PLEASE SCROLL DOWN FOR ARTICLE
This article was downloaded by: On: 26 March 2009
Access details: Access Details: Free Access Publisher Informa Healthcare
Informa Ltd Registered in England and Wales Registered Number: 1072954 Registered office: Mortimer House, 37-41 Mortimer Street, London W1T 3JH, UK
Prosthetics and Orthotics International
Publication details, including instructions for authors and subscription information:
http://www.informaworld.com/smpp/title~content=t714595820
Rates and characteristics of lower limb amputations in Taiwan, 1997
S. Y. Chen a; W. C. Chie b; C. Lan a; M. C. Lin a; J. S. Lai a; I. N. Lien a
a Department of Physical Medicine and Rehabilitation, National Taiwan University Hospital, Taipei, Taiwan b
School of Public Health, College of Public Health, National Taiwan University, Taipei, Taiwan Online Publication Date: 01 April 2002
To cite this Article Chen, S. Y., Chie, W. C., Lan, C., Lin, M. C., Lai, J. S. and Lien, I. N.(2002)'Rates and characteristics of lower limb amputations in Taiwan, 1997',Prosthetics and Orthotics International,26:1,7 — 14
To link to this Article: DOI: 10.1080/03093640208726616 URL: http://dx.doi.org/10.1080/03093640208726616
Full terms and conditions of use: http://www.informaworld.com/terms-and-conditions-of-access.pdf This article may be used for research, teaching and private study purposes. Any substantial or systematic reproduction, re-distribution, re-selling, loan or sub-licensing, systematic supply or distribution in any form to anyone is expressly forbidden.
The publisher does not give any warranty express or implied or make any representation that the contents will be complete or accurate or up to date. The accuracy of any instructions, formulae and drug doses should be independently verified with primary sources. The publisher shall not be liable for any loss, actions, claims, proceedings, demand or costs or damages whatsoever or howsoever caused arising directly or indirectly in connection with or arising out of the use of this material.
Prosthetics and Orthotics International, 2002, 26, 7-14
Rates and characteristics of lower limb
amputations in Taiwan, 1997
S. Y. CHEN*, W. C. CHIE**, C. LAN*, M. C. LIN*, J. S. LAI* and I. N. LIEN* *Department of Physical Medicine and Rehabilitation, National Taiwan University Hospital, Taipei, Taiwan
**School of Public Health, College of Public Health, National Taiwan University, Taipei, Taiwan
Abstract
This study aims to describe the national incidence rate and characteristics of lower limb amputations (LLA) in 1997 from an island-wide database of the national health insurance programme in Taiwan. Some 117,647 discharge records from a sampled database (1 in 20) of the National Health Insurance Research Database were analysed. This study included records (n=171) containing LLA procedures. The LLA procedure rates were obtained by multiplying the number of identified procedures by 20 as the numerator and mid-year total population of Taiwan in 1997 as the denominator. Each procedure was further analysed according to the demographic characteristics of the patients, cause and level of amputation. Summarised gender ratios of LLA procedure rates were obtained by Poisson regression analysis. The crude LLA procedure rate was 18.1 per 100,000 population per year and the crude major LLA procedure rate was 8.8 per 100,000 population per year in Taiwan in 1997. The major cause of LLA procedures was peripheral vascular disease (72%), and the toe was most frequently amputated (48%). The LLA procedure rates, which increased logarithmically with age of patients, were significantly higher in men with a summarised male to female rate ratio of 1.65. The age-standardised LLA procedure rate in Taiwan was lower than that reported in the United States, Finland, the Netherlands, the United Kingdom (Leeds, Middlesborough, and
All correspondence to be addressed to Ssu-Yuan Chen MD, Department of Physical Medicine and Rehabilitation, National Taiwan University Hospital, 7 Chung-Shan South Road, Taipei, Taiwan 10016. E-mail: ssuyuan@ha.mc.ntu.edu.tw
Newcastle), but higher than Spain, Italy, and Japan. The trend of an increasing proportion of PVD-related LLA procedures will prompt the health professionals to develop strategies for LLA prevention.
Introduction
Lower limb amputation (LLA), especially major LLA, is a permanent disabling condition that may restrict mobility, the activities of daily living and employment. Peripheral vascular disease (PVD) with or without diabetes is the major cause of LLA in Western countries. (Anonymous, 1998; Hierton and James, 1973; Laaperi et al, 1993; Liedberg and Persson, 1983; The Global Lower Extremity Amputation Study Group, 2000; van Houtum et al, 1996) The association of diabetes with LLA may be attributable to the combined effects of microangiopathy, peripheral neuropathy, and personal factors. Over the 20-year duration of the National Health and Nutritional Examination Survey I Follow-up Study (Resnick et al, 1999) the relative risk of LLA in people with prevalent diabetes was 7.19 after adjusting for the other independent risk factors. However, trauma is an important cause of LLA in the younger age group (Dillingham and collegues, 1998)
Few epidemiological studies have addressed the incidence of LLA among the Chinese in Taiwan. Lien and colleagues conducted two island-wide surveys of LLA from the surgical records of participating hospitals from 1979 to 1980 and 1986 to 1987. An increasing proportion of PVD-related LLA was observed in the two surveys (Lien, unpublished data, 1990). Recently, the age-adjusted rates of major LLA in Ilan County were reported to be 11.3 individuals
7
S. Y. Chen, W. C. Chie, C. Lan, M. C. Lin, J.S. Lai and I. N. Lien per 100,000 population per year in men, and 8.3
in women, during the study period between July 1995 and June 1997. (The Global Lower Extremity Amputation Study Group, 2000) Han County, in northeastern Taiwan, is surrounded by mountains and faces the Pacific Ocean in the east. However, the LLA incidence in Ilan may not be representative of the rates in Taiwan, since it represents only rural Taiwan and regional variation of LLA incidence may be present (van Houtum and Lavery, 1996).
Taiwan launched the national health insurance programme in 1995, to cover the entire civilian population of 21 million (Cheng and Chiang, 1997). The Bureau of National Health Insurance (BNHI) managed all claimed records from more than 8,000 contracted hospitals and clinics across the island (Bureau of National Health Insurance, 2000) The high coverage rate (96.1% in 1997) of this insurance programme ensures that the claimed record database in BNHI is representative of the entire population of Taiwan. This study aims to describe the national incidence rate and characteristics of LLA in 1997 according to this national database of Taiwan.
Subject and methods
This study is based on data from the National Health Insurance Research Database (NHIRD) provided by the BNHI and managed by the National Health Research Institutes (NHRI) in Taiwan. The NHIRD contains comprehensive claimed records of outpatient and inpatient care of the 21 million beneficiaries of national health insurance in Taiwan. The NHRI used the method of systematic sampling of the entire database to randomly draw a representative and manageable database from the entire database. The sampling proportion of the inpatient data was 1 in 20. Systematic sampling was then performed for each month to randomly select a representative subset. The sample size for each month was proportional to the amount of data for that month. At the end of 1997, a sampled database was obtained by combining the 12 subsets, one from each month. The size of the sampled database was accordingly 5% of that of the entire database. An NHRI working group validated that this database was representative of the entire database, by comparing the distribution of basic characteristics such as age, gender, and the claimed medical expenditure.
This study employed 117,647 discharge records from the sampled database. Each claimed record contains the birth date and gender of the patient, the primary diagnosis, secondary diagnoses including up to four items, the primary surgical procedure, secondary surgical procedures including up to four items, and up to two items of external cause, according to the codes listed in International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM). The records containing both ICD-9-CM procedure codes 84.10 - 84.19 and the claims for surgical fees were identified and included. The type of LLA procedure was obtained from the ICD-9-CM procedure codes in each record. Major LLA was defined as amputation through the ankle or more proximal levels (ICD9CM codes 84.13 -84.19). The cause of each LLA procedure was determined and further classified into mutually exclusive categories according to the ICD-9-CM disease codes and the E codes. For example, LLA procedures with codes 820-829, 895-897, 905-906.4, 928-929, 959, or E codes were considered to be trauma-related. Procedures with codes 940-949 were classified as burn-related. Procedures with code 250, without the above trauma-related codes, were considered to be diabetes-related. Procedures with codes 440-448 or 785.4, but no concomitant code 250, were viewed as being caused by PVD without diabetes.
Statistical analysis
Analysis was performed using the SAS System for Microsoft Windows (version 6.12, SAS Institute Inc., Cary, NC) statistical software. Fisher's exact test for proportions and the t-test for continuous variables were used for comparison among groups. The number of identified procedures multiplied by 20 (the sampling proportion) was taken as the numerator in the LLA procedure rate. The mid-year total population of Taiwan in 1997 (Ministry of Interior, 1997) was used as the denominator of the LLA procedure rate, for each age- and gender-group. The age-adjusted LLA procedure rates were directly standardised to the world standard population, standard European population, and 1990 US population. (US Bureau of the Census, 1992; World Health Organisation, 1994) The summarised gender ratios of LLA procedure rates were obtained by 8
Lower limb amputations in Taiwan
Table 1. Causes of 196 lower limb amputations in 170 patients.
Vascular Diabetes-related PVDC without diabetes Non-vascular Traumatic Infection without PVD Polydactyly Burn Miscellaneous Unknown LLAa procedures Male (n=125) 84 (67.2) 60 (48.0) 24 (19.2) 41 (32.8) 22 (17.6) 7 (5.6) 3 (2.4) 3 (2.4) 2 (1.6) 4 (3.2) Female (n=71) 58 (81.7)b 49 (69.0)b 9 (12.7) 13 (18.3)b 2 (2.8)b 3 (4.2) 3 (4.2) 1 (1.4) 1 (1.4) 3 (4.2) Total (n=196) 142 (72.4) 109 (55.6) 33 (16.8) 54 (27.6) 24 (12.2) 10(5.1) 6(3.1) 4 (2.0) 3 (1.5) 7 (3.6)
Patients with LLA Male (n=110) 71 (64.6) 51 (46.4) 20(18.2) 39 (35.4) 22 (20.0) 6 (5.4) 3 (2.7) 3 (2.7) 2(1.8) 3 (2.7) Female (n=60) 47 (78.3) 39 (65.0)b 8(13.3) 13 (21.7) 2 (3.3)b 3 (5.0) 3 (5.0) 1 (1.7) 1 (1-7) 3 (5.0) Total (n=170) 118(69.4) 90 (52.9) 28 (16.5) 52 (30.6) 24(14.1) 9 (5.3) 6 (3.5) 4 (2.4) 3 (1.8) 6 (3.5) "Lower limb amputations.
bSignificant difference by Fisher's exact test (P < 0.05). c Peripheral vascular disease.
Poisson regression analysis. A P value of less than 0.05 was considered statistically significant.
Result
A total of 171 claimed discharge records through 1997 satisfied the inclusion criteria of this study. According to these records, a total of 196 LLA procedures were performed in 170 patients (male 110, 64.7%). The mean age of all patients with LLA was 60.7±20.3 (standard deviation) years and men were younger than women (57.9±20.5 vs. 65.8±19.1 years, P< 0.05). Of the 25 patients who received at least two or more LLA procedures, one received three LLA procedures over a 62-day admission period, 23 received two LLA procedures in one admission, and one received two LLA procedures over two different admission periods that were three days apart.
Table 1 lists the causes of 196 LLA procedures in 170 patients. PVD with or without diabetes accounted for the majority of LLA procedures in four-fifths of the females and two-thirds of the males. Diabetes, which contributed to a significantly higher proportion of LLA procedures in women than in men, was the most common cause of LLA procedures in each gender group. Trauma was the third most common cause of LLA procedures in men but it was not important in women.
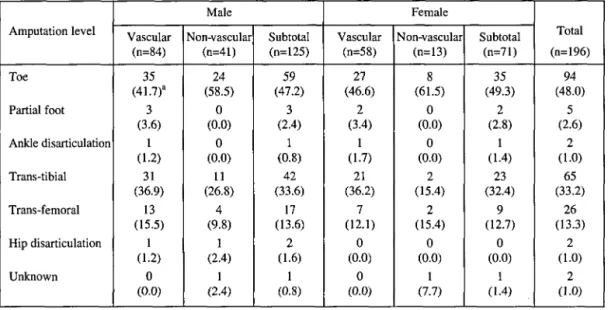
Table 2 lists the amputation level of 196 LLA procedures. Toe amputation was the most common level of LLA. The proportion of toe amputations was higher in LLA procedures performed for non-vascular reasons than for vascular reasons, but the difference was not statistically significant. Of the 95 major LLA procedures, 65 (68.4%) were trans-tibial amputations and 26 (27.4%) were trans-femoral amputations. Gender and the cause of LLA procedure did not affect the amputation level.
Table 3 lists the causes of 95 major LLA procedures in 88 patients. Seven (7) patients received 2 major LLA procedures. PVD, the cause of major LLA procedures in seven-eighths of the women and three-quarters of the men, was the most frequent of all causes. PVD without diabetes accounted for a higher proportion of major LLA procedures in men than in women but not to a statistically significant level. Infection without concurrent PVD was more important than trauma in major LLA procedures. The crude LLA procedure rate was 18.1 per 100,000 population per year and the crude major LLA procedure rate was 8.8 per 100,000 population per year. Table 4 lists the estimates of age-, gender-specific LLA procedure rates and age-adjusted rates to different populations. Using a correction factor obtained from the 196 LLA procedures in 170 patients in this study, it can be estimated that the crude LLA rate at 15.7
9
10 S. Y. Chen, W. C. Chie, C. Lan, M. C. Lin, J.S. Lai and I. N. Lien Table 2. Amputation level of 196 lower limb amputations.
Amputation level Toe Partial foot Ankle disarticulation Trans-tibial Trans-femoral Hip disarticulation Unknown Male Vascular (n=84) 35 (41.7)a 3 (3.6) 1 (1.2) 31 (36.9) 13 (15.5) 1 (1.2) 0 (0.0) Non-vascular (n=41) 24 (58.5) 0 (0.0) 0 (0.0) 11 (26.8) 4 (9.8) 1 (2.4) 1 (2.4) Subtotal (n=125) 59 (47.2) 3 (2.4) 1 (0.8) 42 (33.6) 17 (13.6) 2 (1.6) 1 (0.8) Female Vascular (n=58) 27 (46.6) 2 (3.4) 1 (1.7) 21 (36.2) 7 (12.1) 0 (0.0) 0 (0.0) Non-vascular (n=13) 8 (61.5) 0 (0.0) 0 (0.0) 2 (15.4) 2 (15.4) 0 (0.0) 1 (7.7) Subtotal (n=71) 35 (49.3) 2 (2.8) 1 (1.4) 23 (32.4) 9 (12.7) 0 (0.0) 1 (1.4) Total (n=196) 94 (48.0) 5 (2.6) 2 (1.0) 65 (33.2) 26 (13.3) 2 (1.0) 2 (1.0)
a Percentage of total numbers in column.
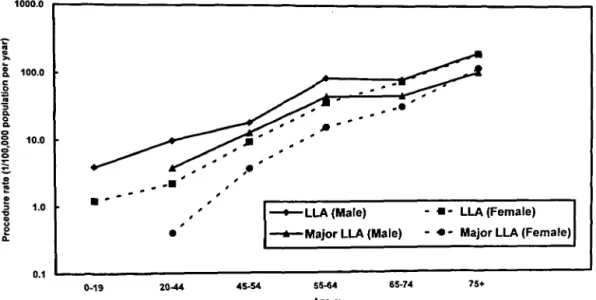
individuals per 100,000 population per year in men, and 7.6 in women. Figure 1 shows that LLA procedure rates increase logarithmically as age increases. Poisson regression analysis demonstrated that LLA procedure rates were significantly higher in men, with a summarised men to women rate ratio of 1.65 (95% confidence interval 1.23-2.21, P<0.001). Similar results were found for major LLA procedures with a summarised gender ratio of 1.76 (95% confidence interval 1.16-2.71, P<0.01). The
gender ratio of LLA procedure rate was higher among younger age groups and approximated 1.0 in the aged population. Furthermore, the major LLA procedure rate of women was higher than men in persons 75 years and older. Discussion
In the past decades, rapid economic development in Taiwan has been accompanied by changing dietary patterns, lifestyles, and blood lipids (Pan and Chiang, 1995) The age-Table 3. Causes of 95 major lower limb amputations in 88 patients.
Vascular Diabetes-related PVDC without diabetes Non-vascular Traumatic Infection without PVD Burn Miscellaneous Unknown
Major LLAa procedures
Male (n=62) 46 (74.2) 33 (53.2) 13 (21.0) 16(25.8) 6 (9.7) 7(11.3) 2 (3.2) 0(0) 1 (1.6) Female (n=33) 29 (87.9) 27(81.8)b 2(6.1) 4(12.1) 0(0) 3(9.1) 0(0) 1 (3.0) 0(0) Total (n=95) 75 (79.0) 60 (63.2) 15(15.8) 20(21.0) 6 (6.3) 10(10.5) 2(2.1) 1 (1.0) 1 (1.0)
Patients with major LLA Male (n=57) 42 (73.7) 30 (52.6) 12(21.0) 15 (26.3) 6(10.5) 6(10.5) 2 (3.5) 0(0) 1 (1.8) Female (n=31) 27 (87.1) 25 (80.6)b 2 (6.4) 4(12.9) 0(0) 3 (9.7) 0(0) 1 (3.2) 0(0) Total (n=88) 69 (78.4) 55 (62.5) 14 (15.9) 19(21.6) 6 (6.8) 9 (10.2) 2 (2.3) 1(1.1) 1(1.1)
a Major LLA: lower limb amputations through the ankle or more proximal levels. b Significant difference by Fisher's exact test (P< 0.05).
c Peripheral vascular disease.
Table 4. Estimates of age-, gender-specific procedure rates of lower limb amputations and gender ratio in Taiwan, 1997. 0-19 y 20-44 y 45-54 y 55-64 y 65-74 y 75+y Crude rate Age-adjusted rate
World standard population Standard European population 1990 US population Major LLA Male 3.9° 9.8 18.2 83.3 78.7 196.0 22.5 18.2 29.1 26.5 Female 1.2 2.2 9.3 35.9 74.0 191.3 13.5 13.0 26.7 24.0 * procedures Total 2.6 6.1 13.8 59.4 76.6 193.7 18.1 15.7 28.1 25.4 Gender ratio (M:F) 3.26 4.42 1.96 2.32 1.06 1.02 1.67 1.40 1.10 1.11 Patients with Male 0.0 3.8 12.8 44.3 45.4 101.6 11.2 8.6 14.8 13.4 Female 0.0 0.4 3.7 15.4 31.2 117.7 6.3 6.1 13.7 12.2 major LLA Total 0.0 2.2 8.3 29.7 39.2 109.6 8.8 7.4 14.3 12.9 Gender ratio (M:F) _ 8.65 3.43 2.87 1.46 0.86 1.78 1.41 1.08 1.09
a LLA: lower limb amputations.
b Major LLA: lower limb amputations through the ankle or more proximal levels. cData is presented as procedure rate per 100,000 population per year.
standardised mortality rate of diabetes increased sharply from 7.38 in 1979 to 21.02 per 100,000 population per year in 1997 (Department of Health, 1998). LLA due to PVD exhibited a similar trend. In the 1979-1980 first island-wide hospital-based survey, PVD accounted for only 27% of the 708 patients with major LLA (Lien, unpublished data, 1990). In this research, PVD with or without diabetes accounted for 78.4% of cases of major LLA. The authors' findings confirm the trend of increasing PVD-related
LLA in Taiwan over the past two decades. The causes of LLA show some gender differences. Diabetes accounts for a significantly higher proportion of LLA in women than men, but trauma accounts for a greater proportion in men. The finding is possibly explained by the fact that men are more prone to traumatic injuries during work and day-to-day activities. These findings are consistent with the report that 83.5% of the 6,069 patients with traumatic amputations were men in Maryland in 1979-1000.0 I 100.0 g 10.0 g"
I
0.1 -LLA (Male) -Major LLA (Male)• - LLA (Female) • - Major LLA (Female)
0-19 20-44 45-54 55-64
Age.y
75+
Fig. 1. Age-, gender-specific procedure rates of lower limb amputations (LLA) in Taiwan. (Note: y-axis is in log scale)
12 S. Y. Chen, W. C. Chie, C. Lan, M. C. Lin, J.S. Lai and I. N. Lien 1993 (Dillingham et al, 1998).
Toe amputation was the most frequent level of LLA procedure. In a population-based study in Tayside, Scotland (Morris et al, 1998) toe amputations accounted for 40% of 258 LLA procedures. In the Netherlands, toe amputations were also the most common in 1,575 LLA procedures among persons with diabetes (van Houtum et al, 1996). However, only 12 (15%) of the total 78 LLA were reported to be minor amputations in Ilan Taiwan (The Global Lower Extremity Amputation Study Group, 2000). The exact reasons for these divergent results are unknown. The previously reported incidence of minor amputation in Ilan may have been underestimated.
The data indicated that the proportion of tibial amputations was higher than that of trans-femoral amputations. Similar findings were reported in studies from Tayside, Scotland and from the Netherlands (Morris et al, 1998; van Houtum et al., 1996). However, the proportion of trans-femoral amputations was higher than that of trans-tibial amputations in reports from Finland and Denmark (Ebskov, 1996; Laaperi
et al, 1993; Siitonen et al, 1993). In the United
States, the reported rate ratio of trans-tibial to trans-femoral amputations is around 1.0 (Dillingham et al, 1998; Feinglass et al, 1999). The reason for these inconsistent findings is unknown and rarely discussed in the literature (van Houtum et al, 1996). Possible explanations might include the racial difference, the prevalence and severity of PVD, availability of medical services and specialists, timing of medical intervention, amputation philosophy, and age demographics of the different study populations.
In this study, the age-standardised incidence of major LLA was higher than that reported in Ilan (The Global Lower Extremity Amputation Study Group, 2000). Methodologically, the incidence rate obtained with the number of LLA procedures as a numerator in the calculation (as in this study) should be equal or higher to that obtained with the number of individuals with LLA as a numerator (as in the Ilan study) for a given population, (van Houtum and Lavery, 1997). Although this methodological problem may explain why the incidence was higher in this study, a possible underestimation of LLA incidence in Ilan study should be considered. Ilan is a rural region and the age-adjusted
prevalence of diabetes was reported to be lower in rural Taiwan (Tai et al, 1987). Accordingly, the incidence of diabetes-related LLA in Ilan might be lower than the average in Taiwan. Residents of Ilan may leave their home and work elsewhere but retain their residency in Ilan, owing to a higher unemployment rate in rural Taiwan. The official residency registry may thus overestimate Han's population, leading to an underestimation of LLA incidence in that region. Furthermore, Ilan County lacks medical resources. Transfer of patients elsewhere to receive LLA might also account for underestimating major LLA incidence.
Previous studies indicated that LLA incidence in the diabetic populations was dominant in men, with a male to female rate ratio range of 1.4 to 5.2 (Moss et al., 1999; Nelson et al, 1988; van Houtum et al, 1996). The authors' findings show a summarised gender ratio of 1.65 for LLA procedures and 1.76 for major LLA procedures. The LLA procedure rate gender ratios were higher in younger age groups than in the aged population. Furthermore, the major LLA procedure rate for women is higher than men among individuals aged 75 years and older. A similar result was reported in Italy for women aged 80 years and over. (The Global Lower Extremity Amputation Study Group, 2000). Further studies are required to clarify this finding.
This study has several limitations. The estimates of LLA incidence are at a procedural level rather than the patient level, and they may include multiple procedures for a single patient (Feinglass et al, 1999; van Houtum et al, 1996). The authors were unable to identify all multiple LLA procedures in an individual because data were obtained from a sampled database. Individual-based estimation was problematic because admissions rather than individuals were sampled. The identification numbers of patients were veiled in this sampled database; therefore, personal data could not be obtained or linked to hospital medical records. Even when multiple LLA procedures were identified in an individual, the exact amputation sites and levels in order remained unknown. Consequently, it was not possible to calculate the exact LLA incidence rate at an individual level because the duplications (same disease, same side, more surgery in the same individual) could not be identified and eliminated in this national
Lower limb amputations in Taiwan 13 database. Furthermore, hospital discharge
records may under-report diabetes (Resnick
et al, 1999) leading to an underestimation of the
proportion of diabetes-related LLA procedures. Finally, the estimates of LLA procedure rate may be underestimated because of the 96.1% coverage rate of the national health insurance programme in Taiwan in 1997.
In summary, the crude LLA procedure rate was 18.1 per 100,000 population per year and the crude major LLA procedure rate was 8.8 per 100,000 population per year in Taiwan in 1997. The age-standardised LLA procedure rates were lower than that reported in the United States, Finland, the Netherlands and the United Kingdom (Leeds, Middlesborough and Newcastle), but higher than Spain, Italy, and Japan (Ebskov, 1996; Feinglass et al, 1999; Laaperi et al, 1993; Siitonen et al, 1993; The Global Lower Extremity Amputation Study Group, 2000; van Houtum et al, 1996). The major cause of LLA procedures was PVD, and toes were most frequently amputated. The LLA procedure rates, which increased logarithmically with age, were significantly higher in men with a summarised male to female rate ratio of 1.65. The increasing proportion of PVD-related LLA in Taiwan should prompt health professionals to develop strategies to prevent LLA. Screening and special protection of PVD among high-risk populations, such as the diabetic or aged population, may help to prevent LLA in the future (Tabet and Berg, 1996).
Acknowledgement
The authors would like to thank the National Health Research Institutes of Taiwan for allowing them to access the National Health Insurance Research Database provided by the Bureau of National Health Insurance, Department of Health, Executive Yuan, Republic of China. The interpretation and conclusions presented herein do not represent those of the Bureau of National Health Insurance, the Department of Health or the National Health Research Institutes.
REFERENCES
ANONYMOUS (1998). Diabetes-related amputations of lower extremities in the Medicare population Minnesota, 1993-1995. MMWR Morb Mortal Wkly Rep 47, 649-652.
BUREAU OF NATIONAL HEALTH INSURANCE (2000). National health insurance annual statistical report, 1999. - Taipei: Bureau of National Health Insurance, Republic of China. pl38-139.
CHENG SH, CHIANG TL (1997). The effect of universal health insurance on health care utilisation in Taiwan: results from a natural experiment. JAMA 278, 89-93. DEPARTMENT OF HEALTH, EXECUTIVE YUAN (1998).
Health statistics, Volume 2. Vital statistics. - Taipei: Department of Health, Executive Yuan, Republic of China.
DILLINGHAM TR, PEZZIN LE, MACKENZIE EJ (1998). Incidence, acute care length of stay, and discharge to rehabilitation of traumatic amputee patients: an epidemiologic study. Arch Phys Med Rehabil 79, 279-287.
EBSKOV LB (1996). Relative mortality in lower limb amputees with diabetes mellitus. Prosthet Orthot Int 20, 147-152.
FEINGLASS J, BROWN JL, LOSASSO A, SOHN MW, MANHEIM LM, SHAH SJ, PEARCE WH (1999). Rates of lower-extremity amputation and arterial reconstruction in the United States, 1979 to 1996. Am J Public Health 89, 1222-1227.
HIERTON T, JAMES U (1973). Lower extremity amputation in Uppsala county 1947-1969: incidence and prosthetic rehabilitation. Acta Orthop Scand 44, 573-582. LAAPERI T, POHIOLAINEN T, ALARANTA H, KARKKAINEN
M (1993). Lower-limb amputations. Ann Chir Gynaecol 82, 183-187.
LIEDBERG E, PERSSON BM (1983). Increased incidence of lower limb amputation for arterial occlusive disease. Acta Orthop Scand 54, 230-234.
MINISTRY OF INTERIOR, EXECUTIVE YUAN (1997). 1997 Taiwan-Fukien Demographic Fact Book, Republic of China. - Taipei: Ministry of Interior, Executive Yuan, Republic of China. p58-59.
MORRIS AD, MCALPINE R, STEINKE D, BOYLE DI, EBRAHIM AR, VASUDEV N, STEWART CP, JUNG RT, LEESE GP, MACDONALD TM, NEWTON RW (1998). Diabetes and lower-limb amputations in the community: a retrospective cohort study. Diabetes Care 21, 738-743.
Moss SE, KLEIN R, KLEIN BE (1999). The 14-year incidence of lower-extremity amputations in a diabetic population: the Wisconsin Epidemiologic Study of Diabetic Retinopathy. Diabetes Care 22, 951-959. NELSON RG, GOHDES DM, EVERHART JE, HARTNER JA,
ZWEMER FL, PETTITT DJ, KNOWLER WC (1988). Lower-extremity amputations in NIDDM: 12-year follow-up study in Pima Indians. Diabetes Care 11, 8-16.
PAN WH, CHIANG BN (1995). Plasma lipid profiles and epidemiology of atherosclerotic diseases in Taiwan -a unique experience. Atherosclerosis 118, 285-295.
14 S. Y. Chen, W. C. Chie, C. Lan, M. C. Lin, J.S. Lai and I. N. Lien RESNICK HE, VALSANIA P, PHILLIPS CL (1999). Diabetes
mellitus and nontraumatic lower extremity amputation in black and white Americans: the National Health and Nutrition Examination Survey Epidemiologic Follow-up Study, 1971-1992. Arch Intern Med 159, 2470-2475.
SIITONEN OI, NISKANEN LK, LAAKSO M, SITTONEN JT, PYORALA K (1993). Lower-extremity amputations in diabetic and nondiabetic patients. A population-based study in eastern Finland. Diabetes Care 16, 16-20. TABET S, BERG AO (1996). Screening for peripheral
arterial disease. In: Guide to clinical preventive service./edited by US Preventive Services Task Force. - Baltimore: Williams & Wilkins. p 63-66.
TAI TY, YANG CL, CHANG CJ, CHANG SM, CHEN YH, LIN
BJ, Ko LS, CHEN MS, CHEN CJ (1987). Epidemiology
of diabetes mellitus in Taiwan, R.O.C.: comparison between urban and rural areas. J Med Assoc Thai
70(Suppl 2), 49-53.
THE GLOBAL LOWER EXTREMITY AMPUTATION STUDY GROUP (2000). Epidemiology of lower extremity amputation in centres in Europe, North America and East Asia. Br J Surg 87, 328-337.
US BUREAU OF THE CENSUS (1992). 1990 Census of
Population: general population characteristics, United States. - Washington, DC: US Bureau of the Census. pl9-20.
VAN HOUTUM WH, LAVERY LA (1996). Regional
variation in the incidence of diabetes-related amputations in the Netherlands. Diabetes Res Clin Pract 31, 125-132.
VAN HOUTUM WH, LAVERY LA (1997). Methodological
issues affect variability in reported incidence of lower extremity amputations due to diabetes. Diabetes Res
Clin Pract 38, 177-183.
VAN HOUTUM WH, LAVERY LA, HARKLESS LB (1996). The impact of diabetes-related lower-extremity amputations in the Netherlands. J Diabetes Complications 10, 325-330.
WORLD HEALTH ORGANIZATION (1994). World Health
Statistics Annual, 1993 - Geneva: WHO. pxxxiv.
Consensus Conference on Poliomyelitis
Consensus Statements and Syndicate Reports
ISPO Consensus Conference, Hammamet, Tunisia16-22 November 1997
Edited by S. Heim, N.A. Jacobs (Chairman), J.S. Jensen, G. Neff, B. Persson Published 2001
Price: ISPO Members US$30 (plus postage and handling US$10) Non-members US$45 (plus postage and handling US$10) Orders, which must be accompanied by the appropriate remittance (cheque or international bank draft made payable to ISPO) should be sent to:
Mrs Aase Larsson ISPO
Borgervaenget 7 2100 Copenhagen 0 DENMARK