應用三度空間立體影像電子射束電腦斷層掃描攝影
評估先天性心臟病患童之氣管支氣管異常
Usefulness of Thr ee-dimensional Electr on Beam Computed Tomogr aphy in Evaluating Tr acheobr onchial anomaly in Childr en with Congenital Hear t disease
計畫編號:NSC 89-2320-B-002-012-M083 執行期限:88 年 08 月 01 日至 89 年 07 月 31 日 主持人:陳世杰 台灣大學 醫學系 放射科 共同主持人:李瑤華 台灣大學 醫學系 放射科 共同主持人:王主科 台灣大學 醫學系 小兒科 一、中文摘要 以三度空間立體影像顯示原發性氣管支 氣管之異常,來幫助診斷之建立並藉以作 為手術治療之範圖。從 1995 年六月到 2000 年九月,本院有 1245 名先天性心臟病的患 者接受電子射束電腦斷層掃描攝影( EBCT ) 的檢查。其中,有 160 名病童(女:男 = 67 : 93;年齡從 1 天到 18 歲又 6 個月)合併有 原發性的氣管支氣管的異常。所有的掃描 都與心電圖的訊號同步。以一部獨立的工 作站來執行三度空間立體影像的重建。再 藉由不同角度投影的不同影像組成一個動 態循環,以便由各個不同角度更加觀察這 些異常。這些患有不正常氣道的病人年齡 都很小,大部分( 42.5% ) 的人都小於 1 歲。 男生( 58.1% )發生的機率比女生高。吾等 總共可以發現九種主要的氣管支氣管異 常。包括兩側三分叉的支氣管( 57% )、右 上肺葉的氣管性支氣管( 18% )、支氣管體 位 反 轉 ( 10% )、 兩 側 分 叉 的 支 氣 管 ( 6% )、 兩 側 上 肺 葉 的 氣 管 性 支 氣 管 ( 2% )、氣管憩室( 2% )、左側支氣管不 發育( 1% ) 以及右側支氣管不發育( 1% ) 。 有些病人是上述異常的組合。藉由三度空 間立體影像之重組,EBCT 提供中央氣管支 氣管異常的一個絕佳的解剖上的展示。因 而能取代傳統較侵襲性的支氣管鏡或支氣 管攝影。 關鍵詞:氣管支氣管異常;先天性心臟 病;小孩;三度空間立體影像;電子射束 電腦斷層掃描攝影。 ABSTRACT
To delineate the primary tracheobronchial anomalies three- dimensionally for
facilitating diagnosis and preparing a road map for surgical planning. From June 1995 to September 2000, we had 1245 patients underwent electron beam computed tomography scanner (EBCT) studies. Among these children, 160 patients (F:M = 67:93; aged 1 day to 18-year-6-month old) associated with the primary tracheobronchial anomalies. All scanning were examined with electrocardiogram-gating. An independent workstation performed the three-dimensional reconstruction. Multiple images were created and dynamic cine observation with changing viewpoints was used to perceive these abnormal structures three-dimensionally. The detected abnormal airways were always at very young age. Most (42.5%) of the patients were found before 1 year old. Male (58.1%) predominate was noted. There were 9 essential patterns of the tracheobronchial anomalies. It included bilateral trifurcated bronchi (57%), tracheal bronchus of the right upper lobe (18%), bronchial situs inversus (10%), bilateral bifurcated bronchi (6%), tracheal bronchi of bilateral upper lobe (2%), tracheal diverticulum (2%), left bronchial agenesis (1%) and right bronchial agenesis (1%). Some combinations of the above anomalies were also found. With the 3D reconstruction, EBCT provided an excellent anatomic definition of the central tracheobronchial abnormalities. It also offered an opportunity to replace traditional invasive bronchography or bronchoscopy.
Keywor ds: tracheobronchial anomaly;
congenital heart disease; children; three-dimensional reconstruction; electron beam computed tomography.
二、BACKGROUND & PURPOSE
Children have congenital tracheobronchial anomaly usually are asymptomatic. However, if stridor, cyanosis, wheezing or recurrent pneumonia occurs, serious consideration of their airway must be taken. Structural features make their airway more vulnerable to stenosis or occlusion by a small amount of edema or mucus [1]. But, many cases still had no symptoms until mechanical insults (e.g., endotracheal intubation) cause mucosal edema that aggravates airway occlusion. Keeping alert to this situation is important to prevent disaster in the perioperative period. Particularly, in cases with congenital heart disease whose arterial O2 saturation is frequently compromised [2].
Conventional axial computed tomography (CT) is now considered the best imaging modality for evaluation of the trachea and major bronchi, and has almost completely replaced the former gold standard of tracheobronchography [3-7]. Yet, there has been no systematic analysis of the primary tracheobronchial anomalies in children with congenital heart disease.
三、RESULTS
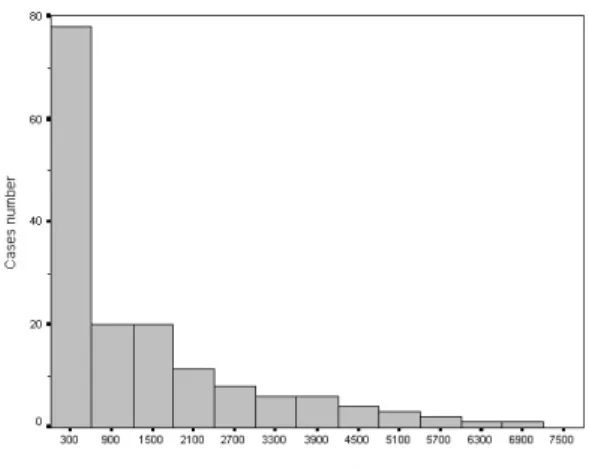
The detected abnormal airways were always at very young age. Most (42.5%) of the patients were found before 1 year old. The number of patients abruptly declined after neonate and gradually decreased with increased ages (Figure 1). Male (58.1%) predominate was also noted.
In the involved cardiac diseases, most of our patients had right atrial isomerism (61%). Tetralogy of Fallot (9%), left atrial isomerism (6%) and double outlet of the right ventricle (6%) were the next common associated problems. The incidence of accompanied primary airway anomalies was low (<5%) in other congenital heart diseases (Table 1).
There were 9 essential patterns of the tracheobronchial anomalies. The most popular one was the bilateral trifurcated bronchi (57%; Figure 2) that consistent with the majority of the related heart disease. The tracheal bronchus of the right upper lobe was the next common one (18%; Figure 3). Another usual presentations were bronchial
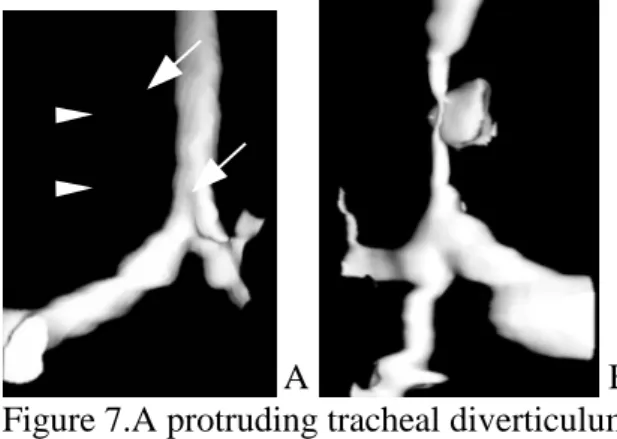
situs inversus (10%; Figure 4) in situs inversus and bilateral bifurcated bronchi (6%; Figure 5) in left atrial isomerism. The other uncommon anomalies included the tracheal bronchi of bilateral upper lobe (2%; Figure 6), tracheal diverticulum (2%; Figure 7), left bronchial agenesis (1%; Figure 8), right bronchial agenesis (1%; Figure 9) and in combination of the above anomalies (Table 2).
四、DISCUSSION
Children with tracheobronchial anomaly easily get repeated infection. Those combined with congenital heart disease sometimes would be critical in acute post-operative period [1]. Theoretically, the surgical correction of cardiac problems is successful but patients experience respiratory failure, desaturation and die. One of the major causes is the complications from unrecognized insidiously tracheobronchial anomalies that became injury during the perioperative manipulation.
Bronchography is a conventionally diagnostic modality that visualizes the airway. However, precipitating further respiratory decompensation is a big problem in cases with heart disease and can be life-threatening. Bronchoscopy can directly visualize the pathology in the abnormal tracheobronchial tree, but it is invasive. Moreover, both of the above procedures are not suitable for screening. EBCT has the advantage of electrocardiogram gated scanning that eliminated the motional artifact of the airway by adjacent beating heart. With the 3D reconstruction, it provided an excellent anatomic definition of the central tracheobronchial abnormalities. Such images seem to be particularly useful in evaluating the full view of airway for diagnosis, thus providing valuable information for preparing a road map for surgical planning. It also offered an opportunity to replace traditional bronchography or bronchoscopy with a safer, less invasive modality.
五、REFERENCES
1. Davis DA, Tucker JA, Russo P. Management of airway obstruction in
patients with congenital heart defects. Ann Oto Rhinol Laryn 1993; 102:163-166.
2. Kazim R, Quaegebeur JM, Sun LS. The association of tracheal anomalies and tetralogy of Fallot. J Cardiothorac Vascular Anesth 1996; 10(5): 589-592. 3. Remy J, Remy-Jardin M, Artaud D, et al.
Multiplanar and three-dimensional reconstruction techniquesin CT: impact on chest diseases. Europ Radiology1998; 8(3): 335-51.
4. Johnson PT, Fishman EK, Duckwall JR, et al. Interactive three - dimensional volume rendering of spiral CT data: current applications in the thorax. Radiographics 1998; 18(1): 165-87. 5. Nicotra JJ, Mahboubi S, Kramer SS.
Three-dimensional imaging of the pediatricairway.International J Pedi Otorhinolaryn 1997; 41(3): 299-305. 6. Lee KS, Yoon JH, Kim TK, et al.
Evaluation of tracheobronchial disease with helical CT with multiplanar and three-dimensional reconstruction: correlation with bronchoscopy. Radiographics 1997; 17(3): 555-67. 7. Sagy M, Poustchi-Amin M, Nimkoff L,
et al. Spiral computed tomographic scanning of the chest with three dimensional imaging in the diagnosis and management of paediatric intrathoracic airway obstruction. Thorax 1996; 51(10): 1005-9.
六、SELF-EVALUATION
The result of this one-year project revealed very consistent with the original proposal. Investigators have established a good protocol for 3D reconstruction of the pediatric airway. The expected goal has successfully achieved by demonstrating the different 3D patterns of the primary tracheobronchial abnormalities and picked up the incidence of these anomalies in the patients with congenital heart disease. The clinical application of this result is great. Because this information will provide surgeon a clear road map of diseased airway before operation that also prevent unexpected findings or manipulations.
七、TABLES & FIGURES
Table 1. Disease patterns of patients.
Major diagnosis Case number Right atrial isomerism 97
Tetralogy of Fallot 15
Left atrial isomerism 9 Double outlet of right ventricle 9 Ventricular septal defect 7 Congenital corrected transposition 4
Atrial septal defect 3
Tricuspid atresia 3
Left pulmonary artery sling 3 Transposition of great artery (L-loop) 2
Others* 8
Total 160 * = Left lung agenesis (n=1); Right lung agenesis (n=1); Scimitar syndrome (n=1); Truncus arteriosus (n=1); Double inlet of indeterminated ventricle with pulmonary atresia (n=1); Patent ductus arteriosus (n=1); Innominate artery syndrome(n=1) ; Total anomalous pulmonary venous return (n=1).
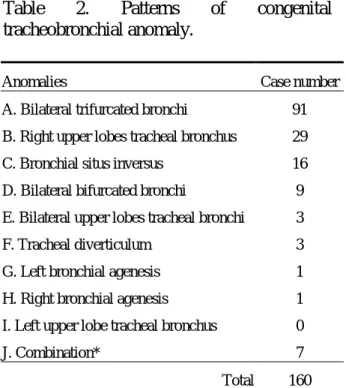
Table 2. Patterns of congenital tracheobronchial anomaly.
Anomalies Case number
A. Bilateral trifurcated bronchi 91 B. Right upper lobes tracheal bronchus 29 C. Bronchial situs inversus 16 D. Bilateral bifurcated bronchi 9 E. Bilateral upper lobes tracheal bronchi 3 F. Tracheal diverticulum 3 G. Left bronchial agenesis 1 H. Right bronchial agenesis 1 I. Left upper lobe tracheal bronchus 0
J. Combination* 7
Total 160
Figure 1. Age distribution of the patients.
Figure 2. Bilateral symmetrical steep short main stem bronchi compatible with bilateral trifurcated bronchi.
A B
Figure 3. Right upper lobe tracheal bronchus (arrows) without (A) and with (B) lower tracheal stenosis (arrowheads).
Figure 4. Bronchial situs inversus representing as left steep and right more horizontal main stem bronchi.
Figure 5. Bilateral symmetrical horizontal long main stem bronchi compatible with bilateral trifurcated bronchi.
Figure 6. Bilateral upper lobes tracheal bronchi (arrows) are noted in normal pattern of the bilateral main stem bronchi.
A B Figure 7.A protruding tracheal diverticulum (arrow) is noted without (A) or with (B) tracheal stenosis (arrowhead).
Figure 8. Left bronchial agenesis with totally absence of the left bronchus and its branches.
2000/10/23
Figure 9. Right bronchial agenesis with totally absence of the right bronchus and its branches.
Figure 10. Normal tracheobronchial tree for comparison.