The Ne w E n g l a nd Jo u r n a l o f Me d i c i ne
HEPATITIS B e ANTIGEN AND THE RISK OF HEPATOCELLULAR CARCINOMA
HWAI-I YANG, M.SC., SHENG-NAN LU, M.D., PH.D., YUN-FAN LIAW, M.D., SAN-LIN YOU, PH.D., CHIEN-AN SUN, SC.D., LI-YU WANG, PH.D., CHUHSING K. HSIAO, PH.D., PEI-JER CHEN, M.D., PH.D., DING-SHINN CHEN, M.D., AND CHIEN-JEN CHEN, SC.D., FORTHE TAIWAN COMMUNITY-BASED CANCER SCREENING PROJECT GROUP*
ABSTRACT
Background The presence of hepatitis B e antigen (HBeAg) in serum indicates active viral replication in hepatocytes. HBeAg is thus a surrogate marker for the presence of hepatitis B virus DNA. We conducted a prospective study to determine the relation between positivity for hepatitis B surface antigen (HBsAg) and HBeAg and the development of hepatocellular carcinoma.
Methods In 1991 and 1992, we enrolled 11,893 men without evidence of hepatocellular carcinoma (age range, 30 to 65 years) from seven townships in Taiwan. Serum samples obtained at the time of enrollment were tested for HBsAg and HBeAg by radioimmunoas-say. The diagnosis of hepatocellular carcinoma was ascertained through data linkage with the computer-ized National Cancer Registry in Taiwan and with death certificates. We performed a multiple regres-sion analysis to determine the relative risk of hepa-tocellular carcinoma among men who were positive for HBsAg alone or for HBsAg and HBeAg, as com-pared with those who were negative for both.
Results There were 111 cases of newly diagnosed hepatocellular carcinoma during 92,359 person-years of follow-up. The incidence rate of hepatocellular carcinoma was 1169 cases per 100,000 person-years among men who were positive for both HBsAg and HBeAg, 324 per 100,000 person-years for those who were positive for HBsAg only, and 39 per 100,000 per-son-years for those who were negative for both. Af-ter adjustment for age, sex, the presence or absence of antibodies against hepatitis C virus, cigarette-smok-ing status, and use or nonuse of alcohol, the relative risk of hepatocellular carcinoma was 9.6 (95 percent confidence interval, 6.0 to 15.2) among men who were positive for HBsAg alone and 60.2 (95 percent confidence interval, 35.5 to 102.1) among those who were positive for both HBsAg and HBeAg, as com-pared with men who were negative for both.
Conclusions Positivity for HBeAg is associated with an increased risk of hepatocellular carcinoma. (N Engl J Med 2002;347:168-74.)
Copyright © 2002 Massachusetts Medical Society. From the Graduate Institute of Epidemiology, College of Public Health, National Taiwan University, Taipei (H.-I.Y., S.-L.Y., C.K.H., C.-J.C.); the Department of Gastroenterology, Kaohsiung Chang-Gung Memorial Hos-pital, Kaohsiung (S.-N.L.); Gung Memorial Hospital and Chang-Gung University, Taoyuan (Y.-F.L.); the Department of Public Health, Na-tional Defense Medical Center, Taipei (C.-A.S.); the Graduate Institute of Aboriginal Health, Tzu Chi University, Hualien (L.-Y.W.); and the Liver Re-search Unit and Hepatitis ReRe-search Center, National Taiwan University Hos-pital (P.-J.C., D.-S.C.) — all in Taiwan. Address reprint requests to Dr. Chien-Jen Chen at the College of Public Health, National Taiwan University, 1 Jen-Ai Rd., Section 1, Taipei 10018, Taiwan, or at [email protected]. *Other members of the Taiwan Community-Based Cancer Screening Project Group are listed in the Appendix.
HRONIC hepatitis B virus (HBV) infection is a serious clinical problem because of its worldwide distribution and potential for ad-verse sequelae, including hepatic cirrhosis and hepatocellular carcinoma. It is particularly prev-alent in the Asian–Pacific region, where patients usu-ally acquire the infection at the time of birth or in early childhood.
The natural course of chronic HBV infection ac-quired early in life can be divided into three phases.1,2
The first phase is characterized by active replication of HBV, positivity for hepatitis B e antigen (HBeAg), and normal-to-low levels of serum aspartate amino-transferase and alanine aminoamino-transferase. The second phase, characterized by immune clearance, usually oc-curs from the age of 15 to 35 years, during which hep-atitis flares may occur as the result of specific, T-lym-phocyte–mediated cellular responses to viral antigens and apoptosis of hepatocytes. This phase subsides as viral replication declines, with the appearance of anti-bodies against HBeAg and clinical remission. In the third, or residual, phase, patients are positive for hep-atitis B surface antigen (HBsAg) and negative for HBeAg, and they do not have active liver disease.1,2
Epidemiologic studies have shown that positivity for HBsAg is one of the most important risk factors for hepatocellular carcinoma.3-5
Positivity for HBeAg usually indicates active rep-lication of HBV. Loss of detectable HBeAg, together with the emergence of antibodies against HBeAg, has been used as a key end point in studies of the efficacy of various agents, including lamivudine and interferon, for the treatment of chronic hepatitis B.6,7 However,
the role of positivity for HBeAg in the prediction of hepatocellular carcinoma remains inconclusive. Various studies of case series have found that the prevalence of HBeAg was lowest among patients with
hepatocel-C
H E PAT I T I S B e A N T I G E N A N D H E PATO C E L LU L A R C A R C I N O M A
lular carcinoma, highest among patients with chronic hepatitis B, and intermediate among those with liver cirrhosis.8,9 In several case–control studies, however,
the prevalence of HBeAg was significantly higher among HBsAg-positive patients with hepatocellular carcinoma than among matched HBsAg-positive con-trols.10-14 All these studies were cross-sectional in
de-sign, with disease status and the prevalence of antigen positivity determined at the same time. The studies did not determine whether positivity for HBeAg preceded the onset of hepatocellular carcinoma. We conducted a prospective study of the relation between positivity for HBeAg and the risk of hepatocellular carcinoma among 11,893 men in Taiwan.
METHODS
Study Cohort
From 1991 to 1992, we invited all 47,079 men between the ages of 30 and 65 years who were living in seven townships in Taiwan to participate in the study; the men were contacted by mail. A total of 11,893 men (25 percent) agreed to participate. Each subject pro-vided written informed consent for us to conduct an interview, col-lect a blood specimen, and perform various serologic and biochem-ical assays. The study was conducted between February 1991 and September 2000.
Data Collection and Blood Tests
All the men were interviewed in person with the use of a struc-tured questionnaire administered by well-trained public health nurs-es. The men were questioned about sociodemographic character-istics, diet, cigarette smoking, consumption of alcohol, betel-nut chewing, their medical and surgical history, and any family history of hepatocellular carcinoma or liver cirrhosis. A 10-ml specimen of blood was collected with the use of a disposable vacuum syringe. Samples of serum separated on the day of blood collection were kept in a freezer (at –70°C) until they were assayed. The specimens were tested at the time of enrollment for HBsAg and HBeAg by radioimmunoassay with the use of a commercial kit (Abbott Lab-oratories) and were tested for antibodies against hepatitis C virus by enzyme immunoassay with the use of a second-generation com-mercial kit (Abbott Laboratories).
For men in whom hepatocellular carcinoma was diagnosed during follow-up who were positive for HBsAg and negative for HBeAg at enrollment, tests for antibodies against HBeAg and HBV DNA in serum samples obtained at the time of enrollment were performed in 2002 as part of a nested case–control substudy. For each man with hepatocellular carcinoma, we identified two healthy controls matched for age, date of enrollment, and township, except that for each of two men with hepatocellular carcinoma, there was only one matched control for whom frozen serum samples were available. Thus, frozen serum samples collected at the time of enrollment were available for a total of 44 men with hepatocellular carcinoma and 86 matched controls who were positive for HBsAg and neg-ative for HBeAg. These samples were tested for antibodies against HBeAg with the use of an enzyme-linked immunoassay (Abbott Laboratories) and were tested for HBV DNA with the use of a branched-chain DNA assay (Quantiplex, Chiron), according to the manufacturer’s instructions. The threshold of detection for the quantitative assay of DNA was 2.5 pg per milliliter.
Follow-up for Hepatocellular Carcinoma
In Taiwan, interferon, lamivudine, or other antiviral or immune therapy was rarely used to treat chronic hepatitis B before 2001. The Bureau of National Health Insurance in Taiwan did not provide
reimbursement for the cost of treatment with lamivudine until March 2001. Since treatment with interferon alfa is expensive and has severe side effects that make it difficult to tolerate, the Bureau of National Health Insurance only recently began to provide reim-bursement for the cost of this treatment. Other antiviral or immune therapies are also rarely used to treat chronic hepatitis B in Taiwan. For these reasons, we did not refer our subjects with chronic hep-atitis B to the hospital for treatment after enrollment.
At the time of enrollment, none of the men had known hepato-cellular carcinoma on the basis of screening tests (abdominal ultra-sonography and serologic tests), interviews, and the absence of link-age with the National Cancer Registry. Cases of hepatocellular carcinoma were ascertained by computerized linkage of data with information from the National Cancer Registry in Taiwan for the period from January 1, 1984, through September 30, 2000. In ad-dition, we linked data with information from death certificates to identify deaths from cases of hepatocellular carcinoma that were not included in the National Cancer Registry. The diagnosis was based on pathological examination in 56 men and on the results of ab-dominal ultrasonographic, angiographic, or computed tomograph-ic studies combined with an elevated serum alpha-fetoprotein level (»400 ng per milliliter) in 55 men.10-13
Statistical Analysis
The person-years of follow-up for each subject were calculated from the date of enrollment to the date of the diagnosis of newly developed hepatocellular carcinoma, the date of death, or the date of the last link to data from the National Cancer Registry (Septem-ber 30, 2000), whichever came first. Incidence rates were calculated by dividing the number of incident cases of hepatocellular carcino-ma by the number of person-years of follow-up. Data for men in whom hepatocellular carcinoma was not diagnosed were censored at the date of death or the last date of follow-up (September 30, 2000). A Cox’s proportional-hazards model was used to estimate the relative risk of hepatocellular carcinoma associated with positivity for HBsAg and HBeAg and other risk factors, including advanced age, positivity for antibodies against hepatitis C virus, cigarette smoking, and consumption of alcohol. The 95 percent confidence intervals for the relative risks were also calculated. Significance lev-els were determined with the use of two-tailed tests. The cumulative incidence of hepatocellular carcinoma was calculated for men who were negative for both HBsAg and HBeAg, those who were positive for HBsAg alone, and those who were positive for both HBsAg and HBeAg, with the use of the Nelson–Aalen method (a nonpara-metric method for estimating the cumulative hazard).15-17 For the
130 men included in the nested case–control substudy described above, we used logistic-regression analysis to determine the associ-ation between the level of HBV DNA and hepatocellular carcinoma. Statistical analysis was performed with Stata software (Stata).
RESULTS
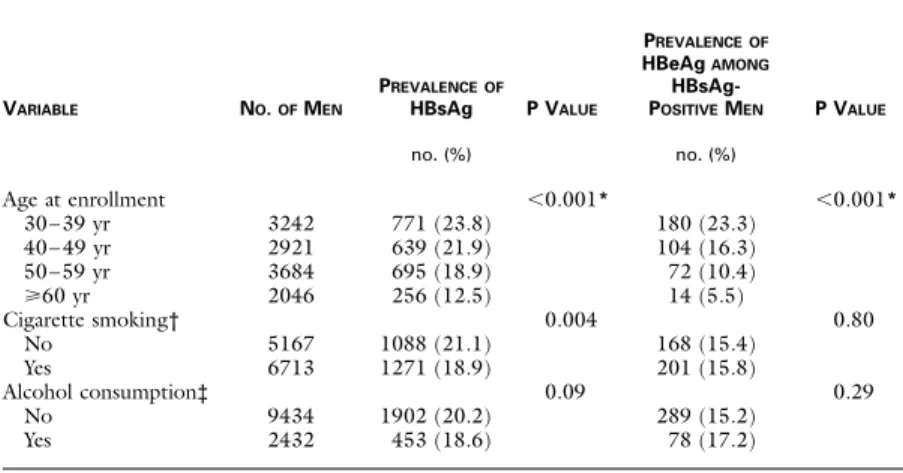
The prevalence of HBsAg among all men and the prevalence of HBeAg among those who were positive for HBsAg are shown in Table 1 according to age, cig-arette-smoking status, and use or nonuse of alcohol. The older the age, the lower the prevalence of HBsAg and HBeAg. The prevalence was consistent with the rates reported previously in Taiwan.1,2 Thus, we
con-sidered the study cohort to be representative of the general population of Taiwanese men in terms of the prevalence of HBsAg and HBeAg.
Men who smoked and those who drank alcohol had a lower prevalence of HBsAg alone but a higher prev-alence of HBeAg among those who were positive for HBsAg than did nonsmokers and nondrinkers. But
The Ne w E n g l a nd Jo u r n a l o f Me d i c i ne
the difference was statistically significant only for the prevalence of HBsAg alone among cigarette smokers and nonsmokers. Age and cigarette-smoking status dif-fered significantly among the men who were negative for both HBsAg and HBeAg, those who were positive only for HBsAg, and those who were positive for both HBsAg and HBeAg (P<0.001 and P=0.02, respectively). The rates of use and nonuse of alcohol were similar in the three groups of men (P=0.14).
A total of 111 cases of hepatocellular carcinoma were diagnosed during a follow-up period of 92,359 person-years; the overall incidence rate was 120.2 cases per 100,000 person-years. The incidence rate was 39.1 among men who were negative for both HBsAg and HBeAg, 324.3 among those who were positive only for HBsAg, and 1169.4 among those who were posi-tive for both HBsAg and HBeAg (Table 2). The prev-alence of HBeAg was 39 percent among the men who were positive for HBsAg. The cumulative incidence of hepatocellular carcinoma is shown in Figure 1 for the three groups. The men who were positive for both HBsAg and HBeAg had a much higher cumulative incidence of hepatocellular carcinoma than those who were positive only for HBsAg and an even higher in-cidence than those who were negative for both (P< 0.001 for both comparisons). The longer the follow-up, the greater the differences among the three groups. Table 3 shows the results of the multiple-regression analysis with the use of the Cox proportional-hazards model. After adjustment for other risk factors, the rel-ative risk of hepatocellular carcinoma was 9.6 (95 per-cent confidence interval, 6.0 to 15.2) for men who were positive for HBsAg alone and 60.2 (95 percent
confidence interval, 35.5 to 102.1) for those who were positive for both HBsAg and HBeAg, as compared with men who were negative for both. An older age at the time of enrollment, the presence of antibodies against hepatitis C virus, cigarette smoking, and con-sumption of alcohol were also associated with an in-creased risk of hepatocellular carcinoma. The findings were similar when the data were stratified according to age, cigarette-smoking status, and use or nonuse of alcohol, in an analysis adjusted for other risk factors (Table 4).
In the nested case–control analysis that involved 130 men who were positive for HBsAg and negative for HBeAg (44 men with newly diagnosed hepato-cellular carcinoma and 86 matched controls), 120 men (92 percent) were positive for antibodies against HBeAg, and 29 (22 percent) were positive for HBV DNA. The proportion of men who were positive for antibodies against HBeAg did not differ significantly between men with hepatocellular carcinoma and con-trols (P=0.16). Seventeen men with hepatocellular carcinoma (39 percent) and 12 controls (14 percent) had detectable serum levels of HBV DNA (>2.5 pg per milliliter). The odds ratio for the development of hepatocellular carcinoma was 3.9 (95 percent confi-dence interval, 1.6 to 9.2) for men who had detectable HBV DNA, as compared with those who had unde-tectable levels. The odds ratio increased with increases in the level of HBV DNA (Table 5).
DISCUSSION
It has been reported that in most patients with hep-atocellular carcinoma, the disease develops after the
*P values are based on a test for trend. †Data were not available for 13 men. ‡Data were not available for 27 men.
TABLE 1. PREVALENCEOF HEPATITIS B SURFACE ANTIGEN (HBsAg) AND HEPATITIS B e ANTIGEN (HBeAg) IN 11,893 MENIN TAIWAN.
VARIABLE NO. OF MEN PREVALENCEOF HBsAg P VALUE PREVALENCEOF HBeAg AMONG HBsAg-POSITIVE MEN P VALUE no. (%) no. (%) Age at enrollment 30–39 yr 40–49 yr 50–59 yr »60 yr 3242 2921 3684 2046 771 (23.8) 639 (21.9) 695 (18.9) 256 (12.5) <0.001* 180 (23.3) 104 (16.3) 72 (10.4) 14 (5.5) <0.001* Cigarette smoking† No Yes 5167 6713 1088 (21.1) 1271 (18.9) 0.004 168 (15.4) 201 (15.8) 0.80 Alcohol consumption‡ No Yes 9434 2432 1902 (20.2) 453 (18.6) 0.09 289 (15.2) 78 (17.2) 0.29
H E PAT I T I S B e A N T I G E N A N D H E PATO C E L LU L A R C A R C I N O M A
development of antibodies against HBeAg.18 In our
follow-up study, with all blood samples collected and assayed before the diagnosis of hepatocellular carcino-ma, the prevalence of HBeAg was 39 percent among men who were positive for HBsAg at the time of en-rollment and who subsequently received a diagnosis of hepatocellular carcinoma — a much higher preva-lence than that reported in a previous case-series study
(18 percent)9 and in previous case–control studies (22
and 25 percent).12,14 Similarly, in our study, the relative
risks of hepatocellular carcinoma among men who were positive for HBsAg alone (9.6) and among those who were positive for both HBsAg and HBeAg (60.2), as compared with men who were negative for both, were much higher than in previous case–control studies.10-14
*HBV denotes hepatitis B virus, CI confidence interval, HBsAg hepatitis B surface antigen, and HBeAg hepatitis B e antigen.
TABLE 2. INCIDENCEOF HEPATOCELLULAR CARCINOMADURING FOLLOW-UP.*
RESULTSOF HBV ANTIGEN TESTS PERSON-YROF FOLLOW-UP NO. OF MEN NO. OF CASESOF HEPATOCELLULAR CARCINOMA INCIDENCE RATE (95% CI) cases/100,000 person-yr
Negative for HBsAg and HBeAg
74,205 9532 29 39.1 (26.2–56.1)
Positive for HBsAg, negative for HBeAg
15,418 1991 50 324.3 (240.7–427.5) Positive for HBsAg
and HBeAg
2,736 370 32 1169.4 (799.9–1650.9)
Figure 1. Cumulative Incidence of Hepatocellular Carcinoma during Follow-up among 11,893 Men in Taiwan, According to the Pres-ence or AbsPres-ence of Hepatitis B Surface Antigen (HBsAg) and Hepatitis B e Antigen (HBeAg) at Enrollment.
The cumulative incidence was estimated with the use of the Nelson–Aalen method. 12 10 8 6 4 2 0 10 0 1 2 3 4 5 6 7 8 9 Year Culmulative Incidence (%) HBsAg+, HBeAg+ HBsAg+, HBeAg¡ HBsAg¡, HBeAg¡
The Ne w E n g l a nd Jo u r n a l o f Me d i c i ne
Both indirect and direct carcinogenic mechanisms are involved in the pathogenesis of hepatocellular car-cinoma induced by chronic HBV infection.19 HBV
may induce hepatocellular carcinoma indirectly by causing chronic necroinflammatory hepatic disease.20
When HBV replication is sustained, as indicated by positivity for HBeAg, malignant transformation may occur as a result of continuous or recurrent cycles of hepatocyte necrosis and regeneration. The accelerat-ed rate of cell turnover may act as a tumor promoter through the accumulation of spontaneous mutations or DNA damage caused by exogenous factors, result-ing in an increased selective growth advantage for transformed cells. The accelerated turnover rate may also result in cleavage of viral DNA at specific motifs, resulting in linear DNA that is inserted into chromo-somal DNA through increased intracellular topoi-somerase I activity.21 Chronic necroinflammation may
induce malignant transformation by generating mu-tagenic reactive oxygen species during the inflamma-tory process.22
Active replication of HBV may also initiate malig-nant transformation through a direct carcinogenic mechanism by increasing the probability of insertion of viral DNA in or near proto-oncogenes, tumor-sup-pressor genes, or their regulatory elements of cellular DNA.23,24 The integration of viral DNA may increase
the production of transactivator protein hepatitis B X antigen, which may induce the malignant
transfor-*Data were not available on cigarette smoking for 13 men, on alcohol consumption for 27, and on antibodies against hepatitis C virus for 77. CI denotes confidence interval, HBV hepatitis B virus, HBsAg hepatitis B sur-face antigen, and HBeAg hepatitis B e antigen.
†This was the reference group. ‡P<0.001.
§P=0.06.
TABLE 3. ADJUSTED RELATIVE RISKOF HEPATOCELLULAR CARCINOMA ACCORDINGTO VARIOUS RISK FACTORS.*
VARIABLE NO. OF CASESOF HEPATOCELLULAR CARCINOMA ADJUSTED RELATIVE RISK (95% CI) Age at enrollment 30–39 yr† 40–49 yr 50–59 yr »60 yr 6 23 55 27 1.0 5.4 (2.2–13.2)‡ 13.5 (5.8–31.7)‡ 17.7 (7.1–43.9)‡ Results of HBV antigen tests
Negative for HBsAg and HBeAg† Positive for HBsAg,
negative for HBeAg Positive for HBsAg
and HBeAg 29 50 32 1.0 9.6 (6.0–15.2)‡ 60.2 (35.5–102.1)‡ Antibodies against hepatitis C virus
No† Yes 98 13 1.0 2.7 (1.5–4.9)‡ Cigarette smoking No† Yes 41 70 1.0 1.5 (1.0–2.2)§ Alcohol consumption No† Yes 80 31 1.0 1.5 (1.0–2.3)§
*The reference group was the group of men who were negative for both hepatitis B surface antigen (HBsAg) and hepatitis B e antigen (HBeAg). CI denotes confidence interval. P<0.001 for all com-parisons.
†The analysis was adjusted for the presence or absence of antibodies against hepatitis C virus, cig-arette-smoking status, and use or nonuse of alcohol.
‡The analysis was adjusted for age (as a continuous variable), the presence or absence of antibodies against hepatitis C virus, and use or nonuse of alcohol.
§The analysis was adjusted for age (as a continuous variable), the presence or absence of antibodies against hepatitis C virus, and cigarette-smoking status.
TABLE 4. ADJUSTED RELATIVE RISKOF HEPATOCELLULAR CARCINOMA, WITH STRATIFICATION ACCORDINGTO AGE, CIGARETTE-SMOKING STATUS,
AND USEOR NONUSEOF ALCOHOL.
VARIABLE ADJUSTED RELATIVE RISK (95% CI)*
NEGATIVEFOR
HBsAg AND HBeAg
POSITIVEFOR HBsAg,
NEGATIVEFOR HBeAg
POSITIVEFOR
HBsAg AND HBeAg
Age at enrollment† «55 yr >55 yr 1.0 1.0 6.1 (3.3–11.4) 14.8 (7.5–29.5) 25.4 (13.3–48.6) 95.5 (42.5–214.5) Cigarette smoking‡ No Yes 1.0 1.0 14.3 (6.1–33.8) 8.9 (5.1–15.5) 67.0 (26.1–171.7) 76.9 (39.4–150.3) Alcohol consumption§ No Yes 1.0 1.0 9.7 (5.6–16.9) 11.4 (5.0–26.3) 69.0 (37.1–128.2) 52.1 (18.0–150.8)
H E PAT I T I S B e A N T I G E N A N D H E PATO C E L LU L A R C A R C I N O M A
mation of hepatocytes, as well as bind to the p53 tu-mor-suppressor gene and disrupt its functions.25-30
The presence of antibodies against HBeAg has been used as an important marker for the resolution of ac-tive HBV infection and for a sustained response to treatment with lamivudine alone or in combination with interferon alfa.7 In the natural history of
chron-ic hepatitis B, the spontaneous or interferon alfa– induced development of antibodies against HBeAg leads to improvement in the clinical outcome.6,31
One study showed that patients who had a response to treatment with interferon alfa (i.e., clearance of HBeAg) were much less likely to have major liver com-plications during a five-year period of follow-up than were treated or untreated patients with persistent HBeAg.31 A long-term controlled trial of treatment
with interferon alfa showed that hepatocellular car-cinoma developed more frequently in untreated pa-tients than in treated papa-tients and that it developed only in those with persistent HBeAg.6 Our study
showed that a negative test for HBeAg was associated with a low risk of hepatocellular carcinoma, suggest-ing that the earlier the development of antibodies against HBeAg occurs, the lower the risk of hepato-cellular carcinoma.
We performed tests for HBsAg and HBeAg only at the time of enrollment. The effect of the appearance of antibodies against HBsAg and HBeAg on the de-velopment of hepatocellular carcinoma was not as-sessed. If the appearance of antibodies against HBeAg occurred after enrollment, the risk of hepatocellular carcinoma among men who were initially positive for HBeAg was underestimated. Tests for antibodies against HBeAg were not performed at the time of enrollment for men who were negative for HBeAg. However, we did perform tests for antibodies against
HBeAg and for HBV DNA in frozen serum samples collected at the time of enrollment from the 44 men in whom hepatocellular carcinoma was subsequently diagnosed and the 86 matched controls, all of whom were initially positive for HBsAg and negative for HBeAg. In this nested case–control analysis, more than 90 percent of the men were positive for anti-bodies against HBeAg, and there was no significant difference in this respect between the men with hep-atocellular carcinoma and the controls. However, pos-itivity for HBV DNA was associated with a signifi-cantly increased risk of hepatocellular carcinoma.
HBV DNA is found in most patients who are pos-itive for HBeAg, in a substantial proportion of those with antibodies against HBeAg (20 to 25 percent), and in some who are negative for HBeAg. Therefore, HBV DNA is the most important predictor of the development of hepatocellular carcinoma in HBsAg-positive Taiwanese men. However, the assay for HBV DNA is expensive and is performed only at special-ized laboratories, whereas the assays for HBeAg, a sur-rogate marker of HBV DNA, and antibodies against HBeAg are inexpensive and are performed routinely. At present, a test for HBeAg may therefore be a more practical method for predicting the risk of hepatocel-lular carcinoma.
In conclusion, HBeAg, in addition to HBsAg, may be a useful marker of the risk of hepatocellular car-cinoma. Persons considered to be at high risk because of positivity for HBeAg would be candidates for an-tiviral-drug treatment and close monitoring for the development of liver diseases associated with chronic HBV infection.
Supported by grants from the Department of Health, Executive Yuan, Taipei, Taiwan.
*The analysis was adjusted for age (as a continuous variable), the presence or absence of antibodies against hepatitis C virus, cigarette-smoking status, and use or nonuse of alcohol. P for trend=0.003.
†This was the reference group. ‡P=0.005.
TABLE 5. LEVELOF HEPATITIS B VIRUS (HBV) DNA IN MENWITH HEPATOCELLULAR CARCINOMAAND MATCHED CONTROLS WHO WERE POSITIVEFOR HEPATITIS B SURFACE ANTIGENAND NEGATIVEFOR HEPATITIS B e ANTIGENAT ENROLLMENT.
HBV DNA MENWITH HEPATOCELLULAR CARCINOMA (N=44) MATCHED CONTROLS (N=86) ADJUSTED ODDS RATIO (95% CI)* no. of men Undetectable (<2.5 pg/ml)† 27 74 1.0 2.5–13.0 pg/ml 7 7 2.3 (0.7–7.3) >13.0 pg/ml 10 5 6.0 (1.7–21.4)‡
The Ne w E n g l a nd Jo u r n a l o f Me d i c i ne
APPENDIX
The following institutions and investigators, in addition to the authors, participated in the Taiwan Community-Based Cancer Screening Project Group: National Taiwan University Hospital — G.-T. Huang, H.-S. Lee, P.-M. Yang, C.-H. Chen; Huhsi Health Center, Penghu County — S.-C. Ho, T.-G. Lu; Provincial Penghu Hospital — W.-P. Wu, C.-T. Chen; Sanchi
Health Center, Taipei County — C.-G. Lin; Provincial Chutung Hospital —
C.-H. Lo; Provincial Potzu Hospital — Y.-Y. Kuo; Kaohsu Health Center,
Pingtung County — C.-T. Lee, C.-C. Chen; and Paihsa Health Center, Pen-ghu County — Y.-C. Ou, W.-C. How.
REFERENCES
1. Chu CM, Liaw YF. Natural history of chronic hepatitis B virus infection: an immunopathological study. J Gastroenterol Hepatol 1997;12:S218-S222.
2. Chen DS. From hepatitis to hepatoma: lessons from type B viral hepa-titis. Science 1993;262:369-70.
3. IARC monographs on the evaluation of carcinogenic risks to humans. Vol. 59. Hepatitis viruses. Lyons, France: International Agency for Re-search on Cancer, 1994.
4. Chen CJ, Yu MW, Liaw YF. Epidemiological characteristics and risk fac-tors of hepatocellular carcinoma. J Gastroenterol Hepatol 1997;12:S294-S308.
5. Beasley RP, Hwang LY, Lin CC, Chien CS. Hepatocellular carcinoma and hepatitis B virus: a prospective study of 22 707 men in Taiwan. Lancet 1981;2:1129-33.
6. Lin SM, Sheen IS, Chien RN, Chu CM, Liaw YF. Long-term beneficial effect of interferon therapy in patients with chronic hepatitis B virus infec-tion. Hepatology 1999;29:971-5.
7. Farrell G. Hepatitis B e antigen seroconversion: effects of lamivudine alone or in combination with interferon alpha. J Med Virol 2000;61:374-9. 8. Chu CM, Liaw YF, Sheen IS, Lin DY, Huang MJ. Sex difference in chronic hepatitis B virus infection: an appraisal based on the status of hep-atitis B e antigen and antibody. Hepatology 1983;3:947-50.
9. Liaw YF, Chu CM, Lin DY, Sheen IS, Yang CY, Huang MJ. Age-specific prevalence and significance of hepatitis B e antigen and antibody in chronic hepatitis B virus infection in Taiwan: a comparison among asymptomatic carriers, chronic hepatitis, liver cirrhosis, and hepatocellular carcinoma. J Med Virol 1984;13:385-91.
10. Lu SN, Lin TM, Chen CJ, et al. A case-control study of primary hep-atocellular carcinoma in Taiwan. Cancer 1988;62:2051-5.
11. Chen CJ, Liang KY, Chang AS, et al. Effects of hepatitis B virus, al-cohol drinking, cigarette smoking and familial tendency on hepatocellular carcinoma. Hepatology 1991;13:398-406.
12. Lin TM, Chen CJ, Lu SN, et al. Hepatitis B virus e antigen and pri-mary hepatocellular carcinoma. Anticancer Res 1991;11:2063-5. 13. Yu MW, You SL, Chang AS, Lu SN, Liaw YF, Chen CJ. Association between hepatitis C virus antibodies and hepatocellular carcinoma in Tai-wan. Cancer Res 1991;51:5621-5.
14. Tsai JF, Jeng JE, Ho MS, et al. Additive effect modification of hepatitis B surface antigen and e antigen on the development of hepatocellular car-cinoma. Br J Cancer 1996;73:1498-502.
15. Aalen O. Nonparametric inference for a family of counting processes. Ann Stat 1978;6:701-26.
16. Breslow N, Crowley J. A large sample study of the life table and prod-uct limit estimates under random censorship. Ann Stat 1974;2:437-53. 17. Peña EA, Rohatgi VK. Small sample and efficiency results for the Nel-son-Aalen estimator. J Stat Plann Inference 1993;37:193-202.
18. Heyward WL, Bender TR , Lanier AP, Francis DP, McMahon BJ, May-nard JE. Serological markers of hepatitis B virus and alpha-fetoprotein lev-els preceding primary hepatocellular carcinoma in Alaskan Eskimos. Lancet 1982;2:889-91.
19. Kew MC. Hepatitis viruses and hepatocellular carcinoma. Res Virol 1998;149:257-62.
20. Chisari FV, Klopchin K, Moriyama T, et al. Molecular pathogenesis of hepatocellular carcinoma in hepatitis B virus transgenic mice. Cell 1989; 59:1145-56.
21. Wang JC. DNA topoisomerases. Annu Rev Biochem 1985;54:665-97. 22. Freeman BA, Crapo JD. Biology of disease: free radicals and tissue in-jury. Lab Invest 1982;47:412-26.
23. Shafritz DA, Kew MC. Identification of integrated hepatitis B virus DNA sequences in human hepatocellular carcinoma. Hepatology 1981;1: 1-8.
24. Matsubara K, Tokino T. Integration of hepatitis B virus DNA and its implications for hepatocarcinogenesis. Mol Biol Med 1990;7:243-60. 25. Popper H, Roth L, Purcell RH, Tennant BC, Gerin JL. Hepatocarci-nogenicity of the woodchuck hepatitis virus. Proc Natl Acad Sci U S A 1987;84:866-70.
26. Kim CM, Koike K , Saito I, Miyamura T, Jay G. HBx gene of hepa-titis B virus induces liver cancer in transgenic mice. Nature 1991;351:317-20.
27. Paterlini P, Poussin K, Kew MC, Franco D, Brechot C. Selective accu-mulation of the X transcript of hepatitis B virus in patients negative for hepatitis B surface antigen with hepatocellular carcinoma. Hepatology 1995;21:313-21.
28. Henkler FF, Koshy R. Hepatitis B virus transcriptional activators: mechanisms and possible role in oncogenesis. J Viral Hepat 1996;3:109-21.
29. Feitelson MA, Zhu M, Duan LX, London WT. Hepatitis B x antigen and p53 are associated in vitro and in liver tissues from patients with pri-mary hepatocellular carcinoma. Oncogene 1993;8:1109-17.
30. Wang XW, Gibson MK, Vermeulen W, et al. Abrogation of p53-induced apoptosis by the hepatitis B virus X gene. Cancer Res 1995;55: 6012-6.
31. Niederau C, Heintges T, Lange S, et al. Long-term follow-up of HBeAg-positive patients treated with interferon alfa for chronic hepatitis B. N Engl J Med 1996;334:1422-7.