中國醫藥大學機構典藏 China Medical University Repository, Taiwan:Item 310903500/23828
6
0
0
全文
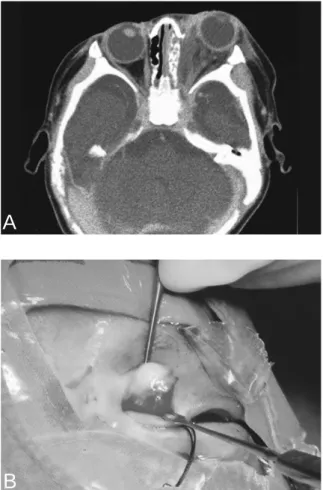
(2) Chun-Hsin Liu, et al.. 145. Table 1. Initial symptoms in 23 children diagnosed as having acute sinusitis with orbital complications. Presenting symptoms Eyelid edema Eyelid erythema Purulent rhinorrhea Fever Chemosis Proptosis Limited ocular motility. Fig. 1. A 3-year-old girl was diagnosed as having subperiosteal abscess. CT scan demonstrated opaque left ethmoidal cells extending through the destroyed bony wall into a well-defined adjacent extraconal soft tissue mass.. n (%) 23 (100.0) 23 (100.0) 17 (73.9) 13 (56.5) 10 (43.5) 7 (30.4) 7 (30.4). of sinusitis symptoms was shorter than 4 weeks. The diagnosis of acute sinusitis with orbital complications was based on clinical symptoms and signs, laboratory tests and diagnostic imaging. Sinusitis was defined by the presence of sinus opacification or air-fluid levels on either plain sinus X-ray film or computerized tomography (CT). All patients in our study had undergone ophthalmologic consultation. The medical history, physical examination, laboratory evaluation, radiological examination, bacteriology, treatment methods and outcome of the 23 patients were evaluated. Surgical management. A. B Fig. 2. A: A 1.5-month-old boy was diagnosed as having orbital abscess. Note the intraconal opacity in the left orbit and protosis. B: The boy underwent orbitotomy.. from January 1995 to July 2004. All of the children had symptoms of upper respiratory tract infection (URI) preceding sinusitis. The duration. Orbital complications of sinusitis were classified as follows [2]: group I, inflammatory edema: group II, orbital cellulites: group III, subperiosteal abscess: group IV, orbital abscess: and group V, cavernous sinus thrombosis. Surgical intervention was suggested when subperiosteal abscess, orbital abscess, or cavernous sinus thrombosis was diagnosed. Criteria for surgical intervention of subperiosteal abscess while on optimal medical therapy included: worsening of visual acuity or ocular motility, or failure to improve clinically within 48 hours. Patients with CT evidence of a medial subperiosteal mass lesion in the orbit were treated by endoscopic sinus surgery (ESS). During the ethmoidectomy, the lamina papyracea was inspected. If the lamina papyracea was intact, a horizontal cut through the inferior aspect of the lamina papyracea was made using a Freer evevator. The incision can be extended vertically and anteriorly. Pus was evacuated by elevating the bone plate medially. Pus and infected tissue.
(3) 146. Orbital Complications of Acute Sinusitis in Children. Table 2. Modality of treatment. Anti only. Anti + ESS. 14 Cellulitis 3 Subperiosteal abscess 3 Subperiosteal abscess Orbital abscess Anti = antibiotics; ESS = endoscopic sinus surgery.. Table 3. Microbiology of 6 children with surgical drainage. Microbiology. n (%). Pus culture Staphylococcus aureus Staphylococcushemolytics Streptococcus pneumonia Klebsiella pneumonia Propionibacterium acnes No growth Blood culture Staphylococcus aureus Staphylococcus hemolytics No growth. 6* 1 (14.3) 1 (14.3) 1 (14.3) 1 (14.3) 2 (28.6) 1 (14.3) 13 2 (15.4) 1 (7.7) 10 (76.9). *One specimen had two bacterial isolates. One child had the same blood and pus culture.. were sent for microbiological examination and culture. Entrance into the orbital tissue was avoided. Patients with CT evidence of medial subperiosteal and orbital mass lesion were treated by combined ESS and orbitotomy. RESULTS. The mean age at presentation was 5.0 years (range, 1.5 mo to 17 yr) ; 15 (65%) of the 23 children were younger than 5 years. The mean duration of symptoms before admission was 3.1 days (range, 1 to 8 d). The mean duration of hospitalization was 8.0 days (range, 3 to 19 d). Amoxicillin/clavulanic acid (Augmentin ®) was administered to 17 of the 23 patients initially and adjusted according to the pus culture or clinical presentation thereafter. The clinical symptoms at admission are shown in Table 1. The most common symptoms were eyelid edema (100%) and eyelid erythema (100%). Leukocytosis (WBC > 15,000/mm3) was found in 11 (47.8%) patients. The mean WBC count on admission was 12,453/mm3 (range, 6130 to 21,300/mm 3). Elevated C-reactive protein. Anti + ESS + orbitotomy. Mean hospitalization (d) 5.6 11.7 10.3 13.3. 3. (CRP) ( > 5 mg/L) was found in 11 (61.1%) of 18 patients with a mean value of 11.3 mg/L (range, 0.05 to 51.08 mg/L). CT was performed in 18 of 23 children. Of the 23 patients, 12 (52.2%) had inflammatory edema, 2 (8.7%) had orbital cellulitis, 6 (26.1%) had subperiosteal abscess (Fig. 1) and 3 (13.0%) had orbital abscess (Fig. 2A). No patient had evidence of cavernous sinus thrombosis. Treatment modalities are shown in Table 2. All patients received intravenous antibiotics beginning on the first day of admission. A total of 15 patients received intravenous antibiotics alone. In addition to intravenous antibiotics, 3 patients (subperiosteal abscess) underwent ESS, and 3 patients (orbital abscess) underwent ESS and orbitotomy (Fig. 2B). Microbiology studies of the blood and pus cultures revealed identifiable causative pathogens in 7 of the 15 patients. Only one child had a concomitant positive blood and pus culture (Staphylococcus hemolytics) and another child had mixed organisms of Staphylococcus aureus and Propionibacterium acnes from pus culture (Table 3). In this study, there was no cavernous sinus thrombosis, intracranial infection, or mortality. After a follow-up period of 1 to 2 months, no visual sequela was found among the 23 children. DISCUSSION. Sinusitis should always be considered in children with orbital swelling. Radiographs of the sinuses should be obtained. The absence of a possible predisposing factor, such as URI, does not rule out sinusitis. Sinusitis is the cause of orbital infections in 74% of patients with orbital swelling [4]. In fact, there is a close structural relationship between the paranasal sinuses and the.
(4) Chun-Hsin Liu, et al.. orbit. When the sinuses are the primary site of infection, inflammation can spread to the orbit along the valveless venous system and the ophthalmic veins into the cavernous sinus. Contiguous spread of infectious pathogens also may occur through the delicate lamina papyracea which separates the ethmoid sinus from the orbit, or through the thin bone separating the orbit from the frontal and maxillary sinuses. The pediatric population is more susceptible to orbital infection than adults [4,5]. In this retrospective study, the mean age of patients was 5.0 years which is similar to other studies [1,5,6]. In addition, there were 15 children (65%) whose ages were less than 5 years. All of the patients in our study had eyelid edema and erythema. Other ophthalmologic manifestations included chemosis (43.5%), protosis (30.4%), and limited ocular motility (30.4%). A high incidence of protosis (80%) and limited ocular motility (80%) has been reported by Arjmand et al [7]. The low incidence of protosis and limited ocular motility in this study may be attributable to the low number of patients with advanced orbital infection. The diagnosis of acute sinusitis is based mainly on clinical signs and symptoms. Diagnosing its complications is more difficult. Although it has been found that elevated erythrocyte sedimentation rate and CRP are sensitive in the diagnosis of acute sinusitis in adults [8], their value is not known in the diagnosis of complications of sinusitis in children. In our study, 11 (61.1%) of 18 patients had elevated CRP ( > 5 mg/L) with a mean value of 11.3 mg/L. Three children who were diagnosed as having orbital abscess had a higher mean value, 29.3 mg/L (range, 18 to 51). Pediatric patients are often uncooperative to ophthalmologic and otolaryngologic examinations. To minimize serious orbital complications of acute sinusitis in children, early diagnosis and institution of appropriate therapy are important. CT scan is indicated in all cases of orbital infection [9]. It provides useful information about the extent and site of inflammatory process in paranasal sinuses. 147. and orbit, enabling accurate staging of orbital infection [10]. In addition, it serves as a useful guid for surgical intervention. The accuracy of CT scan in predicting surgical findings was evaluated by Clary et al, who found that CT scan analysis correlated with surgical findings in 84% of cases [11]. Antimicrobial therapy of acute sinusitis in children with orbital infection is directed against the usual offending pathogens, such as Staphylococcus aureus and Streptococcus pneumoniae [1,3,12]. The culture results of the 6 specimens available in this series generally agreed with the previous studies. We also found a higher positive rate (71.4%) of aerobic pathogens than anaerobic pathogens (28.6%). The presence of anaerobic organisms is likely to be underestimated during bacteriologic studies because of the difficulty of culturing them. Orbital cellulitis is usually a local complication with only 5% of the patients having complications of bacteremia [13]. In this study, only 1 (7.7%) of 13 blood cultures was the same as the pus culture. Penicillin and ampicillin are not effective because of the high incidence of drug resistant bacterea [12,14]. Patients should be treated initially by a-lactamase-resistant antibiotic, such as Augmentin®, to provide adequate coverage for staphylococci as well as streptococci until culture results and sensitivities are obtained. Surgical intervention of acute sinusitis complicated by orbital infection is required when CT scan shows obvious abscess formation, visual acuity worsens for more than 24 hours, or patients are not responsive to antibiotic therapy after 24 to 48 hours of treatment [6,15,16]. Among six children with subperiosteal abscess in our study, three were successfully treated by medical therapy alone. The remaining three were treated by combining antibiotics therapy and surgical drainage without ocular sequela. The length of hospital stay in both medical and surgical groups was similar (11.7 and 10.3 d). A similar result was reported by Souliere Jr et al [16]. In our series, 3 patients were successfully treated by endoscopic drainage without complications. Pereira et al [17] reported a series of 24 patients.
(5) 148. Orbital Complications of Acute Sinusitis in Children. who were successfully treated by endoscopic surgery; Younis and Lazar [15] in a series of 10 patients published a similar result. However, this procedure should only be considered by a surgeon who is skilled in the technique and comfortable with performing ESS in children. The pediatric sinonasal anatomy is more complex than that of adults. Acute sinusitis with orbital complications should be suspected in children with a history of VRI who present with high fever, purulent rhinorrhea, eyelid edema, and eyelid erythema. ® Parenteral antibiotics, such as Augmentin , should be administered as soon as the diagnosis is made. In addition, CT should be performed for staging orbital inflammation and for guiding surgical intervention. REFERENCES. 1. Sobol SE, Marchand J, Tewfik TL, et al. Orbital complications of sinusitis in children. J Otolaryngol 2002;31:131-6. 2. Chandler JR, Langenbrunner DJ, Stevens ER. The pathogenesis of orbital complications in acute sinusitis. Laryngoscope 1970;80:1414-28. 3. Hytonen M, Atula T, Pitkaranta A. Complication of acute sinusitis in children. Acta Otolaryngol Suppl 2000;543:154-7. 4. Schramm Jr VL, Curtin HD, Kennerdell JS. Evaluation of orbital cellulites and results of treatment. Laryngoscope 1982;92:732-8. 5. Uzcategui N, Warman R, Smith A, et al. Clinical practice guideline for the management of orbital cellulitis. J Pediatr Ophthalmol Strabismus 1998;35: 73-9. 6. Juan CM, Chiu CH, Huang YC, et al. Orbital cellulites in children: clinical analysis of 16 cases. Acta Paed Sin 1995;36:286-8.. 7. Arjmand EM, Lusk RP, Muntz HR. Pediatric sinusitis and subperiosteal orbital abscess formation: diagnosis and treatment. Otolaryngol Head Neck Surg 1993;109: 886-94. 8. Hansen JG, Schmidt H, Rosborg J, et al. Predicting acute maxillary sinusitis in a general practice population. BMJ 1995;311:233-6. 9. Towbin R, Han BK, Kaufman RA, et al. Postseptal cellulites: CT in diagnosis and management. Radiology 1986;158:735-7. 10. Hirsch M, Lifshitz T. Computerized tomography in the diagnosis and treatment of orbital cellulitis. Pediatr Radiol 1988;18:302-5. 11. Clary RA, Cunningham MJ, Eavey RD. Orbital complications of acute sinusitis: comparison of computed tomography scan and surgical findings. Ann Otol Rhinol Laryngol 1992;101:598-600. 12.Chang CH, Lai YH, Wang HZ, et al. Antibiotic treatment orbital cellulites: an analysis of pathogenic bacteria and bacterial susceptibility. J Ocul Pharmacol Ther 2000;16:75-9. 13.Weiss A, Friendly D, Egkin K, et al. Bacterial periorbital and orbital cellulites in children. Ophthalmology 1983;90:195-203. 14. Brook I, Frazier EH. Microbiology of subperiosteal orbital abscess and associated maxillary sinusitis. Laryngoscope 1996;106:1010-3. 15.Younis RT, Lazar RH. Endoscopic drainage of subperiosteal abscess in children: a pilot study. Am J Rhinol 1996;10:11-5. 16. Souliere CR Jr, Antoine GA, Martin MP, et al. Selective non-surgical management of subperiosteal abscess of the orbit: computerized tomography and clinical course as indication for surgical drainage. Int J Pediatr Otorhinolaryngol 1990;19:109-19. 17.Pereira KD, Mitchell RB, Younis RT, et al. Management of medial subperiosteal abscess of the orbit in children: a 5 year experience. Int J Pediatr Otorhinolaryngol 1997;38:247-54..
(6) 149. 1 1. 1995. 1. 2004. 7. 23. 5.0 8.0. 65%. 6. 5 3. 3 Staphylococcus haemolyticus. 1. 2005;10:144-9. 404. 2. 2004. 12. 2005. 2. 13 5. 2005. 1. 21.
(7)
數據

相關文件
The aim of this article is to review the management of oral leukoplakia. The topics of interest are clinical diagnosis, methods of management and their outcome, factors associated
We present a new case of POF that was giant and review 10 previously reported giant lesions, with focus on the clinical presentation, radiographic features, and outcome to explore
Aim: The aim of this study is to investigate the prevalence of medical con- ditions and medications used by patients accessing emergency dental care at Manchester Dental
SUMMARY The purpose of this systematic review was to describe the prevalence of whiplash trauma in patients with temporomandibular disorders (TMDs) and to describe clinical signs
Henceforth, the aim of the study was to evaluate whether MRI findings of various degrees of disk displacement could be correlated with the presence or absence of clinical signs
Background: The purpose of this study was to evaluate the immunohistochemical expression of NF-κB and IL-6 in oral premalignant and malignant lesions and to
To clarify this clinical question, this study was performed to evaluate the accuracy of panoramic radiographic findings of interruption of mandibular canal, separately
In this respect, the aim of the present study was to as- sess volumetric as well as morphological surface changes of the orbital cavity in patients treated with both tooth- borne
