ORIGINAL PAPER
Analysis of Network Type Exchange in the Health Care
System: A Stakeholder Approach
Wen-Hui Yang&Jer-San Hu&Ya-Yen Chou
Received: 29 July 2010 / Accepted: 20 October 2010 # Springer Science+Business Media, LLC 2010
Abstract The present study aims to offer a different perspective of network systems using the health care system in Taiwan as an example. By establishing a paradigm that conforms to the reality of the health care system, this study expects to develop a correct analysis approach. The study applies the stakeholder analysis approach and performs the sampling according to the principles of the qualitative method. The main findings include (1) The health care system is a regulated network type exchange system, in which a third party affects all exchanges among stakeholders; (2) under mutual intervention of interests, stakeholders pursue common interests in appearance but individual interests in reality; (3) the intervening impacts on stakeholder interests come from a common source, which dominates the operating and dynamics of the entire system.
Keywords Network organization . Health care system . Network connectedness . Stakeholder analysis . Qualitative method
Introduction
Since implementation of National Health Insurance in 1995, the health care environment and system in Taiwan have undergone drastic changes. Due to the fact that medical services belong to a highly professional business, a high level of information asymmetry exists between doctors and patients. To facilitate operations of the system and supply of medical services, the health care system has to involve numerous stakeholders, including the third-party health insurance payor. As the national health insurance system involves enormous profits in a wide range of areas, it affects the interests of almost all stakeholders in the health care system. It can be viewed as one of the largest and most widely influential single public policies. All these characteristics have made the health care system relatively more complicated than general corporate network systems. The numerous problems that have arisen since launch of the national health insurance have affected the behavior and attitude of members in the system and even impacted the entire medical structure and ecology. These problems include distortion of the medical ecology [1], drug price difference, deteriorating medical quality [2], and increasing limitation on medical staff [3]. They have either directly or indirectly influenced each member in the medical system as well as the equilibrium of the system which involves providers of medical supplies, hospitals, medical staff, and patients. In fact, the national health insurance policy concerns interests of multiple stakeholders. While some stakeholders are financially oriented, others pursue benefits of the policy or benefits for consumers. Their interests are divergent but interactive and intertwining. Problems stemming from their interests are complicated and considerable in amount. Thus, the evolution of the national health insurance is the result of interactions between stakeholders and variation in their interests. This evolution process, as it involves a huge amount of members and interests in a wide range of areas, has increased the complexity and variability of the health care system, which is very much different from corporate network
W.-H. Yang (*)
Department of Health Services Administration, China Medical University,
No.91 Hsueh-Shih Road, Taichung 40402, Taiwan e-mail: [email protected] J.-S. Hu
Department of Business Administration, Fu Jen Catholic University,
Taipei County, Taiwan e-mail: [email protected] Y.-Y. Chou
Department of Marketing and Logistics Management, Far East University,
Tainan County, Taiwan e-mail: [email protected] DOI 10.1007/s10916-010-9618-5
systems constructed through vertical or horizontal integration. However, Department of Health (DH) or Bureau of National Health Insurance (BNHI) which dominate most health and medical policies lack comprehensive and systemic thinking in formulating policies. They have not realized the fact that the health system involves multiple stakeholders with each having different concerns/interests in the resource-limited system. The numerous problems and chaos that we have seen in today’s health care system are the result of their unilateral thinking in formulation of policies.
Previous studies on health care systems investigated system phenomena or related issues mainly from a single-actor perspective or from the dyadic exchange perspective [3, 4]. Most of them analyzed the health care system from the viewpoint of the government or the authority or from the viewpoint of medical service providers. Only a few of them attempted to anatomize the system from the social system perspective. As a result, many of their derived views are biased or superficial and unhelpful for clarifying the root of the observed problems or phenomena. The rapid changes of the social and demographic environment have increased the multiplexity of health care organizations and resource invest-ment involved in a health care system [5]. In Taiwan, the national health insurance has created numerous problems and chaotic situations, which have directly and severely impacted the health care system in many aspects [6]. The scope of the system involved is broad, the number of stakeholders impacted is large, and the multiplexity of interconnections among actors in the system is high. These factors have increased the complexity and dynamics of the health care system. In the increasingly complicated management environment, conven-tional marketing theories developed on the basis of dyadic exchange relationships may not fully delineate the reality of complex exchange phenomena. The marketing view that considers exchanges among multiple businesses using a network paradigm can help us explore exchange behaviors of various types and for various purposes [7]. As the health care system involves complicated and intertwining interests and relations, chaos, and a volatile environment, conventional methods that analyze the care system from a single-actor, dyadic exchange, static, and outcome-oriented perspective can no longer capture the interconnected and dynamic relations in the system. To avoid missing core and realistic issues or deriving ineffective solutions, it is necessary for us to adopt a comprehensive dynamic system view to analyze the various problems and chaotic phenomena in the health care system.
This paper uses Taiwan’s health care system as an example and the business network view as a foundation to analyze interaction relationships among stakeholders and their implica-tions from the stakeholder perspective. This paper proposes a different view of network research to capture multiple facets of this the health care system instead of its appearnaces or images shaped by the authority or service providers and then construct a
paradigm to induce from unresolved issues and chaotic situations a theoretical view that can reflect reality, serve as a basis for future research, and contribute to the development of a sound health care system.
The research focuses and questions of this paper include: (1) How does a health care system operate? How do stakeholders involved in this health care system respectively view the operations of the system? (2) What are the interactions among stakeholders? What is
the implication of their interactions if all the dyadic relations are interconnected?
(3) What are the interests pursued by each stakeholder involved in the health care system? Who is the dominator of the system?
(4) Do stakeholders’ interests conflict or align with one another? What is the homogeneity or heterogeneity in their interaction relationships? Is there any interven-tion or conflict of interests between dyadic relainterven-tions?
Literature review
Network organization in health care industry
To cope with environmental changes, health care institutions usually establish networks based on vertical or horizontal integration of organizations. During 1990s, another form of integration emerged among the US health care institutions. This new form of organizational integration, called the Integrated Delivery Systems (IDS), integrates organizations both horizontally and vertically. According to American Hospital Association (AHA), Integrated Delivery Systems refer to a group of hospitals, physicians, other providers, insurers and/or community agencies. Members in this group work together to provide a coordinated continuum of services to a defined population and are willing to be held clinically and fiscally accountable for the outcomes and the health status of the population served [8, 9]. They rely on a number of coordinating mechanisms, including partnership coordination infrastructure, integration of governance, clinical care, bonding, finances, and information [10] to achieve integrated operation of health care systems. The integrated model of health care services is generally similar to the concentric business network model. To realize the goal of providing continuous care, health care providers usually position themselves in a concentric network, in which they view the focal organization as the center and work with it to jointly provide continuous care [11]. Chang [12] found that interactions among hospitals are mainly centered on medical centers or regional hospitals which generally are larger in scale and have better reputation, more facilities, and sufficient resources. Other types of hospitals will
develop dyadic relations with hospitals at the center of the network but have no interaction with one another even if they have a common cooperation partner. Hence, the health care network is a “center-subcenter-periphery” model. As sug-gested in the above literature, a health care network is basically centered at a hospital, and other members in this network will interact with this focal hospital in a concentric manner.
Unlike conventional business networks consisting of only upstream and downstream firms, the health care network has more types of members. Since implementation of the national health insurance, the insurer (Bureau of National Health Insurance) has become a member of the domestic health care network, and the complexity of operations of the network has thus increased. In the health care industry, government intervention in the relations in the network is very common. The interaction relationships in the network are confined to regulations and restrictions. Government intervention affects the whole industry and network structures therein [13]. The network system with an insurer’s intervention is basically a third-party payor model. In this model, health service providers acquire their incomes from a third party payor not from patients, and their incomes are also limited by this third party payor. The third-party payor will set up various regulations that health service providers need to follow when providing health care services. Although patients do not directly pay the providers of medical services, they are required to pay insurance premium to the third-party payor and also follow certain regulations to seek medical services. In general, this third-party payor regulates and influences all members in this network [14,15].
Network connectedness
Connectedness refers to the notion that relations between organizations in a business network do not exist in isolation and are definitely affected by other organizational relations. Relations in the networks are connected to each and therefore embedded in the environment [16]. Embedded-ness refers to the interdependence between actors and the connections between relations, where the exchanges are dependent on other relations [17]. All members are embedded in a network context, and development of one exchange relation depends on development of another. In other words, two exchange relations are connected to the degree that exchange in one relation is contingent upon exchange in the other [18].
The structure of a connected relationship usually consists of a focal relation that is connected with other relations, either directly or indirectly, in the network [19]. There are also influences between connected relations. One of them is called the effect transmission impact, which is a driver of connected changes. Actors in the network will adjust their
behaviors or change their relations with other actors according to the change of relations they perceive. Therefore, any change of one actor or one relation will result in changes of other actors or relations interconnected in the network. This change is transmissible and its effect will spread to the entire system. The other influence is called the intervening impact, which is a directional effect. Ritter [18] discusses the effects on inter-organizational relationships from an inter-organizational relationship per-spective and proposes that the impact of one relationship on another can have three different features: (1) Neutral effect: Relationship (x) has no impact on relationship (y). (2) Positive effect: Relationship (x) has an overall positive impact on relationship (y). This effect is supporting, enabling or even enforcing the existence of relationship (y). (3) Negative effect: Relationship (x) has an overall negative impact on relationship (y). This effect is hindering, disabling or even excluding the existence of relationship (y). This negative impact can be caused by resource limitations. Hu and Tsai [20] conducted an in-depth inquiry of relational exchange behaviors and their derived exchange effects on dyadic exchanges in the Taiwanese National Health Insurance System. Their findings show that both positive and negative exchange value effects exist in the medical network system, and such effects affect exchange relations between members in the system and may prevent them from attaining the transferred and accumulated exchange value in the value chain.
Research design
The present paper selects Taiwan’s health care system as the research object to investigate stakeholders’ perceptions of and opinions about the health care system. As this network system involves a large number of stakeholders and interconnected relations, more interpersonal, qualita-tive, and systemic insights are needed in the analysis of inter-group relationships. Stakeholder analysis is a cross-sectional analysis technique. It collects information of members involved in an organization, and its interpretation of contexts is a multi-faceted perspective and a subjective value. It has the characteristics of qualitative research methods. Therefore, this technique is suitable for our research from the stakeholder perspective.
This study uses the triangulation method to gather data from multiple sources and the coding process of the qualitative method to analyze the qualitative data. The primary data came from in-depth interview based on a semi-structured interview guideline, and the secondary data from document analysis. Through open coding, codable phrases or segments in the interview transcripts were conceptually labeled and categorized. Later, axial coding
was performed to develop properties and dimensions of the main categories. The entire coding process was carried out on the computer program, NVivo.
The sampling procedure of the qualitative approach is adopted. Based on the concepts related to the theory, data were collected and analyzed concurrently to guide the use of sampling schemes. In the beginning, open sampling was adopted. Through purposive sampling, participants with abundant information were selected for in-depth interview. Later, theoret-ical sampling was applied with a focus on the relationship and heterogeneity among the research categories to collect data until theoretical saturation was reached. At last, a total of 33 valid samples of stakeholders were obtained. The samples were selected through the following procedure: (1) Define stake-holders in the health care system: First of all, we focused on the pharmacy services and collected data from stakeholders of pharmacy services. We chose the pharmacy services mainly because pharmacy services are involved in nearly all medical services and a large proportion of interactions in the health care network take place between stakeholders of pharmacy services. Besides, close interactions between physicians and drug suppliers are normal in the medical industry. If we focused on the medical services which involve a wider range of
stake-holders, including drug and health care products suppliers, medical facility supplier, medical technicians, and members of related organizations, our research scope would be too wide and our results might be out of original focus. According to the concentric network model proposed by Lin and Wan [11] and classifications of stakeholders in the health care system adopted by [21,22], we further defined hospitals as the center of the network system and classified members in the system, including drug suppliers, hospital education institutions, physicians and pharmacists (hospital employees), patients, other medical institutions (other hospitals and clinics), BNHI-licensed pharmacies, and DH/BNHI, into four stakeholder groups. These four stakeholder groups are upstream suppliers, internal stakeholders, end customers, and external stakeholders and third-party groups. Based on the above definition and classification, we proposed a relationship network of stake-holders of pharmacy services in the health care system with hospitals at the center of the network (Fig.1). (2) Select key stakeholder groups: The reputational approach was adopted to let prominent scholars or figures and participants in in-depth interview determine which stakeholder groups are relatively more influential. Results show that Department of Health (DH), Bureau of National Health Insurance (BNHI), hospitals,
Physician Upstream Supplier Pharmacist Pharma Company Hospital Other Medical Organization Health Insurance Pharmacy Patient DH/BNHI
External Organization and Third Party
Downstream Patient
Intra-organization
:focal relationship :dyad relationship
Medical Education Organization Fig. 1 Relationship of
interac-tions between stakeholders of the pharmacy services in the health care system. Source: Adapted from Morgan and Hunt (1994) and Savage et al. (1997)
physicians and pharmacists (hospital employees), pharma companies, and patients are key stakeholder groups. (3) Select samples by purposive sampling from stakeholder groups for interview: This step is intended to select representatives of each stakeholder group who can offer abundant information regard-ing the research questions. Two officials of DH and BNHI, six hospital executives, five executives of pharma companies, ten physicians, five pharmacists, and five patients were selected. Based on theoretic ideas of sampling, we used the factors that may cause changes in or differences between stakeholders as the main sampling criteria. Hospitals were divided by hospital level (medical center, regional hospital, and local hospital) and ownership status (public or private). As physicians possess most professional knowledge in the health care system and are direct providers of medical services to end customers (patients), their behavioral models are largely affected by changes in the health care system. They play a critical role in our investigation of the interconnected relations in the health care system. Hence, we selected relatively more physicians to obtain research data. The selected physicians were specialists in internal medicine, surgery, and other departments (such as emergency, ENT, and dermatology) having at last five years of service experience in the field. From DH/BNHI stakeholder groups, we selected managers in the central government and managers in local branches to understand the perspectives and standpoints of DH/ BNHI from different angles. As to drug suppliers, we divided them by business type into foreign drug manufacturers, local drug manufacturers, and drug distributors. Due to information asymmetry between physicians and patients and lack of medical knowledge among most patients, patients have little influence on the professional operations and actions of members at the B to B level (including DH/BNHI, hospitals, physicians, pharma-cists, and drug suppliers). Despite taking the largest proportion of stakeholders of the health care system, patients can provide very limited information about the research questions. Since they cannot influence the operating procedure of medical services, we selected only a few patients to be our research samples, including chronic patients in need of frequent pharmacy services (for hypertension or diabetes), patients requiring treat-ments to be paid in package (such as hemodialysis), patients who need to undergo surgical operations of internal medicine (such as cardiac ablation or resection of colorectal polyps), and patients receiving orthopedic treatments (for unidentified pains). Besides, we also selected five patients who were able to outline the relationship of stakeholders for further interview.
To accurately understand collected responses and ensure explanatory validity and internal validity, the multi-method approach was adopted for data collection. Based on the triangulation approach, the research data were collected via interview and document analysis. Cross-verification of respond-ents’ responses was constantly conducted during the interview to ensure that the respondents were not affected by the researcher’s personal orientation. After data collection, the
transcribed data were mailed to the respondents to check the accuracy of transcription and several researchers were invited to compare the collected data with data used in previous studies. Researcher convergence was tested to ensure research validity. As to external validity, because this study was based on the qualitative research approach, which was to obtain in-depth data from a relatively smaller sample, we adopted the method introduced by Yin [23] to achieve generalization of the research results. We selected key stakeholders that could provide abundant data relevant to the research questions from each stakeholder group and sought theoretical saturation. Therefore, we could use findings derived from a small sample to reflect and explain some common problems. Besides, to ensure the research reliability, the tape-recorded data were written as verbatim to ensure qualitative data consistency. The interview procedure was also standardized. An interview guideline and a semi-structured questionnaire were developed to ensure setting consistency.
Qualitative study and results Network type exchange system
The analysis of in-depth interview with stakeholders of pharmacy services in the health care system suggests that the health care system is a complicated system involving multiple stakeholders, including hospitals, physicians, pharmacists, pharma companies, DH/BNHI (DH/BNHI), and patients. The analysis also shows that, when asked to describe interactions, exchange relations and activities with other stakeholders, respondents would frequently mention about stakeholders that may affect or be affected by dyadic relations in the system. Hence, any dyadic relation in the health care system has a set of connections with other stakeholders. By integrating all the sets of connections, we can construct an internal exchange network of the health care system. In the following sections, we will analyze exchange relations in the network from two perspec-tives, including the consumer marketing theory and the business marketing theory.
The perspective of the consumer marketing theory
This is an analysis from the business to customer (B to C) perspective with a focus on the dyadic relations between health care service providers, internal employees, and end customers.
In any dyadic relation, both parties in the relation mentioned about the impact of their connections with other stakeholders in the system. For instance, our analysis of the“Physician-Patient” dyadic relationship shows that most physicians mentioned that pharmacy services for patients are affected by the payment system of DH/BNHI and their hospitals will be forced to purchase mainly drugs manufactured by Taiwanese companies. As shown in Table1, actors involved in the“Hospital-Patient”
dyadic relationship include DH/BNHI, physicians, and pharma companies, which jointly form a relationship portfolio “DH/ BNHI-Pharma company-Hospital-Physician-Patient”. Actors involved in the“Physician-Patient” dyadic relationship include DB/BNHI, Hospital, and Pharma company and form a relationship portfolio “DH/BNHI-Pharma company-Hospital-Physician-Patient”. Finally, actors involved in the “Pharmacist-Patient” dyadic relationship include DH/BNHI, Hospital, and Pharma company, creating a relationship portfolio “DH/BNHI-Pharma company-Hospital-“DH/BNHI-Pharmacist-Patient”. The above three portfolios when connected according to interactions among them can form an exchange network of the patient relationship category of the health care system.
The perspective of the business marketing theory
This is an analysis from the business to business (B to B) perspective with a focus on the dyadic relations between health care service providers, internal employees, and upstream suppliers.
In any dyadic relation, both parties mentioned about the impact of their connections with other stakeholders in the system. For instance, in the analysis of the dyadic relations between hospitals, physicians, and pharmacists, we found that all of the actors mentioned about the effects of the Global Budget Payment System set up by DH/BNHI including drop of hospital revenue and decline of salaries for physicians and pharmacists. As shown in Table2, DH/BNHI is the main actor involved in the Physician” and “Hospital-Pharmacist” dyadic relationships. These actors form two relationship portfolios, namely “DH/BNHI-Hospital-Physi-cian” and “DH/BNHI-Hospital-Pharmacist”. Actors involved in the “Physician-Pharmacist” dyadic relationship include DB/BNHI and Hospital and form a relationship portfolio
“DH/BNHI-Hospital-Physician-Pharmacist”. The above three portfolios jointly form an exchange network of the intra-organization relationship category of the health care system.
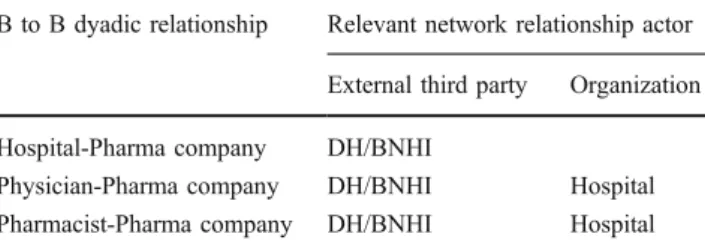
In any dyadic relation, both parties mentioned about the impact of their connections with other stakeholders in the system. For instance, in the analysis of the dyadic relations between hospitals, physicians, pharmacists, and pharma-ceutical companies, we found that all of the actors mentioned about the impacts of the drug price reduction policy launched by DH/BNHI on the dyadic relations. The policy would affect hospitals’ drug acquisition policy and physicians’ prescription behavior, and pharmaceutical com-panies would also attempt to influence pharmacists’ drug acquisition decisions. As shown in Table 3, DH/BNHI is the main actor involved in the“Hospital-Pharma company” dyadic relationship. DH/BNHI and the two actors jointly form a relationship portfolio“DH/BNHI-Pharma company-Hospital”. Actors involved in the “Physician-Pharma company” dyadic relationship include DB/BNHI and hospital, which jointly form a relationship portfolio“DH/BNHI-Pharma company-Hospital-Physician”. Finally, actors involved in the “Pharmacist-Pharma company” dyadic relationship include DH/BNHI, hospital, and physician. These actors jointly form a portfolio “DH/BNHI-Pharma company-Hospital-Pharmacist-Physician”. The above three portfolios jointly create an exchange network of the supplier relationship category of the health care system.
Based on the dyadic relationships between stakeholders of the health care system, this paper analyzes the portfolios of direct and indirect relationships between actors in the dyadic relations and the linkages between portfolios. Three exchange networks have been constructed, including the exchange network of the patient relationship category, the exchange network of the intra-organization relationship
B to C dyadic relationship Relevant network relationship actor
External third party Organization Intra-organization Upstream supplier
Hospital-Patient DH/BNHI Physician Pharma company
Physician-Patient DH/BNHI Hospital Pharma company
Pharmacist-Patient DH/BNHI Hospital Pharma company
Table 1 The relationship portfolios of the patient relationship category
Table 2 The relationship portfolios of the intra-organization relation-ship category
B to C dyadic relationship Relevant network relationship actor
External third party Organization
Hospital-Physician DH/BNHI
Hospital-Pharmacist DH/BNHI
Physician-Pharmacist DH/BNHI Hospital
Table 3 The relationship portfolios of the supplier relationship category
B to B dyadic relationship Relevant network relationship actor
External third party Organization
Hospital-Pharma company DH/BNHI
Physician-Pharma company DH/BNHI Hospital
category, and the exchange network of the supplier relationship category. After the three exchange networks are connected, there is evidence suggesting that the health care system is a network type exchange system. In this system, exchanges and interactions between actors are in a network structure, and dyadic relations do not exist in isolation. Dyadic relations in the system will definitely interact with, affect or be affected by other actors or other relations in the network.
Network type exchange system from the stakeholder perspective
As indicated above, the health care system is a complicated multi-exchange network system consisting of multiple stakeholders. Thus, this study employs the stakeholder perspective and uses the data analysis result to explain the characteristics of exchanges among stakeholders in the network exchange system. These characteristics include pursuit of common interests, intervening impact of interest, and the common source of intervening impact of interest. Pursuit of common interests
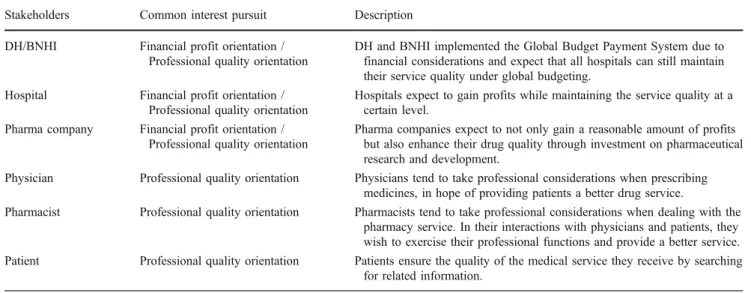
As shown in Table 4, all stakeholders in the health care system pursue a common goal when providing their pharmacy services. This goal is to provide services to patients on the condition that the management efficiency is maximized and the service quality is maintained at a certain level. In other words, it is to pursue both professional quality and fulfillment of the financial goal. Internal members (physicians and pharmacists) are not responsible for the financial operations of the hospital, so their pursuits are mainly oriented to professional quality. Providing the
drug service to patients in a professional manner is a common interest pursued by all intra-organization stake-holders of the health care system.
Intervening impacts of interests
Table5 shows the intervening impacts of interests existent in the effect transmission paths of the interaction relation-ship“Hospital–Physician -Pharmacist-Patient”.
From various perspectives of the actors, including DH/ BNHI, hospital, physician, and pharmacist, this paper analyzes the interests pursued by each stakeholder under mutual intervention of interests. The result indicates that the interests pursued by these stakeholders are inconsistent with the common interests and stakeholders’ attitude and behaviors also vary under the intervening impacts of interests.
Table 6 shows the intervening impacts of interests existent in the effect transmission paths of the interaction relationship“Hospital-Pharmacist-Physician”. From various perspectives of the actors, including DH/BNHI, hospital, physician, and pharmacist, we analyze the interests pursued by each stakeholder under mutual intervention of interests. Our findings suggest that the interests pursued by these stakeholders do not align with the common interests and stakeholders’ attitude and behaviors also vary under the intervening impacts of interests.
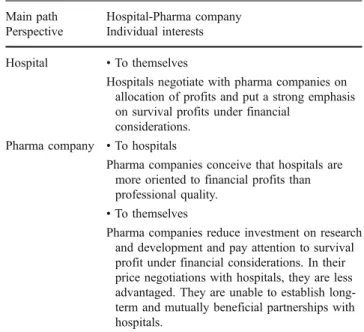
Tables7and8show the intervening impacts of interests existent in the effect transmission paths of the interaction relationships “Hospital-Pharma company” and “Pharma company- Hospital-Physician-Pharmacist”. From various perspectives of the actors, including DH/BNHI, hospital, Pharma company, physician, and pharmacist, we analyze the interests pursued by each stakeholder under mutual
Table 4 Analysis of common interests of stakeholders
Stakeholders Common interest pursuit Description
DH/BNHI Financial profit orientation /
Professional quality orientation
DH and BNHI implemented the Global Budget Payment System due to financial considerations and expect that all hospitals can still maintain their service quality under global budgeting.
Hospital Financial profit orientation /
Professional quality orientation
Hospitals expect to gain profits while maintaining the service quality at a certain level.
Pharma company Financial profit orientation /
Professional quality orientation
Pharma companies expect to not only gain a reasonable amount of profits but also enhance their drug quality through investment on pharmaceutical research and development.
Physician Professional quality orientation Physicians tend to take professional considerations when prescribing
medicines, in hope of providing patients a better drug service.
Pharmacist Professional quality orientation Pharmacists tend to take professional considerations when dealing with the
pharmacy service. In their interactions with physicians and patients, they wish to exercise their professional functions and provide a better service.
Patient Professional quality orientation Patients ensure the quality of the medical service they receive by searching
intervention of interests. Our results indicate that the interests pursued by these stakeholders do not converge and stakeholders’ attitude and behaviors also vary under the intervening impacts of interests.
Table 5 Analysis of intervening impacts of interests involved in the relationships of the patient relationship category
Perspective Individual interests
Hospital • To themselves
Under financial considerations, hospitals set up regulations to control physicians’ drug prescription. • To patients
Due to implementation of the national health insurance, the demands for health care services have drastically increased. However, the confines of global budgeting
affect hospitals’ finance and medical service quality.
Therefore, hospitals will reduce their marketing activities to mitigate the service demands.
Physician • To hospitals and themselves
Physicians conceive that regulations on drug
prescription set up by the hospitals are mainly based on financial considerations, and these regulations affect their professional considerations in prescribing medicines. However, some physicians agree that these regulations can reduce unnecessary use of medicine.
Pharmacist • To hospitals and themselves
Pharmacists conceive that hospitals’ arrangement of
pharmacists based on financial considerations prevents them from providing the best service.
Patient • To hospitals
- Patients perceive changes of the drug service but cannot identify the difference. They can only passively accept and adapt to the changes.
- Patients perceive time-consuming and inconvenience on seeking ambulatory services because of a large volume of the outpatients in hospitals.
• To pharmacists
Patients cannot perceive the
professional functions of pharmacists. They feel that they have not received a good pharmacy service.
Table 6 Analysis of intervening impacts of interests involved in the relationships of the intra-organization relationship category
Perspective Individual interests
Physician • To hospitals and pharmacists
Physicians conceive that hospitals fail to employ sufficient pharmacists due to financial considerations and this insufficiency may affect the quality of
pharmacists’ verification of their prescriptions.
Pharmacist • To hospitals and themselves
Pharmacists conceive that employment of pharmacists is insufficient and the quality of their verification of prescriptions may be affected as a result.
Table 7 Analysis of intervening impacts of interests involved in the relationships of the supplier relationship category (I)
Main path Hospital-Pharma company
Perspective Individual interests
Hospital • To themselves
Hospitals negotiate with pharma companies on allocation of profits and put a strong emphasis on survival profits under financial
considerations.
Pharma company • To hospitals
Pharma companies conceive that hospitals are more oriented to financial profits than professional quality.
• To themselves
Pharma companies reduce investment on research and development and pay attention to survival profit under financial considerations. In their price negotiations with hospitals, they are less advantaged. They are unable to establish long-term and mutually beneficial partnerships with hospitals.
Table 8 Analysis of intervening impacts of interests involved in the relationships of the supplier relationship category (II)
Main path Pharma company-Hospital-Physician-Pharmacist
Perspective Individual interests
Hospital • To themselves and physicians
Under financial stress, hospitals will regulate
physicians’ drug prescription, thus affecting
their drug prescribing attitude and behavior as well as their interactions with pharma companies.
Physician • To themselves, hospitals, and pharma
companies
Physicians conceive that hospitals will regulate their drug prescription due to financial stress, and the regulation may affect their drug prescribing attitude and behavior as well as their interactions with pharma companies. As a result, there may be changes of the sales service of pharma companies.
Pharmacist • To pharma companies
Pharmacists conceive that pharma companies will shift the focus of their sales service onto pharmacists.
Pharma company • To themselves, hospitals, and physicians
Pharma companies conceive that under
hospitals’ regulation and control on drug
prescription, physicians are deprived of the right to prescribe drugs independently, and their interactions with physicians are also affected. As a result, the focus of their sales service is shifted onto pharmacists.
Common source of impacts
In business network systems, actors have common interests and goals. Under mutualism, they interact in an interconnected network and autonomously operate to accumulate their own profits. Any actor or dyadic relation may be the source that activates a domino effect. Dynamics of a general industrial network are not triggered by impacts from a common source. As the health care system is a third-party payor system, there are professional and systemic norms that stakeholders need to follow, and a third party will regulate and affect all dyadic exchange behaviors in the system. As a result, stakeholders are unable to operate autonomously [15, 24]. Besides, the third party has a strong influence on the operation of the entire health care system. It may be the dominant player in the network system. It manipulates external environmental forces and controls actors involved activities, processes, and resources of the network structure [25]. Its influences are transmissible. They may spread across the entire network and dominate the operation of the entire system [26]. Therefore, unlike general industrial networks, the health care network involves a third party that dominates and influences the dynamics of the network, and it has normative influence on all actors in the network. Since this third party has control over and interferes with operations of all actors, it becomes a common source of intervening impacts of interests in the health care network system.
The analysis result suggests that among stakeholders of the health care system, DH/BNHI dominates operations of the entire system due to its role and power in collecting and allocating budget. Many respondents also mentioned about this phenomenon during the interview. The preceding analysis of intervening impacts of interests among stake-holders indicates that DH/BNHI is the source of all intervening impacts. DB/BNHI is not only an insurer that plans and executes the national health insurance policies but also a manager of the health care system. DB/BNHI has multiple and complicated responsibilities, which increase its influence on the operations of the health care system. When intervening in the operations of the health care system as an insurer, due to change of the payment method, DB/BNHI can slash the influence of“price” in the health care service market and further affect the behavior of patients, medical institutions, and employees. As a govern-ment agency, DB/BNHI can manage health care service providers by setting up various regulations and policies. Dominating key economic resources, DB/BNHI is a fund allocator. All actors in the health care system, despite holding varying levels of power, need to abide by the policies and regulations DB/BNHI has set up. These policies and regulations confine the actors’ behavioral models, making it impossible for them to operate autono-mously and independently.
As shown in the above tables, all relationship paths indicate that DH/BNHI is the ultimate source of intervening impacts among all stakeholders of the health care system. When asked to describe the intervening impacts of interests, all respondents mentioned that controls and regulations set up by DH/BNHI are the causes of indirect intervention by other actors in the connected network, and these controls and regulations have prevented them from achieving expected goals autonomously and motivated them to pursue their individual interests.
Conclusion
Summary of findings
This study adopts the network theory and stakeholder analysis to analyze exchange interactions and associa-tions among stakeholders of the health care system in Taiwan from holistic and multiple perspectives. The main findings are as follows: First, the health care system consists of multiple stakeholders, and there are multiple exchange interactions among them. All dyadic exchange relations between any two stakeholders cannot exist in isolation. They will affect or be affected by other actors or other dyadic relations in the system. The finding that all the three identified relationship portfolios are interconnected confirms that the health care system is a network type exchange system. Besides, unlike general business networks, the health care system is a network system that involves a third party, which regulates and affects all stakeholders in this system [15]. Subject to regulations on price, service items, and budget, stake-holders are unable to autonomously operate various marketing portfolios and the management system cannot operate by market mechanisms. This is the first finding of this paper:
Finding 1: The health care system in Taiwan is a regulated network type exchange system, in which a third party regulates all exchanges among stake-holders, and market mechanisms cannot suffi-ciently and autonomously operate.
Second, in this exchange network, inter-organizational relationships do not exist in isolation and will definitely be affected by other inter-organizational relationships. That is, exchange relationships are interconnected to a certain extent, and one exchange relationship is affected by another exchange relationship [18,27]. Besides, due to the fact that stakeholders of the health care system have heterogeneous interests, exchange interactions among stakeholders are affected by intervention and correlation of interests. As a result, many exchange characteristics have been
unveiled from the stakeholder perspective. This is the second finding of this paper:
Finding 2: The health care system involves multiple stakeholders pursuing varying interests. Be-cause these stakeholders are affected by intervention of interests, many of their ex-change characteristics are exposed.
The agreements must be made between actors in the network in order to achieve the particular objectives of the actors. This is also a characteristic of B to B relationships. Members in the network can pursue maximization of the accumulated system value with a common goal [28]. However, according to Ritter [18], resource limitations cause negative effects. An analysis of the Taiwanese public health system has revealed that both positive and negative exchange value effects affect the relationship among actors in the overall health system [20]. Subject to the control and regulation of a third party as well as the constraint of resources, stakeholders who pursue varying interests in nature are impacted by different interven-ing impacts of interests. In the health care system, all stakeholders operate with limited resources and pursue interests that are interconnected. Their competition for scarce resources exposes the nature that their interests are heteroge-neous and motivates them to pursue mainly individual interests. The findings from investigation of stakeholders’ opinions and perspectives indicate that, under intervention and correlation of interests, they are unable to operate toward their original goals and will pursue individual interests instead. Their attitude and behavior will also be oriented to the pursuit of individual interests. As a result, their original pursuit of common interests becomes just a formality and meaningless. This is the first characteristic of network exchanges in the health care system from the stakeholder perspective:
Finding 2-1: Under mutual intervention of interests, stake-holders in the health care system pursue common interests in appearance but individ-ual interests in reality.
Finally, findings from tracing the source of the impacts suggest that the third party in the system is the common source of impacts. This third party influences all stakeholders in the system using various professional and systemic regulations, making it impossible for them to operate autonomously. Because this third party is respon-sible for collection and allocation of all funds, it controls the most important resources in the system and dominates the operations and dynamics of the entire health care system. This is the second characteristic of network exchanges in the health care system from the stakeholder perspective:
Finding 2-2: In the health care system, impacts on stakeholder interests come from a common source, which is the third party that holds the most important resources in the system and dominates the operating models and dynamics of the entire system.
Research implications
This study adopted two theoretic perspectives which have never been used in combination in previous studies to examine the dynamic impacts of interactions between stakeholders in the health care system. One is the network theory perspective, and the other is the stakeholder perspective.
Network theory perspective
According to [29], all facets of a network system cannot be captured if it is examined from the perspective of individuals or dyadic relations rather than from the perspective of interactions between members. However, most previous studies on the health care system analyze operations of the medical system from the single-actor, dyad or consumer marketing theory (B to C) perspective. Many of their concerns of the medical system are biased, superficial or even out of focus. As a result, the core problems underlying the medical system can hardly be uncovered and clarified. Although Hu et al. [30] and Hu and Tsai [20] proposed propositions of network-type exchange systems through review and induction of literature or anatomized the relations in health care systems from the viewpoint of the network theory, their research was mainly based on discussion of theoretic concepts and lacking support of empirical evidence. In this paper, we adopt the network system concepts to analyze the internal operations of the health care system from the perspectives of the business marketing theory (B to B) and the consumer marketing theory (B to C). Moreover, through empirical and qualitative research, we have presented the facts that the health care system belongs to a network type exchange system.
Stakeholder perspective
Most previous studies on the health care system are based on a single perspective and overlook the fact that multiple stakeholders are involved in the health care system and their relations are complicated and interconnected. Therefore, many of their results cannot reflect the true facets of the health care system. For instance, some papers have examined physician
prescrip-tion behavior (PPB) as an impact of detailing activities of pharma salespersons (FLEs) and marketing mix variables deployed [31, 32]. These papers are focused only on the dyadic relations between physicians and pharma salespersons. Although the network connected aspect of the physician-salesperson dyad was emphasized in [33], the author still neglected the other collective actors in the network and investigated how to increase the effectiveness of their sales force in influencing PPB from the viewpoint of pharma companies. Liu et al. [34] integrated the network theories and stakeholder perspec-tive to examine the formation and management of the interaction network formed by stakeholders of the national health insurance policy. However, their research was based on decision-marker’s perspective and considerations of the public policy. Savage et al [22] and Dymond et al [35] analyzed the health care network system from stakeholder perspective. Their analyses were based on the viewpoint of USA Managed Care Organization with a focus on management of stakeholders. All the above-mentioned studies are confined to the single-actor or dyad analysis model. The stakeholders in the health care system are interactive and interconnected. Each stakeholder has a system of stakeholders that is also connected to the system of other stakeholders [36]. Moreover, stakeholders in the health care system have divergent concerns and inter-ests. Therefore, the conventional single-actor dyadic exchange view may not be able to reflect the true conditions of the health care system. Our adoption of the multi-stakeholder perspective highlights the network exchange characteristics of the health care system, revealing that conflicts and interconnectedness of inter-ests affect the internal operations and dynamics of the network. This finding has never been proposed in any of the extant studies on the health care system.
To sum up, we integrate the network theory and stakeholder perspective to analyze the exchange rela-tions in the health care system. Our findings suggest that the health care system is a network type exchange system and demonstrate the characteristics of network exchange between stakeholders. We transcend the conventional dyadic exchange view to construct a paradigm for analyzing a multiple exchange system involving multiple stakeholders.
Pratical implications
For medical policy makers, DH/BNHI should play the role of a coordinator rather than the role of a decision marker. Our findings show that the health care system is a network type exchange system. DH/BNHI should realize this fact so that they can formulate policies based on a comprehensive and systemic thinking model
rather than from a single or individual perspective. If not, they only deal with problems on an ad hoc basis, resulting in distortion of the system. Liu et al. [34] have mentioned that the nature of pluralism within a network cannot be ignored. By connecting people from different backgrounds, with different opinions and experiences, policy makers can derive creative ideas in the policy planning stage and obtain adequate resources for execu-tion of the policy.
Therefore, DH/BNHI should understand their appro-priate role and position in the health care system and realize that they should be the coordinator rather than simply the decision maker. In the policy formulation or execution stage, they should take into account the various opinions and concerns of multiple stakeholders and engage in coordination of their interests. They cannot make or execute decisions arbitrarily, because such action will only lead to conflicts and opposition between members in the system.
For managers of health institutions, their manage-ment of stakeholders should be based on cooperation, coordination, and pursuit of common interests rather than arbitrary control and limitation. Under the confines of the third party in the health care system, all stakeholders appear to pursue common goals and interests but are seeking individual interests in reality. Despite the goal of mutualism, these stakeholders’ interests will conflict with one another, affecting the management efficiency and performance of the organi-zation. To enhance the effectiveness of resource man-agement and maintain the health care service quality at a certain level, decision makers need to investigate the position and interests of each stakeholder and identify the stakeholder whose interests should be prioritized or set up coping strategies according to the objective position and subjective viewpoint of each individual stakeholder [37]. Besides, managers of health care service providers need to identify which stakeholders can cooperate and resolve conflicts rather than to control or reduce costs. Actions of cost control or reduction will only sustain existence of conflicts among stakeholders, making it impossible to maintain a long-term and balanced exchange relationship. The relationship be-tween hospital and pharma companies, for instance, affects job satisfaction of internal employees, such as physicians and pharmacists, and further affects perfor-mance of the organization and the overall health care quality. Therefore, management is no longer a decision-making process of a single stakeholder. The conventional authoritarian decision model should be replaced by cooperation, coordination, participation, and inclusion [37]. Decision makers should set up strategies in accordance with the interests of each stakeholder and
develop an interaction relationship management model to pursue performance and sustainability of the organization [38,39].
Limitations
Several possible limitations in this paper should be noted. First of all, primary data used in this paper were gathered through in-depth interview. Because our inter-view involved subjective opinions of stakeholders, such as weighting of importance of health care quality and financial performance, the responses of the participants would contain social desirability bias [40]. Besides, our interview also involved some sensitive issues that have been long existent in the medical industry. For instance, pharmaceutical price gap and legal issues are involved in the interactions among hospitals, physicians, and pharma companies. These issues might have prevented the respondents from providing truthful answers, causing a gap between interview data and reality. Secondly, despite our efforts to present the subjective values of the respondents using objective approaches in the qualitative analysis, we could hardly avoid involving our personal values in the analysis and generating some error of the results. Nonetheless, this is inevitable in qualitative research. Thirdly, to avoid this research from being out of focus due to adoption of a wide research scope, we focused only on the pharmacy service of the health care services and selected only stakeholders involved in the pharmacy service as research subjects in this paper. However, the service outputs and actors involved in this system are huge in quantity and complicated. Different services or diseases may involve different variables. Our limitation of the research scope to the pharmacy service might have neglected or missed many important facts existing in the network system. Finally, this paper uses the health care system in Taiwan as an example. The health care system in Taiwan is a close system. Physicians are hospital employees, so their behaviors are largely regulated and affected by hospital policies. Besides, unlike the US health insurance system, the system in Taiwan is a single payor system, which means that all health insurance policies are dominated by a single payor (DH/BNHI). Therefore, the results of this paper may not be generalizable to health care systems that belong to the open system or the multi-payor system.
Acknowledgement The authors would like to acknowledge the
funding for this research from Program of Grants for Research from China Medical University (CMU97-312) and hereby express their most sincere gratitude.
References
1. Hsu, S. F., Yang, Y. L., and Chen, H. C., Social dilemma? An equilibrium analysis of providers’ strategies under global budget. J. Manage. 24(2):155–166, 2007.
2. Wu, H. L., A look into medical and economic controls: From health insurance disputes. Econ. Outlook Bimonthly 46–56, 2008.
3. Wang, H. L., Kwan, A. L., Hsiao, Y. C., and Huang, J. Y., The study of the attitude toward medicine practice by physician: Managers performed hospital global budget system in Taiwan. J.
Healthc. Manag. 8(4):317–337, 2007.
4. Huang, K. C., Cheng, Y. H., Chang, H. C., Cheng, W. J., Wen, H. C., and Chiu, C. H., Adaptation strategies of hospitals under the global budget system. Taiwan Journal of Public Health 26
(40):283–291, 2007.
5. Gillies, R. R., Shortell, S. M., Anderson, D. A., Mitchell, J. B., and Morgan, K. L., Conceptualizing and measuring integration: Finding from the health systems integration study. J. Healthc. Manag. 38(4):467, 1993.
6. Wu, C. Q., and Yeh, S. C. J., The current situation and review of National Health Insurance. Taiwan Medical Journal 44(5):55, 2001. 7. Achrol, R. S., Changes in the theory of interorganizationl relations
in marketing: Toward a network paradigm. J. Acad. Mark. Sci. 25 (1):56–71, 1997.
8. Shortell, S. M., Remaking health care in America: the evolution of organized delivery systems, 2nd edition. Jossey-Bass, San Francisco, 2000.
9. Satinsky, M. A., The foundations of integrated care: facing the challenges. American Hospital Publishing, 1998.
10. Lin, B. Y. J., Lin, Y. K., and Lin, C. C., Partnership effectiveness in primary community care networks (PCCNs): A National empirical analysis of partners' coordination infrastructure designs.
Health Care Manage. Rev. 35(3):224–234, 2010.
11. Lin, B. Y. J., and Wan, T. T. H., Creating value for health care organizations: a guide toward successful integrated care. Yeh Yeh Book Gallery, Taipei, 2003.
12. Chang, L. Y., Medicine and sociology. Ju-Liu, Taipei, 2003. 13. Persson, S. G., and Steinby, C., Networks in a protected business
context: Licenses as restraints and facilitators. Ind. Mark. Manage. 35:870–880, 2006.
14. Lu, R. J. F., and Shieh, C. R., Health economics. Proedp, Taipei, 2000. 15. Kotler, P., and Clarke, P. N., Marketing for health care
organizations. Prentice-Hall, Englewood Cliffs, 1987.
16. Salmi, A., Entry into turbulent business networks. The case of a Western company in the Estonian market. Eur. J. Mark. 34(11/
1):1374–1390, 2000.
17. Mattsson, L. G., Industrial marketing. The network perspective. In: Backhaus, K., and Voeth, M. (Eds.), Handbuch Industriegü-termarketing. Gabler Verlag, München, 2004.
18. Ritter, T., A framework for analyzing interconnectedness of
relationships. Ind. Mark. Manage. 29:317–326, 2000.
19. Anderson, J. C., Håkansson, H., and Johanson, J., Dyadic business relationships within a business network context. J. Mark.
58:1–15, 1994.
20. Hu, J. S., and Tsai, Y. F., Paradigms of exchange value effect in market network. Ind. Mark. Manage. 36:636–650, 2007. 21. Morgan, R. M., and Hunt, S. D., The commitment-trust theory of
relationship marketing. J. Mark. 58:20–38, 1994.
22. Savage, G. T., Taylor, R. L., Rotarius, T. M., and Buesseler, J. A., Governance of integrated delivery systems/networks: A
stakeholder approach. Health Care Manag. Rev. 22(1):7–20,
1997.
23. Yin, R. K., Case study research: design and methods, 3rd edition. Sage, Thousand Oaks, 2003.
24. Hu, J. S., Marketing challenges in future business environment. 2002 Enterprise Knowledge Management and Innovation Conference. Knowledge Economy Association in Taiwan, 2002.
25. Gupta, S., Polonsky, M., Woodside, A., and Webster, C. M., The impact of external forces on cartel network dynamics: Direct research in the diamond industry. Ind. Mark. Manage. 39:202– 210, 2010.
26. Johnston, W. J., Lewin, E., and Spekman, R. E., International industrial marketing interactions: Dyadic and network perspective.
J. Bus. Res. 46:259–271, 1999.
27. Ritter, T., and Gemunden, H. G., Interorganizational relationships
and networks: An overview. J. Bus. Res. 56:691–697, 2003.
28. Lenney, P., and Easton, G., Actors, resources, activities and
commitments. Ind. Mark. Manage. 38:553–561, 2009.
29. Johnston, W. J., Peters, L. D., and Gassenheimer, J., Questions about network dynamics: Characteristics, structures, and
inter-actions. J. Bus. Res. 59:945–954, 2006.
30. Hu, J. S., Yang, W. H., and Chou, Y. Y., Classifying healthcare network relationships: An analysis with recommendations for
managers. Int. J. Manag. 23(4):665–678, 2006.
31. Gonul, F., Carter, F., Petrova, E., and Srinivasan, K., Promotion of prescription drugs and its impact on physicians choice behavior. J. Mark. 65:79–90, 2001.
32. Manchanda, P., and Chintagunta, P. K., Responsiveness of physician prescription behaviour to salesforce effort: An individual level analysis. Mark. Lett. 15(2–3):129–145, 2004.
33. Singh, R., Network connectedness of pharmaceutical sales rep (FLE)-physician dyad and physician prescription behavior: A
conceptual model. J. Med. Marketing 8(3):257–268, 2008.
34. Liu, I. C., Chen, D. Y., Hsiao, N. Y., and Lin, C. Y., The application of network analysis in the concept of stakeholders: A case study of national health insurance policy reform in Taiwan. Taiwanese Journal of Social Welfare 4(1):95–130, 2005. 35. Dymond, S., Nix, W. T., Rotarius, M. T., and Savage, T. G., Why
do key integrated delivery stakeholder really matter? Assessing control, coalitions, resources and power. Med. Group Manage. J.
42(6):26–38, 1995.
36. Vandekerckhove, W., and Dentchev, A. N., A network perspective on stakeholder management: Facilitating entrepreneurs in the
discovery of opportunities. J. Bus. Ethics 60:221–232, 2005.
37. Pestoff, V. A., Control and multi-stakeholder organizational. In: Aldershot UK, Brookfield Vt (Eds.), Beyond the Market and State: Social Enterprises and Civil Democracy in a Welfare
Society. Sydney: Ashgate, 106–127, 1998.
38. Preble, J. F., Toward a comprehensive model of stakeholder
management. Bus. Soc. Rev. 110(4):407–431, 2005.
39. Greenley, G. E., Hooley, G. J., and Rudd, J. M., Market orientation in a multiple stakeholder orientation context: Implica-tions for marketing capabilities and assets. J. Bus. Res. 58:1483– 1494, 2005.
40. Neuman, W. L., Social research methods: qualitative and quanti-tative approaches, 5th edition. Allyn and Bacon, Boston, 2002.