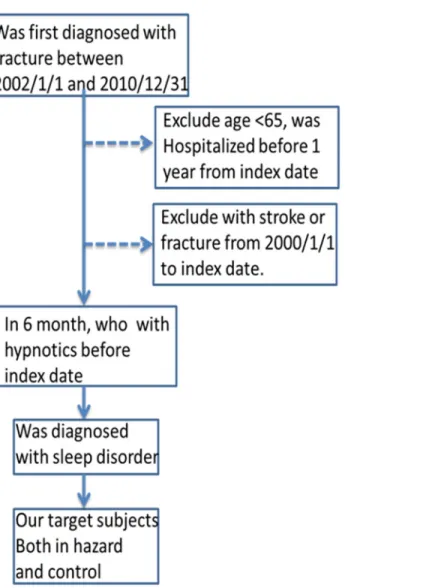
Fig 1
shows the data collection process; 5 weeks was defined as a washout period
and 1 day was used to observe if the patient took the drug or not. We had 4 controls matched
with 1 case; therefore, in total, we needed 6 months to ensure that the data were included.
Ethical Statement
The protocol for this study conformed to the Helsinki Declaration, and was approved by the
Institutional Review Board of Cathay General Hospital (permission code: CGH-P101089).
Personal identifiers from the database were encrypted or otherwise stripped prior to analysis,
and the need for written informed consent was waived by the Institutional Review Board.
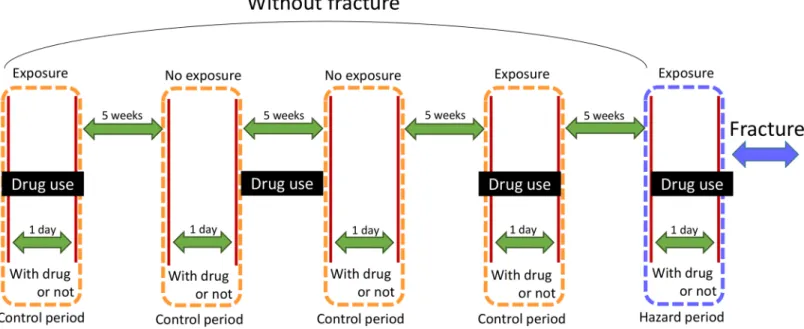
Case-crossover Design
The case-crossover design is widely used to study the acute effects of drug over short durations
[
29
,
30
]. Each enrolled subject has used the drug at least once in the past. The case-crossover
design was compared against a control of their own data prior to fracture diagnosis. This study
enrolled samples between 2002 and 2010 with washout periods of 5, 10, 15, and 20 weeks; thus
each study subject had 4 controls. In each control group, we only observed 1 day whether the
patient took drug before the 5-week-washout period. The control time windows are 1 day same
as the case time window (
Fig 2
). The impact of BDZ and zolpidem lasts less than 1 day; thus
zolpidem or BZD use was defined as use 1 day prior to the fracture. A case-crossover study
design can avoid confounding factors unrelated to time such as gender, but cannot avoid the
factors that are related to time (e.g., comorbidity and other medication).
Fig 1. Flowchart for the selection of the sample from the National Health Insurance Research Dataset. doi:10.1371/journal.pone.0146030.g001
Statistical Analyses
Statistical Product and Service Solution (SPSS) v19.0 is widely used for analytical computing,
data mining, and predictions. The present study used conditional logistic regression analyses
odds ratio (OR) and adjusted OR. Within 95% confidence interval p
< 0.05 was the level of
sig-nificance for fracture. Stratified analysis was used to predict changes to risk of fracture under
different conditions of BDZ and zolpidem use.
Results
Table 1
shows that more women have sleep disorders in this cohort (n = 4071, 67.7%) than
men (n = 1939, 32.3%). Most patients with sleep disorders were grouped in ages 65
–74
(n = 2482, 40.7%) and 75–84 (n = 2809, 46.8%). In our data, most patients with sleep disorders
also had hypertension (n = 3726, 62.0%) and osteoarthritis (n = 3226, 53.7%) and some had
exhibited chronic renal failure (n = 359, 5.9%) and rheumatoid arthritis (n = 176, 2.9%) in the
past year.
Table 2
shows the ORs in patients with sleep disorders. In the hazard period, more patients
used BDZ (n = 1155, 19.2%) than used zolpidem (487, 8.1%). Use of BDZ (4399, 18.0%) was
also more frequent than that of zolpidem (1755, 7.3%) in the control periods. The crude OR of
fractures in patients using BDZ was 1.17 (CI: 1.06
–1.30, p<0.05). After adjusting for use of
antidepressants, antipsychotics and diuretics, the OR was decreased to 1.13 (1.02–1.26,
p
< 0.05). For zolpidem, the adjusted odds ratio was 1.23 (CI: 1.06–1.44, p < 0.05). After
adjusting for comorbidities, used of either BDZ (OR = 1.08, CI: 0.97–1.22, p = 0.14) or
zolpi-dem (OR = 1.13, CI: 0.96
–1.34, p = 0.14) was not significantly associated with fractures
(
Table 2
).
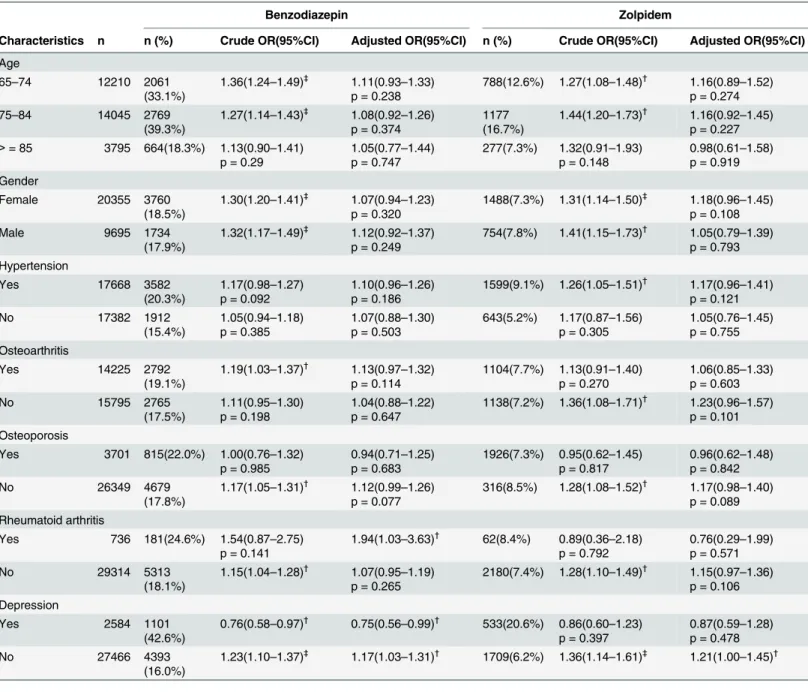
Table 3
shows stratified analysis results revealing different conditions that could impact the
likelihood of fractures. In this study, subjects aged 65–74 with BZD use were associated with
increased risk for fractures, as OR = 1.36 (CI: 1.24
–1.49, p < 0.001), but, after for adjusting
comorbidities, the OR was not significant at 1.11 (CI: 0.93–1.33, p = 0.24). Using conditional
Fig 2. The study design of case cross-over: 1) Hazard period: patients who had been diagnosed with fractures, 2) Control period: patients who had not been diagnosed with fractures, 3) Washout period: 5 weeks for the washing out of residues of drug reaction.
logistics regression analysis, patients in different age groups had no association with increased
risk for fractures, regardless of BDZ or zolpidem use. Before adjustment, both women
(OR = 1.30, CI: 1.20–1.41, p < 0.001) and men (OR = 1.32, CI: 1.17–1.49, p < 0.001) using
BDZ had significantly elevated risk of fractures. However, after adjusting for comorbidities,
neither women nor men showed significantly increased fracture risk. In patients without
depression, the OR was 1.17 (CI: 1.03–1.31, p < 0.05) with fractures after BDZ use.
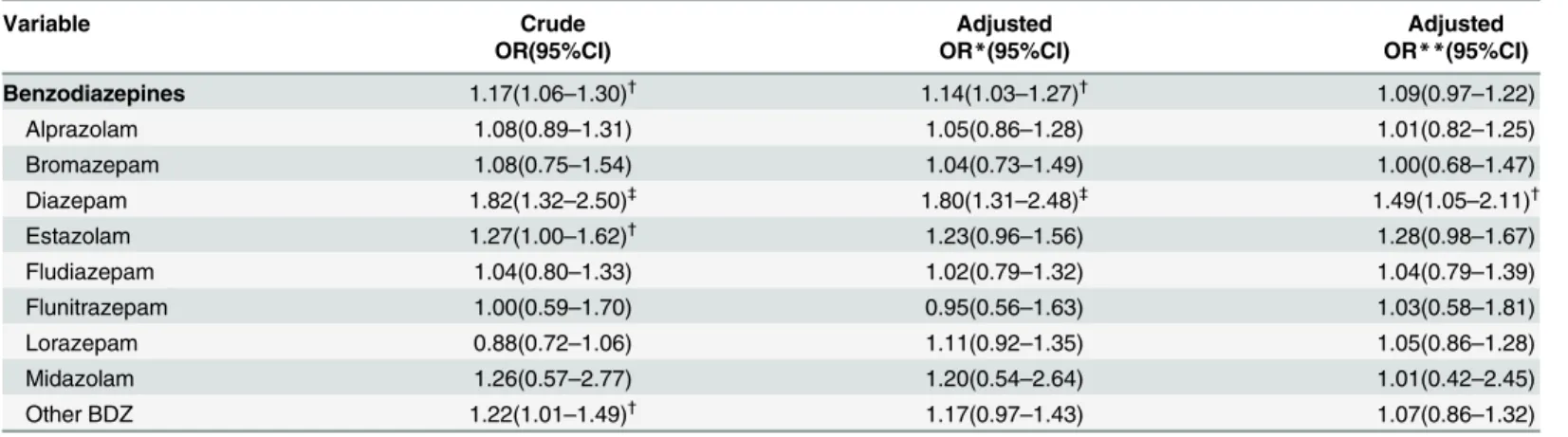
Table 4
shows the ORs for developing fractures according to different BDZ usage by elderly
patients. Several common BDZ subgroups including alprazolam, bromazepam, diazepam,
flu-diazepam, flunitrazepam, lorazepam, midazolam and other BDZs were analyzed individually.
Only diazepam revealed a crude OR of 1.82 (CI: 1.32–2.50, p < 0.001), 1.80 (CI: 1.31–2.48,
p < 0.001) after adjusting for use of antidepressants, antipsychotics and diuretics; and 1.49 (CI:
1.05–2.11, p < 0.05) after adjusting for comorbidities including hypertension, osteoarthritis,
osteoporosis, rheumatoid arthritis, and depression. Use of other BDZs showed no risk after
adjusting for medications or comorbidities.
Table 5
shows the ORs of different fracture sites in elderly patients using zolpidem or BDZ.
Humerus, forearm and wrist sites were not associated with increased fracture risk, while hip
and spine showed particularly increased risk of fractures. For hip fractures, zolpidem was
asso-ciated with a crude OR of 1.53 (CI: 1.04–2.25, p < 0.05) and, when adjusted for medications,
an OR of 1.49 (CI: 1.00
–2.22, p < 0.05). For spine fractures, zolpidem was associated with a
Table 1. Baseline characteristics of study patients (n = 6010).
Characteristics n (%) Gender Female 4071(67.7%) Male 1939(32.3%) Age 65–74 2482(40.7%) 75–84 2809(46.8%) > = 85 759(12.6%) Comorbidity Hypertension 3726(62.0%) Osteoarthritis 3226(53.7%) Osteoporosis 937(15.6%) Diabetes mellitus 1522(25.3%) Anemia 524(8.7%) Depression 583(9.7%) Dementia 325(5.4%) Rheumatoid arthritis 176(2.9%) Heart Failure 570(9.5%) Parkinson Disease 318(5.4%) non-stroke CVD 385(6.4%) COPD 563(9.4%) CRF 353(5.9%) BPH 831(13.8%) hyperlipidemia 1419(23.6%) Gout 734(12.2%)
CVD = cerebral vascular disease, CRF = chronic renal failure, BPH = benign prostate hypertrophy, doi:10.1371/journal.pone.0146030.t001
crude OR of 1.38 (CI: 1.07–1.78, p < 0.05) and, when adjusted for medications, an OR of 1.36
(CI: 1.05–1.76, p < 0.05). BDZ was associated with a crude OR of 1.22 (CI: 1.03–1.44, p < 0.05)
and, when adjusted for medications, an OR of 1.20 (CI: 1.01–1.43, p < 0.05). However, neither
site was related to increased risk of fractures after adjusting for comorbidities.
Discussion
A case-crossover design was used to account for acute drug effects in patients with continued
drug use over the study period. In the case-crossover design, the case has its own control, thus
limiting bias resulting from gender and age, along with other genetic and physiological factors.
Furthermore, it shows the immediate effects within 24 hours, rather than exposure-to-fall time
of up to 6 months as in some other studies [
17
,
18
]. Zolpidem achieves its peak plasma level
within 1.6 hours of ingestion, and the single dose (5
–10 mg) elimination half-life is 2.5–2.6
hours [
39
]. Therefore, the case-crossover approach is suitable to account for acute drug effects
on fracture risk, and has been used previously to study zolpidem use and the risk of
hospitaliza-tions resulting from motor vehicle accidents [
40
] or fractures [
18
,
19
,
21
].
Several prior case control or case cross-over studies have found that BDZ [
22
,
23
] and
zolpi-dem [
18
,
19
,
21
] are associated with increased risk of fractures in the elderly. A Korean case
cross-over design study found that zolpidem is associated with increased fractures among the
elderly with an adjusted OR = 1.72 (95% CI, 1.37–2.16), but the dataset was taken from a
shorter period (one year) and a smaller population (1508 participants) [
19
]. Another case
cross-over study focused on a mixed nursing home population with younger patients (>50
years- old) with a 1-year follow up [
21
]. The present study follows a larger population
(N = 6010) and a longer observation period (9 years, 2002–2010) in a nationwide cohort, and
finds that zolpidem use is not associated with risk of all-site fractures after adjusting for
medi-cation use and comorbidities. The subject group is limited to elderly patients without prior
his-tory of fractures or stroke, and we adjusted for comorbidities including osteoporosis,
hypertension, osteoarthritis and diabetes mellitus in addition to drug use including
anti-depressants, antipsychotics and diuretics. We found that neither zolpidem nor BDZ is
associ-ated with significantly elevassoci-ated fracture risk in elderly individuals with insomnia.
Some previous studies of hypnotics use in elderly patients with insomnia, found an elevated
fracture risk among female patients over 60 years-old [
41
]. However, the present study found
no such increased risk after adjusting for comorbidities and drug use.
One study reported that zolpidem use was associated with a greater risk of fractures among
elderly patients than alprazolam and lorazepam us, but a similar risk to that associated with
diazepam use [
17
]. Other studies also found that zolpidem was associated with a higher risk of
fractures in the elderly [
18
,
42
–
44
]. Our study, however, found that use of BDZ (18.0%) was
associated with a greater risk than used of zolpidem (7.3%) in the controlled periods.
Table 2. Risk of fractures due to the use of hypnotics in elderly insomnia patients.
Hypnotics No. of case No. of control Crude OR *Adjusted OR **Adjusted OR
(n = 6010) (n = 24040) (95% CI) (95% CI) (95% CI)
Benzodiazepine 1155(19.2%) 4339(18.0%) 1.17(1.06–1.30)† 1.13(1.02–1.26)† 1.08(0.97–1.22)p = 0.142
Zolpidem 487(8.1%) 1755(7.3%) 1.27(1.09–1.48)† 1.23(1.06–1.44)† 1.13(0.96–1.34)p = 0.136
OR, odds ratio: CI, 95% confidence interval.
*Adjusted for the use of antidepressant, antipsychotics and diuretics.
**Adjusted for hypertension, osteoarthritis, osteoporosis, rheumatoid arthritis, and depression.
†p< 0.05 means “indicates significance for the comparison between patients who were and were not using drugs”.
Several previous studies focused on the impact of hypnotics use on the risk of hip fractures
[
20
,
21
,
45
] or nonvertebral fractures [
17
]. One previous study found that in elderly users of
hypnotics, most fractures occurred in the femur [
19
]. The present study examined a range of
potential fracture sites including hips, humerus, forearms, wrists, and spine. Similar to other
studies, the crude ORs and ORs adjusted for medication use showed a particularly heightened
Table 3. Risk of fractures due to the use of hypnotics in elderly patients stratified by age group and gender.
Benzodiazepin Zolpidem
Characteristics n n (%) Crude OR(95%CI) Adjusted OR(95%CI) n (%) Crude OR(95%CI) Adjusted OR(95%CI) Age 65–74 12210 2061 (33.1%) 1.36(1.24–1.49)‡ 1.11(0.93–1.33) p = 0.238 788(12.6%) 1.27(1.08–1.48)† 1.16(0.89–1.52) p = 0.274 75–84 14045 2769 (39.3%) 1.27(1.14–1.43)‡ 1.08(0.92–1.26) p = 0.374 1177 (16.7%) 1.44(1.20–1.73)† 1.16(0.92–1.45) p = 0.227 > = 85 3795 664(18.3%) 1.13(0.90–1.41) p = 0.29 1.05(0.77–1.44) p = 0.747 277(7.3%) 1.32(0.91–1.93) p = 0.148 0.98(0.61–1.58) p = 0.919 Gender Female 20355 3760 (18.5%) 1.30(1.20–1.41)‡ 1.07(0.94–1.23) p = 0.320 1488(7.3%) 1.31(1.14–1.50)‡ 1.18(0.96–1.45) p = 0.108 Male 9695 1734 (17.9%) 1.32(1.17–1.49)‡ 1.12(0.92–1.37) p = 0.249 754(7.8%) 1.41(1.15–1.73)† 1.05(0.79–1.39) p = 0.793 Hypertension Yes 17668 3582 (20.3%) 1.17(0.98–1.27) p = 0.092 1.10(0.96–1.26) p = 0.186 1599(9.1%) 1.26(1.05–1.51)† 1.17(0.96–1.41) p = 0.121 No 17382 1912 (15.4%) 1.05(0.94–1.18) p = 0.385 1.07(0.88–1.30) p = 0.503 643(5.2%) 1.17(0.87–1.56) p = 0.305 1.05(0.76–1.45) p = 0.755 Osteoarthritis Yes 14225 2792 (19.1%) 1.19(1.03–1.37)† 1.13(0.97–1.32) p = 0.114 1104(7.7%) 1.13(0.91–1.40) p = 0.270 1.06(0.85–1.33) p = 0.603 No 15795 2765 (17.5%) 1.11(0.95–1.30) p = 0.198 1.04(0.88–1.22) p = 0.647 1138(7.2%) 1.36(1.08–1.71)† 1.23(0.96–1.57) p = 0.101 Osteoporosis Yes 3701 815(22.0%) 1.00(0.76–1.32) p = 0.985 0.94(0.71–1.25) p = 0.683 1926(7.3%) 0.95(0.62–1.45) p = 0.817 0.96(0.62–1.48) p = 0.842 No 26349 4679 (17.8%) 1.17(1.05–1.31)† 1.12(0.99–1.26) p = 0.077 316(8.5%) 1.28(1.08–1.52)† 1.17(0.98–1.40) p = 0.089 Rheumatoid arthritis Yes 736 181(24.6%) 1.54(0.87–2.75) p = 0.141 1.94(1.03–3.63)† 62(8.4%) 0.89(0.36–2.18) p = 0.792 0.76(0.29–1.99) p = 0.571 No 29314 5313 (18.1%) 1.15(1.04–1.28)† 1.07(0.95–1.19) p = 0.265 2180(7.4%) 1.28(1.10–1.49)† 1.15(0.97–1.36) p = 0.106 Depression Yes 2584 1101 (42.6%) 0.76(0.58–0.97)† 0.75(0.56–0.99)† 533(20.6%) 0.86(0.60–1.23) p = 0.397 0.87(0.59–1.28) p = 0.478 No 27466 4393 (16.0%) 1.23(1.10–1.37)‡ 1.17(1.03–1.31)† 1709(6.2%) 1.36(1.14–1.61)‡ 1.21(1.00–1.45)† OR, odds ratio; CI, confidence interval.
Adjusted for hypertension, osteoarthritis, osteoporosis, rheumatoid arthritis and depression except for the variable of own strata.
†p< 0.05 means “indicates significance for the comparison between patients who were and were not using drugs”. ‡p< 0.001 means “indicates significance for the comparison between patients who were and were not using drugs”.
risk of fractures in the hip and spine. For hip fractures, zolpidem was associated with increased
fracture risk even after adjusting for other medication use. For spine fractures, both zolpidem
and BDZ were associated with increased risk after adjustment. However, after adjusting for
Table 4. Risk of fractures from subgroup of benzodiazepines use in elderly insomnia patients.
Variable Crude Adjusted Adjusted
OR(95%CI) OR*(95%CI) OR**(95%CI)
Benzodiazepines 1.17(1.06–1.30)† 1.14(1.03–1.27)† 1.09(0.97–1.22) Alprazolam 1.08(0.89–1.31) 1.05(0.86–1.28) 1.01(0.82–1.25) Bromazepam 1.08(0.75–1.54) 1.04(0.73–1.49) 1.00(0.68–1.47) Diazepam 1.82(1.32–2.50)‡ 1.80(1.31–2.48)‡ 1.49(1.05–2.11)† Estazolam 1.27(1.00–1.62)† 1.23(0.96–1.56) 1.28(0.98–1.67) Fludiazepam 1.04(0.80–1.33) 1.02(0.79–1.32) 1.04(0.79–1.39) Flunitrazepam 1.00(0.59–1.70) 0.95(0.56–1.63) 1.03(0.58–1.81) Lorazepam 0.88(0.72–1.06) 1.11(0.92–1.35) 1.05(0.86–1.28) Midazolam 1.26(0.57–2.77) 1.20(0.54–2.64) 1.01(0.42–2.45) Other BDZ 1.22(1.01–1.49)† 1.17(0.97–1.43) 1.07(0.86–1.32)
*Adjusted for the use of antidepressants, antipsychotics and diuretics.
**Adjusted for the presence of hypertension, osteoarthritis, osteoporosis, rheumatoid arthritis, and depression.
†p< 0.05 means “indicates significance for the comparison between patients who were and were not using drugs”. ‡p< 0.001 means “indicates significance for the comparison between patients who were and were not using drugs”.
doi:10.1371/journal.pone.0146030.t004
Table 5. Risk of different fractures at different locations due to the use of hypnotics in elderly insomnia patients.
Variable Crude Adjusted Adjusted
OR(95%CI) OR*(95%CI) OR**(95%CI)
HIP Benzodiazepines 1.10(0.85–1.42) 1.06(0.81–1.40) 0.99(0.75–1.30) Zolpidem 1.53(1.04–2.25)† 1.49(1.00–2.22)† 1.25(0.83–1.87) Humerus Benzodiazepines 1.47(0.95–2.27) 1.37(0.87–2.16) 1.43(0.90–2.29) Zolpidem 1.28(0.67–2.44) 1.18(0.61–2.29) 1.20(0.59–2.44) Forearm Benzodiazepines 1.20(0.88–1.62) 1.19(0.87–1.62) 1.19(0.87–1.65) Zolpidem 1.09(0.70–1.70) 1.08(0.69–1.70) 1.05(0.66–1.69) Wrist Benzodiazepines 1.61(0.51–5.05) 1.49(0.44–5.03) 1.64(0.53–5.12) Zolpidem 2.00(0.18–22.05) 2.00(0.18–22.05) 4.00(0.25–63.92) Spine Benzodiazepines 1.22(1.03–1.44)† 1.20(1.01–1.43)† 1.11(0.92–1.33) Zolpidem 1.38(1.07–1.78)† 1.36(1.05–1.76)† 1.23(0.85–1.49) Other Benzodiazepines 1.08(0.90–1.29) 1.14(1.03–1.27)† 1.09(0.97–1.22) Zolpidem 1.13(0.87–2.46) 1.25(1.07–1.45)† 1.13(0.96–1.34)
*Adjusted for the use of antidepressants, antipsychotics and diuretics
**Adjusted for the presence of hypertension, osteoarthritis, osteoporosis, rheumatoid arthritis, depression.
†p< 0.05 means “indicates significance for the comparison between patients who were and were not using drugs”.
comorbidities, neither zolpidem nor BDZ was found to be associated with significantly
increased risk of fractures in any particular sites. In addition, hypnotics were not found to be
associated with increased risk of all-site fractures.
We also compared use of several of the BDZs most frequently prescribed to elderly people
including alprazolam, bromazepam, diazepam, estazolam, fludiazepam, flunitrazepam,
loraze-pam and midazolam [
17
,
46
,
47
]. We found that only diazepam shows a higher OR with
increased risk of fractures at 1.49 (CI = 1.05
–2.11, p < 0.05). A possible explanation for this
ele-vated fracture risk is that the elimination half-life of diazepam is prolonged in the elderly [
48
],
suggesting that long half-life BDZs such as diazepam should not be prescribed to elderly
patients. Other BDZs are not associate with increased of fractures after adjusting for
medica-tion use or comorbidities.
Previous studies found that depression is a risk factor associated with fractures in elderly
individuals with osteoporosis [
49
,
50
]. However, the present study found that depression
actu-ally reduces fracture risk. In our stratified analysis data, in both the BDZ and zolpidem groups,
patients without depression had a higher OR than those with depression. One possible
expla-nation for this paradoxical finding is that patients with depression are less active due to
psycho-motor retardation and lower energy levels [
51
], thus reducing the risk of fall-related fractures.
However, further study might be necessary to clarify the association between depression and
fracture risk.
Sleep disorders have been found to increase the risk of depression [
52
,
53
], suicidal thoughts
and behaviors [
54
,
55
], mental symptoms in female violence victims [
56
], cancers [
57
], poor
cardiorespiratory fitness [
58
], and increased inflammatory responses to acute emotional or
cognitive stress [
59
]. One recent study even found that persistent insomnia may increase the
risk of mortality [
60
]. Several studies have found that insomnia itself is an independent risk
fac-tor for falls and fractures among the elderly [
61
–
64
]. Therefore, a careful balance between
zol-pidem and other hypnotics is important to maintain both the mental and physical health of
elderly patients with sleep disorders.
Limitations
Patients with missing data in the LHID 2005 dataset were excluded from consideration,
which could introduce minor biases in the analysis. Additionally, this study used claimed
data, and we could not observe clinical events such as the extent of symptom, recovery time,
actual BDZ and zolpidem dosages or side effects. In addition, before 2000 NHIRD data
were coded using A-codes, which cannot be analyzed. For the ICD codes in diagnoses, there
must be some individual differences, however, as aforementioned studies have shown, the
NHIRD is accurate in diagnoses. Despite these limitations, the LHID provides large samples
and sufficient information about disease diagnoses and drug usage, and LHID data have
been used for many studies of interactions between drugs and disease or between disease and
disease.
Conclusion
This case cross-over study revealed that zolpidem or BDZ use is not associated with increased
risk of all-site fractures in elderly, but that diazepam use is associated with elevated fracture
risk. Increased fracture risk among patients without depression requires further investigation.
Hip and spine fractures were a particular concern for elderly users of zolpidem or BDZ
hyp-notics, although the association was found not to be significant after adjusting for
Author Contributions
Conceived and designed the experiments: YJT SYH HLH. Performed the experiments: FYC
HAC YJY. Analyzed the data: HCL WCCC HWY WSC. Contributed
reagents/materials/analy-sis tools: FYC HAC YJY CLY. Wrote the paper: YJT SYH HLH NST.
References
1. Wang CB, Lin CF, Liang WM, Cheng CF, Chang YJ, Wu HC, et al. Excess mortality after hip fracture among the elderly in Taiwan: a nationwide population-based cohort study. Bone. 2013; 56(1):147–53. Epub 2013/06/04. doi:10.1016/j.bone.2013.05.015PMID:23727435.
2. Ziade N, Jougla E, Coste J. Using vital statistics to estimate the population-level impact of osteoporotic fractures on mortality based on death certificates, with an application to France (2000–2004). BMC pub-lic health. 2009; 9:344. Epub 2009/09/19. doi:10.1186/1471-2458-9-344PMID:19761614; PubMed Central PMCID: PMCPmc2758869.
3. Chen IJ, Chiang CY, Li YH, Chang CH, Hu CC, Chen DW, et al. Nationwide cohort study of hip frac-tures: time trends in the incidence rates and projections up to 2035. Osteoporosis international: a jour-nal established as result of cooperation between the European Foundation for Osteoporosis and the National Osteoporosis Foundation of the USA. 2015; 26(2):681–8. Epub 2014/10/31. doi:10.1007/ s00198-014-2930-zPMID:25354653.
4. Adams AL, Shi J, Takayanagi M, Dell RM, Funahashi TT, Jacobsen SJ. Ten-year hip fracture incidence rate trends in a large California population, 1997–2006. Osteoporosis international: a journal estab-lished as result of cooperation between the European Foundation for Osteoporosis and the National Osteoporosis Foundation of the USA. 2013; 24(1):373–6. Epub 2012/02/22. doi: 10.1007/s00198-012-1938-5PMID:22349963.
5. Burge R, Dawson-Hughes B, Solomon DH, Wong JB, King A, Tosteson A. Incidence and economic burden of osteoporosis-related fractures in the United States, 2005–2025. Journal of bone and mineral research: the official journal of the American Society for Bone and Mineral Research. 2007; 22(3):465– 75. Epub 2006/12/06. doi:10.1359/jbmr.061113PMID:17144789.
6. Pike C, Birnbaum HG, Schiller M, Swallow E, Burge RT, Edgell ET. Economic burden of privately insured non-vertebral fracture patients with osteoporosis over a 2-year period in the US. Osteoporosis international: a journal established as result of cooperation between the European Foundation for Oste-oporosis and the National OsteOste-oporosis Foundation of the USA. 2011; 22(1):47–56. Epub 2010/05/22. doi:10.1007/s00198-010-1267-5PMID:20490782.
7. Yang S, Nguyen ND, Center JR, Eisman JA, Nguyen TV. Association between hypertension and fragil-ity fracture: a longitudinal study. Osteoporosis international: a journal established as result of coopera-tion between the European Foundacoopera-tion for Osteoporosis and the Nacoopera-tional Osteoporosis Foundacoopera-tion of the USA. 2014; 25(1):97–103. Epub 2013/07/31. doi:10.1007/s00198-013-2457-8PMID:23892585. 8. Castano-Betancourt MC, Rivadeneira F, Bierma-Zeinstra S, Kerkhof HJ, Hofman A, Uitterlinden AG, et al. Bone parameters across different types of hip osteoarthritis and their relationship to osteoporotic fracture risk. Arthritis and rheumatism. 2013; 65(3):693–700. Epub 2012/12/04. doi:10.1002/art.37792
PMID:23203458.
9. Gale CR, Dennison EM, Edwards M, Sayer AA, Cooper C. Symptoms of anxiety or depression and risk of fracture in older people: the Hertfordshire Cohort Study. Archives of osteoporosis. 2012; 7:59–65. Epub 2012/12/12. doi:10.1007/s11657-012-0080-5PMID:23225282; PubMed Central PMCID: PMCPmc3736098.
10. Harboun M, Dorenlot P, Cohen N, Steinhagen-Thiessen E, Ankri J. Impact of hip fracture, heart failure and weight loss on the risk of institutionalization of community-dwelling patients with dementia. Interna-tional journal of geriatric psychiatry. 2008; 23(12):1245–52. Epub 2008/05/30. doi:10.1002/gps.2058
PMID:18508392.
11. Johnston SS, Conner C, Aagren M, Ruiz K, Bouchard J. Association between hypoglycaemic events and fall-related fractures in Medicare-covered patients with type 2 diabetes. Diabetes, obesity & metab-olism. 2012; 14(7):634–43. Epub 2012/02/18. doi:10.1111/j.1463-1326.2012.01583.xPMID:
22335246.
12. Khazai NB, Beck GR Jr., Umpierrez GE. Diabetes and fractures: an overshadowed association. Cur-rent opinion in endocrinology, diabetes, and obesity. 2009; 16(6):435–45. Epub 2009/09/26. doi:10. 1097/MED.0b013e328331c7ebPMID:19779334; PubMed Central PMCID: PMCPmc3746497. 13. Yang NP, Deng CY, Lee YH, Lin CH, Kao CH, Chou P. The incidence and characterisation of
hospital-ised acute spinal trauma in Taiwan—a population-based study. Injury. 2008; 39(4):443–50. Epub 2008/ 03/07. doi:10.1016/j.injury.2007.12.007PMID:18321510.
14. Melton LJ 3rd, Sampson JM, Morrey BF, Ilstrup DM. Epidemiologic features of pelvic fractures. Clinical orthopaedics and related research. 1981;(155: ):43–7. Epub 1981/03/01. PMID:7226629.
15. Fang JF, Shih LY, Lin BC, Hsu YP. Pelvic fractures due to falls from a height in people with mental dis-orders. Injury. 2008; 39(8):881–8. Epub 2008/07/12. doi:10.1016/j.injury.2008.03.012PMID:
18617168.
16. Cummings-Vaughn LA, Gammack JK. Falls, osteoporosis, and hip fractures. The Medical clinics of North America. 2011; 95(3):495–506, x. Epub 2011/05/10. doi:10.1016/j.mcna.2011.03.003PMID:
21549874.
17. Finkle WD, Der JS, Greenland S, Adams JL, Ridgeway G, Blaschke T, et al. Risk of fractures requiring hospitalization after an initial prescription for zolpidem, alprazolam, lorazepam, or diazepam in older adults. Journal of the American Geriatrics Society. 2011; 59(10):1883–90. Epub 2011/11/19. doi:10. 1111/j.1532-5415.2011.03591.xPMID:22091502.
18. Wang PS, Bohn RL, Glynn RJ, Mogun H, Avorn J. Zolpidem use and hip fractures in older people. Jour-nal of the American Geriatrics Society. 2001; 49(12):1685–90. Epub 2002/02/15. PMID:11844004. 19. Kang DY, Park S, Rhee CW, Kim YJ, Choi NK, Lee J, et al. Zolpidem use and risk of fracture in elderly
insomnia patients. Journal of preventive medicine and public health = Yebang Uihakhoe chi. 2012; 45 (4):219–26. Epub 2012/08/11. doi:10.3961/jpmph.2012.45.4.219PMID:22880153; PubMed Central PMCID: PMCPmc3412984.
20. Bakken MS, Engeland A, Engesaeter LB, Ranhoff AH, Hunskaar S, Ruths S. Risk of hip fracture among older people using anxiolytic and hypnotic drugs: a nationwide prospective cohort study. Euro-pean journal of clinical pharmacology. 2014; 70(7):873–80. Epub 2014/05/09. doi: 10.1007/s00228-014-1684-zPMID:24810612; PubMed Central PMCID: PMCPmc4053597.
21. Berry SD, Lee Y, Cai S, Dore DD. Nonbenzodiazepine sleep medication use and hip fractures in nurs-ing home residents. JAMA internal medicine. 2013; 173(9):754–61. Epub 2013/03/06. doi:10.1001/ jamainternmed.2013.3795PMID:23460413; PubMed Central PMCID: PMCPmc3676706.
22. Wang PS, Bohn RL, Glynn RJ, Mogun H, Avorn J. Hazardous benzodiazepine regimens in the elderly: effects of half-life, dosage, and duration on risk of hip fracture. The American journal of psychiatry. 2001; 158(6):892–8. Epub 2001/06/01. PMID:11384896.
23. Wagner AK, Zhang F, Soumerai SB, Walker AM, Gurwitz JH, Glynn RJ, et al. Benzodiazepine use and hip fractures in the elderly: who is at greatest risk? Archives of internal medicine. 2004; 164(14):1567– 72. Epub 2004/07/28. doi:10.1001/archinte.164.14.1567PMID:15277291.
24. Chen LF, Lin CE, Chou YC, Mao WC, Chen YC, Tzeng NS. A comparison of complex sleep behaviors with two short-acting Z-hypnosedative drugs in nonpsychotic patients. Neuropsychiatric disease and treatment. 2013; 9:1159–62. Epub 2013/08/27. doi:10.2147/ndt.s48152PMID:23976857; PubMed Central PMCID: PMCPmc3747020.
25. Dolder CR, Nelson MH. Hypnosedative-induced complex behaviours: incidence, mechanisms and management. CNS drugs. 2008; 22(12):1021–36. Epub 2008/11/13. doi: 10.2165/0023210-200822120-00005PMID:18998740.
26. Hwang TJ, Ni HC, Chen HC, Lin YT, Liao SC. Risk predictors for hypnosedative-related complex sleep behaviors: a retrospective, cross-sectional pilot study. The Journal of clinical psychiatry. 2010; 71 (10):1331–5. Epub 2010/05/06. doi:10.4088/JCP.09m05083broPMID:20441722.
27. Poceta JS. Zolpidem ingestion, automatisms, and sleep driving: a clinical and legal case series. Journal of clinical sleep medicine: JCSM: official publication of the American Academy of Sleep Medicine. 2011; 7(6):632–8. Epub 2011/12/16. doi:10.5664/jcsm.1468PMID:22171202; PubMed Central PMCID: PMCPmc3227709.
28. Vermeeren A. Residual effects of hypnotics: epidemiology and clinical implications. CNS drugs. 2004; 18(5):297–328. Epub 2004/04/20. PMID:15089115.
29. Maclure M. The case-crossover design: a method for studying transient effects on the risk of acute events. American journal of epidemiology. 1991; 133(2):144–53. Epub 1991/01/15. PMID:1985444. 30. Maclure M, Mittleman MA. Should we use a case-crossover design? Annual review of public health.
2000; 21:193–221. Epub 2000/07/08. doi:10.1146/annurev.publhealth.21.1.193PMID:10884952. 31. Ho Chan WS. Taiwan's healthcare report 2010. The EPMA journal. 2010; 1(4):563–85. Epub 2010/12/
01. doi:10.1007/s13167-010-0056-8PMID:23199110; PubMed Central PMCID: PMCPmc3405348. 32. Chinese Hospital Association: ICD-9-CM English-Chinese Dictionary. Taipei, Taiwan: Chinese
Hospi-tal Association; 2000.
33. Bureau of National Health Insurance Regulations. Available:http://www.nhi.gov.tw/resource/bulletin/ 421_0890036465-19.doc. Accessed 26 January, 2015.
34. Lin LY, Lee CH, Yu CC, Tsai CT, Lai LP, Hwang JJ, et al. Risk factors and incidence of ischemic stroke in Taiwanese with nonvalvular atrial fibrillation—a nation wide database analysis. Atherosclerosis. 2011; 217(1):292–5. Epub 2011/04/26. doi:10.1016/j.atherosclerosis.2011.03.033PMID:21513938. 35. Chiang YY, Lin HW. Association between psoriasis and chronic obstructive pulmonary disease: a
pop-ulation-based study in Taiwan. Journal of the European Academy of Dermatology and Venereology: JEADV. 2012; 26(1):59–65. Epub 2011/03/11. doi:10.1111/j.1468-3083.2011.04009.xPMID:
21388457.
36. Chung SD, Lin HC. Increased risk of benign prostatic enlargement among patients with liver cirrhosis: a nationwide population-based study. Journal of andrology. 2011; 32(2):159–64. Epub 2010/08/28. doi:
10.2164/jandrol.110.011163PMID:20798385.
37. Lin HY, Lai JI, Lai YC, Lin PC, Chang SC, Tang GJ. Acute renal failure in severe pancreatitis: A popula-tion-based study. Upsala journal of medical sciences. 2011; 116(2):155–9. Epub 2011/01/22. doi:10. 3109/03009734.2010.547636PMID:21250932; PubMed Central PMCID: PMCPmc3078547. 38. Chen HL, Hsiao FY. Domperidone, cytochrome P450 3A4 isoenzyme inhibitors and ventricular
arrhyth-mia: a nationwide case-crossover study. Pharmacoepidemiology and drug safety. 2015; 24(8):841–8. Epub 2015/06/23. doi:10.1002/pds.3814PMID:26098410.
39. U.S. Food and Drug Administration. AMBIEN1(zolpidem tartrate) FULL PRESCRIBING INFORMA-TION. Available:http://www.accessdata.fda.gov/drugsatfda_docs/label/2014/
019908s035,021774s016lbl.pdfAccessed 26 January, 2015.
40. Yang YH, Lai JN, Lee CH, Wang JD, Chen PC. Increased risk of hospitalization related to motor vehicle accidents among people taking zolpidem: a case-crossover study. Journal of epidemiology / Japan Epi-demiological Association. 2011; 21(1):37–43. Epub 2010/10/30. PMID:21030794; PubMed Central PMCID: PMCPmc3899515.
41. Stenbacka M, Jansson B, Leifman A, Romelsjo A. Association between use of sedatives or hypnotics, alcohol consumption, or other risk factors and a single injurious fall or multiple injurious falls: a longitudi-nal general population study. Alcohol (Fayetteville, NY). 2002; 28(1):9–16. Epub 2002/10/16. PMID:
12377356.
42. Zint K, Haefeli WE, Glynn RJ, Mogun H, Avorn J, Sturmer T. Impact of drug interactions, dosage, and duration of therapy on the risk of hip fracture associated with benzodiazepine use in older adults. Phar-macoepidemiology and drug safety. 2010; 19(12):1248–55. Epub 2010/10/12. doi:10.1002/pds.2031
PMID:20931664; PubMed Central PMCID: PMCPmc4018736.
43. Glass J, Lanctot KL, Herrmann N, Sproule BA, Busto UE. Sedative hypnotics in older people with insomnia: meta-analysis of risks and benefits. BMJ (Clinical research ed). 2005; 331(7526):1169. Epub 2005/11/15. doi:10.1136/bmj.38623.768588.47PMID:16284208; PubMed Central PMCID:
PMCPmc1285093.
44. Antai-Otong D. The art of prescribing. Risks and benefits of non-benzodiazepine receptor agonists in the treatment of acute primary insomnia in older adults. Perspectives in psychiatric care. 2006; 42 (3):196–200. Epub 2006/08/19. doi:10.1111/j.1744-6163.2006.00070.xPMID:16916422. 45. Chang CM, Wu EC, Chang IS, Lin KM. Benzodiazepine and risk of hip fractures in older people: a
nested case-control study in Taiwan. The American journal of geriatric psychiatry: official journal of the American Association for Geriatric Psychiatry. 2008; 16(8):686–92. Epub 2008/08/02. doi:10.1097/ JGP.0b013e31817c6a99PMID:18669947.
46. Huang WF, Lai IC. Patterns of sleep-related medications prescribed to elderly outpatients with insom-nia in Taiwan. Drugs & aging. 2005; 22(11):957–65. Epub 2005/12/06. PMID:16323972.
47. Khawaja MR, Majeed A, Malik F, Merchant KA, Maqsood M, Malik R, et al. Prescription pattern of ben-zodiazepines for inpatients at a tertiary care university hospital in Pakistan. JPMA The Journal of the Pakistan Medical Association. 2005; 55(6):259–63. Epub 2005/07/28. PMID:16045100.
48. Mandelli M, Tognoni G, Garattini S. Clinical pharmacokinetics of diazepam. Clinical pharmacokinetics. 1978; 3(1):72–91. Epub 1978/01/01. PMID:346285.
49. Cizza G, Primma S, Csako G. Depression as a risk factor for osteoporosis. Trends in endocrinology and metabolism: TEM. 2009; 20(8):367–73. Epub 2009/09/15. doi:10.1016/j.tem.2009.05.003PMID:
19747841; PubMed Central PMCID: PMCPmc2764354.
50. Cizza G. Major depressive disorder is a risk factor for low bone mass, central obesity, and other medical conditions. Dialogues in clinical neuroscience. 2011; 13(1):73–87. Epub 2011/04/14. PMID:21485748; PubMed Central PMCID: PMCPmc3181971.
51. Lecrubier Y. Physical components of depression and psychomotor retardation. The Journal of clinical psychiatry. 2006; 67 Suppl 6:23–6. Epub 2006/07/20. PMID:16848673.
52. Baglioni C, Battagliese G, Feige B, Spiegelhalder K, Nissen C, Voderholzer U, et al. Insomnia as a pre-dictor of depression: a meta-analytic evaluation of longitudinal epidemiological studies. Journal of
affective disorders. 2011; 135(1–3):10–9. Epub 2011/02/09. doi:10.1016/j.jad.2011.01.011PMID:
21300408.
53. Jaussent I, Bouyer J, Ancelin ML, Akbaraly T, Peres K, Ritchie K, et al. Insomnia and daytime sleepi-ness are risk factors for depressive symptoms in the elderly. Sleep. 2011; 34(8):1103–10. Epub 2011/ 08/02. doi:10.5665/sleep.1170PMID:21804672; PubMed Central PMCID: PMCPmc3138165. 54. Pigeon WR, Pinquart M, Conner K. Meta-analysis of sleep disturbance and suicidal thoughts and
behaviors. The Journal of clinical psychiatry. 2012; 73(9):e1160–7. Epub 2012/10/13. doi:10.4088/ JCP.11r07586PMID:23059158.
55. Susanszky E, Hajnal A, Kopp M. [Sleep disturbances and nightmares as risk factors for suicidal behav-ior among men and women]. Psychiatria Hungarica: A Magyar Pszichiatriai Tarsasag tudomanyos folyoirata. 2011; 26(4):250–7. Epub 2011/11/08. PMID:22058257.
56. Pigeon WR, Cerulli C, Richards H, He H, Perlis M, Caine E. Sleep disturbances and their association with mental health among women exposed to intimate partner violence. Journal of women's health (2002). 2011; 20(12):1923–9. Epub 2011/10/13. doi:10.1089/jwh.2011.2781PMID:21988551; PubMed Central PMCID: PMCPmc3236986.
57. Lehrer S, Green S, Ramanathan L, Rosenzweig KE. Obesity and deranged sleep are independently associated with increased cancer mortality in 50 US states and the District of Columbia. Sleep & breath-ing = Schlaf & Atmung. 2013; 17(3):1117–8. Epub 2013/02/08. doi:10.1007/s11325-013-0811-xPMID:
23389836.
58. Strand LB, Laugsand LE, Wisloff U, Nes BM, Vatten L, Janszky I. Insomnia symptoms and cardiorespi-ratory fitness in healthy individuals: the Nord-Trondelag Health Study (HUNT). Sleep. 2013; 36(1):99– 108. Epub 2013/01/05. doi:10.5665/sleep.2310PMID:23288976; PubMed Central PMCID:
PMCPmc3524509.
59. Heffner KL, Ng HM, Suhr JA, France CR, Marshall GD, Pigeon WR, et al. Sleep disturbance and older adults' inflammatory responses to acute stress. The American journal of geriatric psychiatry: official journal of the American Association for Geriatric Psychiatry. 2012; 20(9):744–52. Epub 2012/02/14. doi:10.1097/JGP.0b013e31824361dePMID:22327621; PubMed Central PMCID: PMCPmc3588882. 60. Parthasarathy S, Vasquez MM, Halonen M, Bootzin R, Quan SF, Martinez FD, et al. Persistent
insom-nia is associated with mortality risk. The American journal of medicine. 2015; 128(3):268–75.e2. Epub 2014/12/03. doi:10.1016/j.amjmed.2014.10.015PMID:25447616; PubMed Central PMCID: PMCPmc4340773.
61. Stone KL, Ewing SK, Lui LY, Ensrud KE, Ancoli-Israel S, Bauer DC, et al. Self-reported sleep and nap habits and risk of falls and fractures in older women: the study of osteoporotic fractures. Journal of the American Geriatrics Society. 2006; 54(8):1177–83. Epub 2006/08/18. doi:10.1111/j.1532-5415.2006. 00818.xPMID:16913982.
62. Stone KL, Ensrud KE, Ancoli-Israel S. Sleep, insomnia and falls in elderly patients. Sleep medicine. 2008; 9 Suppl 1:S18–22. Epub 2008/12/17. doi:10.1016/s1389-9457(08)70012-1PMID:18929314. 63. Latimer Hill E, Cumming RG, Lewis R, Carrington S, Le Couteur DG. Sleep disturbances and falls in
older people. The journals of gerontology Series A, Biological sciences and medical sciences. 2007; 62 (1):62–6. Epub 2007/02/16. PMID:17301039.
64. Brassington GS, King AC, Bliwise DL. Sleep problems as a risk factor for falls in a sample of commu-nity-dwelling adults aged 64–99 years. Journal of the American Geriatrics Society. 2000; 48(10):1234– 40. Epub 2000/10/19. PMID:11037010.