前大腦動脈梗塞中風患者,動作關聯皮質電位的改變; Altered Movement-Related Cortical Potentials in Stroke Patients with Anterior Cerebral Artery Territory Infarct
58
0
0
全文
(2) 中國醫藥大學 醫學研究所 碩士候選人學位考試. 論文題目 中文:前大腦動脈梗塞中風患者,動作關聯皮質電位的改變. 英文:Altered Movement-Related Cortical Potentials in Stroke Patients with Anterior Cerebral Artery Territory Infarct. 本論文係 黃 偉 師 於中國醫藥大學醫學研究所完成之 碩士論文,經考試委員審查及口試合格,特此證明。. 考試委員 蔡崇豪 高嘉鴻 張芳嘉 所長: 藍先元 中華民國. 九十五 年 六 月 二十六 日. 1.
(3) 一、摘要: (一) 中文摘要 關鍵詞:動作關聯皮質電位、中風、前大腦動脈、內側額葉梗塞 動作關聯皮質電位(MRCP)由腦電圖(EEG)組成,是一種緩慢負向位移,啟始 於意志動作之前的1~1.5 秒。它包含至少三項次組成﹕動作準備電位 (Bereitschaftspontial,BP)、負斜波(negative slope,NS’)、及動作電位(motor potential,MP)。一般認為BP的產生是源自內側前額葉皮質,NS’是由雙側感覺 運動皮質區所產生,而MP則被視為源自對側中央區。這些MRCP次組成的產生 源頭乃依據皮質或頭皮記錄到的波形所作成的推論,然而這些理論性假設應該進 一步經由是否改變這些可能源頭的神經活性可以導致MRCP波形的改變來做進 一步印證。至少有兩種方法可以檢測此問題。其一是研究這些區域的病變或損傷 對MRCP的影響。其二是經由外部的電生理功能性擾動(例如重複式經顱磁刺激 術)來調節這些可能的源頭區域,觀察這些干擾如何影響MRCP的型態。在這個 研究中,我們是使用第一種的病變研究,利用前大腦動脈梗塞中風病人和正常人 在動作準備皮質電位的不同,研究前大腦動脈梗塞中風病人動作開始準備過程是 如何受到影響。前大腦動脈梗塞中風是一種較不常見部位的腦血管阻塞型中風。 缺血性腦中風造成的大腦內側額葉局部病灶,不僅造成大腦內側額葉區域的功能 障礙,同時也干擾了連結到此病變區域構造完整的神經網絡。因此,我們假設, 內側額葉缺血性腦中風後,大腦皮質運動神經網絡的失能,造成前大腦動脈梗塞. 2.
(4) 後的區域,動作關聯皮質電位的改變。在此計畫中,進行了七位病人的實驗組及 符合年齡配對的七位正常人控制組動作關聯皮質電位的研究。有三項結果可以提 出: (1) 病人組某些動作關聯皮質電位的次組成,相對於控制組,皆表現出較為 明顯的負波; (2) 病人組兩側腦部,特別是左側腦部,的負斜波相對於控制組, 有明顯的增大現象; (3) 病人組腦部的負斜波,在任何一側手腕活動時,皆沒有 出現「對側顯著」的現象。我們的結論如下:經由運用動作關聯皮質電位在時間 過程上會有顯著變化的優點,我們呈現了左側前大腦動脈灌流區域內側額葉梗塞 中風病人在動作發生前及動作執行中,於兩側腦部會出現動作關聯皮質電位作用 活性明顯增強的現象。這些結果符合先前的大腦前額葉會媒介動作早期準備過程 的概念,而且推測是經由大腦前額葉內側區域的影響。這種影響可藉由本實驗--前大腦動脈灌流區域內側額葉梗塞運動功能缺損後,代償的發生來印証;機轉可 能是來自於輔助運動區-前區部分(pre-SMA),傳送至運動區的抑制性輸入訊息, 因病灶而減少,或者是招募病灶周圍興奮性皮質區域而增加代償。. 3.
(5) (二) 英文摘要 Key words: MRCP, Stroke, ACA, Medial frontal lobe infarct. The movement-related cortical potential (MRCP) is an electroencephalography (EEG) component related to voluntary movement, which is a slow negative shift starting 1-1.5 sec before volitional movement. MRCPs consist of at least 3 subcomponents, the Bereitschaftspontial (BP), the negative slope (NS’), and the motor potential (MP). It is generally agreed that the generator for the BP is from the mesial prefrontal cortex and that for the NS’ can be sufficiently explained by the activation of generators in the sensorimotor cortex bilaterally. The MP can be accounted for by the activation of a source in the contralateral central region. The generating sources of these subcomponents of MRCP were deduced from the scalp or subdural recordings and the hypothesis should be further verified by determining whether functional perturbation of the candidate regions could actually modulate the behavior of MRCP. At least 2 methods may be adopted for this purpose. The first is lesion study of MRCP over the target sites. The second way is to modulate the candidate regions by external electrophysiological functional perturbation (e.g. repetitive transcranial magnetic stimulation, rTMS) to observe how the interference would affect the MRCP conformation. The present research is designed to elucidate. 4.
(6) the MRCP issue relying on lesion study in stroke patients with anterior cerebral artery (ACA) territory infarct. ACA territory is an uncommon site for occlusive vascular strokes. We hypothesized a deficit in the neuronal motor network after ACA infarct would lead to alterations in the movement related cortical network in the ACA infarct patients. We conduct the study in 7 patients and 7 age matched control. Three main results can be summarized as following: (1) some of the MRCP subcomponents showed a more pronounced negativity in the patient group than could be observed in the control group; (2) the amplitudes of NS’ were especially noted to be increased over the bilateral hemispheres in the patient group on the right hand movement as compared with the controls; (3) loss of lateralization of NS’ was noted in the patient group on the right hand movement, similar trend can also be observed on the left hand movement. The results could be due to diminution of pre-SMA (Area F6) inhibitory inputs to the subsequent motor regions or due to the recruitment of the nearby excitatory cortical regions for the compensation of motor impairment of the medial frontal lobe infarct. These results are in line with the idea of prefrontally mediated early preparatory processes prior to the execution of motion and illustrate that medial frontal region are crucial for the modulation or generation of MRCP.. 5.
(7) 二、誌謝辭 本論文之完成,承蒙指導教授蔡崇豪老師之殷切指導、啟發與砥 礪,以及蔡教授所領導之中國醫藥大學附設醫院「神經醫學實驗室」的 人力、物力協助,才能夠順利完成。必須致以最高之謝忱! 由衷感謝高副教授嘉鴻及張博士芳嘉在論文審查時所給予惠賜的 寶貴意見,獻上最誠摯的敬意;研究期間,承蒙本醫學研究所藍所長先 元於雜誌論文討論會中諸多指導,不勝感激。 同時還要特別感謝神經醫學實驗室同仁呂明桂醫師及張雅筑小 姐,對於研究過程的協助,研究問題的討論以及疑惑的解決,給予不可 或缺的幫忙與鼓勵,獻上最誠摯的謝意。 最後,僅以此論文呈現給多年苦心養育栽培我的父親黃蓋厚先生及 母親黃王碧珠女士;以及陪伴我的親愛妻子淑汶,由於您們在生活上的 照料與精神上的支持,使我得以心無旁騖、專心完成此論文。正因諸位 師長、同事、家人的扶持,這本論文對我也深具意義,感謝您們!. 6.
(8) 三、目錄 封面. 0. 學位考試委員審定書. 1. 一、摘要: (一). 中文摘要. 2-3. (二). 英文摘要. 4-5. 二、誌謝辭. 6. 三、目錄:. 7-8. 四、論文正文: 第一章 前言 第一節 研究背景. 9-15. 第二節 研究目的. 15. 第二章 研究方法 第一節 研究材料. 16. 第二節 研究設計. 17-18. 第三節 統計方法. 18-19. 第三章 研究結果 第一節 描述性統計分析. 20-29. 第二節 推論性統計分析. 30-31 7.
(9) 第四章 討論 第一節 結果討論. 32-41. 第二節 其他相關性討論. 42-43. 第三節 研究限制. 44-46. 第五章 結論與建議 第一節 結論. 47. 第二節 建議. 47-48. 五、參考文獻. 49-57. 六、授權書. 58. 8.
(10) 四、論文正文 第一章 前言 (Introduction) 第一節 研究背景 (Background) The mechanism of movement control that integrated in human central nervous system in one of the most intriguing research fields of neuroscience or clinical neurophysiology. There are several ways to investigate the issue and recording of the brain waves over the scalp (i.e. electroencephalography (EEG)), which reflecting the activity of cerebral cortex related to motor integration, is one of the feasible methods for the exploration of the particular domain. Conventionally, EEG was adopted to record spontaneous electrical activity generated in the cerebral cortex. This activity reflects the electrical currents that flow in the extracellular space and these in turn reflect the summated effects of innumerable excitatory and inhibitory synaptic potentials that occur on the cortical neurons (Daly et al., 1990).1 Despite the advantage, it is difficult for the traditional EEG to assess the relationship between the brain activities of the motor and motor-related cortex, including premotor, supplementary motor area (SMA) and prefrontal cortex, and the voluntary limb movement. To overcome the obstacle, Kornhuber and. 9.
(11) Deecke (1965)2 developed a technique, the alleged movement-related cortical potential (MRCP).. Basically, the EEG recording was triggered by. a voluntary electromyographic burst of the limb and the signals were averaged to determine the time-lock relationship between the movement onset and the contralateral cortical activity. By this way, the EEG activity prior to the voluntary movement can be assessed and illustrated. By and large, the MRCP waveform can be divided at least into 3 subcomponents: (1) Bereitschaftspotential (BP), the earliest subcomponent, a slowly rising negativity starting up to 2000 ms before movement onset; (2) negative slope (NS’), termed by Shibasaki et al. (1980),3 representing a steeper increase in negativity with higher amplitudes over central and parietal areas and starting about 500 to 300 ms before movement onset; and (3) motor potential (MP), a further increase in negativity followed by a sharp positivity, appearing around movement onset, its peak features the highest negativity of the MRCP and it is maximally pronounced over the vertex (Deecke et al., 1969).4 For finger movements, the scalp distribution of the BP is widespread and symmetrical, whereas the NS’ and MP show a clear lateralization toward the hemisphere contralateral to the movement. Regarding the generators, BP probable originates from the mesial prefrontal. 10.
(12) cortex including the supplementary motor area (SMA), premotor area and also the cingulate motor area and that for the NS’ can be sufficiently explained by the activation of generators in the sensorimotor cortex bilaterally. (Daly et al., 1990; Shibasaki et al., 1980; Deecke et al., 1969; Ikeda et al., 1995)1, 3-5 The fpMP can be accounted for by the activation of a source in the contralateral central regions. (Shibasaki et al. 1980)3 The generating sources of these different subcomponents of MRCP were mainly deduced from the cortical or scalp recordings (Daly et al., 1990; Deecke et al., 1969; Gerloff et al., 2003)1, 4, 6 and the hypothesis should be further verified by determining whether functional perturbation of the candidate regions could actually modulate the behavior of MRCP. At least two methods can be adopted to investigate the issue. The first would be lesion study of MRCP. In a patient with anterior cerebral arterial infarction, McNabb et al. (1988)7 illustrated that the BP was attenuated and the NS’ became asymmetric. The second method is to modulate the target regions by external electrophysiological functional perturbation to see how the interference would affect the MRCP conformation. In the current thesis, we adopt the lesion study to investigate the issue. Depending on the lesion site and duration, brain lesions may have. 11.
(13) differential impacts on the subcomponents of the MRCP (Gerloff et al., 2003; Wiese et al., 2004; Wiese et al., 2004).6,8,9 Among different sorts of lesions, ischemic stroke patients would be most appropriate for this purpose. Firstly, the arterial domain is well demarcated. Secondarily, the modern neuroimages can clearly portrait the anatomic sites of the lesion. To date, only few studies had examined the issue in patients with stroke or other sorts of brain lesions (McNabb et al., 1988; Singh and Knight1990; Shibasaki, 1975; Kitamura et al., 1996; Honda et al., 1997).7, 10–13 Moreover, the sample sizes in these studies were small and thus led the conclusion remaining to be elucidated. Deecke et al. (1987)14 demonstrated a missing maximum negativity over the vertex (Cz) in patients with unilateral lesions of the SMA. The authors found a reduction of the mean amplitude over the last 100 ms prior to movement onset in the fronto-central midline. Impaired MRCP have been reported in patients with Parkinson’s disease as well (e.g. Jahanshahi et al., 1995; Cunnington et al., 1995).15, 16 This phenomenon was attributed to the reduction of neuronal input into the SMA. It should be noted that lesion of the brain not only leads to functional perturbation of the lesion site but also to areas closely hooking to the. 12.
(14) insulted region. Witte et al. (1998).17 had illustrated that focal brain lesions due to traumatic brain injury do not only lead to functional deficits in the damaged area, but also disturb the structurally intact neuronal network connected to the lesion site. Anatomical studies found that the pre-SMA receives substantial input from the prefrontal cortex (Bates and Goldman-Rakic, 1993; Luppino et al., 1993).18,19 The notion had been strengthened by neuropsychological studies that revealed lesions in the frontal cortex lead to deficits in the neuronal motor network. Kolb and Milner (1981)20 demonstrated impairments in frontal lobe patients to copy complex arm and face movements. They ascribed these results to deficits in short-term memory and in the programming of movements. There are five circuits linking the frontal lobe and subcortical structure: motor, oculomotor, dorsolateral prefrontal, orbitofrontal, and anterior cingulate. Three of these different frontal-subcortical circuits are associated with emotional and cognitive processes in man (Alexander et al., 1986; Cummings, 1993).21,22 These three circuits have been named according to their site of origin on the frontal cortex as dorsolateral prefrontal circuit (originating from the convexity of the frontal lobe, Brodmann’s area 9 and 10), lateral orbitofrontal circuit (originating from the lower lateral parts of. 13.
(15) the prefrontal cortex, Brodmann’s area 10) and anterior cingulate circuit (originating from the medially located cingular cortex, Brodmann’s area 24). After their anatomically diverse areas of origin these circuits run closely adjacent to each other, although segregated, within the subcortical structures of caudate, globus pallidus, substantia nigra, thalamic nuclei and interconnecting white matter structures, e.g. capsula interna and corona radiata, before returning to the frontal cortex, thus forming a closed circuit. These circuits play crucial roles not only in cognitive function but also in motor execution. The anterior cerebral artery (ACA) supplies the rostral sensorimotor cortex and the anterior two-thirds of the corpus callosum by way of its calloso-marginal and pericallosal branches. From the point of view of blood supply, the front-basal ganglia circuitry and the motor-related areas, i.e. SMA, premotor cortex and prefrontal area, are allocated within the ACA domain. Thus it is reasonable to speculate that the ischemic stroke of this artery may lead to damage of these areas and help the determination of the possible modulation or generation source of MRCP. In addition, corpus callosum is often involved in ACA infarct and it may cause fibers connecting bilateral cerebral hemispheres damaged. And its detrimental. 14.
(16) effect on MRCP conformation is also keen to be learned. Finally, since the hand strength in most of the ACA infarct patients was intact and may less the confounding effect of the diminution of muscle strength on MRCP conformation. Footed on the aforementioned ground, the present research was designed to elucidate the MRCP issue in stroke patients with ACA infarct.. 第二節 研究目的 (Aim and Objectives) To examine how will the MRCP conformation be affected by ACA infarct? This will be helpful for the elucidation of the modulator or generator of MRCP.. 15.
(17) 第二章 研究方法 第一節 研究材料 2.1. Population: Seven patients with MRI-illustrated left ACA infarct were recruited from the Department of Neurology of the China Medical University Hospital and the subjects gave their written informed consent prior to the examination. The study was approved by the local ethic committee. The patient group consisted of 5 men and 2 women with a mean age of 63 (± 10.5 SD) years. None of the patients showed signs of a paresis of upper limbs. In order to achieve a homogenous, defined population, all patients with diffuse brain damage, previous brain disorders (e.g. traumatic, inflammatory, toxic, and hypoxic) or psychiatric disorders (e.g. depression) were excluded. The examination took place in the chronic phase at least 2 months after the acute stroke. Seven normal volunteers were examined as a control group. This group consisted of 5 men and 2 women with a mean age of 61 (± 12.0 SD) years.. 16.
(18) 第二節 研究設計 2.2.1. Paradigm and experimental procedure: During MRCP recording, subjects sat comfortably in an armchair with their elbows slightly flexed and their forearms resting on the armrests while looking at a fixed red spot 1.5 meters in front of them. The experimental paradigm consisted of self-paced brisk extension of either side of wrist. Subjects were instructed to carry out the movement in frequency of around 1 movement per 7 seconds. They were further asked to sit as relaxed as possible and not to blink during a period of 2 s before and after movement onset to avoid contamination of artifact. Before recording, the task was practiced until subjects performed sufficiently well. To avoid fatigue effects, the recording sessions were paused every 4 min until the subjects declared themselves ready to go on. The total recording time in the patient group did not exceed 50 min.. 2.2.2. Data acquisition: A 26-channel-EEG as well as vertical electrooculography (EOG) and surface EMG of the either-sided wrist (extensor digitorum communis, EDC) were recorded using a SynAmps amplifier (NeuroScan,. 17.
(19) Neurosoft, Inc. Sterling, Va, USA). All data were digitized, displayed and stored by a PC system. A bandpass filter was set from 0.05 to 70 Hz for EEG data. Twenty six Ag/AgCl EEG electrodes were placed according to the extended International 10–20 system using the EasyCap-system (Electro-Cap International, Eaton, USA) and were referenced to linked earlobe electrodes (A1/A2). Impedance was kept below 5 kΩ. At least one hundred artifact-free EEG epochs per subject were averaged and analyzed. 第三節 統計方法 2.3. Data analysis: All data were analyzed offline. EMG onset for each movement was identified by visual analysis and marked. Trials confounded by artifacts (i.e. blinks or DC-shifts) were removed after visual inspection. No additional algorithms for blink artifact correction were used. EEG data were segmented relative to EMG onset (from 2 s before to 1 s after EMG onset), filtered (high-pass filter at 0.05 Hz, 24 dB/oct, lowpass filter at 70 Hz, 24 dB/oct), baseline-corrected (using the first 200 ms as a baseline) and averaged. Grand Averages of the patient and the control groups were generated. EMG was rectified and averaged. All data. 18.
(20) processing was carried out using BrainVision Analyzer Software (Brainproducts, Munich, Germany). The different subcomponents of the MRCPs were identified visually in the Grand Averages. The averaged MRCP waveforms in the 26 electrodes were obtained to compare the difference between the patients and the normal subjects. We calculated the mean amplitude between -1500 ms and -500 ms which is thought as the Bereitschaftspotential (BP) and the mean amplitude between -500 ms and 0 ms which is thought as the negative slope (NS’). The latency and the amplitude of the motor potential (MP) were also measured. The rectified EMG recordings of the right and left self-paced movements were compared. The amplitude were compared using nonparametric test (Mann-Whitney U Test for 2 independent samples between the groups and Wilcoxon Signed Ranks Test for 2 related samples with C3/C4). All statistics were performed with the Statistical Package for Social Sciences (SPSS 10, Chicago, USA).. 19.
(21) 第三章 研究結果 第一節 描述性統計分析 3.1. Descriptive statistics. 3.1.1 Lesion data: Seven patients (Table 1) with MRI-defined left medial frontal lobe or SMA infarction (Figure 1-6) due to ACA territory ischemic stroke were recruited. The patient group consisted of 5 men and 2 women with a mean age of 63 (± 10.5 SD) years. None of the patients showed signs of a paresis of upper limbs. Seven normal volunteers were examined as control group. The control group consisted of 5 men and 2 women with a mean age of 61 (± 12.0 SD) years.. 20.
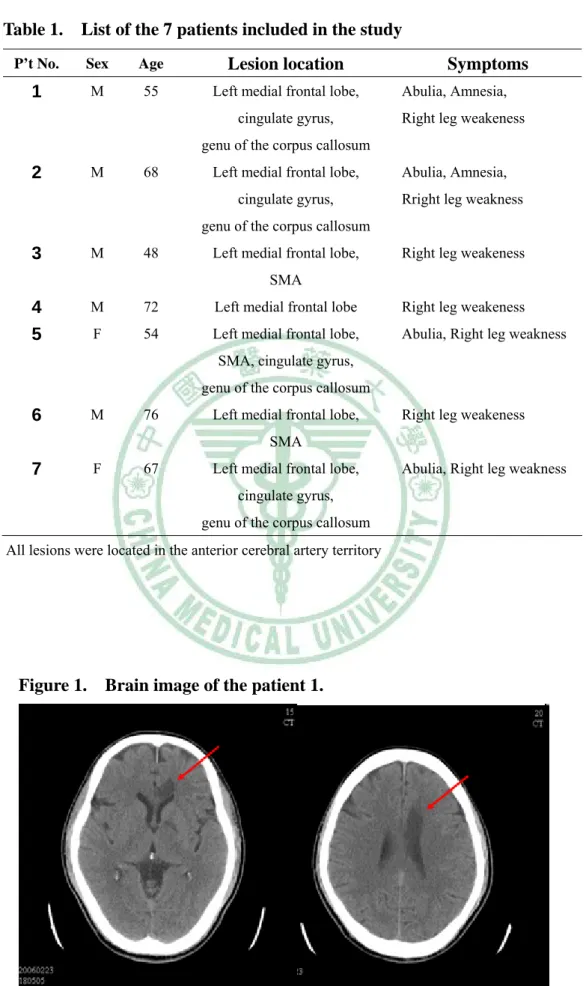
(22) Table 1.. List of the 7 patients included in the study. P’t No.. Sex. Age. Lesion location. 1. M. 55. Left medial frontal lobe, cingulate gyrus,. Symptoms Abulia, Amnesia, Right leg weakeness. genu of the corpus callosum. 2. M. 68. Left medial frontal lobe, cingulate gyrus,. Abulia, Amnesia, Rright leg weakness. genu of the corpus callosum. 3. M. 48. Left medial frontal lobe,. Right leg weakeness. SMA. 4 5. M. 72. Left medial frontal lobe. Right leg weakeness. F. 54. Left medial frontal lobe,. Abulia, Right leg weakness. SMA, cingulate gyrus, genu of the corpus callosum. 6. M. 76. Left medial frontal lobe,. Right leg weakeness. SMA. 7. F. 67. Left medial frontal lobe,. Abulia, Right leg weakness. cingulate gyrus, genu of the corpus callosum All lesions were located in the anterior cerebral artery territory. Figure 1.. Brain image of the patient 1.. CT scan: The image showed acute infarction of the left medial frontal 21.
(23) lobe in the anterior cerebral arterial territory.. DWI of MRI scan of patient 1: bright foci in the left medial frontal lobe, genu of the corpus callosum, medial parietal lobe. Coronal view.. T2-weighted MRI scan of patient 1.. 22.
(24) Saggital view of patient 1: FLAIR MRI scan showed bright foci in the anterior two-third of corpus callosum. MRA of patient 1 showed segmental absence of distal portion of the left anterior cerebral artery.. 23.
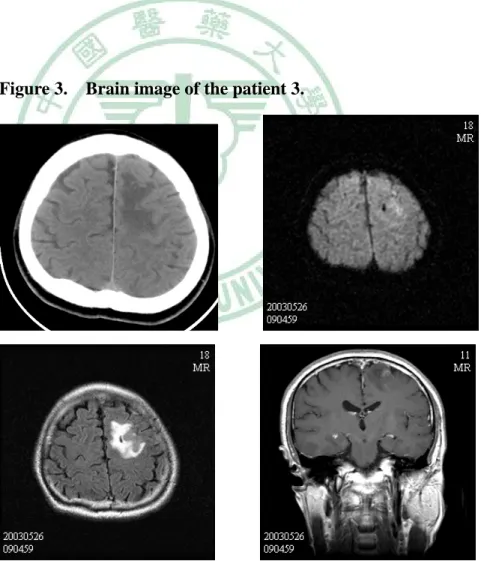
(25) Figure 2.. Brain image of the patient 2.. MRI showed acute infarction of left medial frontal lobe, cingulate gyrus and genu of the corpus callosum.. Figure 3.. Brain image of the patient 3.. Brain CT and MRI showed subacute infarction of left medial frontal lobe and SMA.. 24.
(26) Figure 4.. Brain image of the patient 4.. Brain MRI showed acute infarction of left medial frontal lobe.. 25.
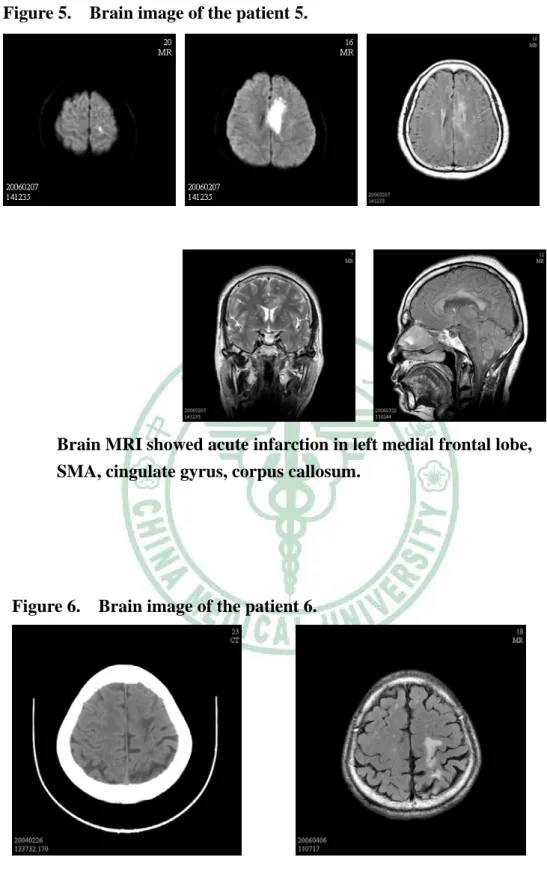
(27) Figure 5.. Brain image of the patient 5.. Brain MRI showed acute infarction in left medial frontal lobe, SMA, cingulate gyrus, corpus callosum.. Figure 6.. Brain image of the patient 6.. Brain CT and MRI showed infarction of left medial frontal lobe and SMA.. 26.
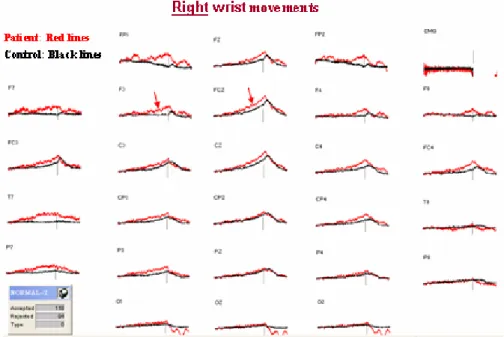
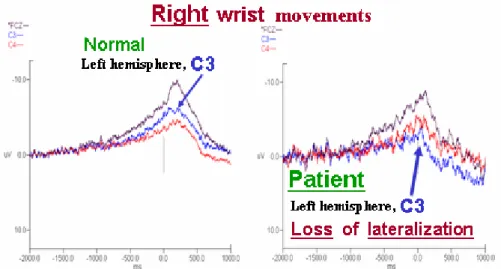
(28) 3.1.2 MRCPs: patient group In the patient group, all of the MRCP subcomponents showed a more pronounced negativity than could be observed in the control group. The NS’ were increased bilaterally with dominantly over the lesioned hemisphere during right hand movement (Figure 7, 8). Moreover, loss of lateralization was also noted in the patient group as comparing the amplitude of C3 with C4 during the either the left or the right wrist movement (Figure 9, 10).. 27.
(29) Figure 7. Grand Averages of the MRCPs for patient group (red lines) and the control group (black lines). Increased BP, NS’ and MP over lesioned (left) hemisphere were observed in patient group under right wrist movement.. Figure 8. Grand Averages of the MRCPs for patient group (red lines) and the control group (black lines). The amplitudes of BP, NS and MP of intact (right) hemisphere were not increased as observed in Figure 7 in patient group under left wrist movement. However, the normal lateralization was not detected as compared with the controls.. 28.
(30) Figure 9. Loss of lateralization in patient group as comparing amplitude of C3 with C4 during right wrist movement.. Figure 10. Loss of lateralization in patient group as comparing amplitude of C4 with C3 during left wrist movements.. 29.
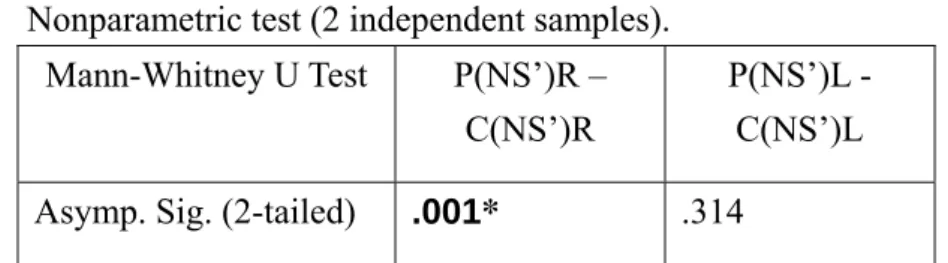
(31) 第二節 推論性統計分析 3.2. Inferential statistics Mann-Whitney U Test performed for the NS’ (-500 ms to 0 ms) revealed a significant difference of amplitude between patients and control groups (P = 0.001) during right wrist movement (Table 2). Wilcoxon Signed Ranks Test performed for the NS’ (-500 ms to 0 ms) revealed no significant difference of amplitude as comparing amplitude of C3 with C4 during either-sided wrist movement (Table 3) in the patients group and suggested loss of lateralization. On the other hand, Wilcoxon Signed Ranks Test performed for the NS’ (-500 ms to 0 ms) revealed a significant difference of amplitude as comparing amplitude of C3 with C4 (P = 0.036) during left wrist movement (Table 3) in the control group and suggested lateralization. Mann-Whitney U Test performed for the BP (-1500 ms to -500 ms) revealed no significant difference of amplitude between patients and control groups during either-sided wrist movement. (Table 4).. 30.
(32) Nonparametric test (2 independent samples). Mann-Whitney U Test. Asymp. Sig. (2-tailed). P(NS’)R – C(NS’)R. P(NS’)L C(NS’)L .314. .001*. Table 2. Significant difference of NS’ amplitude between patients and control groups (P = 0.001) during right wrist movement. P: Patients; C: Control; R: Right wrist movement; L: Left wrist movement. Nonparametric test (2 related samples). Wilcoxon Signed Ranks Test. C(NS’)L3 – C(NS’) L4. P(NS’)L3 – P(NS’) L4. C(NS’)R3 C(NS’) R4. P(NS’)R3 – P(NS’) R4. Asymp. Sig. (2-tailed). .036*. .779. .575. .779. Table 3. Significant difference of NS’ as comparing amplitude of C3 with C4 during left-sided hand movement (P = 0.036) in the control group that suggest lateralization. No significant difference of NS’ as comparing amplitude of C3 with C4 during either-sided hand movement (P = 0.779) in the patients group and suggest loss of lateralization. C: Control; P: Patients; L: Left wrist movement; R: Right wrist movement; 3: C3; 4: C4. Nonparametric test (2 independent samples). Mann-Whitney U Test. Asymp. Sig. (2-tailed). P(BP)R C(BP)R .149. P(BP)L C(BP)L .224. Table 4. No significant difference of BP amplitude between patients and control groups during either-sided wrist movement. P: Patients; C: Control; R: Right wrist movement; L: Left wrist movement. 31.
(33) 第四章 討論 (Discussion) 第一節 結果討論 The present study examined movement related-cortical potentials (MRCPs) in the stroke patients with left ACA infarct and compared the data with those of the controls. Three main results can be summarized: (1) some of the MRCP subcomponents showed a more pronounced negativity in the patient group than could be observed in the control group; (2) the amplitudes of NS’ were especially noted to be increased over the bilateral hemispheres in the patient group on the right hand movement as compared with the controls (3) loss of lateralization of NS’ was noted in the patient group on the right hand movement, similar trend can also be observed on the left hand movement. The present study revealed increased NS’ components in stabilized stroke patients. These MRCP components have been suggested to reflect different processes. NS’ is lateralized toward the hemisphere contralateral to upper extremity movements in healthy control subjects and is supposed to represent the programming of specific movement characteristics, such as the required force (Lang, 2003).23 In a recent review, Toma and Hallett (2003)24 concluded that the NS’ component is generated by the anterior. 32.
(34) bank of the central sulcus, corresponding to the contralateral primary motor cortex (M1). Functional recovery of these processes may be possible after poststroke paresis and this deficit might also be partially compensated by enhanced activity during movement execution. This finding was in line with Wiese et al (2005),25 who examined 12 patients with infarction in the territory of the left middle cerebral artery for more than 1 year. They found significantly decreased NS component over the lesioned hemisphere contralateral to the movement which was interpreted to represent impaired M1 functioning in cortical stroke patients and increased MP component over the contralesional hemisphere which implied the represence of functional reorganization of motor execution. In contrast to the patients’ population as studied by Wiese et al., the current patients were with lesions located in the mesial frontal cortex with intact primary motor cortex. The increased NS’ component and loss of lateralization of MRCPs over the lesioned hemisphere contralateral to the hand movement in the current study might reflect enhanced ipsilesional M1 functional activation in ACA territory stroke patients. The enhanced contribution of the ipsilesional prerolandic area might reflect the need for increased attentional resources during voluntary. 33.
(35) movement, compensating for the reduced planning abilities and supervising movement execution. Since the primary lesion was allocated in the medial frontal region, we speculated that the aforementioned enhancing phenomenon could be attributed to the release of the M1 from certain kind of inhibition or restriction from the lesion site. The possibility will be discussed in the later part of this session (Figure 11). In addition, a trend towards more increased MRCP subcomponents at electrodes FC3, T7, P7; F3, C3, CP3, P3; FZ, FCZ, CZ and F4, C4, CP4, FC4 during right wrist movement was also observed in patient group. The phenomenon suggests that the impaired unilateral medial frontal region may have pathophysiological impact on motor preparation or planning bilaterally, with somewhat more obvious impact on the ipsilesional side. The finding kept with the modern concept that the fibers of the supplementary motor areas (SMA) or nearby regions travel bilaterally to innervate the areas for motor control and execution (Deecke et al., 1987; Luppino et al., 1993; Ikeda et al., 1995, 1999)14,19,5,26. From the clinical point of view, these patients had decreased ability to divide their attention and may perform the movement less automatically, which culminated in the requirement of more attentional resources to perform the task.. 34.
(36) Improvement of motor function in most patients after hemiparetic stroke is associated with reorganization of central motor networks (Liepert et al., 2000; Nelles et al., 2001)27,28. In these patients, three patterns of activation have been identified likely representing different mechanisms of reorganization: (1) enlarged activation in primary motor cortex (M1) of the damaged hemisphere (contralateral to movement). (2) Recruitment of secondary motor cortices (SMA, premotor cortex, cingulate areas) or somatosensory cortex in the lesioned hemisphere. (3) Recruitment of sensorimotor motor cortex in the undamaged hemisphere ipsilateral to the moving limb (Weiller et al., 1993; Cramer et al., 1997; Cao et al., 1998).29-31 In a functional MRI (fMRI) study on cortical stroke patients, Cramer et al. (1997)30 found ipsilesional premotor cortex activation and Cao et al., (1998)31 concluded profound activation was observed during the ipsilateral paretic hand movements in two patients with left frontal infarction. Ipsilateral responses in stroke patients were supposed to represent a compensation of the brain damage in the contralateral middle cerebral artery (MCA) territory stroke patients. These patients were paretic in the initial stage after stroke, since their lesions include structures, which were vital for executing movements.. 35.
(37) In addition to stroke patients, Wiese et al. (2004)8 reported phenomenon of electrophysiological functional change after traumatic frontal lobe injury. They found significantly reduced BP area, delayed BP onset over the lesioned hemisphere and increased MP component over the hemisphere contralateral to lesion side, which was interpreted to represent the relatively enhanced contribution of the postrolandic ipsilateral cortex during motor execution and pointed to a contribution of the ipsilateral hemisphere in reorganizing the cortical motor network in these patients. Feydy et al. (2002)32 described different patterns of reorganization over time by using fMRI, with a focalization of ipsilesional SM1 activity mainly seen in subcortical stroke and a persistent recruitment of areas outside the ipsilesional SM1, including the contralesional motor cortex, was observed in cortical stroke. The presence of recruitment or focusing seemed to depend mainly on whether the M1 was damaged; persistent recruitment was observed in 3 of 4 patients with M1 injury, and focusing was seen in 8 of 10 patients with spared M1. It is likely that the cerebral cortex involvement is the pivotal factor for the determination of recruitment. If this is true, then it would be possible that the recruitment. 36.
(38) phenomenon can also be observed in patients after ACA infarct, in which the cerebral cortex of the frontal, SMA or cingulated gyrus may be involved. Thus the current findings may reflect the electrophysiological pattern after reorganization rather than naïve lesion after ischemic stroke. Phenomenon of reorganization had also been illustrated in middle cerebral arterial stroke patients by using transcranial magnetic stimulation. Caramia et al. (1996)33 found ipsilateral motor evoked responses in stroke patients’ hand muscles 3–15 days after the incident elicited in the unaffected hemisphere, a finding that could be replicated in several other studies (Netz et al., 1997; Caramia et al., 2000).34,35 Activations of the ipsilateral motor cortical network during finger movements had also been described in PET (Weiller et al., 1993, 1992; Chollet et al., 1991; Seitz et al., 1998)28, 36-38, and EEG studies (Green et al., 1999)39 in patients with stabilized stroke. The present study also revealed increased MP (data not shown) components of lesioned hemisphere when moving the contralateral hand in stabilized stroke patients. The MP has been suggested to reflect afferent sensory input from the periphery (Lang, 2003; Toma and Hallett, 2003)23,24 but also activity of the pyramidal neurons, which generate the. 37.
(39) final motor output to the spinal cord (Ikeda and Shibasaki, 2003).40 Furthermore, varying effects on NS’ and MP on the lesioned side might be explained by vulnerability effects, depending on the functional properties of M1 neurons. To our knowledge, only two studies exist that examined MRCPs in patients with frontal lesions caused by cerebrovascular events. McNabb et al. (1988)7 recorded MRCPs from one patient 6 weeks after the sudden onset of a dense right hemiplegia and mutism with left anterior cerebral artery territory infarction, involving the left medial frontal and parietal cortex and corpus callosum, and showed an attenuated Bereitschaftspotential and a less asymmetry of the NS' component of the premotor negativity with right finger than with left finger movement. The authors hypothesized that this difference was due to simultaneous activation of motor centers in both hemispheres. Singh and Knight (1990)10 recorded MRCPs from 11 patients with lesions centered in dorsolateral prefrontal cortex (5 right, 6 left) and all patients were studied at least 6 months post-lesion. The authors reported reduced or abolished BP and NS subcomponents in their patient group, while the MP component was relatively spared and suggested premotor (area 6). 38.
(40) and frontal eye field (area 8) make larger contributions to MRCP generation. Unilateral lesion of either the left or the right frontal cortex resulted in bilateral MRCP reduction indicating that each frontal lobe had bilateral input into sensorimotor regions. It is intriguing to find that the current data travel in a complete opposite way to those of previous reports. In the current study, the main lesion sites were allocated at the medial frontal regions, including SMA, which are different from the previous report with dorsolateral prefrontal involvement where premotor cortex may be engaged. From the physiological point of view, pre-SMA (Area F6) may convey inhibitory impulses, i.e. generation of negative seizures (Noachtar and Lüders, 1999; Satow et al., 2002)41,42; loss of motor function induced by electric stimulation to the negative motor areas (Lüders et al., 1995)43, to relevant motor regions in addition to excitatory ones. It is more likely that diminution of the inhibitory impulses of pre-SMA may contribute to the larger amplitudes of MRCP in the current ACA infarct patients (Figure 11). Another possibility is that more excitatory cortical regions are recruited for the motor execution functional set after a time lag of stroke as compared with the pre-stroke or early stroke state. The later possibility may also be attributed to the. 39.
(41) development of the current findings. However, this speculation requires further fMRI study for the elucidation.. 40.
(42) Normal. Left prefrontal lobe. Right prefrontal lobe. Medial frontal lobe. Striatum. +. SMA-proper (F3). Pre-SMA (F6) -. -. M1. M1. Left medial frontal lobe or SMA infarct. Left prefrontal lobe. Striatum. Right prefrontal lobe. Medial frontal lobe. + SMA-proper (F3). Pre-SMA (F6) -. -. M1. M1. Figure 11. Proposed model to illustrate that the diminution of the inhibitory impulses of pre-SMA (Area F6) may contribute to the release effect of M1 and the larger amplitude of MRCP in current patients with left medial frontal lobe or SMA infarct. 41.
(43) 第二節 其他相關性討論 The interpretation of supplementary motor areas (SMA) involvement is supported by anatomical studies. The prefrontal cortex is known to be connected to the SMA by two main routes. The first one connects the prefrontal cortex to the striatum, from there via pallidum to the thalamic nuclei ventralis anterior and ventralis lateralis and finally to the cortical motor areas. One of the cortical areas is the SMA. Afferent fibers from the above mentioned thalamic nuclei have been demonstrated (Jürgens, 1984).44 On the other hand a more direct cortico-cortical route between the prefrontal cortex and the mesial motor areas exists, connecting not only the rostral SMA with area 46 (Luppino et al., 1993; Lu et al., 1994),19,45 but also with prefrontal areas 8, 9, 11 and 12 (Bates and Goldman-Rakic,1993).18 These anatomical findings indicate that pre-SMA is involved in the control of motor processing and fulfils the ‘supramotor’ hypothesis (Rizzolatti et al., 1998).46 In addition to the contribution of the SMA, intracranial recordings (Ikeda et al., 1995; Neshige et al., 1988)5,47 and dipole analysis studies (Praamstra et al., 1996)48 found the contra- and ipsilateral sensorimotor cortex to be involved in the generation of the BP component. Therefore, disturbed activity of the bilateral sensorimotor areas 42.
(44) during movement preparation, possibly caused by deranged neuronal input from the prefrontal cortex (BA 46, 10, 12) via the ventral premotor cortex (Barbas and Pandya, 1987)49 may also contribute to the altered BPs in the current patients. The anterior cingulate circuit, origining in the anterior cingulated gyrus and projecting to the ventral striatum. The latter includes the nucleus accumbens, olfactory, and part of the ventromedial caudate and putamen. The ventral striatum then connects to the ventral and rostrolateral globus pallidus and rostrodorsal substantial nigra, which in turn projects to the paramedian part of the MD nucleus of thalamus ultimately projects back to the anterior cingulated cortex. Each cingulate gyrus has complex reciprocal connections with other limbic structures and frontal cortex and appears to provide an interface between the decision-making process of the frontal lobe and the emotional world of the limbic system. Dysfunction of the circuit results in the medial frontal-anterior cingulated syndrome with apathy and reduced initiative. The integrity of this circuit is critical for drive and motivation. The clinical manifestations of abulia or akinetic mutism appeared in the current four patient can probably be a result of functional or structural damage to the anterior cingulate circuit.. 43.
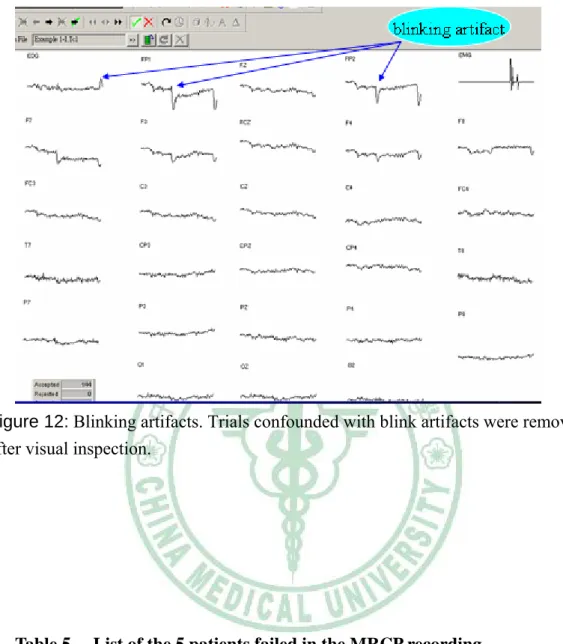
(45) 第三節 研究限制 (Study limitation) 1) Low spatial resolution: the main restriction of scalp-recorded potentials is the low spatial resolution. A direct identification of the neuronal structures underlying the MRCPs is not possible. Literature dealing with source localization of MRCPs exists. Source density studies found active generators at midline locations which were interpreted as SMA activity in a time period surrounding movement onset (Knösche et al., 1996)50 as well as during the BP-period (Cui et al., 1999).51 Recent functional magnetic resonance imaging (fMRI) studies, providing a much better spatial resolution, came to the conclusion that SMA, namely its anterior part (pre-SMA), is involved in the early stage of the movement preparation process (Lee et al., 1999; Cunnington et al., 2002).52,53 2) Old age: Recording of the movement-related cortical potentials requires good cooperation from the subjects. Avoidance of blinking artifacts (Figure 12), relaxation, proper timing and briskness of movements are especially important, and all these factors depend on the subject. Subjects failed in recording of the MRCPs in this study due to too much blinking artifacts are listed in Table 5.. 44.
(46) 3) Sample size: ACA infarct patients are relatively rare as compared with other types of ischemic stroke and cause the sample sizes in the current study being insufficient to allow further stratification according to acute or chronic stage. More subjects are necessary to observe alterations of the temporal or spatial distribution of the MRCP and differential effects on the MRCP subcomponents after lesions of the cortical motor areas.. 45.
(47) Figure 12: Blinking artifacts. Trials confounded with blink artifacts were removed after visual inspection.. Table 5.. List of the 5 patients failed in the MRCP recording Lesion location. Symptoms. P’t No.. Sex. Age. 1. F. 83. Left high medial frontal lobe. Abulia, Right leg weakeness. 2 3 4 5. M. 66. Left frontal and parietal lobe. Right leg weakness. F. 82. Right medial frontal lobe. Left leg weakeness. F. 83. Left medial frontal lobe. Right leg weakeness. M. 68. Left medial frontal lobe. Right leg weakness. All lesions were located in the anterior cerebral artery territory. 46.
(48) 第五章 結論與建議 第一節 結論 (Conclusion) In conclusion, by taking advantage of the superior temporal resolution of the MRCPs, we demonstrated enhanced activity (with ipsilesional dominantly) directly preceding movement onset and during movement execution in stroke patients with left ACA territory infarct. These results are in line with the idea of prefrontally mediated early preparatory processes (Wiese et al., 2004; Keidel, 1983),8, 54 presumably affected by medial structures (Cunnington et al., 2002).53 The results could be due to diminution of pre-SMA inhibitory inputs to the subsequent motor regions or due to the recruitment of the nearby excitatory cortical regions for the compensation of motor impairment of the ACA infarct.. 第二節 建議 (Suggestion) The MRCP paradigm used in this study enables us to examine movements initiated by the subject and the high temporal resolution of the EEG allowed the investigators to distinguish between the processes of motor planning and execution. Our findings complement imaging studies. 47.
(49) and provide an example of the successful application of the MRCPs to the study of vascular brain lesions. More subjects are necessary to determine the effects of temporal or spatial distribution of the MRCP and differential effects on the MRCP subcomponents under functional MRI image and MRCP topographic mapping. In this proposal, we demonstrate alterations in the movement related cortical network in the stroke patients by comparing ACA infarct patients’ MRCPs to those of a healthy control group and to observe how the change of cortical excitability will affect the MRCP behavior. Footing on this ground, we verify the role and the hypothetic accuracy of the MRCP generated regions of the brain. We believe the findings help out understand the functional reorganization of the motor preparation of the brain after ACA infarct. Further study with functional MRI is mandatory to visualize the alteration of set pattern for motor execution.. 48.
(50) 五、參考文獻 (References) 1.. Daly DD, Pedley TA (eds): Current practice of clinical EEG. 2nd ed. New York, Raven Press, 1990.. 2.. Kornhuber HH, Deecke L. Changes in the brain potential in voluntary movements and passive movements in man: readiness potential and reafferent potentials. Pflügers Arch Gesamte Physiol Menschen Tiere. 1965; 284:1–17.. 3.. Shibasaki H, Barrett G, Halliday E, Halliday AM. Components of the movement-related cortical potential and their scalp topography. Electroencephalogr Clin Neurophysiol. 1980; 49:213–226.. 4.. Deecke L, Scheid P, Kornhuber HH. Distribution of readiness potential, pre-motion positivity, and motor potential of the human cerebral cortex preceding voluntary finger movements. Exp Brain Res. 1969; 7:158 –168.. 5.. Ikeda A, Lüders HO, Shibasaki H, Collura TF, Burgess RC, Morris HH, Hamano T. Movement-related potentials associated with bilateral simultaneous and unilateral movements recorded from human supplementary motor area. Electroenceph Clin Neurophysiol 1995; 95:323–34.. 6.. Gerloff C. Movement-related cortical potentials in patients with focal brain lesions. In: Jahanshahi M, Hallett M, eds. The Bereitschaftspotential. Movement-Related Cortical Potentials. New York, NY: Kluwer. 49.
(51) Academic/Plenum Publishers; 2003. 7.. McNabb AW, Carroll WM, Mastaglia FL. "Alien hand" and loss of bimanual coordination after dominant anterior cerebral artery territory infarction. J Neurol Neurosurg Psychiatry. 1988;51(2):218-22.. 8.. Wiese H, Stude P, Nebel K, Osenberg D, Volzke V, Ischebeck W, Stolke D, Diener HC, Keidel M. Impaired movement-related potentials in acute frontal traumatic brain injury. Clin Neurophysiol. 2004;115:289–98.. 9.. Wiese H, Stude P, Nebel K, Osenberg D, Ischebeck W, Stolke D, Diener HC, Keidel M. Recovery of movement-related potentials in the temporal course after prefrontal traumatic brain injury: a follow-up study. Clin Neurophysiol. 2004; 115:2677–92.. 10. Singh J, Knight RT. Frontal lobe contribution to voluntary movements in humans. Brain Res 1990;531:45–54. 11. Shibasaki H. Movement-associated cortical potentials in unilateral cerebral lesions. J Neurol. 1975;209:189 –198. 12. Kitamura J, Shibasaki H, Takeuchi T. Cortical potentials preceding voluntary elbow movement in recovered hemiparesis. Electroencephalogr Clin Neurophysiol. 1996;98:149 –156. 13. Honda M, Nagamine T, Fukuyama H, Yonekura Y, Kimura J, Shibasaki H.. 50.
(52) Movement-related cortical potentials and regional cerebral blood flow change in patients with stroke after motor recovery. J Neurol Sci. 1997; 146:117–126. 14. Deecke L, Lang W, Heller HJ, Hufnagl M, Kornhuber HH. Bereitschaftspotential in patients with unilateral lesions of the supplementary motor area. J Neurol Neurosurg Psychiatry 1987; 50:1430–4. 15. Jahanshahi M, Jenkins IH, Brown RG, Marsden CD, Passingham RE, Brooks DJ. Self-initiated versus externally triggered movements. I. An investigation using measurement of regional cerebral blood flow with PET and movement-related potentials in normal and Parkinson’s disease subject. Brain 1995; 118:913–33. 16. Cunnington R, Iansek R, Bradshaw JL, Phillips JG. Movement-related potentials in Parkinson’s disease. Presence and predictability of temporal and spatial cues. Brain 1995; 118:935–50. 17. Witte OW. Lesion-induced plasticity as a potential mechanism for recovery and rehabilitative training. Curr Opin Neurol 1998; 11:655–62. 18. Bates JF, Goldman-Rakic PS. Prefrontal connections of medial motor areas in the rhesus monkey. J Comp Neurol 1993;336:211–28. 19. Luppino G, Matelli M, Camarda R, Rizzolatti G. Corticocortical connections of Area F3 (SMA-proper) and Area F6 (pre-SMA) in the macaque monkey. J. 51.
(53) Comp Neurol 1993 ;338:114–40. 20. Kolb B, Milner B. Performance of complex arm and facial movements after focal brain lesions. Neuropsychologia 1981;19:491–503. 21. Alexander GE, Crutcher MD. Parallel organization of functionally segregated circuits linking basal ganglia and cortex. Ann Rev Neurosci. 1986; 9: 357-81. 22. Cummings JL. Frontal-subcortical circuits and human behavior. Arch Neurol. 1993; 50:873-80. 23. Lang W. Surface recordings of the Bereitschaftspotential in normals. In: Jahanshahi M, Hallett M, eds. The Bereitschaftspotential: Movement-Related Cortical Potentials. New York, NY: Kluwer Academics/Plenum Publishers; 2003:19 –34. 24. Toma K, Hallett M. Generators of the movement-related cortical potentials and dipole source analysis. In: Jahanshahi M, Hallett M, eds. The Bereitschaftspotential: Movement-Related Cortical Potentials. New York, NY: Kluwer Academic/Plenum Publishers; 2003:113–30. 25. Wiese H, Stude P, Sarge R, Nebel K, Diener HC, Keidel M. Reorganization of motor execution rather than preparation in poststroke hemiparesis. Stroke. 2005; 36:1474-9. 26. Ikeda A, Yazawa S, Kunieda T, et al. Cognitive motor control in human. 52.
(54) pre-supplementary motor area studied by subdural recording of discrimination/selection-related potentials. Brain 1999;122:915–31. 27. Liepert J, Bauder H, Miltner WH, Taub E, Weiller, C. Treatment- induced cortical reorganization after stroke in humans. Stroke 2000; 31: 1210– 6. 28. Nelles G, Jentzen W, Jueptner M, Muller S, Diener HC. Arm training induced brain plasticity in stroke studied with serial positron emission tomography. NeuroImage 2001; 13: 1146–54. 29. Weiller C, Ramsay SC, Wise RSJ, Friston KJ, Frackowiak RSJ. Individual patterns of functional reorganization in the human cerebral cortex after capsular infarction. Ann Neurol 1993; 33:181–9. 30. Cramer SC, Nelles G, Benson RR, Kaplan JD, Parker RA, Kwong KK, Kennedy DN, Finklestein SP, Rosen BR. A functional MRI study of subjects recovered from hemiparetic stroke. Stroke. 1997; 28:2518 –27. 31. Cao Y, D’Olhaberriague L, Vikingstad EM, Levine SR, Welch KMA. Pilot study of functional MRI to assess cerebral activation of motor function after poststroke hemiparesis. Stroke 1998; 29:112–22. 32. Feydy A, Carlier R, Roby-Brami A, Bussel B, Cazalis F, Pierot L, Burnod Y, Maier MA. Longitudinal study of motor recovery after stroke: recruitment and focusing of brain activation. Stroke. 2002; 33:1610 –17.. 53.
(55) 33. Caramia MD, Iani C, Bernardi G. Cerebral plasticity after stroke as revealed by ipsilateral responses to magnetic stimulation. Neuroreport 1996;7:1756–60 34. Netz J, Lammers T, Hömberg V. Reorganization of motor output in the non-affected hemisphere after stroke. Brain 1997;120:1579–86 35. Caramia MD, Palmieri MG, Giacomini P, Iani C, Dally L, Silvestrini M. Ipsilateral activation of the unaffected motor cortex in patients with hemiparetic stroke. Clin Neurophysiol 2000;111:1990–6 36. Weiller C, Chollet F, Fristion KJ, Wise RSJ, Frackowiak RSJ. Functional reorganization of the brain in recovery from striatocapsular infarction in man. Ann Neurol 1992;31:463–72 37. Chollet F, DiPiero V, Wise RJS, Brooks DJ, Dolan RJ, Frackowiak RSJ. The functional anatomy of motor recovery after stroke in humans: a study with positron emission tomography. Ann Neurol 1991;29:63–71 38. Seitz RJ, Ho¨flich P, Binkofski F, Tellmann L, Herzog H, Freund HJ. Role of the premotor cortex in recovery from middle cerebral artery infarction. Arch Neurol 1998;55:1081–8 39. Green JB, Bialy Y, Sora E, Ricamato A. High-resolution EEG in poststroke hemiparesis can identify generators during motor tasks. Stroke 1999; 30: 2659–65.. 54.
(56) 40. Ikeda A, Shibasaki H. Generator mechanisms of the Bereitschaftspotential as studied by epicortical recording in patients with intractable partial epilepsy. In: Jahanshahi M, Hallett M, eds. The Bereitschaftspotential: Movement-Related Cortical Potentials. New York, NY: Kluwer Academic/Plenum Publishers; 2003:45–59. 41. Noachtar S, Lüders HO. Focal akinetic seizures as documented by electroencephalography and video recordings. Neurology. 1999;53(2):427-9. 42. Satow T, Ikeda A, Yamamoto J, Takayama M, Matsuhashi M, Ohara S, Matsumoto R, Begum T, Fukuyama H, Hashimoto N, Shibasaki H. Partial epilepsy manifesting atonic seizure: report of two cases. Epilepsia. 2002;43(11):1425-31. 43. Lüders HO, Dinner DS, Morris HH, Wyllie E, Comair YG. Cortical electrical stimulation in humans: the negative motor areas. Adv Neurol 1995; 67: 115–29. 44. Jürgens U. The efferent and afferent connections of the supplementary motor area. Brain Res 1984;300:63–81 45. Lu MT, Preston JB, Strick PL. Interconnection between the prefrontal cortex and the premotor areas in the frontal lobe. J Comp Neurol 1994; 341:375–92. 46. Rizzolatti G, Luppino G, Matelli M. The organization of the cortical motor system: new concepts. Electroenceph clin Neurophysiol 1998;106:283–96.. 55.
(57) 47. Neshige R, Lüders H, Shibasaki H. Recording of movement-related potentials from scalp and cortex in man. Brain 1988;111:719–36. 48. Praamstra P, Stegeman DF, Horstink MWIM, Cools AR. Dipole source analysis suggests selective modulation of the supplementary motor area contribution to the readiness potential. Electroenceph clin Neurophysiol 1996;98:468–77. 49. Barbas H, Pandya DN. Architecture and frontal cortical connections of the premotor cortex (area 6) in the rhesus monkey. J Comp Neurol 1987; 256:211–28. 50. Knösche T, Praamstra P, Stegemann D, Peters M. Linear estimation discriminates midline sources and a motor cortex contribution to the readiness potential. Electroenceph clin Neurophysiol 1996;99: 183–90. 51. Cui RQ, Huter D, Lang W, Deecke L. Neuroimage of voluntary movement: topography of the Bereitsschaftspotential, a 64-channel DC current source density study. Neuroimage 1999; 9:124–34. 52. Lee KM, Chang KH, Roh JK. Subregions within the supplementary motor area activated at different stages of movement preparation and execution. Neuroimage 1999;9:117–23. 53. Cunnington R, Windischberger C, Deecke L, Moser E. The preparation and execution of self-initiated and externally-triggered movement: a study of. 56.
(58) event-related fMRI. Neuroimage 2002; 15:373–85. 54. Keidel M. Motor intention potential. Electrophysiologic objectization of a single intended movement. Naturwissenschaften. 1983; 70:180–5.. 57.
(59)
數據

+6

Outline
相關文件
28 Specifically, in this study we determined that (1) individuals having comorbid OSA and MetS, that is SZ, have a greater prevalence of calcified carotid artery atherosclerotic
原文題目(出處): Prevalence of calcified carotid artery atheromas on the panoramic images of patients with syndrome Z, coexisting obstructive sleep apnea, and metabolic
A lingual mucoperiosteal flap was raised in the 48 region after making an incision from the medial aspect of anterior border of the mandibular ramus and extending to the
Winnick, “Salivary gland inclusion in the anterior mandible: report of a case with a review of the literature on aberrant salivary gland tissue and neoplasms,” Oral Surgery,
The noncalcifying and LC-rich CEOTs occurred only in Asian patients, had a predilection for the anterior and premolar region of the maxilla, had none of calcification foci in the
In cases of anterior intrabony maxillary midline lesions with cortical erosion, entities such as nasopalatine duct cyst, keratocystic odontogenic tumor, periapical in-
In this case, a 16-year-old female presented with a well-demarcated radiolucent lesion of 2.5 cm di- ameter in the anterior maxillary region associated with an impacted
The case presented here is of a geriatric patient who presented to us with a fracture at the right parasymphysis and left dentoalveolar region of the mandible and was su ffering
