Outcomes of Coronary Artery Bypass Grafting in Patients with Inflammatory Rheumatic Diseases: An 11-year Nationwide Cohort Study
Chao-Han Lai, MD, PhD,1 Wu-Wei Lai, MD,1 Meng-Jiun Chiou, BS,3 Liang-Miin Tsai, MD,2 Jih-Sheng Wen, MD,1 Chung-Yi Li, PhD3,4
Departments of 1Surgery and 2Internal Medicine, National Cheng Kung University Hospital, College of Medicine, National Cheng Kung University, Tainan, Taiwan; 3Department of Public Health, College of Medicine, National Cheng Kung University, Tainan, Taiwan; 4Department of Public Health, College of Public Health, China Medical University, Taichung, Taiwan
Correspondence for reprints: Chung-Yi Li, PhD
Department of Public Health, College of Medicine, National Cheng Kung University, Tainan, Taiwan
No. 1, University Road, Tainan 70101, Taiwan Tel: 886-6-2353535, ext. 5862
Fax: 886-6-2359033
E-mail: [email protected]
Running title: CABG in Patients with Inflammatory Rheumatic Diseases Conflict of interest: None.
Word count: 2884
Keywords: Coronary artery bypass grafting (CABG), inflammatory rheumatic diseases, rheumatoid arthritis (RA), systemic lupus erythematosus (SLE), ankylosing spondylitis (ASp)
ABSTRACT
Objective: Patients with inflammatory rheumatic diseases have an increased
risk of developing coronary atherosclerosis. However, outcomes of surgical revascularization in these patients have been rarely studied. We aimed to determine whether, or which,
inflammatory rheumatic diseases may pose effects on mortality and adverse cardiac outcomes after coronary artery bypass grafting (CABG).
Methods: Using the National Health Insurance Research Database of Taiwan, we identified 40,639 adult patients who underwent first-time CABG between 2000 and 2010. Among these patients, 101 had rheumatoid arthritis (RA), 56 had systemic lupus erythematosus (SLE) and 73 had ankylosing spondylitis (ASp). The odds ratios (ORs) of operative mortality and hazard ratios (HRs) of overall mortality and adverse cardiac outcomes after CABG (i.e., myocardial infarction and repeat revascularization) in relation to RA, SLE and ASp were estimated. Results: With adjustment for potential confounders including patient characteristics, hospital levels and combined surgery, SLE was an independent predictor for operative mortality (adjusted OR 2.63, 95% confidence interval [C.I.] 1.04-6.65; P=.04) and ASp was marginally associated with operative mortality (adjusted OR 2.41, 95% C.I. 0.99-5.88; P=.054). In addition, SLE was a significant independent predictor for overall mortality during the follow-up period (adjusted HR 2.23, 95% C.I. 1.51-3.31; P<.0001) and might possibly increase the risk of repeat revascularization (adjusted HR 1.89, 95% C.I. 0.97-3.68; P=.06). Neither RA nor ASp was significantly associated with overall mortality and adverse cardiac outcomes. Conclusions: Our study may help surgeons and physicians recognize the potential risks inherent to SLE and ASp when conducting CABG surgery and providing follow-up care.
ULTRAMINI ABSTRACT
Among patients undergoing coronary artery bypass grafting, operative mortality was significantly associated with systemic lupus erythematosus (SLE) and was marginally associated with ankylosing spondylitis. In addition, SLE was a significant independent predictor for overall mortality and might possibly increase the risk of repeat
INTRODUCTION
Despite recent advances in diagnostic procedures and therapeutic modalities, coronary artery disease (CAD) remains the leading cause of death globally.1 It is well established that
several conventional risk factors (e.g., age, male gender, diabetes and hypertension) account for the development of CAD. Recently, other novel risk factors have been implicated. Evidence suggests the essential role of chronic inflammation in the pathogenesis of coronary atherosclerosis.2-5 Inflammatory rheumatic diseases, a group of disorders that primarily
affects joints, may involve different organ systems with a wide spectrum of clinical
manifestations. These inflammatory rheumatic disorders may result in chronic, relapsing and systemic inflammatory responses and increase cardiovascular risks in affected patients.2-7
Patients withinflammatory rheumatic diseases have a high burden of cardiovascular diseases that may cause increased morbidity and mortality.
Although patients with inflammatory rheumatic diseases appear to be more susceptible to coronary atherosclerosis, outcomes of patients who underwent surgery for coronary
revascularization have not been well documented. While several studies demonstrated single-hospital experiences of coronary artery bypass grafting (CABG) in patients with
inflammatory rheumatic diseases, all except one were case series/reports collecting 7 patients or less.8-12 The largest among these series included 44 patients with sinflammatory
rheumatic diseases composed mainly of patients with rheumatoid arthritis (RA).13 Limited
surgical experiences in any one single center were probably due to the rarity of this special patient population. Thus, conducting investigations using a large database would be a reasonable and practical approach.13-15
The National Health Insurance Research Database (NHIRD) of Taiwan contains a large sample size and high validity of diagnosis for catastrophic illnesses (e.g., inflammatory rheumatic diseases, cancers and end-stage renal disease [ESRD]) in the claims data. This
database may provide a valuable and real-world platform to review the outcomes of various surgical procedures in patients with certain rare diseases. Literature reviews indicate that a number of inflammatory rheumatic diseases, including RA, systemic lupus erythematosus (SLE), ankylosing spondylitis (ASp), systemic sclerosis (SSc), polymyositis-dermatomyositis (PM-DM) and inflammatory bowel diseases (IBD), are risk factors for the development of CAD, myocardial infarction and cardiovascular death.2-7 Through the NHIRD of Taiwan, we
attempted to describe the characteristics and outcomes of patients with inflammatory
rheumatic diseases undergoing CABG and to conduct risk analysis to recognize whether, or which, inflammatory rheumatic diseases might be associated with increased risks of
mortality and adverse cardiac outcomes during the perioperative period and long-term follow-up.
PATIENTS AND METHODS The CABG cohort
This retrospective cohort study was performed using the NHIRD of Taiwan. Our access to the NHIRD was approved by the Review Committee of the National Health Research Institutes. The whole study was approved by the Institutional Review Board of National Cheng Kung University Hospital (approval number: A-EX-102-010). The details of the NHIRD of Taiwan are contained in the Appendix E1.
The procedures that established the study cohort are summarized in Figure 1. We selected hospitalizations with the International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM) procedure codes for CABG from January 1, 2000 to December 31, 2010. Overall, there were 41,113 hospitalizations for CABG during the study period. Among these hospitalizations, we identified a total number of 40,639 adult patients aged at least 18 years who underwent first-time CABG as the CABG cohort. Using the ICD-9-CM diagnosis codes, we extracted patients with RA, SLE, ASp, SSc, PM-DM and IBD from the database. In the CABG cohort, the diagnosis of RA was preoperatively established in 101 patients (0.25%), SLE in 56 patients (0.14%) and ASp in 73 patients (0.18%). Patients with SSc (7 patients), PM-DM (7 patients) and IBD (2 patients) were few in number and thus were not included for further analysis.
Comorbidities and Outcome Measurements
Based on the hospital care data and prior hospitalizations of each patient, we recognized baseline medical comorbidities using ICD-9-CM codes, including hypertension, diabetes mellitus (DM), dyslipidemia, congestive heart failure (CHF), chronic kidney disease (CKD), peripheral artery disease (PAD), prior stroke and chronic obstructive pulmonary disease (COPD). Patients with ESRD were further identified from the CKD patients if they were registered with a dialysis catastrophic illness certificate. We also
identified whether the patients were hospitalized with the diagnosis of acute coronary syndrome (ACS). In addition, we recorded the levels of hospitals (medical centers, regional hospitals or district hospitals) where the CABG procedures were conducted. Concomitant procedures such as valve procedures and thoracic aortic surgery were also recorded.
Outcomes measured and analyzed in this study included operative mortality, overall mortality and adverse cardiac outcomes, including myocardial infarction and repeat revascularization, after CABG surgery. All patients of this cohort were evaluated for any occurrence of myocardial infarction and hospitalization for repeat revascularization (defined as either percutaneous coronary intervention (PCI or re-CABG) until mortality, withdrawal from the insurance program or December 31, 2010. For myocardial infarction and repeat revascularization, the date of the first episode would be counted if patients experienced more than one time.
The ICD-9-CM codes of procedures, diseases and adverse outcomes described in this study are listed in Table E1.
Statistical analysis
The patients who did not have the above inflammatory rheumatic diseases associated with CAD constituted the control group of this study. Patients with different inflammatory rheumatic diseases were compared separately with the control group to describe the differences in baseline characteristics and outcomes. Categorical variables, expressed as numbers and percentages, were compared by the Chi-square test or Fisher’s exact test as necessary. Continuous variables, expressed as mean ± standard deviation, were compared by the Student’s t test. Kaplan-Meier estimates of overall survival, freedom from myocardial infarction and freedom from repeat revascularization were plotted. Logistic regression analysis was performed to estimate the odds ratios (ORs) of operative mortality associated with RA, SLE and ASp with adjustment for potential confounding variables that have
been taken into account in relevant studies,18-21 including patient characteristics (age, sex, hypertension, DM, dyslipidemia, CHF, CKD, PAD, prior stroke, COPD and ACS), hospital levels and combined surgery. To estimate the hazard ratios (HRs) of overall
mortality after CABG associated with RA, SLE and ASp, Cox proportional hazard regression model was performed with adjustment for potential confounding variables. The model performance was assessed by using the C-statistic (for logistic) or Harrell’s C (for Cox). To assess the HRs of myocardial infarction and repeat revascularization associated with RA, SLE and ASp, we conducted competing risk regression models in which mortalities over the follow-up period were treated as competing risk events. The competing risk of mortality is an important consideration in studies involving geriatric patients with considerable
comorbidities.22 The difference between traditional survival analysis and competing risk
approach may not be substantial when the follow-up time is short, or if the competing risk is low. Nevertheless, under the circumstances that the proportion of patients experiencing a competing risk is equal or greater to the proportion of patients experiencing the primary outcome, or when the follow-up period is more than 5 years, competing risk analyses should be perform to demonstrate unbiased results.22 The HRs of competing risk regression was
computed using the “stcrreg” command in STATA (StataCorp LP, College Station, TX), which is based on Fine and Gray’s proportional hazard regression model.23 The statistical
analyses were performed using SAS software (SAS Institute, Cary, NC) and STATA for Windows. A P value below 0.05 was considered statistically significant.
RESULTS
Baseline characteristics and operative data
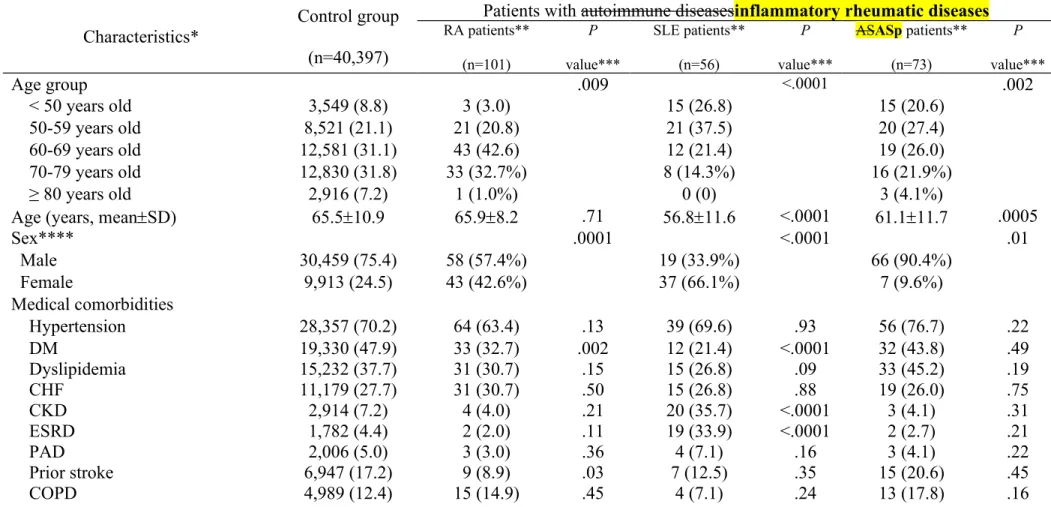
Comparisons of baseline characteristics and operative data between patients without inflammatory rheumatic diseases (control group) and RA, SLE and ASp patients in the CABG cohort are summarized in Table 1. Of the 40,397 patients without inflammatory rheumatic diseases, the mean age was 65.5 years old with a male-to-female ratio of about 3:1. Notably, patients undergoing CABG in Taiwan had a high prevalence of CKD (7.2%), ESRD (4.4%) and prior stroke (17.2%).
Of the 101 RA patients, the mean age was similar to that of the control group but the distribution was more centralized to the 60-69 year age group. Despite a male predominance, patients with RA were still less male-predominant than those without sinflammatory
rheumatic diseases. In addition, patients with RA had significantly lower proportions of DM and prior history of stroke than the control group.
The 56 SLE patients in the cohort were significantly younger and much more female-predominant compared with the control group. Patients with SLE had a significantly lower proportion of DM but were more likely to have CKD and also ESRD . Notably, the CABG procedures conducted for SLE patients were highly concentrated in medical centers
The 73 ASASp patients were significantly younger and more male-predominant than patients without inflammatory rheumatic diseases. The frequencies of medical
comorbidities, distribution of hospital levels and the proportions of overall combined procedures in ASp patients were not significantly different from those of the control group. Finally, the average total hospital costs per hospitalization of RA, SLE andASp patients were generally equal to that ofinflammatory rheumatic diseases.
Operative mortality and overall mortality
Among the three inflammatory rheumatic diseases, SLE was associated with significantly increased odds of operative mortality (crude OR 2.55, 95% confidence interval [C.I.] 1.05-6.20; P=.04) while RA and ASp were not (Table 2). To further assess whether RA, SLE or ASp might be independently associated with operative mortality, multiple logistic regression analysis was performed. After adjustment for potential confounding variables, SLE was an independent predictor for operative mortality (adjusted OR 2.63, 95% C.I. 1.04-6.65; P=.04) and ASp was associated with increased risk of operative mortality at the margin of
significance (adjusted OR 2.41, 95% C.I. 0.99-5.88; P=.054). The HRs of overall mortality associated with RA, SLE and ASp are shown in Table 2. Among the three inflammatory rheumatic diseases, SLE was significantly associated with overall mortality (crude HR 1.60, 95% C.I. 1.08-2.36; P=.02) whereas RA and ASp were not (Table 2). After controlling for potential confounding variables, SLE remained an independent predictor for overall mortality after CABG (adjusted HR 2.23, 95% C.I. 1.51-3.31; P<.0001).
Adverse cardiac outcomes
The Kaplan-Meier estimates of freedom from myocardial infarction and freedom from repeat revascularization after CABG are showed in Figures 2B and 2C. It should be noted that freedom from these two adverse cardiac events is not event-free survival; mortalities are considered to be competing risk events rather than non-informative censoring events in these analyses. The occurrences of myocardial infarction and repeat revascularization of the CABG cohort and HRs of myocardial infarction and repeat revascularization associated with RA, SLE and ASp are shown in Table 3. Among the three inflammatory rheumatic diseases, SLE was significantly associated with repeat revascularization after CABG (crude HR 2.08, 95% C.I. 1.07-4.07; P=.03), whereas neither RA nor ASp was significantly associated with myocardial infarction or repeat revascularization after CABG. After controlling for possible confounding variables, repeat revascularization occurred more frequently in patients with
DISCUSSION
Decades of studies have gradually established the link between inflammatory rheumatic diseases (e.g., RA) and accelerated atherosclerosis, as evidenced by higher frequencies of CAD and cardiovascular deaths in patients with these disease entities.2-5
Because CABG is currently one of the two main revascularization strategies for patients with CAD, we aimed to elucidate the impact of different CAD-associated inflammatory
rheumatic diseases on patients who needed CABG as their revascularization therapies. Even in this nationwide database, the patients of SSc, PM-DM and IBD were still too rare to provide sufficient numbers for analyses. Therefore, we focused on patients with preoperatively diagnosed RA, SLE or ASp, and compared baseline characteristics and surgical results of these patients versus those who did not have inflammatory rheumatic diseases. Probably due to the significant differences in disease characteristics among RA, SLE and ASp, outcomes of patients with theseinflammatory rheumatic diseases undergoing CABG were considerably diverse.
The largest single-hospital series among relevant literature reported by Birdas et al. consisted of 44 patients with inflammatory rheumatic diseases (0.8%) that were identified from a total of 5,496 patients undergoing CABG during a study period of 7 years.13 Of the 44
patients, 35 patients (79.6%) had RA, 8 had SLE and 1 had scleroderma. The authors found that the early mortality of CABG in patients with inflammatory rheumatic diseases was acceptable (2/44, 4.5%) as compared with that reported by STS database (2.7%; P>0.05). More recently, Varghese et al. investigated the in-hospital outcomes of RA patients after coronary revascularization using the Nationwide Inpatient Sample in the United States.14 In
this large database study that collected 5,485 patients (0.8%) with RA identified from 674,994 patients undergoing coronary revascularization, patients with RA were less likely than
accepted risk factor for CAD and patients with RA has a higher risk for cardiovascular death, RA patients in this cohort had an improvement of in-patient mortality and a reduced length of hospitalization after coronary revascularization, regardless of CABG or PCI, compared with the control group. In agreement with previous results reported by Varghese et al., patients with RA in our study were less likely to die during the perioperative period in contrast to those without inflammatory rheumatic diseases although the statistical significance was not achieved. In addition, we found that the risks of overall mortality, myocardial infarction and repeat revascularization in RA patients were substantially similar to those of patients without inflammatory rheumatic diseases (Tables 2 & 3). Taken together, these
observations suggested that patients with RA should go ahead with the CABG procedures if indicated as these patients had at least equal outcomes in comparison to those without inflammatory rheumatic diseases.
While previous studies focused mainly on RA, we broadened the scope of our study to explore the impact of SLE and ASp on patients undergoing CABG. Using a nationwide database approach, we found that CABG procedures for SLE patients in this cohort were more likely to be conducted in medical centers. Despite younger age and a lower prevalence of traditional risk factors for CAD (e.g., DM), patients with SLE suffered from accelerated atherosclerosis and had a much higher prevalence of CKD and ESRD. It is plausible to speculate that SLE patients had poorer medical conditions than usual, leading to a higher risk of surgical mortality. CABG in SLE patients has been considered to be a surgical challenge because these patients usually have unique characteristics of multiple organ involvement and long-term use of immunosuppressants such as steroids.8 Graft thrombosis is a major
concern in these patients, and thus postoperative administration of heparin has been recommended. Even after adjustment of potential confounding factors, SLE was still an independent predictor of operative mortality and overall mortality (Table 2). In addition, SLE
might possibly increase the risk of repeat revascularization following CABG (Table 3). Although details of graft choices were unavailable in the NHIRD of Taiwan, accelerated vein graft stenosis could possibly be the cause and extensive arterial grafting has been advised in these patients.10 In a PCI cohort reported by Maksimowicz-McKinnon et al.,25 SLE patients
were more likely to experience myocardial infarction and more often required repeat PCI than non-SLE patients within 1 year. Therefore, patients with SLE may be more likely to
experience adverse cardiac outcomes after coronary revascularization either by CABG or PCI and thus post-revascularization risk reduction should be more aggressive.
There are some limitations to our study. First, we conducted a nationwide study involving only small numbers of patients with inflammatory rheumatic diseases and adverse outcomes, fully understanding that these results can only be considered as suggestions for future studies in large clinical databases (such as the STS Adult Cardiac Database or the Nationwide Inpatient Sample in the United States14 used by Varghese et
al.). Second, large reimbursement cuts in Taiwan, as attested to by the low total hospital costs
in the CABG cohort, may reduce the quality of cardiac care.28 Whether this economic factor
brought more negative impacts on patients with inflammatory rheumatic diseases undergoing CABG was uncertain as these patients inevitably need multi-disciplinary care. Thus, our findings require further validation in other healthcare systems. Third, some variables of interest were unavailable in this secondary data analysis, such as the extent of CAD, intraoperative choice of bypass grafts, details of immunosuppressants during the follow-up period and causes of death, and therefore these variables cannot be considered in the analyses. Finally, although studies have demonstrated the high accuracy of ICD-9 diagnosis in NHIRD of Taiwan, the validity issue related to the medical claim data is always a concern. In addition, a relatively small percentage of data missing or miscoding of diagnoses is inherent in studies using large databases. Nevertheless, such coding errors are
random and should not be a valid argument for the observed findings of our study because such non-differential disease misclassification tends to bias the results toward the null.
In summary, we studied the impact of RA, SLE and ASp on patients undergoing CABG. Among patients undergoing CABG, those with RA had outcomes similar to those of patients without inflammatory rheumatic diseases. SLE was an independent prognostic predictor of both operative mortality and overall mortality and was probably associated with repeat revascularization, whereas ASp appeared to be associated with operative mortality. Since CAD is highly prevalent in patients with inflammatory rheumatic diseases, our findings may help surgeons and physicians recognize the inherent risks associated with SLE and ASp in patients undergoing CABG.
ACKNOWLEDGEMENT
The study was based on data from the NHIRD provided by the National Health
Insurance (NHI) administration, Ministry of Health and Welfare of Taiwan, and managed by the National Health Research Institutes of Taiwan. However, the interpretation and
conclusions contained herein do not represent those of the NHI administration, Ministry of Health and Welfare of Taiwan, or the National Health Research Institutes of Taiwan.
REFERENCES
1. Deb S, Wijeysundera HC, Ko DT, Tsubota H, Hill S, Fremes SE. Coronary artery bypass graft surgery vs percutaneous interventions in coronary revascularization: a systematic
review. JAMA. 2013;310:2086-95.
2. Onat A, Direskeneli H. Excess cardiovascular risk in inflammatory rheumatic diseases: pathophysiology and targeted therapy. Curr Pharm Des. 2012;18:1465-77.
3. Roifman I, Beck PL, Anderson TJ, Eisenberg MJ, Genest J. Chronic inflammatory diseases and cardiovascular risk: a systematic review. Can J Cardiol. 2011;27:174-82. 4. Kaplan MJ. Management of cardiovascular disease risk in chronic inflammatory disorders. Nat Rev Rheumatol. 2009;5:208-17.
5. Shoenfeld Y, Gerli R, Doria A, Matsuura E, Cerinic MM, Ronda N, et al. Accelerated atherosclerosis in autoimmune rheumatic diseases. Circulation. 2005;112:3337-47.
6. Gandhi S, Narula N, Marshall JK, Farkouh M. Are patients with inflammatory bowel disease at increased risk of coronary artery disease? Am J Med. 2012;125:956-62.
7. Ungprasert P, Charoenpong P, Ratanasrimetha P, Thongprayoon C, Cheungpasitporn W, Suksaranjit P. Risk of coronary artery disease in patients with systemic sclerosis: a systematic review and meta-analysis. Clin Rheumatol. 2014;
8. Ura M, Sakata R, Nakayama Y, Ohtsuka Y, Saito T. Coronary artery bypass grafting in patients with systemic lupus erythematosus. Eur J Cardiothorac Surg. 1999;15:697-701. 9. Bozbuga N, Erentug V, Kaya E, Akinci E, Yakut C. Coronary artery bypass grafting in patients with systemic lupus erythematosus. J Card Surg. 2004;19:471-2.
10. Bossert T, Falk V, Gummert JF, Rahmel A, Mohr FW. Coronary artery bypass grafting in patients with systemic lupus erythematosus. Z Kardiol. 2003;92:219-21.
11. Maeda K, Nishi H, Sakaguchi T, Miyagawa S, Ueno T, Kuratani T, et al. Coronary Artery Bypass Grafting in a Patient Initially Presenting with Systemic Lupus Erythematosus. Ann Thorac Cardiovasc Surg. 2013;
12. Lin CH, Lee ML, Hsu RB. Cardiac surgery in patients with systemic lupus erythematosus. Interact Cardiovasc Thorac Surg. 2005;4:618-21.
13. Birdas TJ, Landis JT, Haybron D, Evers D, Papasavas PK, Caushaj PF. Outcomes of coronary artery bypass grafting in patients with connective tissue diseases. Ann Thorac Surg. 2005;79:1610-4.
14. Varghese JJ, Koneru S, Scaife SL, Zahnd WE, Francis ML. Mortality after coronary artery revascularization of patients with rheumatoid arthritis. J Thorac Cardiovasc Surg. 2010;140:91-6.
15. Francis ML, Varghese JJ, Mathew JM, Koneru S, Scaife SL, Zahnd WE. Outcomes in patients with rheumatoid arthritis and myocardial infarction. Am J Med. 2010;123:922-8. 16. Weng MY, Huang YT, Liu MF, Lu TH. Incidence of cancer in a nationwide population cohort of 7852 patients with primary Sjogren's syndrome in Taiwan. Ann Rheum Dis.
2012;71:524-7.
17. Hsieh TH, Wang JD, Tsai LM. Improving in-hospital mortality in elderly patients after acute coronary syndrome--a nationwide analysis of 97,220 patients in Taiwan during 2004-2008. Int J Cardiol. 2012;155:149-54.
18. LaPar DJ, Stukenborg GJ, Guyer RA, Stone ML, Bhamidipati CM, Lau CL, et al. Primary payer status is associated with mortality and resource utilization for coronary artery bypass grafting. Circulation. 2012;126:S132-9.
19. Sabik JF, 3rd, Blackstone EH, Gillinov AM, Smedira NG, Lytle BW. Occurrence and risk factors for reintervention after coronary artery bypass grafting. Circulation.
2006;114:I454-60.
volume-outcome relationship: temporal trends and selection effects in California, 1998-2004. Health Serv Res. 2008;43:174-92.
21. Nashef SA, Roques F, Sharples LD, Nilsson J, Smith C, Goldstone AR, et al. EuroSCORE II. Eur J Cardiothorac Surg. 2012;41:734-44; discussion 44-5.
22. Berry SD, Ngo L, Samelson EJ, Kiel DP. Competing risk of death: an important consideration in studies of older adults. J Am Geriatr Soc. 2010;58:783-7.
23. Fine JP, Gray RJ. A proportional hazards model for the subdistribution of a competing risk. J Am Stat Assoc. 1999;94:496-509.
24. Ward MM. Outcomes of hospitalizations for myocardial infarctions and cerebrovascular accidents in patients with systemic lupus erythematosus. Arthritis Rheum. 2004;50:3170-6. 25. Maksimowicz-McKinnon K, Selzer F, Manzi S, Kip KE, Mulukutla SR, Marroquin OC, et al. Poor 1-year outcomes after percutaneous coronary interventions in systemic lupus erythematosus: report from the National Heart, Lung, and Blood Institute Dynamic Registry. Circ Cardiovasc Interv. 2008;1:201-8.
26. Roman MJ, Salmon JE. Cardiovascular manifestations of rheumatologic diseases. Circulation. 2007;116:2346-55.
27. Lundberg G, King S. Coronary revascularization in women. Clin Cardiol. 2012;35:156-9.
28. Chang GM, Cheng SH, Tung YC. Impact of cuts in reimbursement on outcome of acute myocardial infarction and use of percutaneous coronary intervention: a nationwide
population-based study over the period 1997 to 2008. Med Care. 2011;49:1054-61. 29. Cheng CL, Kao YH, Lin SJ, Lee CH, Lai ML. Validation of the National Health Insurance Research Database with ischemic stroke cases in Taiwan. Pharmacoepidemiol Drug Saf. 2011;20:236-42.
30. Yu YB, Gau JP, Liu CY, Yang MH, Chiang SC, Hsu HC, et al. A nation-wide analysis of venous thromboembolism in 497,180 cancer patients with the development and validation of a risk-stratification scoring system. Thromb Haemost. 2012;108:225-35.
Tables
Table 1. Comparisons of baseline characteristics and operative data between patients without CAD-associated autoimmune
diseasesinflammatory rheumatic diseases (control group) and RA, SLE and ASASp patients in the CABG cohort of Taiwan, 2000-2010.
Characteristics*
Control group (n=40,397)
Patients with autoimmune diseasesinflammatory rheumatic diseases RA patients** (n=101) P value*** SLE patients** (n=56) P value*** ASASp patients** (n=73) P value*** Age group .009 <.0001 .002 < 50 years old 3,549 (8.8) 3 (3.0) 15 (26.8) 15 (20.6) 50-59 years old 8,521 (21.1) 21 (20.8) 21 (37.5) 20 (27.4) 60-69 years old 12,581 (31.1) 43 (42.6) 12 (21.4) 19 (26.0) 70-79 years old 12,830 (31.8) 33 (32.7%) 8 (14.3%) 16 (21.9%) ≥ 80 years old 2,916 (7.2) 1 (1.0%) 0 (0) 3 (4.1%)
Age (years, meanSD) 65.510.9 65.98.2 .71 56.811.6 <.0001 61.111.7 .0005
Sex**** .0001 <.0001 .01 Male 30,459 (75.4) 58 (57.4%) 19 (33.9%) 66 (90.4%) Female 9,913 (24.5) 43 (42.6%) 37 (66.1%) 7 (9.6%) Medical comorbidities Hypertension 28,357 (70.2) 64 (63.4) .13 39 (69.6) .93 56 (76.7) .22 DM 19,330 (47.9) 33 (32.7) .002 12 (21.4) <.0001 32 (43.8) .49 Dyslipidemia 15,232 (37.7) 31 (30.7) .15 15 (26.8) .09 33 (45.2) .19 CHF 11,179 (27.7) 31 (30.7) .50 15 (26.8) .88 19 (26.0) .75 CKD 2,914 (7.2) 4 (4.0) .21 20 (35.7) <.0001 3 (4.1) .31 ESRD 1,782 (4.4) 2 (2.0) .11 19 (33.9) <.0001 2 (2.7) .21 PAD 2,006 (5.0) 3 (3.0) .36 4 (7.1) .16 3 (4.1) .22 Prior stroke 6,947 (17.2) 9 (8.9) .03 7 (12.5) .35 15 (20.6) .45 COPD 4,989 (12.4) 15 (14.9) .45 4 (7.1) .24 13 (17.8) .16
ACS 9,084 (22.5) 29 (28.7) .13 11 (19.6) .61 12 (16.4) .22 Hospital level .29 .0002 .16 Medical center 22,047 (54.6) 48 (47.5) 46 (82.1) 44 (60.3) Regional hospital 16,408 (40.6) 46 (45.5) 8 (14.3) 23 (31.5) District hospital 1,942 (4.8) 7 (6.9) 2 (3.6) 6 (8.2) Combined surgery 4,523 (11.2) 7 (6.9) .17 9 (16.1) .25 13 (17.8) .07 Valve procedures 4,225 (10.5) 7 (6.9) .25 8 (14.3) .35 13 (17.8) .04 Aortic surgery 720 (1.8) 0 (0) .16 2 (3.6) .19 2 (2.7) .24
Total hospital cost (NTD, meanSD) 414,181209,580 423,677190,038 .65 436,540222,220 .43 454,484360,830 .10
RA, rheumatoid arthritis; SLE, systemic lupus erythematosus; ASASp, ankylosing spondylitis; SD, standard deviation; DM, diabetes mellitus; CHF, congestive heart failure; CKD, chronic kidney disease; ESRD, end-stage renal disease; PAD, peripheral artery disease; COPD, chronic obstructive pulmonary disease; ACS, acute coronary syndrome; NTD, New Taiwan Dollar
* Data are expressed as patient number (percentage) unless otherwise indicated.
** Two patients with combination of RA and SLE were counted in both RA and SLE patient groups. One patient with combination of RA and ASASp was counted in both RA and ASASp patient groups.
*** The P values were calculated by comparison with the control group. **** Sex data were missing or undetermined in 25 patients (0.06%).
Table 2. Odds ratios of operative mortality and hazard ratios of overall mortality after CABG associated with RA, SLE and ASASp.
Variables
Operative mortality Overall mortality
Mortality rate (95% CI) Crude OR (95% CI) Adjusted OR* (95% CI) Crude HR (95% CI) Adjusted HR** (95% CI) Control group (n=40,397) 4.0% (3.8%-4.2%) 1.00 1.00 1.00 1.00 RA (n=101) 3.0% (0.6%-8.4%) 0.85 (0.29-2.47) 0.81 (0.27-2.39) 1.14 (0.82-1.59) 1.20 (0.87-1.67) SLE (n=56) 8.9% (3.0%-19.2%) 2.55 (1.05-6.20) 2.63 (1.04-6.65) 1.60 (1.08-2.36) 2.23 (1.51-3.31) ASASp (n=73) 6.9% (0.8%-12.9%) 1.91 (0.80-4.59) 2.41 (0.99-5.88) 1.06 (0.72-1.57) 1.40 (0.94-2.07) RA, rheumatoid arthritis; SLE, systemic lupus erythematosus; ASASp, ankylosing spondylitis; OR, odds ratio; HR, hazard ratio; CI, confidence interval.
* Based on the multiple logistic regression analysis (C-statistic = 0.71) with adjustment for age, sex, hypertension, DM, dyslipidemia, CHF, CKD, PAD, prior stroke, COPD, ACS, hospital levels and combined valve and/or aortic surgery.
** Based on Cox proportional hazard regression model (Harrell’s C = 0.72) with adjustment for age, sex, hypertension, DM, dyslipidemia, CHF, CKD, PAD, prior stroke, COPD, ACS, hospital levels and combined valve and/or aortic surgery.
Table 3. Hazard ratios of myocardial infarction and repeat revascularization after CABG associated with RA, SLE and ASASp.
Variables
Myocardial infarction Repeat revascularization
Crude HR (95% CI) Adjusted HR* (95% CI) Crude HR (95% CI) Adjusted HR* (95% CI) Control group (n=40,397) 1.00 1.00 1.00 1.00 RA (n=101) 0.78 (0.32-1.86) 0.78 (0.32-1.87) 1.14 (0.58-2.24) 1.09 (0.56-2.13) SLE (n=56) 1.41 (0.58-3.40) 1.32 (0.54-3.25) 2.08 (1.07-4.07) 1.89 (0.97-3.68) ASASp (n=73) 0.63 (0.20-1.94) 0.68 (0.22-2.09) 0.64 (0.24-1.70) 0.62 (0.23-1.63)
RA, rheumatoid arthritis; SLE, systemic lupus erythematosus; ASASp, ankylosing spondylitis; HR, hazard ratio; CI, confidence interval. * Based on Fine and Gray’s proportional hazard regression model with adjustment for age, sex, hypertension, DM, dyslipidemia, CHF, CKD, PAD, prior stroke, COPD, ACS, hospital levels and combined valve and/or aortic surgery.
FIGURE LEGENDS
FIGURE 1. Study flow chart: cohort assembly of 40,639 adult patients undergoing first-time surgical revascularization for coronary artery disease between 2000 and 2010 in the National Health Insurance Research Database (NHIRD) of Taiwan.
*RA, rheumatoid arthritis; SLE, systemic lupus erythematosus (SLE); ASp, ankylosing spondylitis; SSc, systemic sclerosis; PM-DM, polymyositis-dermatomyositis; IBD, inflammatory bowel diseases
FIGURE 2. Kaplan-Meier estimates of (A) overall survival (B) freedom from myocardial infarction (C) freedom from repeat revascularization in patients without CAD-associated autoimmune diseasesinflammatory rheumatic diseases (control group) and RA, SLE and ASASp patients in the CABG cohort of Taiwan, 2000-2010. The proportions and 95% confidence intervals of overall survival, freedom from myocardial infarction and freedom from repeat revascularization at 2, 4, 6, 8 and 10 years are summarized in Table E2.