Leukemia Risk After Cardiac Fluoroscopic Interventions Stratified by
Procedure Number, Exposure Latent Time, and Sex: A Nationwide Population-Based Case-Control Study
Kai-Che Wei, MD a,b,c, Hon-Yi Lin, MD, PhD d,e, Shih-Kai Hung, MD, PhD d,e,
Yu-Tung Huang, PhD f, Moon-Sing Lee, MD d,e, Wen-Hua Wang, MD g, Chieh-Shan Wu,
MD a, Yu-Chieh, Su, MD e,h, Bing-Jie Shen, MD d,e, Shiang-Jiun Tsai, MS d, Wei-Ta
Tsai, MS d,i, Liang-Cheng Chen, MD d, Chung-Yi Li, PhD j,*, Wen-Yen Chiou, MD d,e,j,*
a Department of Dermatology, Kaohsiung Veterans General Hospital, Kaohsiung,
Taiwan
b Institute of Clinical Medicine, College of Medicine, National Cheng Kung
University, Tainan, Taiwan
c Faculty of Yuhing Junior College of Health Care and Management, Kaohsiung,
Taiwan
d Department of Radiation Oncology, Buddhist Dalin Tzu Chi Hospital, Chiayi,
Taiwan
e School of Medicine, Tzu Chi University, Hualien, Taiwan
f Master degree program in Aging and Long-Term Care, College of Nursing,
Kaohsiung Medical University, Kaohsiung, Taiwan
Taiwan
h Division of Hematology Oncology, Department of Internal Medicine, Buddhist
Dalin Tzu Chi Hospital, Chiayi, Taiwan
i Department of Biomedical Imaging and Radiological Sciences, National Yang-Ming
University, Taipei, Taiwan
j Department of Public Health, College of Medicine, National Cheng Kung
University, Tainan, Taiwan
* Corresponding Author: Chung-Yi Li, PhD and Wen-Yen Chiou, MD Corresponding Authors:
Dr. Chung-Yi Li
Address: Department of Public Health, College of Medicine, National Cheng Kung University, No.1, University Road, Tainan City 701, Taiwan (R.O.C.)
E-mail: [email protected]; Telephone: +886 52648000 extension 5679; Fax: +886 526511033
Dr. Wen-Yen Chiou
Address: Department of Radiation Oncology, Buddhist Dalin Tzu Chi Hospital, No. 2, Ming Sheng Road, Dalin, Chiayi, Taiwan (R.O.C.)
E-mail: [email protected]; Telephone: +886 52648000 extension 5695; Fax: +886 52651103
Running title: Leukemia Risk after Cardiac Fluoroscopic Interventions
Total number of pages: 13; Electronic word count for main manuscript: 2457 Tables: 4; Figures: 0
List of abbreviations:
PTCA: percutaneous transluminal coronary angioplasty EPS: electrophysiological study
Gy: gray (unit)
NHIRD: National Health Insurance Research Database NHRI: National Health Research Institutes
ICD-9-CM: International Classification of Disease, Ninth Revision, Clinical Modification
DM: diabetes mellitus
COPD: chronic obstructive pulmonary disease CAD: coronary artery disease
CHF: chronic heart failure OR: odds ratio
What has been known in this topic?
Iatrogenic radiation exposure can increase the risk of malignancies.
The frequency of percutaneous cardiac fluoroscopic interventions is increasing, as well as cumulative radiation exposure over the past 10 years.
What does this paper add?
The risk of leukemia in patients who underwent cardiac angiographic catheterization increased by 1.566 fold and occurred as early as 3 years following the procedure. Leukemia risk is more significant in patients who received multiple procedures, indicative of a possible dose-dependent relationship.
ABSTRACT Purpose
The number of cardiac fluoroscopic interventions have increased rapidly worldwide over the past decade. Percutaneous transluminal coronary angioplasty (PTCA) and stent implantation have become increasingly popular, and these advancements have allowed patients to receive repetitive treatments for restenosis. However, these advancements also significantly increase radiation exposure that may lead to higher cumulative doses of radiation. In the current study, a nationwide population-based case-controlled study was used to explore the risk of leukemia after cardiac angiographic fluoroscopic intervention.
Materials and Methods
A total of 5026 patients with leukemia and 100,520 control patients matched for age and sex (1:20) by propensity score method without any cancer history were enrolled using the Registry Data for Catastrophic Illness and the National Health Insurance Research Database (NHIRD) of Taiwan between 2008 and 2010. All subjects were retrospectively surveyed (from year 2000) to determine receipt of cardiac fluoroscopic interventions. Data were analyzed using conditional logistic regression models, and estimated crude and adjusted odds ratios (95% confidence interval).
After adjusting for age, gender, and comorbidities, PTCA was found to be associated with an increased risk of leukemia with an adjusted OR of 1.566 (95% CI, 1.282-1.912) while coronary angiography alone without PTCA and cardiac
electrophysiologic study were not. Our results also showed that an increased frequency of PTCA and coronary angiography was associated with a higher risk of leukemia (adjusted OR: 1.326 to 1.530 [all p < 0.05]). Gender subgroup analyses demonstrated that males were associated with a higher risk of leukemia compared with females.
Conclusions
These results provide additional data in the quantification of the long-term health effects of radiation exposure derived from the cardiac fluoroscopic diagnostic and therapeutic intervention. PTCA alone or PTCA with coronary angiography was associated with an elevated risk of leukemia. Continued follow-up of existing cohorts will be valuable to help assess lifetime risks of cancer.
INTRODUCTION
It has been well established that radiation increases the risk of cancer, based historically on survivors of atomic bombs and nuclear accidents [1]. Leukemia, thyroid cancer and breast cancer are the types most associated with nuclear/radiation exposure. Malignancies arising from iatrogenic radiation sources have been
documented following various types of exposure, including radiation therapy for cancer or benign disease. Squamous cell carcinoma, basal cell carcinoma, breast cancer, and sarcoma are the most common types [2, 3]. In addition to radiotherapy, it has been reported that 0.9% of cancers in the US (2004) may be caused by diagnostic X-rays, including plain films and computerized tomography (CT) scans [4].
Cardiac fluoroscopic interventions, including percutaneous transluminal coronary angioplasty (PTCA) and electrophysiologic studies (EPS), utilizing low-energy X-ray can exert higher doses of radiation than most other X-ray examinations. Therefore, a cardiac fluoroscopy intervention with its associated radiation exposure, might pose a higher risk of radiation-induced malignancy. However, the risk of malignancy was considered to be low, because the radiation dose delivered during each single procedure of cardiac catheter intervention was typically low and the net benefits for current heart disease outweighed possible risks of malignancy in the future.
registry, PTCA has been performed more than one million times annually in the US [5] and an estimated 35,000 times in Taiwan. Furthermore, these advancements allow patients to receive repetitive treatments for restenosis; however, inevitably the
radiation exposure increases significantly and may lead to higher life-long cumulative dose of radiation. An increasing number of cases have emerged with cardiac
fluoroscopy-induced radiation skin ulcers, the more severe form of skin damage associated with high doses of radiation (more than 15 Gy) [6]. This type of patient is no longer rare in the daily practice. Taken together, patients today who received PTCA have been exposed to an increased radiation dose compared with those patients treated over a decade ago.
Since the use of cardiac angiographic fluoroscopic interventions in medicine is widespread and appears to be increasing, there is a compelling need for additional data to quantify the long-term health effects of the diagnostic and therapeutic uses of radiation. However, there is a paucity of research regarding the relationship between radiation exposure from cardiac fluoroscopic procedures and the risk of cancer. There is currently a lack of definitive data and regulations about safe radiation thresholds of cumulative radiation exposure over a lifetime [7, 8]. In the current study, a nationwide population-based case-control study was used to explore the risk of leukemia post-cardiac angiographic fluoroscopic intervention.
MATERIALS AND METHODS
Ethics statement
All study protocols and procedures were approved by the Buddhist Dallin Tzu Chi Hospital Institutional Review Boards (Approval number B10402021). The IRB exempted requirement for written informed consent as this was a de-identified and encrypted database.
Databases
Patients were drawn from the National Health Insurance Research Database (NHIRD), one of the largest and most comprehensive databases in the world, which was released for research purposes by the National Health Research Institutes (NHRI), Taiwan [9, 10]. The NHIRD provides all medical claims for approximately 99% of Taiwanese people [11]. In order to ensure accuracy of the claims, NHIRD performs quarterly expert reviews on a sample taken from every 50 to 100 ambulatory and inpatient claims [12]. False diagnostic reports yield severe penalties from NHIRD [13]. Several studies have proved data accuracy of NHIRD [14].
Study groups
This was a population-based case-control study. First, leukemia patients were identified using the International Classification of Disease, Ninth Revision, Clinical Modification (ICD-9-CM) code (Code 202.4, 203.1, 204.0, 204.1, 204.2, 204.8, 204.9, 205.0, 205.1, 205.2, 205.8, 205.9, 206.0, 206.1, 206.2, 206.8, 206.9, 207.0,
207.2, 207.8, 208.0, 208.1, 208.2, 208.8, 208.9) from Registry Data for Catastrophic Illness. Catastrophic illness certificate, a peer-confirmed data subset, which could further ensure the accuracy of a cancer diagnosis was used for validation of a leukemia diagnosis [9, 10]. Patients with previously diagnosed leukemia and any other cancer history were excluded. Between Jan. 2008 and Dec. 2010, 5026 newly diagnosed leukemia patients were recruited. Secondly, 884,023 persons without any cancer history based on results from the Longitudinal Health Insurance Database served as controls. One million beneficiaries were randomly selected using the NHIRD by the NHRI and were included in the Longitudinal Health Insurance Database, which contained all claim data of the cohort from 1996 to 2010.
According to Facts 2014-2015 From the Leukemia and Lymphoma Society, age and sex are significantly associated with the incidence of leukemia and the incidence rates for all types of leukemia are higher among males than females [15]. We used a propensity score to balance groups before all analyses because of an initial significant between-group difference in age and gender. With a match ratio of 1:20, 5026
leukemia patients and 100520 controls were eligible for study inclusion.
Measurements of endpoints and covariates
To evaluate the association between the cardiac angiographic fluoroscopic intervention and leukemia, the data, including PTCA (ICD-9-CM procedure code
36.0, 36.01, 36.02, 36.05, 36.06, 36.09, 36.2), coronary angiography only without PTCA (ICD-9-CM procedure code 37.21, 37.22, 37.23, 37.29, 88.53, 88.54, 88.55, 88.56) and cardiac electrophysiological study (EPS) (ICD-9-CM procedure code 37.26, 37.27, 37.34), were collected. The number of PTCA, coronary angiography only without PTCA, and cardiac EPS were recorded, and the time between 1st
PTCA/1st coronary angiography/1st cardiac EPS to the last day of observation were
calculated.
The observation period for both groups was determined to begin January 1, 2000. The end of observation was defined as the last day before a leukemia diagnosis was made. The observation period of persons in the control group was the same as their corresponding leukemia patient after matching.
The potential risk factors of leukemia included gender, age, previous cancer treatment, exposure to certain chemicals, and life style like smoking. People who had any cancer history other than leukemia were excluded from our study. Adjusted independent variables included age, gender, and comorbidities. Persons who had previous certain chemicals exposure history were very few in general population and could be omitted in this large scale population-based study. Adjusted comorbidities included a number of major life style related illnesses, such as hyperlipidemia, diabetes mellitus (DM), hypertension, chronic obstructive pulmonary disease
(COPD), coronary artery disease (CAD), and congestive heart failure (CHF). Though our study database has no information about smoking status, COPD, a surrogate variable of chronic smoking behavior, has been adjusted in this study.
Statistical analysis
For patient characteristics and comorbidities in each group, chi-square and t-tests were used to evaluate differences between category and continuous variables.
Conditional logistic regression models and estimated odds ratios and their 95% confidence intervals were then used. Crude odds ratios were estimated from simple conditional logistic regression that takes into account the matching variables including age and gender in the analysis. We then adjusted for all the risk factors investigated in the conditional logistic regression model. In this study, we used two statistical
packages (SAS [version 9.2; SAS Institute, Inc., Cary, NC] and SPSS [version 12, SPSS Inc., Chicago, IL]) to analyze data. A p value < 0.05 was indicative of a statistically significant difference.
RESULTS
Patient characteristics and comorbidities for each group are shown in Table 1. Mean patient age was 52.7 years for both groups. In the leukemia group, males accounted for 57% of the newly diagnosed leukemia patients which was the same proportion reported by the Facts 2014-2015 From the Leukemia and Lymphoma Society [15]. No significant differences between proportions of gender were observed between study groups after matching.
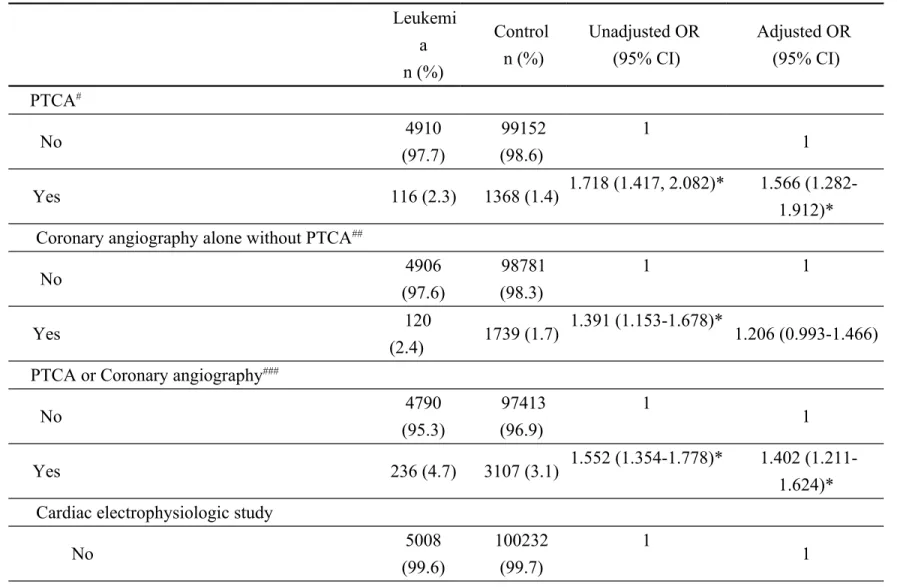
Conditional logistic regression analysis showed an association between percutaneous cardiac fluoroscopic procedures and leukemia (Table 2). Taken together, PTCA and coronary angiography were significantly associated with leukemia. If analyzed separately, PTCA was significantly associated with leukemia but coronary angiography alone without any PTCA was not significant after adjustment. The association between cardiac EPS and leukemia was not statistically significant.
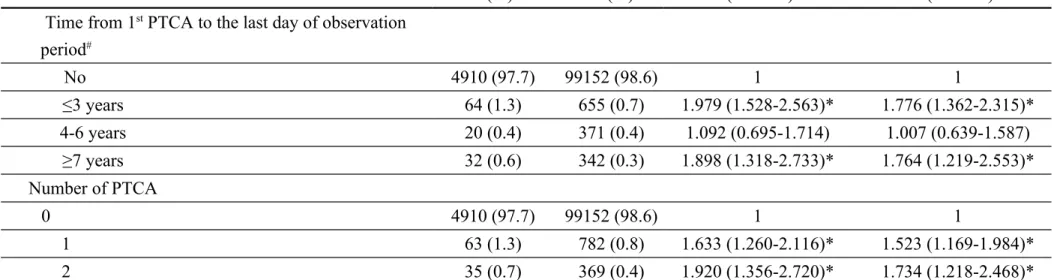
An elevated risk of leukemia was observed for time from first time PTCA or first time PTCA/coronary angiography to the last day of observation time in two time periods, ≦3 years and ≧7 years post 1st procedure (Table 3). Our results also showed
that PTCA and coronary angiography were associated with a higher risk of leukemia. Gender subgroup analyses (Table 4) showed males had a higher risk of leukemia than females. The greater number of PTCA and coronary angiography in both males and females, the higher the adjusted odds ratio (OR) of leukemia was observed. Males
also showed an elevated risk of leukemia during these two latent periods, ≦3 years and ≧7 years while females had elevated risk during the period of ≦3 years.
DISCUSSION
In this study, we have used a national health insurance database to examine the effects of cardiac fluoroscopic intervention on the incidence of leukemia. We demonstrate that cardiac fluoroscopic intervention increases the risk (OR: 1.566) of leukemia. The risk becomes significant within three years after receiving the initial cardiac fluoroscopic catheterization procedure. Compatible with the carcinogenic effect of radiation, a stochastic effect (ie, the higher cumulative radiation exposure) leads to a higher risk of radiation malignancy. Furthermore, the odds ratio of leukemia was increased with an increased number of interventions received in our study. This data reinforces the importance of reducing radiation exposure during procedures and for the arrangement of proper post-procedure follow-up.
Radiation exposure is inevitable when patients receive cardiac catheterization, however the benefits are believed to outweigh the possible risks of radiation damage. However, the dose of radiation exposure can be reduced without adversely effecting the treatment outcome through better technique and strict adherence to established safety guidelines. There have been many comprehensive reviews and practicable recommendations regarding how to reduce radiation dose that demonstrate practicality and feasibility [16].
has been reviewed in the literature. However, most studies used the methods of presumptive estimation dose-risk - that is LAR (lifetime attributable risk) to
estimate the cancer risk [7, 17]. The cancer risk estimations were based on theoretical conjectures, which were mainly derived from observations of effects of radiation in survivors of the Hiroshima/Nagasaki atomic bomb [18-20]. These estimates may not fit for patients who received cardiac fluoroscopic procedures who are exposed to pure X-rays with an energy spectrum between 40 KV (kilo-volt) and 120 KV. Whereas, the survivors of an atomic bomb or nuclear plant accident are exposed simultaneously to multiple types of radiation sources (including alpha particles, beta particles, and gamma ray) and absorption of radio-isotopes and X-rays in a wide range of different energy levels (from energy levels from kilo-volts to million-volts) at the same time. Therefore, compared to previous studies, our study results are more applicable in clinical practice.
Based on the database of survivors of atomic bombs, radiation-related malignancies have a latency period before tumors develop [17, 18]. This latency period depends upon the cancer types. Hematologic malignancies are the earliest type of radiation malignancies, as early as 2~3 years, while an excess of solid tumors is observed after >10 years. The effects of age at exposure and sex and in temporal pattern of risks are also significant. Our data is consistent with the prevalence of
hematologic malignancies in atomic bomb survivors.
The difficulties in studying cardiac fluoroscopy induced radiation carcinogenesis may be due to the fact that radiation-induced cancers are biologically
indistinguishable from other extrinsic and intrinsic cancers. Further, the background radiation is omnipresent and is one of the leading causes of leukemia. Since radiation-induced tumors cannot be distinguished from tumors in general, only the
epidemiologic studies may be best suited to answer this question. However, the risk of radiation would be masqueraded while there were only a small numbers of subjects with cancers related to low-dose radiation as reported in the literature [21, 22]. Our study was a nationwide population-based study which included all patients with leukemia and all hospitals in Taiwan; therefore, this study had a sufficient number of cases for epidemiologic analysis.
To the best of our knowledge, there have been only two large-scale studies investigating cancer risk associated with cardiac fluoroscopic intervention. In 2005, Lambe et al. [23] reported there was no indication of increased risk of cancer except for a transient excess of lung cancers, following PTCA performed between 1989 and 1998. However, in 2005 the variables associated with these procedures may be much different, since the radiation exposure dose derived from PTCA 10 years ago was significantly less than that it is currently. Radiation dose in each procedure of PTCA
in each patient has increased in the last 10 years [24]. Furthermore, repeated cardiac fluoroscopy procedures in a short time, as well as considering the procedure length increases the cumulative dose. Therefore, the risk of cancer could be increasing while the total radiation exposure is also increasing. In 2013, Huang et al. [25] used a population database to report elevated risk of breast cancer in female cardiovascular patients and lung cancer in both genders after cardiac radiation exposure, but the risk of leukemia was not elevated. However, leukemia is a relatively rare disease, with incidence ranges between 7.3 to 13.9 per 100,000 people for different races [15], and the absolute number of leukemia cases among the one-million-population database is small even though the relative risk could be high. Our study design was
case-controlled rather than cohort as previous studies and therefore could find the elevated relative risk of leukemia.
Common risk factors for leukemia and coronary vascular diseases (CVD) may cause statistic bias. Fortunately, none of the major risks of CVD, including diabetes mellitus, obesity, male gender and hyperlipidemia, are also risk factors for leukemia. Smoking is well known to increase the risk of CVD and cancer, but it does not increase the risk of leukemia. By careful adjustment of basic characters of study and control group, like age and gender, the bias has been minimized [15].
available for calculation in each cardiac fluoroscopic procedure; therefore, the recommendation for a safe limit of radiation exposure for cardiac fluoroscopy procedures cannot be provided. However, our data demonstrated that the risk of leukemia increases with an increasing number of PTCA procedures, suggesting a dose-dependent correlation of radiation dose and risk of leukemia. Second, our study design provided little information about exposure upon the radiation-vulnerable groups, such as children and pregnant women. Because PTCA, indicated for coronary artery disease, had been performed mostly in middle aged to elderly groups, it was unlikely to answer the radiation effect of PTCA upon these vulnerable groups. On the other hand, EPS was performed for patients with a wide age range; but the case numbers of EPS were too small to answer this question based on our data. Conclusions
Since the use of cardiac angiographic fluoroscopic intervention in medicine is widespread and appears to be increasing, our study results provide additional data to quantify the long-term health effects of radiation exposure derived from the cardiac fluoroscopic diagnostic and therapeutic intervention. In our study, PTCA alone or PTCA with coronary angiography was associated with an elevated risk of leukemia. Continued follow-up and establishment of cohorts of patients exposed to new or modified diagnostic and treatment protocols may help resolve questions in these
Conflict of interest
The authors declare no competing interests.
Acknowledgements
This study is partly based on data from the National Health Insurance Research Database provided by the Bureau of National Health Insurance, Department of Health in Taiwan and managed by National Health Research Institutes (registry number 100266). However, the interpretation and conclusions contained herein are not those of the Bureau of National Health Insurance, Department of Health, or National Health Research Institutes.
References
[1] Thompson DE, Mabuchi K, Ron E, Soda M, Tokunaga M, Ochikubo S, et al. Cancer incidence in atomic bomb survivors. Part II: Solid tumors, 1958-1987. Radiation research. 1994;137; S17-67.
[2] Miller AB, Howe GR, Sherman GJ, Lindsay JP, Yaffe MJ, Dinner PJ, et al. Mortality from breast cancer after irradiation during fluoroscopic examinations in patients being treated for tuberculosis. The New England journal of medicine. 1989;321; 1285-1289.
[3] Schwartz RA, Burgess GH, Milgrom H. Breast carcinoma and basal cell epithelioma after x-ray therapy for hirsutism. Cancer. 1979;44; 1601-1605. [4] Berrington de Gonzalez A, Darby S. Risk of cancer from diagnostic X-rays: estimates for the UK and 14 other countries. Lancet. 2004;363; 345-351.
[5] Mozaffarian D, Benjamin EJ, Go AS, Arnett DK, Blaha MJ, Cushman M, et al. Heart disease and stroke statistics--2015 update: a report from the American Heart Association. Circulation. 2015;131; e29-322.
[6] Balter S, Miller DL. Patient skin reactions from interventional fluoroscopy procedures. AJR American journal of roentgenology. 2014;202; W335-342.
[7] Godino C, Maccagni D, Pavon AG, Viani G, Cappelletti A, Margonato A, et al. Estimating incidence of organ cancer related to PCI radiation exposure in patients treated for acute and chronic total occlusions. The Journal of invasive cardiology.
2013;25; 441-445.
[8] Picano E, Vano E. The radiation issue in cardiology: the time for action is now. Cardiovascular ultrasound. 2011;9; 35.
[9] Chen HF, Chen P, Li CY. Risk of malignant neoplasms of liver and biliary tract in diabetic patients with different age and sex stratifications. Hepatology. 2010;52; 155-163.
[10] Chen PC, Muo CH, Lee YT, Yu YH, Sung FC. Lung cancer and incidence of stroke: a population-based cohort study. Stroke. 2011;42; 3034-3039.
[11] Lu JF, Hsiao WC. Does universal health insurance make health care unaffordable? Lessons from Taiwan. Health affairs. 2003;22; 77-88.
[12] Cheng TM. Taiwan's new national health insurance program: genesis and experience so far. Health affairs. 2003;22; 61-76.
[13] Bureau of National Health Insurance Website (2000) Methods for estimating false claims.
[14] Cheng CL, Kao YH, Lin SJ, Lee CH, Lai ML. Validation of the national health insurance research database with ischemic stroke cases in Taiwan.
Pharmacoepidemiol Drug Saf. 2011:20(3); 236–242.
[15] Facts 2014-2015 From the Leukemia and Lymphoma Society, Available at http://www.lls.org/sites/default/files/file_assets/facts.pdf. Accessed September 14, 2015.
[16] Abdelaal E, Plourde G, MacHaalany J, Arsenault J, Rimac G, Dery JP, et al. Effectiveness of low rate fluoroscopy at reducing operator and patient radiation dose during transradial coronary angiography and interventions. JACC Cardiovascular interventions. 2014;7; 567-574.
[17] Pierce DA, Preston DL. Radiation-related cancer risks at low doses among atomic bomb survivors. Radiation research. 2000;154; 178-186.
[18] Hsu WL, Preston DL, Soda M, Sugiyama H, Funamoto S, Kodama K, et al. The incidence of leukemia, lymphoma and multiple myeloma among atomic bomb survivors: 1950-2001. Radiat Res. 2013;179; 361-382.
[19] Ron E, Preston DL, Mabuchi K, Thompson DE, Soda M. Cancer incidence in atomic bomb survivors. Part IV: Comparison of cancer incidence and mortality. Radiation research. 1994;137; S98-112.
[20] Preston DL, Kusumi S, Tomonaga M, Izumi S, Ron E, Kuramoto A, et al. Cancer incidence in atomic bomb survivors. Part III. Leukemia, lymphoma and multiple myeloma, 1950-1987. Radiation research. 1994;137; S68-97.
[21] Brenner DJ, Doll R, Goodhead DT, Hall EJ, Land CE, Little JB, et al. Cancer risks attributable to low doses of ionizing radiation: assessing what we really know. Proceedings of the National Academy of Sciences of the United States of America. 2003;100; 13761-13766.
risks of low-dose radiation. Nature reviews Cancer. 2009;9; 596-604.
[23] Lambe M, Hall P, Granath F, Sadr Azodi O, Nilsson T. Coronary angioplasty and cancer risk: a population-based cohort study in Sweden. Cardiovascular and interventional radiology. 2005;28; 36-38.
[24] Carpeggiani C, Landi P, Michelassi C, Marraccini P, Picano E. Trends of increasing medical radiation exposure in a population hospitalized for cardiovascular disease (1970-2009). PloS one. 2012;7; e50168.
[25] Hung MC, Hwang JJ. Cancer risk from medical radiation procedures for coronary artery disease: a nationwide population-based cohort study. Asian Pacific journal of cancer prevention : APJCP. 2013;14; 2783-2787.
Table 1. Patient demographic and clinical characteristics stratified by disease group Leukemia Control Chi-squared
n (%) n (%) P-value# Total 5026 100520 Age* 52.7 52.7 0.984 Gender* 0.773 Male 2865 (57.0) 57092 (56.8) Female 2161 (43.0) 43428 (43.2) Hyperlipidemia 0.656 No 3313 (65.9) 65953 (65.6) Yes 1713 (34.1) 34567 (34.4) Diabetes <0.001 No 3483 (69.3) 74623 (74.2) Yes 1543 (30.7) 25897 (25.8) Hypertension 0.466 No 2710 (53.9) 54728 (54.4) Yes 2316 (46.1) 45792 (45.6) COPD <0.001 No 3435 (68.3) 73076 (72.7) Yes 1591 (31.7) 27444 (27.3) CAD 0.114 No 3599 (71.6) 73005 (72.6) Yes 1427 (28.4) 27515 (27.4)
Time between CAD to the last day of
observation period** 0.138 No 3599 (71.6) 73005 (72.6) ≤3 years 343 (24.0) 6221 (22.6) 4-6 years 283 (19.8) 5803 (21.1) 7-9 years 422 (29.6) 8759 (31.8) 10-12 years 334 (23.4) 5969 (21.7) 13-15 years 45 (3.2) 763 (2.8) CHF <0.001 No 4482 (89.2) 93328 (92.8) Yes 544 (10.8) 7192 (7.2)
disease; CHF, chronic heart failure.
* Factors were used for propensity-score match to balance study groups.
** The end of observation period was defined as the last day of the year before a diagnosis of leukemia. The observation period of persons in the control group was the same date as their matched leukemia patient.
Table 2. Association between cardiac fluoroscopic intervention procedures and leukemia Leukemi a n (%) Control n (%) Unadjusted OR (95% CI) Adjusted OR (95% CI) PTCA# No 4910 (97.7) 99152 (98.6) 1 1 Yes 116 (2.3) 1368 (1.4) 1.718 (1.417, 2.082)* 1.566 (1.282-1.912)* Coronary angiography alone without PTCA##
No 4906 (97.6) 98781 (98.3) 1 1 Yes 120 (2.4) 1739 (1.7) 1.391 (1.153-1.678)* 1.206 (0.993-1.466) PTCA or Coronary angiography###
No 4790 (95.3) 97413 (96.9) 1 1 Yes 236 (4.7) 3107 (3.1) 1.552 (1.354-1.778)* 1.402 (1.211-1.624)* Cardiac electrophysiologic study
No 5008 (99.6) 100232 (99.7) 1 1 28
Yes 18 (0.4) 288 (0.3) 1.251 (0.776, 2.016) 1.157 (0.716-1.868) Abbreviations: PTCA: percutaneous transluminal coronary angioplasty; OR: odds ratio; CI: confidence interval.
a Adjusting for age, gender, hyperlipidemia, diabetes, hypertension, COPD, CAD, and CHF. #Persons who have ever received PTCA before a diagnosis of leukemia.
##Persons who have ever received a coronary angiography but never PTCA.
###Persons who have ever received PTCA and persons who have ever received coronary angiography but never PTCA.
*P value < 0.05.
Table 3. Association between cardiac fluoroscopic intervention procedures and leukemia by time to disease and number of procedure
Leukemia n (%) Control n (%) Unadjusted OR (95% CI) Adjusted OR (95% CI) Time from 1st PTCA to the last day of observation
period# No 4910 (97.7) 99152 (98.6) 1 1 ≤3 years 64 (1.3) 655 (0.7) 1.979 (1.528-2.563)* 1.776 (1.362-2.315)* 4-6 years 20 (0.4) 371 (0.4) 1.092 (0.695-1.714) 1.007 (0.639-1.587) ≥7 years 32 (0.6) 342 (0.3) 1.898 (1.318-2.733)* 1.764 (1.219-2.553)* Number of PTCA 0 4910 (97.7) 99152 (98.6) 1 1 1 63 (1.3) 782 (0.8) 1.633 (1.260-2.116)* 1.523 (1.169-1.984)* 2 35 (0.7) 369 (0.4) 1.920 (1.356-2.720)* 1.734 (1.218-2.468)* 29
≥3 18 (0.4) 217 (0.2) 1.679 (1.037-2.717)* 1.435 (0.883-2.334) Time from 1st PTCA/coronary angiography to the last
day of observation period#
No 4790 (95.3) 97413 (96.9) 1 1
<=3 years 103 (2.0) 1354 (1.3) 1.553 (1.268-1.902)* 1.391 (1.127-1.717)*
4-6 years 55 (1.1) 853 (0.8) 1.318 (1.001-1.735)* 1.190 (0.899-1.576)
>=7 years 78 (1.6) 900 (0.9) 1.771 (1.402-2.237)* 1.622 (1.275-2.062)*
Sum number of PTCA and coronary angiography
0 4790 (95.3) 97413 (96.9) 1 1
1 137 (2.7) 1923 (1.9) 1.455 (1.220-1.735)* 1.326 (1.103-1.594)*
2 60 ( 1.2) 726 (0.7) 1.689 (1.295-2.201)* 1.523 (1.161-1.998)*
≥3 39 (0.8) 458 (0.5) 1.744 (1.255-2.424)* 1.530 (1.095-2.140)*
Time from 1st cardiac electrophysiologic study to the
last day of observation period#
No 5008 (99.6) 100232 (99.7) 1 1 ≤3 years 0.9 (0.2) 99 (0.1) 1.821 (0.919-3.606) 1.616 (0.813-3.210) 4-6 years 3 (0.1) 74 (0.1) 0.812 (0.256-2.576) 0.736 (0.231-2.342) ≥7 years 6 (0.1) 115 (0.1) 1.045 (0.459-2.375) 1.017 (0.446-2.316)
Number of cardiac electrophysiologic study
0 5008 (99.6) 100232
(99.7)
1
1
1 16 (0.3) 235 (0.2) 1.363 (0.820-2.263) 1.261 (0.758-2.099)
2 1 (0.0) 50 (0.0) 0.400 (0.055-2.899) 0.374 (0.052-2.715)
>=3 1 (0.0) 3 (0.0) 6.667 (0.693-64.090) 5.166 (0.529-50.414)
Abbreviations: PTCA: percutaneous transluminal coronary angioplasty; OR: odds ratio; CI: confidence interval.
a Adjusting for age, gender, hyperlipidemia, diabetes, hypertension, COPD, CAD, and CHF.
# The end of the observation period was defined as the last day of the year before a diagnosis of leukemia. The observation
period of persons in the control group was the same as their matched leukemia patient. *P value < 0.05.
Table 4. Association between cardiac fluoroscopic intervention procedures and leukemia by gender
Total Male Female
Unadjusted OR (95% CI) Adjusted OR (95% CI) Unadjusted OR (95% CI) Adjusted OR (95% CI) Unadjusted OR (95% CI) Adjusted OR (95% CI) Time from 1st PTCA to the last day of the observation period#
No 1 1 1 1 1 1
≤3 years 1.979 (1.528-2.563)* 1.775 (1.362- 1.996 (1.443- 1.870 (1.340- 2.235 (1.363- 2.006
2.313)* 2.761)* 2.611)* 3.664)* 3.323)* 4-6 years 1.092 (0.695-1.714) 1.006 (0.638-1.586) 1.168 (0.696-1.959) 1.077 (0.637-1.820) 0.946 (0.337-2.655) 0.861 (0.305-2.432) ≥7 years 1.898 (1.318-2.733)* 1.763 (1.219-2.550)* 1.916 (1.250-2.936)* 1.768 (1.144-2.730)* 2.341 (1.017-5.388)* 2.269 (0.979-5.263) Number of PTCA 0 1 1 1 1 1 1 1 1.633 (1.260-2.116)* 1.522 (1.168-1.983)* 1.597 (1.164-2.192)* 1.526 (1.102-2.113)* 1.721 (1.036-2.859)* 1.622 (0.968-2.719) 2 1.920 (1.356-2.720)* 1.732 (1.217-2.466)* 1.833 (1.189-2.827)* 1.670 (1.074-2.595)* 2.855 (1.442-5.649)* 2.612 (1.308-5.214)* ≥3 1.679 (1.037-2.717)* 1.435 (0.882-2.332) 2.118 (1.238-3.622)* 1.849 (1.073-3.187)* 1.086 (0.251-4.707) 0.826 (0.189-3.605) Time from 1st PTCA/coronar y angiography to the last day of observation period#
No 1 1 1 1 1 1
≤3 years 1.553 (1.268-1.902)* 1.390 (1.126- 1.466 (1.128- 1.334 (1.015- 1.818 (1.271- 1.659
1.716)* 1.906)* 1.754)* 2.598)* 2.400)* 4-6 years 1.318 (1.001-1.735)* 1.190 (0.899-1.575) 1.440 (1.037-2.001)* 1.316 (0.938-1.845) 1.064 (0.610-1.858) 0.964 (0.547-1.697) ≥7 years 1.771 (1.402-2.237)* 1.621 (1.275-2.060)* 1.819 (1.367-2.421)* 1.663 (1.237-2.235)* 1.609 (1.014-2.553)* 1.487 (0.927-2.383) Sum number of PTCA and coronary angiography 0 1 1 1 1 1 1 1 1.455 (1.220-1.735)* 1.325 (1.102-1.593)* 1.413 (1.130-1.767)* 1.302 (1.029-1.647)* 1.444 (1.054-1.978)* 1.349 (0.973-1.869) 2 1.689 (1.295-2.201)* 1.523 (1.161-1.997)* 1.739 (1.248-2.423)* 1.594 (1.133-2.241)* 1.850 (1.122-3.048)* 1.622 (0.973-2.703) ≥3 1.744 (1.255-2.424)* 1.529 (1.094-2.137)* 1.903 (1.298-2.789)* 1.673 (1.129-2.478)* 1.609 (0.759-3.411) 1.401 (0.654-2.999) Abbreviations: PTCA: percutaneous transluminal coronary angioplasty; OR: odds ratio; CI: confidence interval.
a Adjusting for age, hyperlipidemia, diabetes, hypertension, COPD, CAD, and CHF.
# The end of observation period was defined as the last day of the year before a diagnosis of leukemia. The observation period of persons in the
control group was the same as their matched leukemia patient. *P value < 0.05.