Received: February 25, 2007 Accepted: May 26, 2007
Reprint requests to: Dr. Szu-Yu Hsiao, Kaohsiung Medical University Hospital, No.100, Shih-Chuan 1st Road, Kaohsiung, Taiwan 80756, ROC.
Dental health status and treatment needs of elementary school
children in Taiwan
S
HUN-T
EH
UANG1,2,3Y
AO-T
INH
O4Y
I- M
INGC
HUNG2Y
U-S
HANL
IN4N
AI-T
INGW
ANG4S
ZU-Y
UH
SIAO31
Graduate Institute of Oral Health Sciences, College of Dental Medicine, Kaohsiung Medical University, Kaohsiung, Taiwan, ROC.
2
Faculty of Dental Hygiene, College of Dental Medicine, Kaohsiung Medical University, Kaohsiung, Taiwan, ROC.
3
Department of Dentistry, Kaohsiung Medical University Hospital, Kaohsiung, Taiwan, ROC.
4
Graduate Institute of Dental Sciences, College of Dental Medicine, Kaohsiung Medical University, Kaohsiung, Taiwan, ROC.
Through implementation of preventive strategies such as a fluoride-containing mouth rinse program (FCMRP)since 1991, the dental health status of primary school children in Taiwan has recently been improved. The purposes of this study were to assess whether the dental health status has improved after these many years of efforts and to determine how much dental treatment children still need. In this study, 2324 children aged 6~12 years old, were recruited by a stratified cluster sampling method with probability proportional to size. Subjects were examined for dental health and evaluated for treatment needs. The rules and criteria of the dental examination followed those published by the World Health Organization(WHO). The examiners received reliability training prior to conducting the examinations. The data were analyzed by JMP software. The filling rate of permanent teeth of 12-year-old children was 58.78%. Compared to the previous data, the dental status of Taiwan’s school children has improved, and WHO oral health targets for the year 2000 were achieved. Furthermore, the filling rate has also remarkably improved.(J Dent Sci, 2(2):103-109 , 2007)
Key words: caries prevalence, DMFT index, school children.
The caries prevalence of permanent teeth for 11-year-old children in Taiwan in 1979 was 50.50%, and the mean ± standard deviation of the DMFT index was 1.0 ± 1.2 for boys and 1.7 ± 2.4 for girls1.
The DMFT index for 12-year-old children in 1983 was 3.37 ± 2.94 for boys and 4.23 ± 3.64 for girls2.
In addition, the average of the DMFT index was 3.76 ± 3.30, while the caries prevalence rate was 85.12%2.
Xiao et al.3 showed that the caries prevalence of
permanent teeth for 11-year-old children was 66.50%, and the DMFT index were 4.48 for boys and 5.42 for girls. From 1979 to 1990, remarkable increases in
both the DMFT index and caries prevalence rate occurred, which might have been caused by increased consumption of sweetened foods and sugar. Meanwhile, dental awareness and the practice of teeth brushing were not well established, nor was the usage of fluoride and fissure sealant popular in practice. These factors might also have contributed to such problems.
In the 1990s, according to the worsening tendency of dental health status, it was estimated that our school children’s DMFT index would exceed 6.00 by 2000. This fact shocked the dental profession and government authorities. After serious discussion at several symposiums, the Department of Health (DOH) decided to adopt several strategies for improving the oral health of schoolchildren. The first was a fluoride-containing mouth rinse (FCMR) program. A 2% NaF solution in 10 ml was gargled for 1 minute after lunch once a week by school children from the 1st to 6th grades. Another program adopted was the
brushing teeth after lunch (BTAL) program. This program was promoted in school children older than the 4th grade.
The first program was conducted by the Taiwan Academy of Pediatric Dentistry for 6 years from 1991 to 1997. A remarkable caries reduction rate of 40% on average was observed, and the DOH transferred this program to the Taiwan Dental Association for nationwide implementation for all school-aged children.
The National Health Insurance System (NHIS) was launched in 1995. In 2000, the coverage rate of the FCMR program was over 97%. Tsai et al.4 showed
that the DMFT index of permanent teeth for 12 year olds was 3.31, which indicated the dental health status of 12-year-old children in primary schools had steadily improved.
The NHIS covers most items of dental treat- ment including operative restoration, pulp therapy, periodontal treatment, and oral surgery. The filling rate of permanent teeth before 1995 was 30%, and it had increased to more than 40% in 2000. It is obvious that the NHIS has contributed to improvements in schoolchildren’s dental health.
According to targets set by the World Health Organization (WHO), the DMFT index for 12- year-old children worldwide should have been < 3.0 by the year 2000. The mean DMFT index of 12-year-old children in the world was 1.74 in September 20015. Countries whose DMFT index was
< 3.0 accounted for 70% of the 128 countries in the world (85% of the population worldwide). Although the dental health status of 12-year-old children in Taiwan has steadily improved, we still have some inequalities when compared with other countries. Considering that children in primary schools in Taiwan had received the FCMR program since 2000, it is worthwhile discussing if there has been any further improvement in children’s dental health status. The purpose of our survey was to investigate the dental status of children in primary schools, and to analyze their dental treatment needs.
MATERIALS AND METHODS
Materials and sample design
The detailed study design was described in a study of Yang et al.11 In total, 2496 children aged 6~12
years old in primary schools were recruited by a
clustered stratified random sampling method to investigate their caries prevalence rate, DMFT index and its components, and dental treatment needs.
Dental examination
The protocol in this study was designed according to the criteria set by the WHO6. The dental
examination was performed by dentists who had received special training for assessing the dental health status and treatment needs of people with disabilities. Ten well-trained dentists, who were evaluated prior to the study and who achieved acceptable inter-examiner agreement, carried out the dental examinations.
A dental mirror, a standard dental explorer, a WHO periodontal probe, and a flashlight were used for the dental examination in the lobby or open space of the schools with the help of the nursing staff. Some individuals were examined in wheelchairs or even on their beds because of physical limitations. Dental radiographs were not used in this study.
The examination items included the dental health status, DMFT index and its components, caries prevalence and filling rates, and dental treatment needs. Prostheses that were or were not being worn were recorded, and the need for such devices was determined. The dental examinations were carried out between 2001 and 2002.
Statistical analysis
All data including the dental examination and fluoride exposure were coded and keyed into a computer. The statistical analyses were carried out with JMP software .
RESULTS
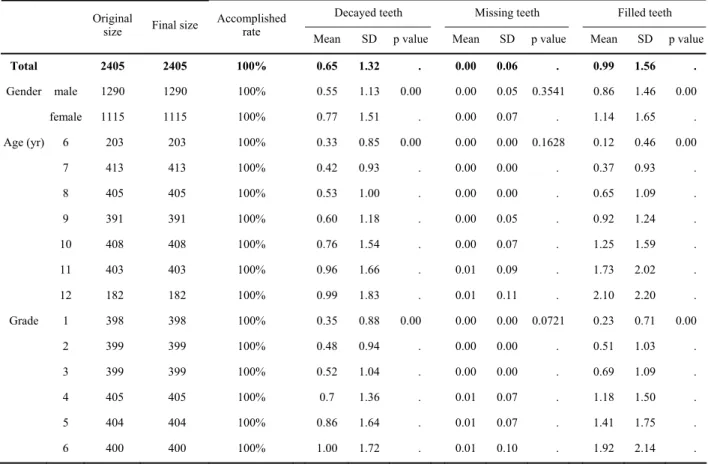
The study sample included 2405 children, among whom 2405 children (1290 boys and 1115 girls) completed all data collection procedure, for a completion rate of 100%. The dental health status examination of the permanent teeth showed that the restoration rate of permanent teeth for the entire sample was 58.78% from 27.11% for 6-year-old to 71.27% for 12-year-old children. The prevalence rate of boys (56.92%) was less than that of girls (60.61%) (p = 0.1258) (Table 1). The filling rate increased from 27.11% in 6-year-old children to 71.27% in
12-year-old children (p=0.0000). The filling rate obviously increased with age. The filling rates for boys and girls were 56.92% and 60.61%, respectively (Table 1).
The average number of decayed teeth (DT) was 0.33 for 6 year olds, and 0.99 for 12 year olds (Table 2). The mean missing teeth (MT) was 0.00 for 6-year-old children and 0.01 for 2 year olds. The mean number of filled teeth (FT) was 0.12 for 6 year olds and 2.10 for 12 year olds. The caries rate was obviously higher in girls than boys (60.61% vs. 56.92%).
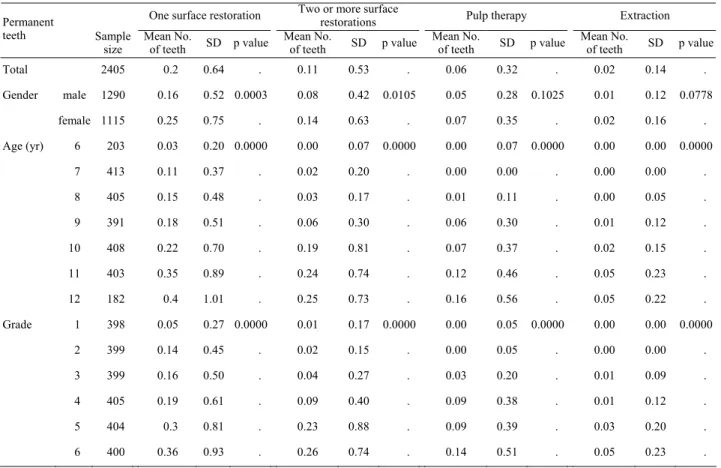
The assessment of treatment needs of the permanent teeth showed that 12.31% of children needed 1 surface restoration, 6.03% needed 2 or more surface restorations, 3.92% needed pulp therapy, and 1.47% needed an extraction. The figures for 6-year-old children were 2.49%, 0.50%, 0.50% and 0.50%, while those for 12-year-old children were 21.35%, 13.48%, 9.55% and 5.06%, respectively (all p values=0.0000) (Table 3). The treatment needs
increased with age. The number of teeth needing 1 surface restoration was 0.03 ± 0.20, that for 2 or more surface restoration was 0.02 ± 0.20, that for pulp therapy was 0.00 ± 0.07, and that for extraction was 0.00 ± 0.00 for 6 year olds, while for 12 year olds the figures were 0.40 ± 1.01, 0.25 ± 0.73, 0.16 ± 0.56 and 0.05 ± 0.22, respectively (all p values=0.0000) (Table 4). The percentages of children in need of 1 surface restoration, 2 or more surface restorations, pulp therapy, and extraction increased significantly with age (all p values=0.0000). There was no significant difference found between genders in the need for pulp therapy (p=0.1025) or extraction (p=0.0778), except those for 1 surface restoration (girls > boys, p=0.0003) and for 2 or more surface restorations (girls > boys, p = 0.0105).
DISCUSSION
Xiao et al.3 reported that the mean values for DT, Table1. Age and gender distributions of restoration rates of permanent teeth
Restoration rate Permanent teeth Original No. in the sample Final sample Accomplished rate
Mean SD p value Total 2405 2405 100% 58.78 44.18 Gender male 1290 1290 100% 56.92 45.31 0.1258 female 1115 1115 100% 60.61 43.00 Age (yr) 6 203 203 100% 27.11 43.50 0.0000 7 413 413 100% 42.50 46.33 8 405 405 100% 53.00 44.87 9 391 391 100% 60.21 43.05 10 408 408 100% 63.64 44.60 11 403 403 100% 64.84 41.11 12 182 182 100% 71.27 37049 Grade 1 398 398 100% 36.04 46.33 0.0000 2 399 399 100% 47.81 45.62 3 399 399 100% 56.15 45.35 4 405 405 100% 63.42 42.87 5 404 404 100% 63.21 43.50 6 400 400 100% 67.04 39.39 SD, standard deviation.
MT, and FT were 2.55, 1.47, and 0.46, respectively, for 12-year-old children with a DMFT index of 4.48. In this survey, Yang11 reported the mean value of the DMFT index to be 3.10. with DT of 0.99, MT of 0.01, and FT of 2.10 at the same age. Tsai et al.4 reported
that the mean values of the DMFT index of 6-, 9-, and 12-year-old children were 0.39, 1.36, and 3.31, respectively. In this survey, the mean values of the DMFT index of 6-, 9-, and 12-year-old children were 0.45, 1.52, and 3.10, respectively11. From the above
data, we found that during the past 20 years, the DMFT index of 12-year-old children in Taiwan dropped 40%, from 4.48 to 3.10, and caries prevalence and 2 of its 3 components, DT and ET, also significantly decreased, while FT prominently increased. These improvements were associated with dental health promotion programs such as the FCMR and TBAM programs. In addition, the filling rate of permanent teeth was found to be higher than that 20 years ago; DT occupied the largest portion of the DMFT index before, but in 2002 it was replaced by FT.
Due to the achievement of dental health promotion programs and the high filling rate of permanent teeth, the mean number of extracted teeth due to caries dropped from 1.47 per child in 1980 to 0.01 in 2002, with the mean of DT also dropping from 2.55 to 0.99. In addition, the mean value of FT also increased from 0.46 to 2.10. According to these results, we suggest that all the efforts of dentists, government authorities, school teachers, and parents of children have greatly improved the dental health status of school children in Taiwan, and we have achieved the goals of the WHO. Although Taiwan had almost achieved the WHO goal for 2000 (a DMFT index of < 3.0), there is still a long distance to the 2010 goal of a DMFT index of < 2.0. So dental caries are still an epidemic disease in Taiwan, in spite of the significant improvements when compared with the situation 10 years ago.
From the report of the Health Promotion Bureau4,
the DMFT indices of 6-, 9-, and 12-year-old children were 0.39, 1.36, and 3.31, respectively. In our survey, the DMFT indices of 6-, 9-, and 12-year-old children
Table2. Age and gender distributions of the 3 components of the DMFT index of permanent teeth
Decayed teeth Missing teeth Filled teeth Original
size Final size
Accomplished
rate Mean SD p value Mean SD p value Mean SD p value
Total 2405 2405 100% 0.65 1.32 . 0.00 0.06 . 0.99 1.56 . Gender male 1290 1290 100% 0.55 1.13 0.00 0.00 0.05 0.3541 0.86 1.46 0.00 female 1115 1115 100% 0.77 1.51 . 0.00 0.07 . 1.14 1.65 . Age (yr) 6 203 203 100% 0.33 0.85 0.00 0.00 0.00 0.1628 0.12 0.46 0.00 7 413 413 100% 0.42 0.93 . 0.00 0.00 . 0.37 0.93 . 8 405 405 100% 0.53 1.00 . 0.00 0.00 . 0.65 1.09 . 9 391 391 100% 0.60 1.18 . 0.00 0.05 . 0.92 1.24 . 10 408 408 100% 0.76 1.54 . 0.00 0.07 . 1.25 1.59 . 11 403 403 100% 0.96 1.66 . 0.01 0.09 . 1.73 2.02 . 12 182 182 100% 0.99 1.83 . 0.01 0.11 . 2.10 2.20 . Grade 1 398 398 100% 0.35 0.88 0.00 0.00 0.00 0.0721 0.23 0.71 0.00 2 399 399 100% 0.48 0.94 . 0.00 0.00 . 0.51 1.03 . 3 399 399 100% 0.52 1.04 . 0.00 0.00 . 0.69 1.09 . 4 405 405 100% 0.7 1.36 . 0.01 0.07 . 1.18 1.50 . 5 404 404 100% 0.86 1.64 . 0.01 0.07 . 1.41 1.75 . 6 400 400 100% 1.00 1.72 . 0.01 0.10 . 1.92 2.14 . SD, standard deviation.
were 0.45, 1.52, and 3.10, respectively. Within 2 years, the DMFT index of 12-year-old children dropped from 3.31 to 3.10, and the amount of change was about 0.2 teeth per child. This was mainly attributed to successful extensions of oral health promotion programs such as the BTAM and FCMR. Both of these programs were initiated in 1992. In 2001, more than 94% of school children were enrolled in these programs, and almost all children were enrolled in 2002.
In this study, the DMFT index of 6-year-old children was 0.45; the DMFT index of permanent teeth for 9-year-old children was 1.52. In Spain7, the
DMFT index of 6-year-old children was 0.25 and of the permanent teeth of 9-year-old children was 1.50. Our DMFT index in 2002 was higher than that in Spain in 1998 for 6- and 9-year-old children, but our caries prevalence rate was higher than theirs. In this study, the DMFT index of 12-year-old children was 3.31. In Spain, the DMFT index of 12-year-old
children was 3.30. The DMFT index in Taiwan in 2002 was lower than that in Spain in 1998 for 12-year-old children.
In Spain, 13.1% of 12-year-old children needed dental treatment, among which, 67.6% needed 1 surface restoration, 23.7% needed 2 or more surface restorations, 9.7% needed pulp therapy, and 9.8% needed an extraction. Treatment needs of girls were higher than those of boys in every age group. One surface restoration was the main type of treatment need for every age group. In our study, the percentage of children 12 years old who needed 1 surface restoration was 21.35%, that for 2 or more surface restorations was 13.48%, that for pulp therapy was 9.55%, and that for extraction was 5.06%. Our assessments of the needs for 2 or more surface restorations, pulp therapy, and extraction were close to those of Spain, but as for 1 surface restoration, Taiwanese children’s need was much lower than that of Spanish children. We also found higher treatment
Table3. Age and gender distributions of the treatment needs of permanent teeth
One surface restoration Two or more surface restorations Pulp therapy Extraction Original size Final size Accomplished rate Sample
size No. of teeth p value Sample size No. of teeth p value Sample size No. of teeth p value Sample size No. of teeth p value Total 2405 2405 100% 292 12.31 . 143 6.03 . 93 3.92 . 35 1.47 . Gender male 1290 1290 100% 135 10.57 0.0055 67 5.25 0.0851 41 3.21 0.0549 13 1.02 0.0463 female 1115 1115 100% 157 14.32 . 76 6.93 . 52 4.74 . 22 2.01 . Age (yr) 6 203 203 100% 5 2.49 0.0000 1 0.50 0.0000 1 0.50 0.0000 0 0.00 0.0000 7 413 413 100% 35 8.52 . 5 1.22 . 0 0.00 . 0 0.00 . 8 405 405 100% 40 10.03 . 9 2.26 . 5 1.25 . 1 0.25 . 9 391 391 100% 50 12.89 . 18 4.64 . 18 4.64 . 3 0.77 . 10 408 408 100% 52 12.90 . 33 8.19 . 19 4.71 . 6 1.49 . 11 403 403 100% 72 18.32 . 53 13.49 . 33 8.40 . 16 4.07 . 12 182 182 100% 38 21.35 . 24 13.48 . 17 9.55 . 9 5.06 . Grade 1 398 398 100% 17 4.30 0.0000 3 0.76 0.0000 1 0.25 0.0000 0 0.00 0.0000 2 399 399 100% 42 10.69 . 6 1.53 . 1 0.25 . 0 0.00 . 3 399 399 100% 44 11.06 . 11 2.76 . 8 2.01 . 3 0.75 . 4 405 405 100% 48 12.00 . 25 6.25 . 24 6.00 . 3 0.75 . 5 404 404 100% 64 16.20 . 41 10.38 . 26 6.58 . 10 2.53 . 6 400 400 100% 77 19.64 . 57 14.54 . 33 8.42 . 19 4.85 . SD, standard deviation.
needs in girls than boys. From the above data, it is obvious that although we did not control caries problems very well, we still have made much progress in preventing permanent tooth caries. In Taiwan, the NHIS provides for most items of dental treatment except orthodontic and prosthodontic treatments. As a result, the filling rate in our study had increased to 60%; this achievement had already caught up with the situation reported by Beltran-Aguilar et al. in the US8.
In a study by Wong et al.9 of Chinese children in
rural areas, they found that the dental treatment need for 1 surface restoration was 61.0%, that for 2 or more surface restorations was 56.0%, that for pulp therapy was 40.0%, and that for an extraction was 32.0% for 5~6-year-old children. The dental treatment need for 1 surface restoration was 38.0%, that for 2 or more surface restorations was 11.0%, that for pulp therapy was 14.0%, and that for an extraction was 17.0% for 12-year-old children. All figures were higher than those found in our study.
After various dental health promotion programs
had been carried out and the National Health Insurance System was launched in Taiwan, the DMFT index of 12-year-old children dropped to 2.74, and the filling rate increased to 70%. Compared to previous reports, the dental caries status of schoolchildren in Taiwan has already significantly improved. But when compared to the situations in developed countries, we still have a lot of work to do. (1) Caries prevalence is still high and listed as an epidemic disease of primary school children. We suggest that schoolteachers or nurses teach children how to establish proper oral health practices, and to take responsibility for their own oral health. (2) We do not have a system of dental hygienists to promote and contribute to dental health education in Taiwan. The establishment of the dental hygienist system is an urgent task. (3) Application of fluoride and fissure sealants are both very effective for the prevention of dental caries. We should promote these programs to improve the dental health status of schoolchildren in Taiwan.
Table4. Age and gender distributions of the percentages of treatment needs of permanent teeth
One surface restoration Two or more surface restorations Pulp therapy Extraction Permanent
teeth Sample
size Mean No. of teeth SD p value Mean No. of teeth SD p value Mean No. of teeth SD p value Mean No. of teeth SD p value Total 2405 0.2 0.64 . 0.11 0.53 . 0.06 0.32 . 0.02 0.14 . Gender male 1290 0.16 0.52 0.0003 0.08 0.42 0.0105 0.05 0.28 0.1025 0.01 0.12 0.0778 female 1115 0.25 0.75 . 0.14 0.63 . 0.07 0.35 . 0.02 0.16 . Age (yr) 6 203 0.03 0.20 0.0000 0.00 0.07 0.0000 0.00 0.07 0.0000 0.00 0.00 0.0000 7 413 0.11 0.37 . 0.02 0.20 . 0.00 0.00 . 0.00 0.00 . 8 405 0.15 0.48 . 0.03 0.17 . 0.01 0.11 . 0.00 0.05 . 9 391 0.18 0.51 . 0.06 0.30 . 0.06 0.30 . 0.01 0.12 . 10 408 0.22 0.70 . 0.19 0.81 . 0.07 0.37 . 0.02 0.15 . 11 403 0.35 0.89 . 0.24 0.74 . 0.12 0.46 . 0.05 0.23 . 12 182 0.4 1.01 . 0.25 0.73 . 0.16 0.56 . 0.05 0.22 . Grade 1 398 0.05 0.27 0.0000 0.01 0.17 0.0000 0.00 0.05 0.0000 0.00 0.00 0.0000 2 399 0.14 0.45 . 0.02 0.15 . 0.00 0.05 . 0.00 0.00 . 3 399 0.16 0.50 . 0.04 0.27 . 0.03 0.20 . 0.01 0.09 . 4 405 0.19 0.61 . 0.09 0.40 . 0.09 0.38 . 0.01 0.12 . 5 404 0.3 0.81 . 0.23 0.88 . 0.09 0.39 . 0.03 0.20 . 6 400 0.36 0.93 . 0.26 0.74 . 0.14 0.51 . 0.05 0.23 . SD, standard deviation.
REFERENCES
1. Hong YC, Chang CK, Duh FG, Knutson JW. Report on the Taiwan dental survey. Proc Natl Sci Counc ROC, 3: 250-258, 1979.
2. Lan CF. Investigation of teeth and oral status in Taiwan. National Health Administration of Oral Health in cooperation with Social Medical Department of Yang-Ming Medical College, Taipei, 1983.
3. Xiao YY, Guan SW, Chen YJ. Report of caries situation of students in middle and primary schools in Taiwan. Chin Dent J, 15: 78-86, 1996.
4. Tsai YL, Hsiang CL, Lu HK, Li LA, Hsu GH. Department of Health. Oral status survey of the population 6~18 years old, 1999~2000. Department of Health, Executive Yuan, Taipei, Taiwan, 2000.
5. World Health Organization. WHO Oral Health Country / Area Profile Program. Global caries data for 12-year-old age group 2002. Available at: http://www.whocollab.od.mah.se/ expl/globalcar. html. Accessed March 14, 2003.
6. World Health Organization. Oral Health survey-basic method. Geneva 1997. Available at: http://www.whocolab.od.mah.se/ expl/orhsurvey97.html. Accessed March 14, 2003.
7. Alvarez-Arenal A, Alvarez-Riesgo JA, Pena-Lopez JM, Fernandez-Vazquez JP. DMFT, DMFT and treatment requirements of schoolchildren in Asturias, Spain. Comm Dent Oral Epidemiol, 26: 166-169, 1998.
8. Beltran-Aguilar ED, Estupinan-Day S, Baez R. Analysis of prevalence and trends of dental caries in the Americas between the 1970s and 1990s. Int Dent J, 49: 322-329, 1999. 9. Wong MC, Lo EC, Schwarz E, Zhang HG. Oral health status
and oral health behaviors in Chinese children. J Dent Res, 80: 1459-1465, 2001.
10. Isamil AI, Messer JG, Hornett PJ. Prevalence of dental caries and fluorosis in seven-to 12-year–old children in northern Newfoundland and Forteau, Labrador. Can Dent Assoc, 64: 118-124, 1998.
11. Yang YH, Hu SW, Shieh TY, Huang ST, Hsieh MH. Elementary schoolchildren’s nutrition and health survey in Taiwan 2001-2002. Chinese Dental Journal, 25: 169-182, 2006.