Designing a Rule-based System for Mobile Healthcare
Yun-Lin Tsai
a, Cheng-En Pang
a, Shein-Yung Cheng
a, Chin-Li Lin
b, Jia-Sheng Heh
a Information and Computer Science Engineering, Chung Yuan Christian University, Taiwan aYunlin Elder-Caring Association, Yunlin County, Taiwan b
Abstract
The population in Taiwan will become elder adult population; the healthcare requirement of elder adult population has a year-by-year increase tendency. Elder adult usually suffer form one or more chronic diseases, example include arthritis, hypertension and diabetes. Change in the care mode by the technology development. This paper designing a care rule base to apply in the Mobile Healthcare work flow, and rule-based system creates the care inform message to notify the caregiver by the state of the elder adult including the disease state, physical state, living state, assist instrument state, and the care requirement we purposed. The caregiver can provide appropriate care according to the care inform message. The caregivers received the information and deal properly with the requirement timely by mobile device, and they can employ accessing the care data via 3G network to providing active and timely care action and care suggestion. The combination with Tele-Healthcare service can improve the quality and the performance of Healthcare service.
Keyword: Tele-Healthcare, Rule-based, Mobile
Healthcare
Introduction
An overview of the medical situation in Taiwan, the medical resource in the country is less than in the urban areas. The needs to improve healthcare layer in the country include the lack of medicinal resource, health consultation and homecare service, and individual and physical disabled elder need the immediate and effective home-care mode [3]. According to the ministry of the interior, the physical disabled elder population is about one hundred and eighty thousand people, the need of
home-care increases day by day [4].
Besides providing a more complete home care service, if we can provide mobile healthcare in good time and apply this service to certain less medical resource area to assist in caring individual elders and physical disabled elders, then we can develop a well care medical system.
Johns points out that the first goal of any type Mobile Healthcare service is to carry the knowledge and experience of caregiver from one place to another place [8]. The main two types of Mobile Healthcare include interactive video mode and store-and-forward mode [11]. The main difference between them is that the interactive video mode supply timely care to cared person and the other mode is asynchronous transfer technique. For example, transfer the cared person diagnosis data [6]. In this paper, we purposed the Mobile Healthcare System built on mobile device to improving the efficiency and performance in the mobile healthcare application.
1. Background
At the start, the definition of the Tele-Home-Care means that transferring disease measurement data by using video, audio and other information technology and providing a professional service at the remote point. Today the researcher Koch points out the definition of the Tele-Homecare is “a two-way interactive audio-visual communication between a healthcare provider and a patient in his/her place or residence”.
The researcher Choi has implemented MobileNurse system which consists of PDAs and mobile support system (MSS) which supports clinical data exchange between PDAs and hospital information system. MobileNurse has four modules each of which performs: patient information management, medical order check,
nursing recording, nursing care plan [5]. The researcher Kafeza proposes the Healthcare Alert Management System (HAMS) and integrates the HAMS with existing hospital information system. When the patient enters the hospital, the system will build a complete care process and send alert to the related medical person [9].
Blount builds a platform, called Personal Care Connect, to facilitate the remote monitoring of patient [1]. Handheld computers are widely used in family practice residency programs in the United States. Handheld computer may offer solutions to administrative and information management that are more realistic than those offered by desktop computers [2].
In this paper, we construct a mobile Healthcare Service. When the cared person requests care assistance the caregiver will record the request to the mobile device. If the time of the request is up, the system will refer the request priority and then send a message to notify the caregiver to do the care action by the rule reasoning. When the caregiver completes the care action, they must report the state of this action to the system and the manager will monitor and manage the mobile caregiver care state and quality.
2. The Analysis of the Care Assistance 2.1 The Roles and the States of Cared Person
There are two types of the participants in the Mobile Healthcare Service: cared person and caregiver. Cared person is someone who is mentally ill, mentally handicapped, physically disabled or whose health is impaired by sickness or old age. Caregiver is someone who provides care to the cared person.
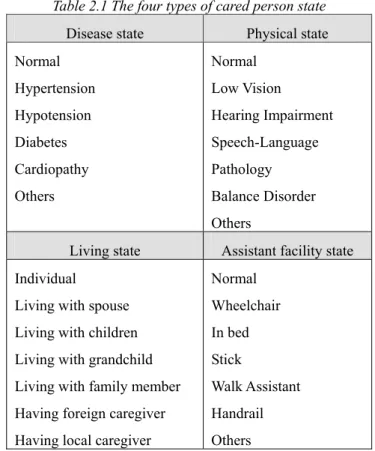
The Mobile Healthcare service model and Tele-Homecare model are like the above. In this paper, we purposed the activity ability of the cared person into four types, including disease state, physical state, family state, and assistant facility state. The example of this activity ability of the cared person is shown as the following Table 2.1.
Table 2.1 The four types of cared person state
Disease state Physical state Normal Hypertension Hypotension Diabetes Cardiopathy Others Normal Low Vision Hearing Impairment Speech-Language Pathology Balance Disorder Others
Living state Assistant facility state Individual
Living with spouse Living with children Living with grandchild Living with family member Having foreign caregiver Having local caregiver
Normal Wheelchair In bed Stick Walk Assistant Handrail Others
In the table 2.1, we can clearly define the cared person states, and in the following chapter we will describe the states of cared person as the input part of the rule in inference process.
2.2 The Definition and Classification of the Care Assistance
In this paper, we study literatures about the care assistance for the cared person from these three researchers Emanuel [7], Kinsella [14], and Maglaveras [10], and trying to categorize these assistances into six types of the care assistance in mobile healthcare service we supported. There are six types of care assistances in the Mobile Healthcare service including Nursing Assistance, Clinical Assistance, Homemaking, Food Assistance, Emotion Caring, and Transportation.
The definition of the assistance for the cared person request is as the following:
assistance= (assistanceType, assistanceSub_type)
“assistanceType” is the main type of the care assistance,
and “assistanceSub_type”is the sub type of the main type
care assistance. The six care assistances describe the need of the cared person clearly. The six main type assistance
and its sub type are as the following Table2.2.
Table2.2 The six types of the care assistances
Nursing Assistance Clinical Assistance Homemaking 1. Take medicine hit 2. Physical measurement 3. Others 1. Bruise nursing 2. Medicine injection 3. Others 1. Clearing the clothes 2. Improving living environment 3. Others
Food Assistance Transportation Emotion Caring
1. Assist to meal 2. Buy lunchbox 3. Others 1. Accompany her/him to hospital 2. Call the taxi 3. Others
1. Accompany to take a walk 2. Visit friendly 3. Others
3. Care Rule Design
3.1 The Facts mapping to the Care Assistance
After the caregiver created the care assistance from the cared person who requested, the mobile healthcare system must transfer the requirement to the fact object. In this paper, we define the fact object as "task”. The definition is as the following.
task = (Patient, Assistance, Description, Timerequest,
Timealert, Priority)
“Patient” means the cared person who requests this assistance; “Assistance” means the type of assistance; “Description” means the description of this assistance; “Timerequest” means the care time of the assistance; “Talert
”
means the time to alert the caregiver; “Priority” means the priority level of the assistance.
When the fact object was created from the care task, we must refer the cared person states (Patient) and the type of the care assistance (Assistance). The “Patient” definition is as the following.
(Patient (name ) (p_Disease ) (p_Physical ) (p_Living) (p_Facility ))
For example:
(Patient (name “Jin-Hwo Lin”) (p_Disease “Apoplexy ” “Diabetes”) (p_Physical “Normal”) (p_Living Individual”) (p_Facility “Stick” “Hearing Aid”))
The Assistance definition is as the following. (Assistance (main_type) (sub_type))
For example:
(Assistance (“Food Assistance”) (“Buy lunchbox on someone’s behalf”))
When the Patient object and Assistance object are constructed, we can construct the task object if the assistance is required. For example, cared person “Jin-Hwo Lin” wants to eat a lunchbox at noon but he can not prepare meal by himself. So he requests the “Buy lunchbox on someone’s behalf” of the “Food Assistance” at noon on someday. The task is as the following.
task = (Patient(Jin-Hwo Lin), Assistance(“Food Assistance”)(“Buy lunchbox on someone’s behalf”)), “by the lunchbox at noon”, “2007/06/08 12:00PM”, “2007/06/08 11:30PM”, “high”)
3.2 The Care Rules and the Alert
The care rules are constructed by the caregiver or the professional medical person in the CLIPS system. The condition part (Left Hand Side) of the rule is the above fact object (Patient, Assistance), and the action part (Right Hand Side) of the rule is the care notification message.
The care notification message is build by the care message template, and the system will send the message to the caregiver. This message will notify the caregiver that he has new care task to do. A simple care rule example is as the following:
(defrule check-disease(patient(disease ”Asthma”)) =>
(assert (alert (msg "this cared person had Asthma "))) ) The care assistances for the cared person request are different, so we design the different rule for the care assistances and distinguish rule for identifying care assistance type. A sample distinguish rule is as the
following.
(defrule ?req<-(task(id?id)(main_type?main_type) (sub_type?sub_type)(patient?pid))
Î
(if( (req?main_type “Homemaking” ) then
(assert (assistance(main_type “Homemaking”) (sub_type?sub_type) )) )
In this paper, we define six rule modules for the six main type care assistances. The following table Table 3.1 is the care assistance and corresponding care rules modules.
Table 3.1 the six assistance rule module
Assistance Type Rule Module
Nursing Assistance NA_Rule Clinical Assistance CA_Rule
Homemaking HM_Rule
Food Assistance FA_Rule
Emotion Caring EC_Rule
Transportation T_Rule And then the check “Asthma” disease rule in the NA_Rule module is as the following:
(defrule NA_Rule::check-disease(patient (disease “Asthma”))
=>
(assert (alert (msg “this cared person had Asthma”))) ) For example, the cared person requests the “Buy lunchbox” in “Food Assistance” and the cared person has Diabetes disease, so the caregiver needs to buy the low-sugar and low-salt lunchbox for the cared person. The rule is as the following:
(defrule FA_Rule::find_disease(patient ( disease “Diabetes”))
=>
(assert(alert (msg “buy the lunchbox, and the lunchbox is low-salt and low-sugar ”))) )
When the rule is triggered the system will send the notification message to the caregiver.
3.3 The Design of Care Alert
In this paper, we define the care notification message to the caregiver as the care alert. There are two types to sending care alert to the caregiver, one is that when the cared person request a care assistance the system will send a care alert that contains the cared person request assistance and the care suggestions about the assistance by the rule-based system inference, the other is that the system and the Tele-Homecare System cooperate with each other, if the Tele-Homecare System find a emergency state about the cared person then the Mobile Healthcare system will send a care alert to the caregiver mobile device.
In this paper, we apply the care alert to the first type of the above. And the care alert definition is as the following:
alert = (Patient, Description, Caregiver, Timedeadline)
“Patient” means the cared person;”Description” means
the description of the care alert content; “Caregiver” means the care alert receiver. “Timedeadline” means that
how long the system will check after the alert is sent. The system can check that the caregiver do this work on time by this parameter.
For example, the cared person Jin-Hwo Lin who has diabetes and his request care assistance is the food assistance, and then the care alert is as the following: alert = (Patient(“Jin-Hwo Lin”), “help him to buy a lunchbox at noon, pay attention to his diabetes, must to buy a low-sugar lunchbox”, Caregiver(Shu-Ywe Lai),
“2007/06/08 12:30PM”)
The system will send the message to the caregiver and check at 2007/06/08.
4. Mobile Healthcare System
In this paper, we construct a mobile Healthcare Service. The Mobile Healthcare Service is shown as Figure4.1 .In the figure left, the person in the case block is the cared person who uses the local measurement instrument to do physical measurement and the data will be transferred to the Tele-Homecare system in the Tele-Care block via the
internet. The data will be stored in the Tele-Homecare system. When the cared person requests care assistance the caregiver will record the request to the mobile device. If the time of the request is up, the system will refer the request priority and create the care alert to notify the caregiver to do the care action by the rule reasoning. When the caregiver completes the care action, they must report the state of this action to the system and the manager will monitor and manage the mobile caregiver care state and quality.
Figure 4.1 the Mobile Healthcare Service
4.1 The Architecture of Mobile Healthcare System
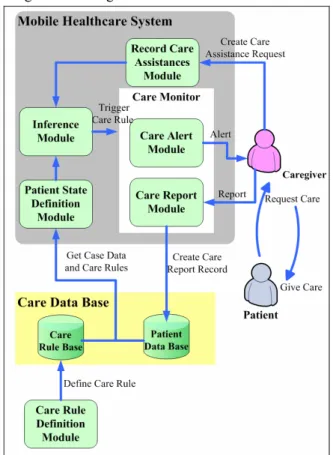
The Figure 4.2 is the Mobile Healthcare system module architecture diagram. The caregiver received the request of the cared person, and then the caregiver creates a care assistance request to the “Record Care Assistances” module that will check this request time and its priority. If the time of request was up, the “Record Care Assistances” module will trigger the “Inference” module. The “Inference” module will infer according the rules in the section three. Then the “Patient State Definition” module will get the patient state and rule from the system database for the rule reasoning. The caregivers can use the “Care Rule Definition” external module of the Mobile Healthcare System to define the care rule. When the “Inference” module triggers a rule and sends a care alert to the “Care Monitor” block. The “Care Monitor” block
contains two modules: the “Care Alert” module that sends the care alert to the caregiver mobile device and the “Care Report” module that receive the caregiver’s report after doing the care action. The “Care Report” module will store the report data to the system database for the manager monitoring the state of the service.
Figure4.2 Mobile Healthcare System Architecture
4.2 The Mobile Healthcare Example
The following example describes the flow of the mobile care service with the Mobile Healthcare system.
Figure 4.3 the Mobile Healthcare Example
First, the cared person request a care assistance, a situation was created that the cared person request when
the caregiver visit him at home; another situation was created that the cared calls the caregiver to tell the request of cared person. This care assistance is the “Cover for buying lunchbox “of the “Food Assistance”.
Second, the caregiver records the request to the system according to the assistance type. And the system will do the rule reasoning according the four physical information (Disease, Living, Physical, Assistant) and create an appropriate care alert. In this example, because this cared person who has liver function disease, so the system will create a message about buying a low-salt lunchbox. Third, the message created by the system will show in the mobile device to notify the caregiver. The caregiver will do the assistance to buy a low-salt lunchbox and send to the cared person.
Figure 4.4 the care alert screen
Finally, the caregiver will report the state of the action to the server via the mobile device.
5. Conclusion
In this paper, the Mobile Healthcare system provides the real-time without space limit care service to caregiver. The system will automatically to notify the caregiver about cared guideline of the care assistance which cared person requested, this guideline was created by the mobile healthcare system to provide an appropriate care alert to the caregiver according the states of cared person and the type of the care assistance. So the caregivers will get a better result of care test while they are using the mobile healthcare system with the PDA in the home-care service, and the system will also improve the fault of the Tele-Homecare system.
5.1 The Design of Experiment
This system will be applied to a care family organization for elder in a certain country in Taiwan. When the mobile caregivers of the organization do the home-care service, they use this system on the mobile device in their hand and the cooperators can monitor the status of the service with the Tele-health system.
There are two systems in the organization: one is the twenty-four/all day call center system, and the other is case data manage system. The Mobile Healthcare system will reduce the delay time of the care action and raise the care ratio and quality to improve the cared person’s life.
5.2 The Future work
In the future, we are considering extending the mobile healthcare service combines the resource in local area including the local library, the policy station, and the household registration office to provide a complete community healthcare service.
Acknowledgement
The authors would like to thank “Yunlin Elder-Caring Association” in Taiwan for their help and recommendations in this experiment.
Reference
[1] M. Blount, V. M. Batra, A. N. Capella, M. R. Ebling, W. F. Jerome, S. M. Martin, M. Nidd, M. R. Niemi, and S. P. Wright. (2007). “Remote health-care monitoring using Personal Care Connect”. IBM Systems Journal, 46(1), 95-113. [2] Dan F. Criswell and Michael L. Parchman. (2002).
Handheld Computer Use in U.S. Family Practice Residency Programs. Journal of the American Medical Informatics Association, 9, 80-86.
[3] H.-S. Chen, F.-R. Guo, C.-Y. Chen, J.-H. Chen and T.-S. Kuo. (2001). Review of telemedicine projects in Taiwan. International Journal of Medical Informatics, 61(2-3), 117-129.
[4] Chia-Hui Chen, Mer-Ri Su, Shiow-Li Hwang, Sao-Jie Chen, Yu-Tzu Dai, and Heng-Shuen Chen. (2004). Home Telehealth: Bring Care to the Site of
Living. Formosan Journal of Medicine, 8(6), 837-845. (in Chinese)
[5] Jinwook Choi, Jonghoon Chun, Kangsun Lee, Sanggoo Lee, Donghoon Shin, Sookyung Hyun, Daehee Kim, and Donggyu Kim. (2004). “MobileNurse hand-held information system for point of nursing care.” Computer Methods and Programs in Biomedicine, 74(3), 245-254.
[6] Ashish N. Dwivedi, Rajeev K. Bali, aouf N. G. Naguib, and Nahy S. Nassar. (2006). “The Efficacy of the M-Health Paradigm: Incorporating Technological”, Organisational and Managerial Perspectives, Springer US
[7] E. J. Emanuel, D. L. Fairclough, J. Slutsman, H. Alpert, D. Baldwin and L. L. Emanuel, (1999). Assistance from family members, friends, paid care givers, and volunteers in the care of terminally ill patients. New England Journal Medicine, 341, 956–963.
[8] P. M. Johns. (1997). Integrating information systems and health care, Logistics Information Management, 10(4), 140-145.
[9] Eleanna Kafeza, Dickson K.-W. Chiu, S.-C. Cheung, and Marina Kafeza. (2004). Alerts in Mobile Healthcare Application: Requirements and Pilot Study. IEEE Transactions on Information Technology in Biomedicine, 8(2), 173-181. [10] Nicos Maglaveras, Ioanna Chouvarda, Vassilis G.
Koutkias, George Gogou, Irini Lekka, Dimitrios Goulis, Avram Avramidis, Charalambos Karvounis, George Louridas, and E. Andrew Balas. (2005). The Citizen Health System (CHS): A Modular Medical Contact Center Providing Quality Telemedicine Services. IEEE Transactions on Information Technology in Biomedicine, 9(3), 353-362.
[11] Strode SW, Gustke S, Allen A. (1999)"Technical and clinical progress in telemedicine". JAMA. 1999;281:1066-1068