電針合併中藥萃取物治療肺癌的抗腫瘤效應之研究; The anti-cancer effects of electro-acupuncture combined with Chinese herbal extract in lung carcinoma
73
0
0
全文
(2)
(3)
(4) Index Figures and Tables Index……….……………………………vii Abstract………………………………………..........................ix Chinese abstract…………………………………......................x Abbreviation…………………………………...........................xi Chapter 1. Introduction……………………………..............1. Chapter 2. Articles review…………………………...............3. 1. Database of Lung cancer Classification of Lung cancer…………………………...……...3 Genetics of Lung cancer……………………………...………...5 Diagnosis of Lung cancer………………………………...…….6 Treatment of Lung cancer………………………………………7 2. Database of Acupuncture Acupuncture ----a new strategy in cancer treatment………......12 Electroacupuncture---improving body immunity in cancer patients………………………………………………………...13 Zusanli (ST-36) ---a most useful acupuncture point…………..15 3. Database of Honokiol Anti-tumorigenic activities………...………………………….18 iv.
(5) Neurotrophic activity………………..………..…………….....18 Anti-thrombolytic activity………………………………..…...18 Chapter 3. Materials and Method………………................21. 1. Materials………………………………….………………………21 2. Methods…………………………………………………….……..21 Cell culture…………………………………………………….21 MTT assay…………………………...……………..…………21 Quantification of apoptosis by flow cytometry………...……..22 Western blot analysis………………..………………………...23 Caspase activity………………..……………………………...23 In vivo tumor xenograft study..…………………………….....24 Meridian Selection………………..…………………………...25 Operation of ST 36 electrical-acupuncture in mice…………...26 Electro-acupuncture protocol………………………………….27 Grouping………………………………………………………28 BLI Procedure and Image Analysis…………………………...29 Pathological analysis………………………………………….30 Statistics……………………………………………………….31 Chapter 4 :. Results………………………….........................32 v.
(6) Honokiol induced cell apoptosis in human lung cancer cells....32 Electroacupuncture combined with intraperitoneal injection of Honokiol inhibits tumour growth in the mouse xenograft model of A549 cell...............................................................................32 Electroacupuncture and Honokiol prevent body weight loss in the mouse xenograft model of A549 cells………….................33 Pathological findings of A549 cell xenografts..........................33 Honokiol induces mitochondrial-dependent apoptosis and electroacupuncture could amplify the effect…………………..34 Chapter 5 : Discussion………………………….…..............35 Chapter 6 :. Conclusion……………………………………..37. Figures collection………………………………....………….38 Reference……………………………….................…………..51 Acknowledgement……………………….................…………61. vi.
(7) Figures and Tables Index Table.1. Frequency of histological types of lung cancer…………….….3. Table.2. Sub-types of non-small cell lung cancer in smokers and. never-smokers………………………………………………………….....4 Fig. 1. The molecular structure of Honokiol………………………….18. Fig. 2. Yellow MTT is reduced to purple formazan…………………..22. Fig. 3. A549 cells were injected subcutaneously into the flanks and. measured once a week with a caliper…………………………………...25 Fig. 4 The mice anesthetized and acupuncture procedure…………….27 Fig. 5 Electro-acupuncture grouping and experiment flow chart……..29 Fig. 6 IVIS system…………………………………………………….30 Fig. 7. Honokiol induced the apoptosis of human lung cancer cells. (MTT assay)…………………………..………………………………...38 Fig. 8. Honokiol induced the apoptosis of human lung cancer cells. (annexin V/PI double staining)……………………...…………………..39 Fig. 9. Honokiol induced the apoptosis of human lung cancer cells. (TUNEL method)…………………………………………..…………...40 Fig. 10. Honokiol induces apoptosis by triggering the mitochondrial. apoptotic pathway……………………………………………………….41 Fig. 11. Honokiol induces the activation of caspase-3 in A549 cells…42. Fig. 12. Honokiol induced the implanted tumor of human lung cancer. cells significantly reduced after 2 and 3 weeks…………………………43 Fig. 13 Honokiol induced the implanted tumor of human lung cancer cells significantly reduced in the end of experiment……………………44 Fig. 14. The specimens in the different groups………………………..45 vii.
(8) Fig. 15. The weights of the implanted tumor were significantly reduced. in HK group and EA+HK group………………………………………..46 Fig. 16 Electroacupuncture and Honokiol may prevent body weight loss in the mouse xenograft model of A549 cells……………………………47 Fig. 17. Comparison 4 groups in the structural changes of A549 cells. displayed by H&E stain ×400…………………………………………...48 Fig. 18 Honokiol induces mitochondrial-dependent apoptosis in A549 cells xenograft model……………………………………………………49 Fig. 19. Honokiol induces apoptosis via caspase3 and cytochrome C. mediated in A549 cells xenograft model………………………………..50. viii.
(9) Abstract Non-small cell lung cancer is a affects approximately 80% of all lung malignant primary tumor that responds poorly to both chemotherapy and radiation therapy. In the present study, we investigated the anticancer effect of a honokiol, an active component isolated and purified from the Magnolia officinalis in human lung cells. Honokiol induced cell apoptosis in human lung cancer cell lines (A549 cell). Honokiol also induces upregulation of Bax and Bak, downregulation of Bcl-XL and dysfunction of mitochondrial in lung cancer cells. Importantly, animal studies have revealed a dramatic reduction in tumor volume after 21 days of treatment. Besides, electroacupuncture zusanli acupoint (ST36) combined with intraperitoneal injection of Honokiol inhibits tumour growth in the mouse xenograft model of A549 cells. This study demonstrates that honokiol may be a novel anticancer agent for the treatment of lung cancer cells and electroacupuncture could amplify the chemo-therapeutic effect in lung cancer treatment.. Key words: Honokiol, ST36, non-small cell lung cancer, apoptosis. ix.
(10) Chinese Abstract 非小細胞肺癌大約站肺部的原發性惡性腫瘤的 80%,而且一般被認 為這些患者對化學治療與放射治療沒有很好的反應,手術開刀的五年 存活率也大約僅有 40%左右。在本實驗中,我們探討從木蘭科植物厚 朴中純化分離出的淬取物---和厚朴酚(honokiol)之對抗人類肺癌細胞 的效應。經由我們的實驗發現,和厚朴酚將會誘發人類肺癌細胞(A549 cell)的細胞凋亡,另外和厚朴酚也會使得肺癌細胞(A549 cell)粒線體 的作用改變,以及粒線體上 Bax and Bak 蛋白的向上調控,Bcl-XL 蛋 白的向下調控。更重要的,在肺癌細胞荷瘤動物模型之實驗中,我們 給予免疫抑制小鼠連續 21 天的腹膜內注射和厚朴酚(1.5 mg/kg),結 果顯示很明顯的腫瘤抑制效應。除此之外,我們也同給予使用電針足 三里(2 Hz)以及電針足三里(2 Hz)合併連續 21 天的腹膜內注射和厚朴 酚的兩組實驗,此實驗發現合併電針足三里與腹膜內注射和厚朴酚比 單純給和厚朴酚的腫瘤抑制率更高,而單純電針足三里並未能使腫瘤 抑制。因此,本實驗闡明了和厚朴酚是在治療肺癌上一新興的抗癌藥 物,而電針足三里將會加成擴大和厚朴酚抗癌的化學效應。. 關鍵字:和厚朴酚、足三里、非小細胞肺癌、細胞凋亡. x.
(11) Abbreviation NSCLC. non-small cell lung carcinoma. SCLC. small cell lung carcinoma. CT. computed tomography. EGFR. epidermal growth factor receptor. PET. positron emission tomography. VATS. Video-assisted thoracoscopic surgery. CHART. continuous hyperfractionated accelerated radiotherapy. PCI. prophylactic cranial irradiation. EGF-R. epidermal growth factor receptor. TCM. traditional Chinese medicine. NCCAM. National Center for Complementary and Alternative Medicine. NIH. National Institutes of Health. AMA. American Medical Association. PENS. Percutaneous Electrical Nerve Stimulation. EA. electro-acupuncture. GI. gastrointestinal xi.
(12) MAPK. mitogen-activated protein kinase. NF-κB. nuclear factor kappa B. VEGF. vascular endothelial growth factor. COX-2. cyclooxygenase 2. PS. phosphatidylserine. PI. Propidium iodine. TUNEL. Terminal deoxynucleotidyl transferase dUTP nick end labeling. PVDF. Immobilon polyvinyldifluoride. HK. Honokiol. IL-2. Interleukin 2. NK cell. Natural killer cell. H&E. hematoxylin-eosin. ANOVA. analysis of variance. xii.
(13) Chapter 1. Introduction. Lung cancer, the most common cause of cancer-related death in men and the second most common in women (after breast cancer)[1], is responsible for 1.3 million deaths worldwide annually.[2] The main types of lung cancer are small cell lung carcinoma and non-small cell lung carcinoma. This distinction is important, because the treatment varies; non-small cell lung carcinoma (NSCLC) is sometimes treated with surgery, while small cell lung carcinoma (SCLC) usually responds better to chemotherapy and radiation.[3] Lung cancer may be seen on chest radiograph and computed tomography (CT scan). The diagnosis is confirmed with a biopsy. This is usually performed via bronchoscopy or CT-guided biopsy. Treatment and prognosis depend upon the histological type of cancer, the stage (degree of spread), and the patient's performance status. Possible treatments include surgery, chemotherapy, and radiotherapy. With treatment, the five-year survival rate is 14%.[4] Although chemotherapy may, in the near future, be shown to produce promising results as neo-adjuvant and adjuvant strategies for early-stage patients and some progress has been made in the treatment of locally-advanced and advanced disease, treatment outcomes for NSCLC are still to be considered disappointing[5, 6]. Clinical research of new treatment strategies is warranted. Advances in the knowledge of tumor biology and mechanisms of oncogenesis have granted the singling out of several molecular targets for NSCLC treatment [7]. Therefore, it is important to explore a novel and adequate remedy. In my master time, I make efforts for the anti-cancer and anti-metastasis effects of new strategies in lung carcinoma. 1.
(14) Honokiol, a small molecular weight natural product, has been shown to possess potent anti-neoplastic and anti-angiogenic properties. Although the effects of Honokiol-induced tumor apoptosis have been studied in some cancers, the role of Honokiol in the process of cell apoptosis in lung cancer cell remains largely unknown. To the best of our knowledge, this study is the first to attempt to determine the apoptosis activity of Honokiol in human lung cancer cell lines and antitumor activity against human lung cancer in xenograft model[8-10]. Acupuncture, an ancient form of medicine that originated in China, is one of the most effective alternative medical treatments with the advantages of simple application, low cost and minimal side effects. The immunomodulatory effect of Zusanli (ST 36) acupoint was reported in many studies. We combined ST-36 electroacupuncture with intraperitoneal injection of Honokiol in male nude mice. Our data would provide that Honokiol group and combining group reduced cells survival and tumor growth in human lung cancer cells in vitro and in vivo. The present study would be designed to determine whether Honokiol has the antitumor activity against human lung cancer as well as potentiates the antitumor activity of ST-36 electroacupuncture in A549 lung cancer xenograft model, if so, to examine the possible mechanism in the phenomenon, and to provide some potential implications for the treatment of human lung cancer.. 2.
(15) Chapter 2. Articles review. 1. Database of Lung cancer Classification of Lung cancer The vast majority of lung cancer are carcinomas—malignancies that arise from epithelial cells. There are two main types of lung carcinoma, categorized by the size and appearance of the malignant cells seen by a histopathologist under a microscope: non-small cell (80.4%) and small-cell (16.8%) lung carcinoma[2]. This classification, based on histological criteria, has important implications for clinical management and prognosis of the disease. Table.1. Frequency of histological types of lung cancer. Histological type. Frequency (%). Non-small cell lung carcinoma. 80.4. Small cell lung carcinoma. 16.8. Carcinoid. 0.8. Sarcoma. 0.1. Unspecified lung cancer. 1.9. Non-small cell lung carcinoma (NSCLC) The non-small cell lung carcinomas are grouped together because their prognosis and management are similar. There are three main sub-types: squamous cell lung carcinoma, adenocarcinoma, and large cell lung carcinoma. 3.
(16) Table.2 Sub-types of non-small cell lung cancer in smokers and never-smokers Frequency of non-small cell lung cancers (%) Histological sub-type. Smokers. Never-smokers. Squamous cell lung carcinoma. 42. 33. 39. 35. 4. 10. Carcinoid. 7. 16. Other. 8. 6. Adenocarcinoma (not Adenocarcinoma. otherwise specified) Bronchioloalveolar carcinoma. Accounting for 31.2% of lung cancers, squamous cell lung carcinoma usually starts near a central bronchus. A hollow cavity and associated necrosis are commonly found at the center of the tumor. Well-differentiated squamous cell lung cancers often grow more slowly than other cancer types.[3] Adenocarcinoma accounts for 29.4% of lung cancers.[11] It usually originates in peripheral lung tissue. Most cases of adenocarcinoma are associated with smoking; however, among people who have never smoked ("never-smokers"), adenocarcinoma is the most common form of lung cancer. A subtype of adenocarcinoma, the bronchioloalveolar carcinoma, is more common in female never-smokers, and may have different responses to treatment. Small cell lung carcinoma (SCLC) 4.
(17) Small cell lung carcinoma (SCLC, also called "oat cell carcinoma") is less common. It tends to arise in the larger airways (primary and secondary bronchi) and grows rapidly, becoming quite large. The "oat" cell contains dense. neurosecretory. granules. (vesicles. containing. neuroendocrine. hormones), which give this an endocrine/paraneoplastic syndrome association. While initially more sensitive to chemotherapy, it ultimately carries a worse prognosis and is often metastatic at presentation. Small cell lung cancers are divided into limited stage and extensive stage disease. This type of lung cancer is strongly associated with smoking.[12] Genetics of Lung cancer Similar to many other cancers, lung cancer is initiated by activation of oncogenes or inactivation of tumor suppressor genes.[13] Oncogenes are genes that are believed to make people more susceptible to cancer. Proto-oncogenes are believed to turn into oncogenes when exposed to particular carcinogens.[14] Mutations in the K-ras proto-oncogene are responsible for 10–30% of lung adenocarcinomas.[15, 16] The epidermal growth factor receptor (EGFR) regulates cell proliferation, apoptosis, angiogenesis, and tumor invasion.[15] Mutations and amplification of EGFR are common in non-small cell lung cancer and provide the basis for treatment with EGFR-inhibitors. Her2/neu is affected less frequently.[15] Chromosomal damage can lead to loss of heterozygosity. This can cause inactivation of tumor suppressor genes. Damage to chromosomes 3p, 5q, 13q, and 17p are particularly common in small cell lung carcinoma. The p53 tumor suppressor gene, located on chromosome 17p, is affected in 60-75% of cases.[59] Other genes that are often mutated or amplified are c-MET, NKX2-1, LKB1, PIK3CA, and BRAF.[15]. 5.
(18) Several genetic polymorphisms are associated with lung cancer. These include polymorphisms in genes coding for interleukin-1,[17] cytochrome P450,[18] apoptosis promoters such as caspase-8[19], and DNA repair molecules such as XRCC1.[20] People with these polymorphisms are more likely to develop lung cancer after exposure to carcinogens. Diagnosis of Lung cancer Performing a chest radiograph is the first step if a patient reports symptoms that may be suggestive of lung cancer. This may reveal an obvious mass, widening of the mediastinum (suggestive of spread to lymph nodes there), atelectasis (collapse), consolidation (pneumonia), or pleural effusion. If there are no radiographic findings but the suspicion is high (such as a heavy smoker with blood-stained sputum), bronchoscopy and/or a CT scan may provide the necessary information. Bronchoscopy or CT-guided biopsy is often used to identify the tumor type.[3] Sputum atypia is associated with an increased risk of lung cancer. Sputum cytologic examination combined with other screening examinations may play an important role in the early detection of lung cancer.[21]. 6.
(19) Treatment of Lung cancer Treatment for lung cancer depends on the cancer's specific cell type, how far it has spread, and the patient's performance status. Common treatments include surgery, chemotherapy, and radiation therapy.[3] Surgery If investigations confirm lung cancer, CT scan and often positron emission tomography (PET) are used to determine whether the disease is localized and amenable to surgery or whether it has spread to the point where it cannot be cured surgically. Blood tests and spirometry (lung function testing) are also necessary to assess whether the patient is well enough to be operated on. If spirometry reveals poor respiratory reserve (often due to chronic obstructive pulmonary disease), surgery may be contraindicated. Surgery itself has an operative death rate of about 4.4%, depending on the patient's lung function and other risk factors.[22] Surgery is usually only an option in non-small cell lung carcinoma limited to one lung, up to stage IIIA. This is assessed with medical imaging (computed tomography, positron emission tomography). A sufficient preoperative respiratory reserve must be present to allow adequate lung function after the tissue is removed. Procedures include wedge resection (removal of part of a lobe), segmentectomy (removal of an anatomic division of a particular lobe of the lung), lobectomy (one lobe), bilobectomy (two lobes), or pneumonectomy (whole lung). In patients with adequate respiratory reserve, lobectomy is the preferred option, as this minimizes the chance of local recurrence. If the patient does not have enough functional lung for this, wedge resection may 7.
(20) be performed.[23] Radioactive iodine brachytherapy at the margins of wedge excision may reduce recurrence to that of lobectomy.[24] Video-assisted thoracoscopic surgery and VATS lobectomy have allowed for minimally invasive approaches to lung cancer surgery that may have the advantages of quicker recovery, shorter hospital stay and diminished hospital costs.[25] Chemotherapy Small cell lung carcinoma is treated primarily with chemotherapy and radiation, as surgery has no demonstrable influence on survival. Primary chemotherapy is also given in metastatic non-small cell lung carcinoma. The combination regimen depends on the tumor type. Non-small cell lung carcinoma is often treated with cisplatin or carboplatin, in combination with gemcitabine, paclitaxel, docetaxel, etoposide, or vinorelbine. In small cell lung carcinoma, cisplatin and etoposide are most commonly used. Combinations with carboplatin, gemcitabine, paclitaxel, vinorelbine, topotecan, and irinotecan are also used.[26] in extensive-stage small-cell lung cancer celecoxib may safely be combined with etoposide, this combination showed improve outcomes.[27] Adjuvant chemotherapy for NSCLC Adjuvant chemotherapy refers to the use of chemotherapy after surgery to improve the outcome. During surgery, samples are taken from the lymph nodes. If these samples contain cancer, the patient has stage II or III disease. In this situation, adjuvant chemotherapy may improve survival by up to 15%. Standard practice is to offer platinum-based chemotherapy (including either cisplatin or carboplatin).[28] 8.
(21) Adjuvant chemotherapy for patients with stage IB cancer is controversial, as clinical trials have not clearly demonstrated a survival benefit.[29] Trials of preoperative chemotherapy (neoadjuvant chemotherapy) in resectable non-small cell lung carcinoma have been inconclusive. Radiotherapy Radiotherapy is often given together with chemotherapy, and may be used with curative intent in patients with non-small cell lung carcinoma who are not eligible for surgery. This form of high intensity radiotherapy is called radical radiotherapy.[30] A refinement of this technique is continuous hyperfractionated accelerated radiotherapy (CHART), in which a high dose of radiotherapy is given in a short time period.[31] For small cell lung carcinoma cases that are potentially curable, chest radiation is often recommended in addition to chemotherapy. The use of adjuvant thoracic radiotherapy following curative intent surgery for non-small cell lung carcinoma is not well established and is controversial. Benefits, if any, may only be limited to those in whom the tumor has spread to the mediastinal lymph nodes.[32] For both non-small cell lung carcinoma and small cell lung carcinoma patients, smaller doses of radiation to the chest may be used for symptom control (palliative radiotherapy). Unlike other treatments, it is possible to deliver palliative radiotherapy without confirming the histological diagnosis of lung cancer. Brachytherapy (localized radiotherapy) may be given directly inside the airway when cancer affects a short section of bronchus. It is used when inoperable lung cancer causes blockage of a large airway.[33]. 9.
(22) Patients with limited stage small cell lung carcinoma are usually given prophylactic cranial irradiation (PCI). This is a type of radiotherapy to the brain, used to reduce the risk of metastasis. More recently, PCI has also been shown to be beneficial in those with extensive small cell lung cancer. In patients whose cancer has improved following a course of chemotherapy, PCI has been shown to reduce the cumulative risk of brain metastases within one year from 40.4% to 14.6%.[34] Recent improvements in targeting and imaging have led to the development of extracranial stereotactic radiation in the treatment of early-stage lung cancer. In this form of radiation therapy, very high doses are delivered in a small number of sessions using stereotactic targeting techniques. Its use is primarily in patients who are not surgical candidates due to medical comorbidities.[35] Interventional radiology Radiofrequency. ablation. should. currently. be. considered. an. investigational technique in the treatment of bronchogenic carcinoma. It is done by inserting a small heat probe into the tumor to kill the tumor cells.[36] Targeted therapy In recent years, various molecular targeted therapies have been developed for the treatment of advanced lung cancer. Gefitinib (Iressa) is one such drug, which targets the tyrosine kinase domain of the epidermal growth factor receptor (EGF-R), expressed in many cases of non-small cell lung carcinoma. It was not shown to increase survival, although females, Asians, nonsmokers, and those with bronchioloalveolar carcinoma appear to derive the most benefit from gefitinib.[37] 10.
(23) Erlotinib (Tarceva), another tyrosine kinase inhibitor, has been shown to increase survival in lung cancer patients[38] and has recently been approved by the FDA for second-line treatment of advanced non-small cell lung carcinoma. Similar to gefitinib, it also appeared to work best in females, Asians, nonsmokers, and those with bronchioloalveolar carcinoma.[37] The angiogenesis inhibitor bevacizumab, (in combination with paclitaxel and carboplatin), improves the survival of patients with advanced non-small cell lung carcinoma.[39] However, this increases the risk of lung bleeding, particularly in patients with squamous cell carcinoma. Advances in cytotoxic drugs, pharmacogenetics and targeted drug design show promise. A number of targeted agents are at the early stages of clinical research, such as cyclo-oxygenase-2 inhibitors, the apoptosis promoter exisulind, proteasome inhibitors, bexarotene,[40] and vaccines.[41] Future. areas. of. research. include. ras. proto-oncogene. inhibition,. phosphoinositide 3-kinase inhibition, histone deacetylase inhibition, and tumor suppressor gene replacement.[42] The differential diagnosis for patients who present with abnormalities on chest radiograph includes lung cancer as well as nonmalignant diseases. These include infectious causes such as tuberculosis or pneumonia, or inflammatory conditions such as sarcoidosis. These diseases can result in mediastinal lymphadenopathy or lung nodules, and sometimes mimic lung cancers. Lung cancer can also be an incidental finding: a solitary pulmonary nodule (also called a coin lesion) on a chest radiograph or CT scan taken for an unrelated reason.[4]. 11.
(24) 2. Database of Acupuncture Acupuncture ----a new strategy in cancer treatment Acupuncture is an ancient form of medicine that originated in China, which has been practiced for over 2000 years. It is one of the most effective alternative medical treatments with the advantages of simple application, low cost and minimal side effects[43, 44]. Acupuncture is a technique of inserting and manipulating fine filiform needles into specific points on the body to relieve pain or for therapeutic purposes.[45] The word acupuncture comes from the Latin acus, "needle", and pungere, "to prick". In Standard Mandarin, 針砭 (zhēn biān) (a related word, 針灸 (zhēn jiǔ), refers to acupuncture together with moxibustion).. According to traditional Chinese medical theory, acupuncture points are situated on meridians along which qi, the vital energy, flows. There is no known anatomical or histological basis for the existence of acupuncture points or meridians.[46] Modern acupuncture texts present them as ideas that are useful in clinical practice.[47] According to the NIH consensus statement on acupuncture, these traditional Chinese medical concepts "are difficult to reconcile with contemporary biomedical information but continue to play an important role in the evaluation of patients and the formulation of treatment in acupuncture."[46] 12.
(25) The earliest written record that is available about acupuncture is Huangdi Neijing (黃帝內經 or Yellow Emperor's Inner Canon), which suggests acupuncture originated in China and would explain why it is most commonly associated with traditional Chinese medicine (TCM). Different types of acupuncture (Classical Chinese, Japanese, Tibetan, Vietnamese and Korean acupuncture) are practiced and taught throughout the world.[48] Acupuncture has been the subject of active scientific research since the late 20th century[48] but it remains controversial among Western medical researchers and clinicians.[48] Due to the invasive nature of acupuncture treatments, it is difficult to create studies that use proper scientific controls[46, 48]. Some scholarly reviews have concluded that the effectiveness of acupuncture as a treatment can be explained primarily through the placebo effect [49], while other studies have suggested some efficacy in the treatment of specific conditions.[48, 50] The World Health Organization published a review of controlled trials using acupuncture and concluded it was effective for the treatment of 28 conditions and there was evidence to suggest it may be effective for several dozen more. Additionally, the National Center for Complementary and Alternative Medicine (NCCAM) of the National Institutes of Health (NIH), the American Medical Association (AMA) and various government reports have studied and commented on the efficacy (or lack thereof) of acupuncture. There is general agreement that acupuncture is safe when administered by well-trained practitioners. using. sterile. needles,. and. that. further. research. is. appropriate.[51, 52] Electroacupuncture ---improving body immunity in cancer patients Electroacupuncture is a form of acupuncture in which pairs of acupuncture needles are attached to a device that generates continuous 13.
(26) electric pulses between them. Another term is Percutaneous Electrical Nerve Stimulation (PENS). According to some acupuncturists, this practice augments the use of regular acupuncture, can restore health and well-being, and is particularly good for treating pain. For the most part, there is insufficient scientific evidence regarding the safety or efficacy of electroacupuncture, although there is evidence for its efficacy in treating post-chemotherapy vomiting not for acute or delayed nausea severity. The Medical Letter on Drugs and Therapeutics advises doctors to tell their patients that devices used for electroacupuncture and electro interstitial scanning "lack a scientifically plausible rationale and should be regarded as bogus."[53]. Electroacupuncture is quite similar to traditional acupuncture in that the same points are stimulated during treatment. As with traditional acupuncture, needles are inserted on specific points along the body. The needles are then attached to a device that generates continuous electric pulses using small clips. These devices are used to adjust the frequency and intensity of the impulse being delivered, depending on the condition being treated [54]. 14.
(27) Electroacupuncture uses two needles at time so that the impulses can pass from one needle to the other. Several pairs of needles can be stimulated simultaneously, usually for no more than 30 minutes at a time." According to the principles of traditional Chinese medicine, illness is caused when qi does not flow properly throughout the body. Acupuncturists determine whether qi is weak, stagnant or otherwise out of balance, which indicates the points to be stimulated. Electroacupuncture is considered to be especially useful for conditions in which there is an accumulation of qi, such as in chronic pain syndromes, or in cases where the qi is difficult to stimulate." Electroacupuncture is also variously termed EA, electro-acupuncture or incorporated under the generic term electrotherapy. The above description does not reflect the full scope of practice nor application of electroacupuncture. While application of electrical currents to specific acupuncture points is used as an alternative to stimulating these areas of the body (instead of using manual manipulation techniques), practitioners also apply electroacupuncture using a neurophysiological model. In this approach, the same practitioners that use traditional acupuncture points, will also incorporate mapping of neuronal pathways, cutaneous and spinal distributions, to bring about a therapuetic response. In addition to pain, electroacupuncture may be used to treat musculoskeletal trauma and muscle dysfunction, over-use injuries (tendinitis or RSI), spasms and sprains.[53] Zusanli (ST-36) ---a most useful acupuncture point Zusanli is one of the most frequently used of all acupuncture points and is certainly the most intensively studied single point treatment in acumoxa therapy. The indications for use of this acupuncture point are many, and the claimed benefits are substantial. Many proposals for acupuncture research in 15.
(28) the West rely upon complex treatment protocols involving several acupuncture points; single-point acupuncture research to confirm Chinese reports is rare. If one wishes to demonstrate that acupuncture is therapeutically beneficial, and to do so with a simple treatment that is easily reproduced, needling zusanli seems most appropriate. While many acupuncturists would prefer, on the basis of their training, to administer a more complex treatment, few can deny that the proclaimed benefits of treating this point, even alone, are worthy of investigation. There have been two main directions taken in modern clinical research with treatment at zusanli. One is the treatment of abdominal pain and spasm, usually affecting the stomach, gallbladder, or kidney. In this case, stimulation of the acupuncture point is reported to have immediate effects (within seconds or minutes) and patients often receive only one treatment. These reports are presented first. The other is the treatment of impaired immune functions, especially deficits in leukocyte and immunoglobulin production. In this case, stimulation of the acupuncture point is carried out daily, usually for 10–14 days consecutively, and this course of therapy might be repeated (sometimes after a short break of a few days). One of the studies mentioned below combines these two areas of concern: treatment of cancer patients suffering from abdominal pain (cancer patients usually have impaired immune functions, either spontaneously or as the result of medical therapies). Electroacupuncture (EA) is widely applied in clinical practice and is becoming more recognized worldwide. Not only do domestic medical institutions offer the full range of EA treatments, but international institutions have also done much research concerning its mechanisms. The understanding of this treatment has had tremendous breakthroughs, particularly in the areas of biochemistry, hematology, and nerve physiology. 16.
(29) Acupuncture has been used for pain relieving, decreasing drug side-effect, improving body immunity in cancer patients, Acupuncture point (acupoint) of ST-36 is one of the most effective points, with a wide range of effects for analgesia immunity[55, 56], homeostasis and GI disorders. ST-36 is located near the knee joint approximately 10 mm lateral to the anterior tubercle of the tibia in humans[57, 58].. Accupoint : Zusanli (ST-36). 17.
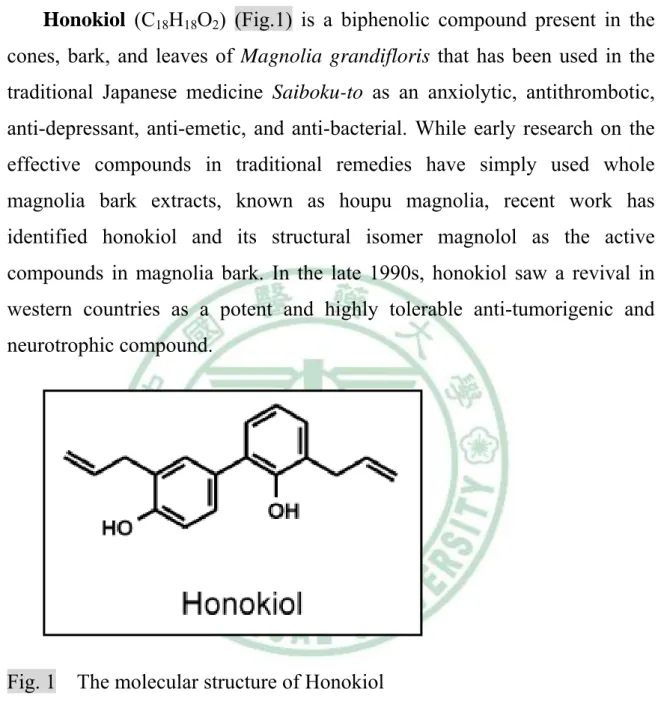
(30) 3. Database of Honokiol -----a new anti-neoplastic agent Honokiol (C18H18O2) (Fig.1) is a biphenolic compound present in the cones, bark, and leaves of Magnolia grandifloris that has been used in the traditional Japanese medicine Saiboku-to as an anxiolytic, antithrombotic, anti-depressant, anti-emetic, and anti-bacterial. While early research on the effective compounds in traditional remedies have simply used whole magnolia bark extracts, known as houpu magnolia, recent work has identified honokiol and its structural isomer magnolol as the active compounds in magnolia bark. In the late 1990s, honokiol saw a revival in western countries as a potent and highly tolerable anti-tumorigenic and neurotrophic compound.. Fig. 1 The molecular structure of Honokiol Anti-tumorigenic activities Honokiol has shown pro-apoptotic effects in melanoma, sarcoma, myeloma, leukemia, bladder, lung, prostate, and colon cancer cell lines.[59-62]. Honokiol. inhibits. phosphorylation. of. Akt,. p44/42. mitogen-activated protein kinase (MAPK), and src. Additionally, honokiol modulates the nuclear factor kappa B (NF-κB) activation pathway, an upstream effector of vascular endothelial growth factor (VEGF), 18.
(31) cyclooxygenase 2 (COX-2), and MCL1, all significant pro-angiogenic and survival factors. Honokiol induces caspase-dependent apoptosis in a TRAIL-mediated manner, and potentiates the pro-apoptotic effects of doxorubicin and other etoposides. So potent is honokiol's pro-apoptotic effects that it overcomes even notoriously drug resistant neoplasms such as multiple myeloma and chronic B-cell leukemia. Neurotrophic activity Honokiol has been shown to promote neurite outgrowth and have neuroprotective effects in rat cortical neurons. Additionally, honokiol increases free cytoplasmic Ca2+ in rat cortical neurons.[63] Anti-thrombolytic activity Honokiol inhibits platelet aggregation in rabbits in a dose-dependent manner, and protects cultured RAEC against oxidized low density lipoprotein injury. Honokiol significantly increases the prostacyclin metabolite 6-keto-PGF1alpha, potentially the key factor in honokiol's anti-thrombotic activity.[64] Numerous naturally occurring substances are recognized as antioxidants, cancer preventive agents, or even as a cancer therapy drug such as Taxol, Honokiol, an active component isolated and purified from the Magnolia officinalis, which is one kind of useful Chinese herb, has been demonstrated to possess the effects of anti-oxidation, against lipid peroxidation and anti-inflammatory in vitro and in vivo[65, 66]. Honokiol has also been shown to be a systemically available and non-toxic inhibitor of angiogenesis[62, 67, 68]. The recent studies reported that honokiol induces caspase-dependent apoptosis in B-cell chronic lymphocytic leukemia cells and overcomes conventional drug resistance in human multiple myeloma by 19.
(32) induction of caspase-dependent and -independent apoptosis[60, 61]. It has been also reported that honokiol induces apoptosis and inhibits the in vitro growth other human cancer cell lines such as colon cancer cell line RKO, lung cancer cell line CH27. Although a full assessment of the clinical potential of the compounds is not yet possible, the pharmacokinetics of honokiol has been thoroughly investigated, revealing that honokiol is available upon clinical cancer therapy. More natural products containing a variety of therapeutic compounds useful in preventing the development of malignancies continue to be discovered; however, very little is known about their underlying mechanisms of action or their molecular target [69, 70]. 20.
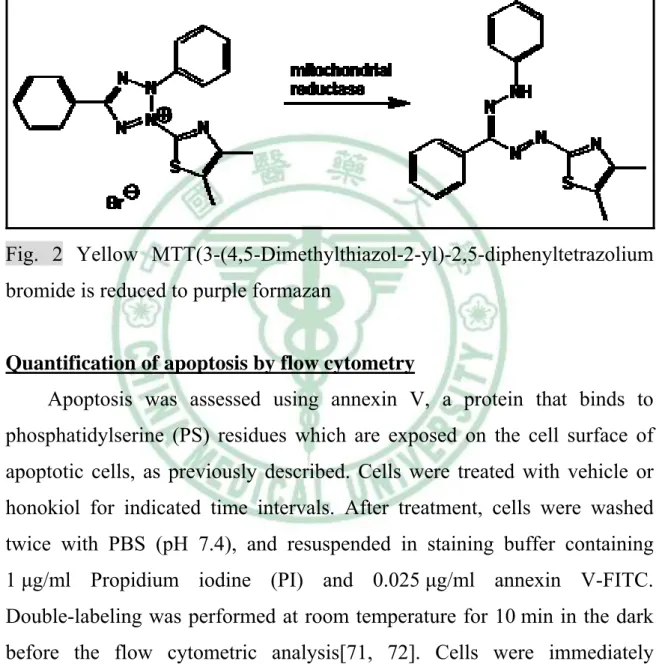
(33) Chapter 3. Materials and Methods. 1. Materials Honokiol was purchased from Wako (Osaka, Japan). Anti-mouse and anti-rabbit IgG-conjugated horseradish peroxidase, rabbit polyclonal antibodies specific for Bax, BclxL, Bak, PARP, caspase 3, caspase 9 were purchased from Santa Cruz Biotechnology (Santa Cruz, CA, USA). All other chemicals were obtained from Sigma-Aldrich (St. Louis, MO, USA). We used Trio 300 (Ito Co., Ltd., Japan) as electrical stimulator mode.. 2. Methods Cell culture The human lung adenocarcinoma cell lines (A549) was obtained from the American Type Culture Collection. The cells were maintained in Dulbecco's modified Eagle's medium/Nutrient Mixture Ham's F12 (DMEM/F12) medium which was supplemented with 10% heat-inactivated FCS, 2mM-glutamine, penicillin (100 U/ml) and streptomycin (100 ng/ml) at 37°C with 5% CO2.. MTT assay Cell viability was determined by MTT assay which are laboratory tests and standard colorimetric assays (an assay which measures changes in color) for measuring the activity of enzymes that reduce MTT to formazan. Yellow MTT(3-(4,5-Dimethylthiazol-2-yl)-2,5-diphenyltetrazolium. bromide. is. reduced to purple formazan in living cells (Fig. 2). After treatment with honokiol for 2 days, cultures were washed with PBS. MTT (0.5 mg/ml) was then added to each well and the mixture was incubated for 2 h at 37 °C. Culture medium was then replaced with an equal volume of DMSO to 21.
(34) dissolve formazan crystals[71]. After the mixture was shaken at room temperature for 10 min, absorbance of each well was determined at 550 nm using a microplate reader (Bio-Tek, Winooski, VT). Each clone was plated in triplicate in each experiment, and each experiment was repeated at least three times.. Fig. 2 Yellow MTT(3-(4,5-Dimethylthiazol-2-yl)-2,5-diphenyltetrazolium bromide is reduced to purple formazan. Quantification of apoptosis by flow cytometry Apoptosis was assessed using annexin V, a protein that binds to phosphatidylserine (PS) residues which are exposed on the cell surface of apoptotic cells, as previously described. Cells were treated with vehicle or honokiol for indicated time intervals. After treatment, cells were washed twice with PBS (pH 7.4), and resuspended in staining buffer containing 1 μg/ml Propidium iodine (PI) and 0.025 μg/ml annexin V-FITC. Double-labeling was performed at room temperature for 10 min in the dark before the flow cytometric analysis[71, 72]. Cells were immediately analyzed using FACScan and the Cellquest program (Becton Dickinson). Quantitative assessment of apoptotic cells was also assessed by the terminal deoxynucleotidyl transferase-mediated deoxyuridine triphosphate nick endlabeling (TUNEL) method, which examines DNA-strand breaks during apoptosis by using BD ApoAlert™ DNA Fragmentation Assay Kit. 22.
(35) Briefly, cells were incubated with honokiol for the indicated times. The cells were trypsinized, fixed with 4% paraformaldehyde, and permeabilized with 0.1% Triton-X-100 in 0.1% sodiumcitrate. After being washed, the cells were incubated with the reaction mixture for 60 min at 37 °C. The stained cells were then analyzed with flow cytometer[71, 73].. Western blot analysis The cellular lysates were prepared as described previously. Proteins were. resolved. on. SDS-PAGE. and. transferred. to. Immobilon. polyvinyldifluoride (PVDF) membranes. The blots were blocked with 4% BSA for 1 h at room temperature and then probed with rabbit anti-human antibodies against Bax, Bcl-2 (1:1000) for 1 h at room temperature. After three washes, the blots were subsequently incubated with a donkey anti-rabbit peroxidase conjugated secondary antibody (1:1000) for 1 h at room. temperature.. The. blots. were. visualized. by. enhanced. chemiluminescence using Kodak X-OMAT LS film (Eastman Kodak, Rochester, NY).. Caspase activity The assay is based on the ability of the active enzyme to cleave the Ac-DEVD-pNA (for caspase-3). The cell lysates were prepared and incubated with specific caspase-3 antibodies. Immunocomplexes were incubated with peptide substrate in assay buffer (100 mMNaCl, 50 mM 4-(2-hydroxyethyl)-1-piperazine-ethanesulphonic acid (HEPES), 10mM dithiothreitol,. 1mM. EDTA,. 10%. glycerol,. 0.1%. 3-[(3-cholamidopropyl)dimethylammonio]-1-propanesulfonate(CHAPS), pH 7.4) for 2 h at 37 °C. The release of p-nitroaniline was monitored at 405 nm. Results are represented as the percent change of the activity compared to the untreated control. 23.
(36) In vivo tumor xenograft study Male nude mice [6 weeks old; BALB/cA-nu (nu/nu)] were purchased from the National Science Council Animal Center (Taipei, Taiwan) and maintained in pathogen-free conditions. A549 cells were injected subcutaneously into the flanks of these nude mice (1 ×106 cells in 200μl) (Fig. 3A,B), and tumors were allowed to develop for ~14 days until they reached a size of approximately 100 mm3, when treatment was initiated. The mice were treated with vehicle, intraperitoneal injection 1.5 mg/kg Honokiol every day for 21 days (6 mice/group). The volume of the implanted tumor in dorsal side of mice was measured once a week with a caliper (Fig. 3C,D), using the formula V = (LW2) π/6: where V, volume (mm3); L, biggest diameter (mm); W, smallest diameter (mm). Xenografts that were smaller than pretreatment size were defined as tumor reduction[9, 10]. Three weeks after the beginning of the treatment, the xenografts were removed, and the specimens were processed for pathological analyses[8]. All protocols complied with institutional guidelines and were approved by Animal Care Committee of China Medical Taiwan University.. 24.
(37) Fig. 3 A549 cells were injected subcutaneously into the flanks of these nude mice [A,B]. The volume of the implanted tumor in dorsal side of mice was measured once a week with a caliper.[C,D]. Meridian Selection The acupuncture points used were the bilateral Zusanli (ST 36) acupoints, located on the calf of the anterior-tibia myo-muscle near the knee, according to the manual designed by Huang’s research. Non-acupoints were selected in the contralateral side of the upper limbs. It was demonstrated that the calcium ion concentration was significantly higher in the acupoint area than that in the non-acupoint and non-meridian locations. Thus, ion-selected EA electrodes were introduced for further detection of calcium ion concentration in acupoints in rats to ensure an 25.
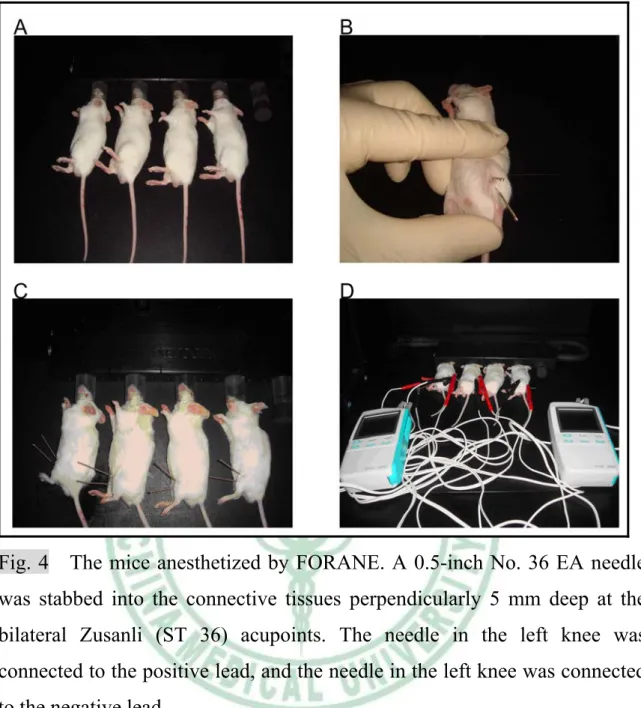
(38) accurate location of acupoints and nonacupoints for the study. The immunomodulatory effect of Zusanli (ST 36) acupoint was reported in many studies. For example, it could increase IL-2 level and NK cell activity and decreased level of IL-6 and IL-10 in the acupuncture group of cancer patient after 10 days of treatment[8, 57]; moxibustion on this point increase the white blood counts of the patients with late stage cancer; increase lymphocyte subgroups CD3+ and CD4+ and increased lymphocyte proliferation rate[10].. Operation of ST 36 electrical-acupuncture in mice The mice anesthetized by FORANE (isoflurane, USP), a nonflammable liquid administered by vaporizing, were placed on the wooden operating table. A 0.5-inch No. 36 EA needle (Han’s Instrument, Taiwan) was stabbed into the connective tissues perpendicularly 5 mm deep at the bilateral Zusanli (ST 36) acupoints. The needle in the right knee was connected to the positive lead, and the needle in the left knee was connected to the negative lead (Fig. 4). An electrical stimulus (2 Hz pulses) was delivered for 30 minutes, followed by 90 minutes of recovery, 1.5 mg/kg honokiol were injected intra-peritoneal in combined (EA+HK) group.. 26.
(39) Fig. 4 The mice anesthetized by FORANE. A 0.5-inch No. 36 EA needle was stabbed into the connective tissues perpendicularly 5 mm deep at the bilateral Zusanli (ST 36) acupoints. The needle in the left knee was connected to the positive lead, and the needle in the left knee was connected to the negative lead. Electro-acupuncture protocol Instrument:stainless steel needle : 0.20 mm*13 mm (36#) Acupoint:susanli acupoint (ST36) and non-acupoint (near ST-36) connected to the positive (anode) and the negative (cathode) wicks of a stimulator (mode Trio 300, Ito Co., Ltd., Japan) Deepness:The depth of insertion from 2 to 4 mm according to the 27.
(40) Electro-acupuncture parameter: Pulse : square biphasic wave, positive and negative Width : 50 micro-sec Frequncy: 2 Hz Intensities : 0.8 to 1 mA to produce a visual muscle contraction The electrical stimulation was applied to the animals for 15 minutes every day. Grouping Mice were injected subcutaneously with A549 cells. After the tumors reached 100mm3 in size, electroacupuncture group (EA), Honokiol group (HK), electroacupuncture conbined with Honokiol group (EA+HK) and vehicle (CON) was administered daily for 3 weeks( Fig. 5).. Grouping A5 49 sub cells cut inje an eo cting us l y. male athymic nude mice (nu nu), 5–7 weeks of age. randomization. Electrical acupuncture x6. Electrical acupuncture + Honokiol x6. Honokiol x6. 28. Control x6 39.
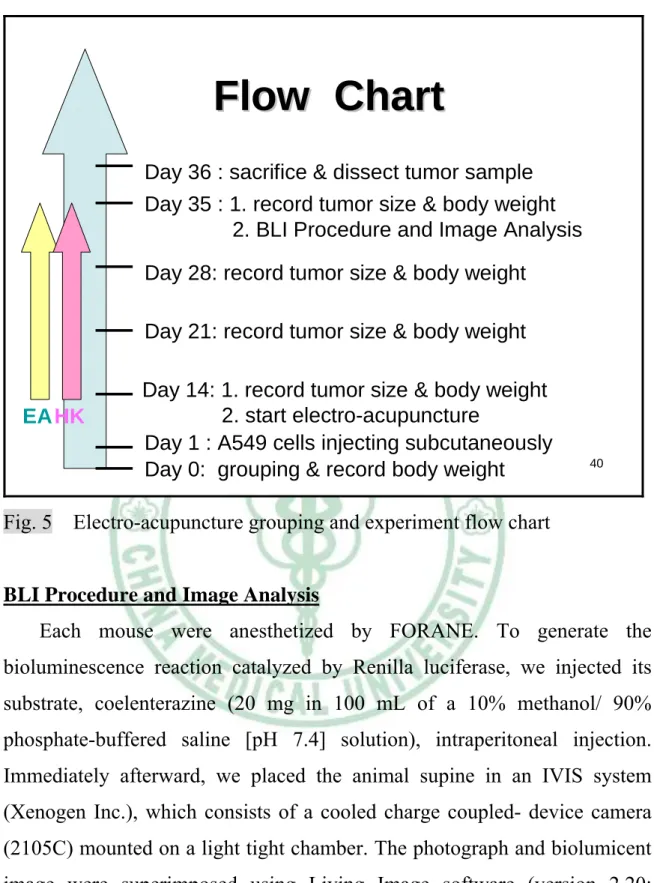
(41) Flow Chart Day 36 : sacrifice & dissect tumor sample Day 35 : 1. record tumor size & body weight 2. BLI Procedure and Image Analysis Day 28: record tumor size & body weight Day 21: record tumor size & body weight. EAHK. Day 14: 1. record tumor size & body weight 2. start electro-acupuncture Day 1 : A549 cells injecting subcutaneously Day 0: grouping & record body weight. 40. Fig. 5 Electro-acupuncture grouping and experiment flow chart. BLI Procedure and Image Analysis Each mouse were anesthetized by FORANE. To generate the bioluminescence reaction catalyzed by Renilla luciferase, we injected its substrate, coelenterazine (20 mg in 100 mL of a 10% methanol/ 90% phosphate-buffered saline [pH 7.4] solution), intraperitoneal injection. Immediately afterward, we placed the animal supine in an IVIS system (Xenogen Inc.), which consists of a cooled charge coupled- device camera (2105C) mounted on a light tight chamber. The photograph and biolumicent image were superimposed using Living Image software (version 2.20; Xenogen Inc.) (Fig. 6). 29.
(42) Fig. 6 IVIS system. Pathological analysis For hematoxylin-eosin (H&E) staining the xenografts were fixed in 10% neutral buffered formalin and embedded in paraffin. We performed the following procedures to complete H&E staining: 1. Deparafinize and hydrate slides to distilled water. 2. Stain in Harris’Hematoxylin for 4 minutes. 3. Rinse in tap water for 1 minute. 4. Clarify in 1% hydrochloric acid solution for 1 minute. 5. Rinse in tap water for 1 minute. 6. Blue in 0.5% ammonium hydroxide solution for 1 minute. 7. Rinse in tap water for 1 minute. 8. Dip in 95% alcohol three times. 9. Dip in Eosin four times. 10. Dehydrate in 95% alcohol, absolute alcohol and clear in xylene, two 30.
(43) changes each. 11. Mount with synthetic resin. The sections were then observed, and representative images were taken under a microscope (Olympus, Tokyo, Japan).. Statistics The values given are means ± S.E.M. Statistical analysis between two samples was performed using Student’s t test. Statistical comparisons of more than two groups were performed using one-way analysis of variance (ANOVA) with Bonferroni’s post hoc test. In all cases, P < 0.05 was considered as significant.. 31.
(44) Chapter 4 : Results Honokiol induced cell apoptosis in human lung cancer cells To investigate the potential cell death of Honokiol in human lung cancer cells, we first examined the effect of Honokiol on cell survival in human lung cancer cells (A549). Treatment of A549 cells with Honokiol-induced cell death in a concentration-dependent manner by using MTT assay (Fig. 7). We next investigated whether Honokiol induces cell death through an apoptotic mechanism. Annexin V-PI double-labeling was used for the detection of PS externalization, a hallmark of early phase of apoptosis. As compared to vehicle-treated cells, a high proportion of annexin V+ labeling was detected in cells treated with Honokiol (Fig. 8). To determine whether Honokiol induces apoptosis by triggering the mitochondrial apoptotic pathway, we measured the change in the expression of Bcl-2 family proteins. Treatment of A549 cells with Honokiol induced Bax and Bak protein levels. In addition, Honokiol decreased the expression of Bcl-xL and Bcl-2 (Fig. 9). On of the hallmarks of the apoptotic process is the activation of cysteine proteases, which represent both initiators and executors of cell death. Honokiol increased the activation of caspase-3 in A549 cells (Fig. 10).. Electroacupuncture. combined. with. intraperitoneal. injection. of. Honokiol inhibits tumour growth in the mouse xenograft model of A549 cells On the basis of the Honokiol-induced apoptotic effect exhibited in vitro, we decided to determine whether Honokiol possessed antitumor activities in vivo and electroacupuncture amplified the chemotherapeutic effect in cancer cells. We established xenografts of A549 cells in nude mice; as tumors reached 100 mm3 in size, the mice were divided into three groups and treated with either vehicle or Honokiol. We measured and recorded the volume of 32.
(45) the implanted tumor in dorsal side of mice once a week. We found that the volume of the implanted tumor was significantly reduced after 2 and 3 weeks in Honokiol group (HK) and electroacupuncture conbined with Honokiol group (EA+HK) (Fig. 11). Three weeks after the beginning of the treatment, we took the photograph and biolumicent image of mice (Fig. 12) and then we scarified the mice and the xenografts were removed (Fig. 13). The specimens were weighted and processed for pathological analyses.We also found that the weights of the implanted tumor were significantly reduced in HK group and EA+HK group (Fig. 14).. Electroacupuncture and intraperitoneal injection of Honokiol prevent body weight loss in the mouse xenograft model of A549 cells To observe to tumor reduction, we measured the tumors volume of the mice during the treatment, besides we recorded body weight of every mouse once a week to inspect the other physical condition. In the control group, we noted that the body weight of the mice was lost inversely the volume of the implanted tumor enlarged at the same time. However, in the EA, HK, EA+HK groups, we found that the appearance of body weight loss was not occurred (Fig. 15).. Pathological findings of A549 cell xenografts In A549 cell mouse xenografts treated, H&E staining showed different in the size and appearance of A549 cells and darker in the staining in the control and EA group (Fig. 16A&B). In the HK, and EA+HK groups, being regular in the arrangement of A549 cells, smaller in size , but not obvious in heteromorphism , and fewer in caryocinesia. In addition, necrobiosis of the tumor tissue appeared and inflammatory infiltration of lymphocytes in the interstitial tissue occurred (Fig. 16C&D).. 33.
(46) Honokiol induces mitochondrial-dependent apoptosis in A549 cells xenograft model and electroacupuncture could amplify the effect Finally, ex vivo analysis of tumors excised from mice showed significantly increased Bax and Bak protein expression in the HK and HK+EA groups compared with that in the control group, as shown by decreasing the expression of Bcl-xL and Bcl-2 (Fig. 17). Moreover, cytochrome C and caspase 3 protein expression in the HK and HK+EA groups also significantly exceeded the control group (Fig. 18). Taken together, these results suggest that Honokiol inhibits tumor growth by inducing A549 cell apoptosis in vivo and electroacupuncture could amplify the effect.. 34.
(47) Chapter 5 :. Discussion. Honokiol, an active component isolated and purified from the Magnolia officinalis, has been demonstrated to possess the effects of anti-oxidation, against lipid peroxidation and anti-inflammatory. Recently, alternative mechanisms of action have been proposed to account for the antitumor effect of Honokiol and many studies have been initiated to explore the antitumor efficacy of Honokiol. However, the anti-tumor effects of Honokiol on lung cancer cells are mostly unknown. In this study, we identified Honokiol as a potential lead base on anti-tumor activity in human lung cancer cells with good pharmacological properties. Mitochondrial dysfunction has been implicated as being a key mechanism in apoptosis in various cell death paradigms. Two major events have been noted in apoptosis involving mitochondrial dysfunction. One event is the change in the membrane permeability and subsequent loss of membrane potential. Bcl-2 family proteins regulate mitochondria-dependent apoptosis with the balance of anti- and pro-apoptotic members arbitrating life-and-death decisions. On the other hand, Honokiol treatment results in a significant increase of Bax and Bak expression, and a decrease of Bcl-xL, suggesting that changes in the ratio of proapoptotic and anti-apoptotic Bcl-2 family proteins might contribute to apoptosis-promotion activity of Honokiol. In agreement of these observations, we noted that the mitochondrial dysfunction may be involved in Honokiol-induced cell apoptosis of human lung cancer cells[74, 75].. Natural product drugs have been suggested to play a dominant role in pharmaceutical care. Natural products are one of the important sources of potential cancer chemotherapeutic and chemopreventive agents. Honokiol has been widely used in the traditional Chinese and Japanese medicine for several thousand years, mainly, for the treatment of anti-thrombocytic, 35.
(48) anti-bacterial, anti-inflammatory, and anxiolytic effects. Previous reports have demonstrated that Honokiol is also possessing potent anti-neoplastic and anti-angiogenic properties. However, the precise molecular mechanism of exhibited anti-tumor activity by Honokiol is not well understood. Thus, the results of this study provide evidences for the anti-tumor activity of Honokiol in gastric cancer, and more importantly, the molecular basis for its effect. The present study has demonstrated that Honokiol causes apoptosis in lung cancer cells in vitro and in vivo. Honokiol-induced apoptosis in lung cancer cells through the mitochondria dysfunction leading to activate involves a caspase-3-mediated mechanism. The proposed working models for the molecular basis would provide valuable insights for approaches to the development of effective chemotherapy by targeting appropriate signal transducers[76, 77].. 36.
(49) Chapter 6 :. Conclusion. Honokiol induced cell apoptosis in human lung cancer cell lines (A549 cell). Honokiol also induces upregulation of Bax and Bak, downregulation of Bcl-xL, Bcl-2 and dysfunction of mitochondrial in lung cancer cells. Animal studies have revealed a dramatic reduction in tumor volume after 21 days of treatment. Besides, electroacupuncture zusanli acupoint (ST36) combined with intraperitoneal injection of Honokiol inhibits tumour growth in the mouse xenograft model of A549 cells. This study demonstrates that honokiol may be a novel anticancer agent for the treatment of lung cancer cells and electroacupuncture could amplify the chemo-therapeutic effect in lung cancer treatment.. 37.
(50) Figures collection. Fig. 7. Honokiol induced the apoptosis of human lung cancer cells ( in. MTT assay) A549 cells were incubated with various concentrations of honokiol for 24 hr (A) or 48 hr (B), and the cell viability was examined by MTT assay. The IC50 values were examined about 20μM after 24 hr treatment. Results are expressed as the mean ± S.E. *, p < 0.05 compared with control. 38.
(51) Fig. 8. Honokiol induced the apoptosis of human lung cancer cells (in. annexin V/PI double staining) Cells were treated with vehicle or honokiol for 24 hr, the percentage of apoptotic cells was also analyzed by flow cytometric analysis of annexin V/PI double staining (A&B). Results are expressed as the mean ± S.E. *, p < 0.05 compared with control. 39.
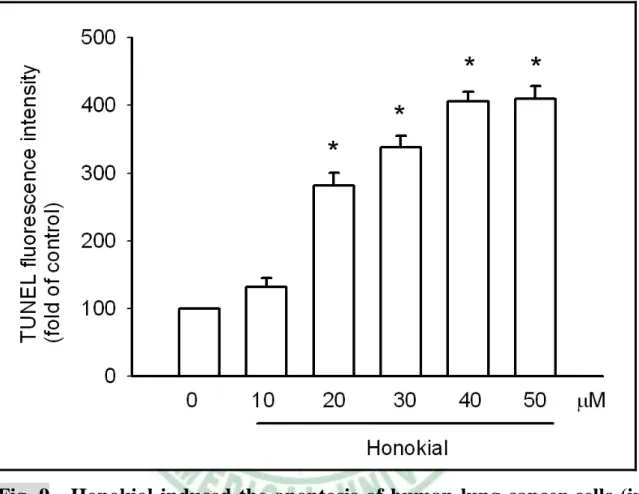
(52) Fig. 9. Honokiol induced the apoptosis of human lung cancer cells (in. TUNEL method) Cells were treated with vehicle or various concentrations of Honokiol for 24 hr, the TUNEL positive cells were examined by flow cytometry. Results are expressed as the mean ± S.E. *, p < 0.05 compared with control.. 40.
(53) Fig. 10. Honokiol induces apoptosis by triggering the mitochondrial. apoptotic pathway. A549 cells were incubated with Honokiol (20μM) for different time intervals, the Bax, Bak and Bcl-XL expressions were examined by Western blot analysis. Each experiment was repeated at least three times.. 41.
(54) Fig. 11. Honokiol induces the activation of caspase-3 in A549 cells. A549 cells were incubated with different concentrations of Honokiol (A). Then we treated A549 cells in 20μM for different time intervals, and the caspase-3 activities were examined by caspase ELISA kit. On the other hand, the caspase-3 expressions were examined by Western blot analysis. Results are expressed as the mean ± S.E. *, p < 0.05 compared with control. Each experiment was repeated at least three times.. 42.
(55) Fig. 12. Honokiol induced the implanted tumor of human lung cancer. cells significantly reduced after 2 and 3 weeks We established xenografts of A549 cells in nude mice; as tumors reached 100 mm3 in size, the mice were divided into four groups and treated with either vehicle, Honokiol or acupuncture. We measured and recorded the volume of the implanted tumor in dorsal side of mice once a week. We found that the volume of the implanted tumor was significantly reduced after 2 and 3 weeks in Honokiol group (HK) and electroacupuncture conbined with Honokiol group (EA+HK). Results are expressed as the mean ± S.E. *, p < 0.05 compared with control; #, p < 0.05 compared with honokiol-treated group.. 43.
(56) Fig. 13. Honokiol induced the implanted tumor of human lung cancer. cells significantly reduced in the end of experiment BLI Procedure and Image Analysis showed the tumor size and bioluminescent intensity in the different groups. The volume of Honokiol group (HK) and electroacupuncture conbined with Honokiol group (EA+HK) was significantly reduced.. 44.
(57) Fig. 14 the specimens in the different groups In the end of experiment, we scarified the mice and the xenografts were removed. The specimens were weighted and processed for pathological analyses.We also found that the volume of the implanted tumor was significantly reduced in HK group and EA+HK group.. 45.
(58) Fig. 15. The weights of the implanted tumor were significantly reduced. in HK group and EA+HK group In the end of experiment, we scarified the mice and the xenografts were removed. The specimens were weighted and processed for pathological analyses.We also found that the weights of the implanted tumor were significantly reduced in HK group and EA+HK group. Results are expressed as the mean ± S.E. *, p < 0.05 compared with control. Each experiment was repeated at least three times.. 46.
(59) Fig. 16. Electroacupuncture and Honokiol may prevent body weight. loss in the mouse xenograft model of A549 cells We recorded body weight of every mouse once a week to inspect the other physical condition. In the control group, we noted that the body weight of the mice was lost inversely the volume of the implanted tumor enlarged at the same time. However, in the EA, HK, EA+HK groups, we found that the appearance of body weight loss was not occurred. Results are expressed as the mean ± S.E. *, p < 0.05 compared with control. Each experiment was repeated at least three times.. 47.
(60) Fig. 17. Comparison 4 groups in the structural changes of A549 cells. displayed by H&E stain ×400 Control and EA group : being regular in the size and appearance of A549 cells , darker in the staining HK and EA+HK groups : being different in the arrangement of A549 cells , smaller in size , obvious in heteromorphism , and fewer in pyknosis. 48.
(61) Fig. 18. Honokiol induces mitochondrial-dependent apoptosis in A549. cells xenograft model ex vivo analysis of tumors excised from mice showed significantly increased Bax and Bak protein expression in the HK and HK+EA groups compared with that in the control group, as shown by decreasing the expression of Bcl-xL and Bcl-2. Each experiment was repeated at least three times.. 49.
(62) Fig. 19. Honokiol induces apoptosis via caspase3 and cytochrome C. mediated in A549 cells xenograft model ex vivo analysis of tumors excised from mice showed significantly cytochrome C and caspase 3 protein expression in the HK and HK+EA groups also significantly exceeded the control group. Each experiment was repeated at least three times.. 50.
(63) Reference 1.. "Deaths by cause, sex and mortality stratum" (PDF). World Health Organization. Retrieved on 2008-12-25. http://www.who.int/whr/2004/annex/topic/en/annex_2_en.pdf.. 2.. "Cancer". World Health Organization. http://www.who.int/mediacentre/factsheets/fs297/en/. Retrieved on 2007-06-25.. 3.. Vaporciyan, AA; Nesbitt JC, Lee JS et al. (2000). Cancer Medicine. B C Decker. pp. 1227–1292.. 4.. Minna, JD; Schiller JH (2008). Harrison's Principles of Internal Medicine (17th ed.). McGraw-Hill. pp. 551–562.. 5.. Gupta GP, Massague J. Cancer metastasis: building a framework. Cell 2006; 127: 679-695.. 6.. Woodhouse EC, Chuaqui RF, Liotta LA. General mechanisms of metastasis. Cancer 1997; 80: 1529-1537.. 7.. AbouEl Hassan MAI, Braam SR, Kruyt FAE. Paclitaxel and vincristine potentiate adenoviral oncolysis that is associated with cell cycle and apoptosis modulation, whereas they differentially affect the viral life cycle in non-small-cell lung cancer cells. Cancer Gene Therapy 2006; 13: 1105-1114.. 8.. Iwa M, Tateiwa M, Sakita M, Fujimiya M, Takahashi T. Anatomical evidence of regional specific effects of acupuncture on gastric motor function in rats. Autonomic Neuroscience-Basic & Clinical 2007; 137: 67-76.. 9.. Hu J, Chen LJ, Liu L, Chen X, Chen PL, Yang G, Hou WL, Tang MH, Zhang F, Wang XH, Zhao X, Wei YQ. Liposomal honokiol, a potent anti-angiogenesis agent, in combination with radiotherapy produces a synergistic antitumor efficacy without increasing toxicity. 51.
(64) Experimental & Molecular Medicine 2008; 40: 617-628. 10.. Hou W, Chen L, Yang G, Zhou H, Jiang Q, Zhong Z, Hu J, Chen X, Wang X, Yuan Y, Tang M, Wen J, Wei Y. Synergistic antitumor effects of liposomal honokiol combined with adriamycin in breast cancer models. Phytotherapy Research 2008; 22: 1125-1132.. 11.. Travis WD, Travis LB, Devesa SS. Lung cancer.[erratum appears in Cancer 1995 Jun 15;75(12):2979]. Cancer 1995; 75: 191-202.. 12.. Rosti G, Bevilacqua G, Bidoli P, Portalone L, Santo A, Genestreti G. Small cell lung cancer. Annals of Oncology 2006; 17 Suppl 2: ii5-10.. 13.. Fong KM, Sekido Y, Gazdar AF, Minna JD. Lung cancer. 9: Molecular biology of lung cancer: clinical implications. Thorax 2003; 58: 892-900.. 14.. Salgia R, Skarin AT. Molecular abnormalities in lung cancer. Journal of Clinical Oncology 1998; 16: 1207-1217.. 15.. Herbst RS, Heymach JV, Lippman SM. Lung cancer. New England Journal of Medicine 2008; 359: 1367-1380.. 16.. Aviel-Ronen S, Blackhall FH, Shepherd FA, Tsao M-S. K-ras mutations in non-small-cell lung carcinoma: a review.[see comment]. Clinical Lung Cancer 2006; 8: 30-38.. 17.. Engels EA, Wu X, Gu J, Dong Q, Liu J, Spitz MR. Systematic evaluation of genetic variants in the inflammation pathway and risk of lung cancer. Cancer Research 2007; 67: 6520-6527.. 18.. Wenzlaff AS, Cote ML, Bock CH, Land SJ, Santer SK, Schwartz DR, Schwartz AG. CYP1A1 and CYP1B1 polymorphisms and risk of lung cancer among never smokers: a population-based study. Carcinogenesis 2005; 26: 2207-2212.. 19.. Son J-W, Kang H-K, Chae MH, Choi JE, Park JM, Lee WK, Kim CH, Kim DS, Kam S, Kang YM, Park JY. Polymorphisms in the caspase-8 gene and the risk of lung cancer. Cancer Genetics & Cytogenetics 52.
(65) 2006; 169: 121-127. 20.. Yin J, Vogel U, Ma Y, Qi R, Sun Z, Wang H. The DNA repair gene XRCC1 and genetic susceptibility of lung cancer in a northeastern Chinese population. Lung Cancer 2007; 56: 153-160.. 21.. Fan Y-G, Hu P, Jiang Y, Chang R-S, Yao S-X, Wang W, He J, Prorok P, Qiao Y-L. Association between sputum atypia and lung cancer risk in an occupational cohort in Yunnan, China. Chest 2009; 135: 778-785.. 22.. Strand T-E, Rostad H, Damhuis RAM, Norstein J. Risk factors for 30-day mortality after resection of lung cancer and prediction of their magnitude.[see comment]. Thorax 2007; 62: 991-997.. 23.. El-Sherif A, Gooding WE, Santos R, Pettiford B, Ferson PF, Fernando HC, Urda SJ, Luketich JD, Landreneau RJ. Outcomes of sublobar resection versus lobectomy for stage I non-small cell lung cancer: a 13-year analysis. Annals of Thoracic Surgery 2006; 82: 408-415; discussion 415-406.. 24.. Fernando HC, Santos RS, Benfield JR, Grannis FW, Keenan RJ, Luketich JD, Close JM, Landreneau RJ. Lobar and sublobar resection with and without brachytherapy for small stage IA non-small cell lung cancer. Journal of Thoracic & Cardiovascular Surgery 2005; 129: 261-267.. 25.. Casali G, Walker WS. Video-assisted thoracic surgery lobectomy: can we afford it? European Journal of Cardio-Thoracic Surgery 2009; 35: 423-428.. 26.. MacCallum C, Gillenwater HH. Second-line treatment of small-cell lung cancer. Current Oncology Reports 2006; 8: 258-264.. 27.. Aruajo AMF, Mendez JC, Coelho AL, Sousa B, Barata F, Figueiredo A, Amaro T, Azevedo I, Soares M. Phase II study of celecoxib with cisplatin plus etoposide in extensive-stage small cell lung cancer. 53.
(66) Cancer Investigation 2009; 27: 391-396. 28.. Tsuboi M, Ohira T, Saji H, Miyajima K, Kajiwara N, Uchida O, Usuda J, Kato H. The present status of postoperative adjuvant chemotherapy for completely resected non-small cell lung cancer. Annals of Thoracic & Cardiovascular Surgery 2007; 13: 73-77.. 29.. Horn L, Sandler AB, Putnam JB, Jr., Johnson DH. The rationale for adjuvant chemotherapy in stage I non-small cell lung cancer. Journal of Thoracic Oncology: Official Publication of the International Association for the Study of Lung Cancer 2007; 2: 377-383.. 30.. Arriagada, R; Goldstraw P, Le Chevalier T (2002). Oxford Textbook of Oncology (2nd ed.). Oxford University Press. p. 2094.. 31.. Saunders M, Dische S, Barrett A, Harvey A, Gibson D, Parmar M. Continuous hyperfractionated accelerated radiotherapy (CHART) versus conventional radiotherapy in non-small-cell lung cancer: a randomised multicentre trial. CHART Steering Committee.[see comment]. Lancet 1997; 350: 161-165.. 32.. Lally BE, Zelterman D, Colasanto JM, Haffty BG, Detterbeck FC, Wilson LD. Postoperative radiotherapy for stage II or III non-small-cell lung cancer using the surveillance, epidemiology, and end results database.[see comment]. Journal of Clinical Oncology 2006; 24: 2998-3006.. 33.. Celebioglu B, Gurkan OU, Erdogan S, Savas I, Kose K, Kurtman C, Gonullu U. High dose rate endobronchial brachytherapy effectively palliates symptoms due to inoperable lung cancer. Japanese Journal of Clinical Oncology 2002; 32: 443-448.. 34.. Slotman B, Faivre-Finn C, Kramer G, Rankin E, Snee M, Hatton M, Postmus P, Collette L, Musat E, Senan S, Group ERO, Lung Cancer G. Prophylactic cranial irradiation in extensive small-cell lung cancer.[see comment][reprint in Ned Tijdschr Geneeskd. 2008 Apr 54.
(67) 26;152(17):1000-4; PMID: 18549175]. New England Journal of Medicine 2007; 357: 664-672. 35.. Hof H, Muenter M, Oetzel D, Hoess A, Debus J, Herfarth K. Stereotactic single-dose radiotherapy (radiosurgery) of early stage nonsmall-cell lung cancer (NSCLC). Cancer 2007; 110: 148-155.. 36.. Simon CJ, Dupuy DE, DiPetrillo TA, Safran HP, Grieco CA, Ng T, Mayo-Smith WW. Pulmonary radiofrequency ablation: long-term safety and efficacy in 153 patients.[see comment]. Radiology 2007; 243: 268-275.. 37.. Bencardino K, Manzoni M, Delfanti S, Riccardi A, Danova M, Corazza GR. Epidermal growth factor receptor tyrosine kinase inhibitors for the treatment of non-small-cell lung cancer: results and open issues. Internal & Emergency Medicine 2007; 2: 3-12.. 38.. Feld R, Sridhar SS, Shepherd FA, Mackay JA, Evans WK, Lung Cancer Disease Site Group of Cancer Care Ontario's Program in Evidence-based C. Use of the epidermal growth factor receptor inhibitors gefitinib and erlotinib in the treatment of non-small cell lung cancer: a systematic review. Journal of Thoracic Oncology: Official Publication of the International Association for the Study of Lung Cancer 2006; 1: 367-376.. 39.. Sandler A, Gray R, Perry MC, Brahmer J, Schiller JH, Dowlati A, Lilenbaum R, Johnson DH. Paclitaxel-carboplatin alone or with bevacizumab for non-small-cell lung cancer.[see comment][erratum appears in N Engl J Med. 2007 Jan 18;356(3):318]. New England Journal of Medicine 2006; 355: 2542-2550.. 40.. Dragnev KH, Petty WJ, Shah SJ, Lewis LD, Black CC, Memoli V, Nugent WC, Hermann T, Negro-Vilar A, Rigas JR, Dmitrovsky E. A proof-of-principle clinical trial of bexarotene in patients with non-small cell lung cancer. Clinical Cancer Research 2007; 13: 55.
數據
![Fig. 3 A549 cells were injected subcutaneously into the flanks of these nude mice [A,B]](https://thumb-ap.123doks.com/thumbv2/9libinfo/8933099.268315/37.892.136.780.110.770/fig-a-cells-injected-subcutaneously-flanks-nude-mice.webp)
+7


相關文件
Human papillomavirus- related squamous cell carcinoma of the oropharynx: a comparative study in whites and African Americans. Prevalence of human papillomavirus type 16 DNA in
- In the current lesion, the epithelioid cells were positive for S100 protein and no sustentacular cells were identified, effectively ruling out PGL as the diagnosis. -
Results of immunohistochemical staining with TTF-1 offered the critical evidence to verify whether the gingival and lung masses were synchronous double primary tumors or the
(E) Varying numbers of tumour cells expressing cancer antigen 125 are present in the lining of tubules (objective magnification ¥10).. The arrowed cells show strong nuclear
High pre-treatment serum level of vascular endothelial growth factor (VEGF) is associated with poor outcome in small-cell lung cancer. Telomerase as tumor
patients with stage I/II disease but not in those with stage III disease.43 A high serum level of VEGF is associated with poor survival among patients with small cell lung
Central granular cell odontogenic tumour, report of the first malignant case and review of the literature. Human leucocyte antigen typing in
Our case highlights an enigmatic presentation of oral submucous fibrosis and its coexistence with oral cancer presenting with unusual neurological disturbance of the inferior
