行政院國家科學委員會補助專題研究計畫
成果報告
計畫名稱: 中國地區醫療支出與所得差距之計量研究
計畫類別: X 個別型計畫
□ 整合型計畫
計畫編號:NSC
97-2410-H-009-060
執行期間:2008 年 11 月 01 日至 2009 年 07 月 31 日
計畫主持人:
周文林
共同主持人:--計畫參與人員:
齊孝慈,沈玟均,陳俊良,莊宏瑋
成果報告類型(依經費核定清單規定繳交):x 精簡報告
□完整報告
本成果報告包括以下應繳交之附件:
□赴國外出差或研習心得報告一份
□赴大陸地區出差或研習心得報告一份
□出席國際學術會議心得報告及發表之論文各一份
□國際合作研究計畫國外研究報告書一份
處理方式:除產學合作研究計畫、提升產業技術及人才培育研究計畫、
列管計畫及下列情形者外,得立即公開查詢
□涉及專利或其他智慧財產權,□一年□二年後可公開查詢
執行單位:
中
華
民
國
年
月
日
(一) 中、英文摘要及關鍵詞
中文摘要
本計畫利用中國城鄉地區的資料,探討中國的醫療支出不均,所得
不均,與(地方)政府財政次赤字之間的長期關係。採用的計量方法
是由 Westerlund and Edgerton (2007) 開發的一套新的面板共積
檢定方法。研究結果顯示,所得不均與政府財政赤,能夠解釋中國
城鄉地區醫療支出的不均狀態。如欲降低城鄉醫療支出的不均情
況,我們的研究結果指出,中國政府需要拿出一套可行的一個長期
方案,使得經濟落後的貧困地區,能夠有較為快速的增長 ,同時
維持穩健的財政狀況。
關鍵字:醫療支出的不均,所得不均,政府財政次赤字,面板共積
檢定方法。
英文摘要
ABSTRACT
This project examines the long-run relationship between health expenditure inequality, income inequality, and provincial government budget deficits by using new panel cointegration tests of Westerlund and Edgerton (2007) with health care expenditure data in China’s urban and rural areas. We find the income inequality and real provincial government budget deficits are useful in explaining the disparity in health care expenditure prevailing between urban and rural areas. In order to reduce health inequality, one long-run policy suggestion from our findings is for the government to implement more rapid economic development and stronger financing schemes in poorer rural areas.
Keywords: health care expenditure inequality, income inequality, government budget deficits,
(二) 報告內容
1. IntroductionAn important feature of China’s economic reforms which began in 1978 is the dramatic change in its health system from a centrally planned system to a market-based one (Ma, Lu and Quan, 2008). Unfortunately, as admitted by the Chinese government, the reform in the health system has not been successful. The most cited problems with China’s reformed health system include the heavy reliance on private financing, dramatic falling of the health insurance coverage, and rising health care costs (Yip and Hsio, 2008; Wagstaff and Lindelow, 2008). To cite one example, between 1993 and 2003, the health insurance coverage rate in urban areas dropped from around 70 percent to 55 percent. The drop was much more dramatic in the rural areas, from the peak of around 85 percent in 1975 to about 9.5 percent in 2003 (Ma, Lu and Quan, 2008). As a result, a majority of the rural population must pay out of pocket for all heath services. The out-of-pocket share of health care spending in China has risen sharply from 20.4 percent in 1978 to 53.6 percent in 20041.
There has been growing concern on the widening inequalities in health and their socioeconomic impacts in the literature. For example, Liu, Hsiao, and Eggleston (1999) observed that the growing gap in income and health status between urban and rural residents is correlated with increasing gaps in income and health care utilization. Yip and Mahal (2008) found an increase in interprovincial inequality in life expectancy at birth and infant mortality between 1980 and 2000. The same was the case with within-rural, within-urban, and between rural-urban inequalities in infant mortality (Zhang and Kanbur, 2005).
Possibly due to the lack of time series data, the above-mentioned studies on inequalities in health are largely relying on the survey research, or cross-sectional models, time-series econometric methods were rarely used. Cross-section models generally do not allow the time necessary for changes in the time-dependent independent variables to have an impact on the dependent variable. To allow for time lag in the adjustment of the dependent variable, we pool the cross-section data with time-series data. In this project we investigate the relationship between health and income inequality in a panel setting by utilizing pooled cross-section and time-series data. The main objective of this project is to investigate the relationship between health inequality, income inequality, and government budget deficits in China by using new panel cointegration tests of Westerlund and Edgerton (2007, 2008) in a panel setting. Our use of the government budget deficits and the income inequality variables in the panel tests is motivated by Gerdtham and Jönsson (2000) who make comments on important issues for future research on the determinants of health care expenditure. One comment is that: “Empirical studies in recent years have been remarkably unwilling to test “new”variables in their models. One possible candidate as an explanatory variable is government budget deficits, which are likely to be a strong constraint on public health expenditure.”In addition, we also examine how the “new”variable on income inequality would explain the regional disparity in health care
expenditure in China. To facilitate the analysis, more disaggregate panel data on urban and rural households’per capita health care expenditure in China are collected in 28 provinces for 1995-20062.
The structure of the study is as follows. Section 2 is on the test methods, and empirical results. The major findings and their policy implications are discussed in Section 3.
2. Panel cointegration tests
In order to understand the factors that contributed to the health inequality, we utilize the panel cointegration tests developed by Westerlund and Edgerton (2007, 2008) with pooled cross-section and time-series data for urban and rural areas in China. Unlike most panel cointegration tests that either do not handle the structural changes or unable to handle cross-sectional
dependence, this new version of panel test overcomes both problems. The tests are designed based on the Lagrange multiplier (LM) principle, allowing for cross-sectional dependence and have been shown to work well in small samples. Details of the tests are described in the re Westerlund and Edgerton (2007, 2008) and will not be repeated here.
2.1 Data for health spending and income inequality measures
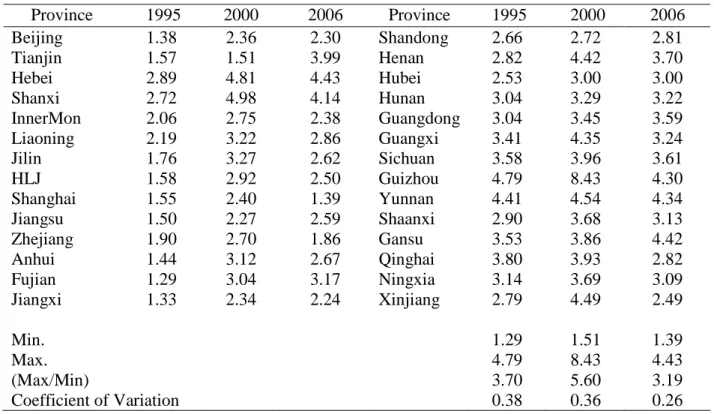
More disaggregate panel data classified by urban and rural areas are used to test the relationship between health inequality and income inequality. As the officially and privately published Gini coefficients are not useful in time series analysis due to the short time span, we computed ratios of per capita disposable income of urban households to per capita net income of rural households for 28 Chinese provinces, and use the resulting ratios as a proxy variable for the income equality. As data with the urban-rural classification are available in 1995, our sample starts from 1995. Similarly, we obtain the ratios of per capita health expenditure of urban households to per capita health expenditure of rural households, and treat the resulting ratios as a proxy for health inequality. Table 1 displays the values of the ratios on per capita health expenditure for three selected years, 1995, 2000, and 2006. Our compiled data show that average real per capita household health care expenditure in urban areas was RMB57.04 yuan in 1995, while that of a rural household was only RMB24.53 yuan. The corresponding figures were
RMB270.78 and RMB95.06 in 2006, indicating a widening urban-rural gap in health care spending over time. The health expenditure inequality between the most and least serious provinces increased from 3.70 in 1995 to 5.60 in 2000 before declining to 3.19 in 2006.
In addition to the income inequality measure, we also compute the ratio of the variability (standard deviation) of urban household income to that of rural household income. We consider a new variable on provincial government budget deficits. The importance of this variable has been given in Gerdtham and Johsson (2000). The governmental budget deficits are likely to become a strong constraint on public health expenditure in many Chinese provinces, they are of particular relevance and importance to China. Data for provincial government budget deficits are adjusted for inflation rates. The major sources for our data various issues of China Statistical
Yearbook, Yearbook of Public Health in Peoples’RepublicofChina,and various provincial Statistical Yearbooks.
2.2 Test results for relationship between inequalities in health and in income
As mentioned in Section 1, our use of the income inequality and government budget deficits in the panel cointegration tests was motivated byGerdtham and Johsson(2000). Details of the test model is specified in the Appendix which links the health care expenditure inequality (Y) to income inequality (X) and one of the following other factors: variability in income inequality (Z1), real government budget deficits (BD), and variability in real government budget
deficits (Z2). Table 2 shows the test results of panel cointegraion3using the Lagrange
Multiplier-type test developed in Westerlund and Edgerton (2007)4which accounts for the cross-sectional
3Prior to the cointegration tests, we have tested the stationarity property of the series, and all series are found to be
nonstationary.
4We also tried the tests in Westerlund and Edgerton (2008) which permits structural changes. Since the test program
dependency, an important property when using pooled cross-section and time-series data. It can be easily seen from Table 2 that the null hypothesis of cointegration in the panel can not be rejected, suggesting the existence of long-run relationship between health inequality and income inequality, or that between variability in income inequality and variability in real government budget deficits, etc. in the panel. These test results suggest that income inequality (or its variability), and provincial government budget deficits (or their variability) are useful in explaining the health care spending inequality between the urban and rural areas in China. These results may also suggest that the health inequality has a high chance to be affected by the income gap between the richer urban and poorer rural households, and the local government’s budget deficits.
The recent emphasis on health in China’s government policies, and the large increases in government expenditure on health indicate that the Chinese government’s commitment to tackle the health sector problems is stronger than five years ago (Wagstaff and Lindelow, 2008). Our findings here suggest that to tackle the issue on health inequalities, it is important to have policies that will make the poorer areas to grow faster and the government finances to become stronger. Our findings also provide supportive evidence to the Chinese government’s recent policy shift from the richer coastal areas to the poorer rural areas aiming at achieving equitable growth.
3. Conclusions
Previous studies on health inequalities in China largely relied on survey methods with cross-section data. In this project, we attempt to add quantitative content to the research on health inequality by using econometric methods with pooled cross-section and time-series data.
Examining historical data suggests that inequalities exist in the health care expenditure across regions. The likely causes that contributed to this diverging situation are explored using a new panel cointegration test. We investigate the long-run relationship between health inequality, income inequality and government budget deficits using panel cointegration tests with panel data for urban and rural areas. We find income inequality, and real provincial government budget deficits are useful in explaining the long-run behavior of health inequality, more specifically, the inequality between the urban and rural areas. Moreover, we contribute to the literature by providing the earlier studies (e.g., Lou, 2008) on regional fiscal disparities that were based on survey approaches or descriptive statistics with systematic quantitative evidence that the fiscal difficulties (or deficits) are constraining the rural areas’health care spending, hence resulting in health care disparities. Our findings also suggest that to tackle the issue on health inequality, it is important to make the poorer areas to grow faster and to improve the government finances in poorer areas. Finally, our test results render quantitative support for the Chinese government’s recent policy shift from the richer coastal areas to the poorer rural areas aiming at achieving the goal of equitable growth.
APPENDIX
Panel cointegration test equation for health expenditure inequality
it kt t
it X BD Z
Y 11 2 1 k 1,2, (A1)
where Y = health care expenditure inequality, X= income inequality, BD= real government budget deficits, Z1=variability in income inequality, and Z2= variability in real government
REFERENCES
Gerdtham, U-G., Johsson, B. 2000. International comparisons of health expenditure: theory, data and econometric analysis. In A.J. Culyer and J.P. Newhoouse, ed., Handbook of Health
Economics, Volume 1A, Amsterdam, Elsevier, 11-53.
Liu, Y., Hsiao, W.C., Eggleston, K., 1999. Equity in health and health care: The Chinese experience.
Social Science and Medicine 49, 1349-1356.
Lou, J. 2008. The reform of intergovernmental fiscal relations in China: Lessons learned. In Lou, J. and Wang, S. (eds), Public Finance in China: Reform and Growth for A Harmonious Society. Washington, D.C.: The World Bank, 155-169.
Ma, J., Lu M., Quan, H., 2008. From a national, centrally planned health system to a system based on the market: Lessons from China. Health Affairs 27, 937-948.
Wagstaff, A. and Lindelow, M. 2008. Health reform in rural China: Challenges and options. In Lou, J. and Wang, S. (eds), Public Finance in China: Reform and Growth for A Harmonious
Society. Washington, D.C.: The World Bank, 265-286.
Westerlund, J. Edgerton, D.L., 2007. A panel bootstrap cointegration test. Economics Letters 97, 185-190.
Westerlund, J. Edgerton, D.L., 2008. A simple test for cointegration in dependent panels with structural breaks. Oxford Bulletin of Economics and Statistics 70, 665-690.
Yip, W., Hsiao, W.C., 2008. The Chinese health system at a crossroads. Health Affairs 27, 460-468. Yip, W., Mahal, A., 2008. The health care system of China and India: Performance and future
challenges. Health Affairs 27, 921-932.
Zhang, X., Kanbur, R., 2005. Spatial inequality in education and health care in China. China
Table 1. Ratios of urban HCE to rural HCE by province in selected years Province 1995 2000 2006 Province 1995 2000 2006 Beijing 1.38 2.36 2.30 Shandong 2.66 2.72 2.81 Tianjin 1.57 1.51 3.99 Henan 2.82 4.42 3.70 Hebei 2.89 4.81 4.43 Hubei 2.53 3.00 3.00 Shanxi 2.72 4.98 4.14 Hunan 3.04 3.29 3.22 InnerMon 2.06 2.75 2.38 Guangdong 3.04 3.45 3.59 Liaoning 2.19 3.22 2.86 Guangxi 3.41 4.35 3.24 Jilin 1.76 3.27 2.62 Sichuan 3.58 3.96 3.61 HLJ 1.58 2.92 2.50 Guizhou 4.79 8.43 4.30 Shanghai 1.55 2.40 1.39 Yunnan 4.41 4.54 4.34 Jiangsu 1.50 2.27 2.59 Shaanxi 2.90 3.68 3.13 Zhejiang 1.90 2.70 1.86 Gansu 3.53 3.86 4.42 Anhui 1.44 3.12 2.67 Qinghai 3.80 3.93 2.82 Fujian 1.29 3.04 3.17 Ningxia 3.14 3.69 3.09 Jiangxi 1.33 2.34 2.24 Xinjiang 2.79 4.49 2.49 Min. 1.29 1.51 1.39 Max. 4.79 8.43 4.43 (Max/Min) 3.70 5.60 3.19 Coefficient of Variation 0.38 0.36 0.26
Note: Sichuan combines Sichuan Province and Chongqing City.
Table 2 Panel test results for relationship between health inequality, income inequality, and real budget deficits
Dependent variable: Health expenditure inequality (Y)
Independent variables LM statistica pvalueb
1. Income inequality (X) -1.073 0.944
2. Variability in X (Z1) -0.670 0.876
3. Real budget deficits (BD) -0.623 0.910
4. Variability in BD (Z2) -0.250 0.686
5. X and BD 2.083 0.938
6. X and Z2 1.846 0.992
7. Z1and BD 2.083 0.910
8. Z1and Z2 1.146 1.000
Notes: Null hypothesis (H0) is: cointegration in the panel against alternative
hypothesis (H1) of no cointegration. aLM=Lagrange multiplier. See Westerlund and
Edgoerton (2007) for details of the test procedure. bThe p-value denotes the
(三) 計畫成果自評
研究內容是按照原計畫進行的,因此內容與原計畫相符的程度甚高。
主要成果已經投到國際期刊 Health Economic
s
,並且已獲接受。
茲附上該期刊編輯四月份關於評審的來函如下。
******************************************************************* >Date: 28-Apr-2009 > > Dear Author >> We would like to inform you that your manuscript is accepted for publication, > with two conditions.
>
> 1. We ask that you go over your manuscript and change the word "health" to > "health spending" or "health expenditure" or "health care" if that's what it > means. You use the term health inequality and health expenditure (for > example) interchangeably and it is very confusing. In the health economics > literature, if we say "health", we mean health outcome and health status. >
> 2. We ask that you resubmit this revision end of April 29 (UK time). >
> We hope this is agreeable to you. >
> Manuscript ID HEC-08-0248.R3 entitled "REGIONAL INEQUALITY IN >CHINA’S HEALTH CARE EXPENDITURES" which you submitted to Health >Economics, has been reviewed.
>
> The referee(s) have recommended publication, but also suggest some minor > revisions to your manuscript. Therefore, I invite you to respond to the > referee(s)' comments and revise your manuscript.
>
> You can upload your revised manuscript and submit it through your Author
> Center. Log intohttp://mc.manuscriptcentral.com/hec and enter your Author
> Center, where you will find your manuscript title listed under "Manuscripts > with Decisions".
>
> When submitting your revised manuscript, you will be able to respond to the > comments made by the referee(s) in the space provided. You can use this > space to document any changes you make to the original manuscript. >
> Once again, thank you for submitting your manuscript to Health Economics. I > look forward to receiving your revision.
> Sincerely, > > > Dr Winnie Yip > Health Economics > wyip@hsph.harvard.edu