A Population-Based Nested Case-Control Study in Taiwan: Use of
5
␣-Reductase Inhibitors Did Not Decrease Prostate Cancer Risk in
Patients with Benign Prostate Hyperplasia
J
I-A
NL
IANG,
a,dL
I-M
INS
UN,
gM
ING-C
HIAL
IN,
hS
HIH-N
IC
HANG,
b,c,e,iF
UNG-C
HANGS
UNG,
c,eC
HIH-H
SINM
UO,
c,eC
HIA-H
UNGK
AOa,fa
Institute of Clinical Medicine Science and School of Medicine, College of Medicine,
bProgram for Cancer
Biology and Drug Discovery, and
cInstitute of Environmental Health, College of Public Health, China
Medical University, Taichung, Taiwan;
dDepartment of Radiation Oncology,
eManagement Office for Health
Data, and
fDepartment of Nuclear Medicine and PET Center, China Medical University Hospital, Taichung,
Taiwan;
gDepartment of Radiation Oncology, Zuoying Armed Forces General Hospital, Kaohsiung, Taiwan;
hDepartment of Nuclear Medicine, E-DA Hospital, Kaohsiung, Taiwan; China Medical University, Taichung,
Taiwan;
iInstitute of Biomedical Sciences, Academia Sinica, Taipei, Taiwan
Key Words. 5␣-Reductase inhibitors • Benign prostate hyperplasia • Prostate cancer
Disclosures: The authors indicated no financial relationships.
The content of this article has been reviewed by independent peer reviewers to ensure that it is balanced, objective, and free from commercial bias. No financial relationships relevant to the content of this article have been disclosed by the authors or independent peer reviewers.
Section Editors: Scott Ramsey: None; Bong-Min Yang: None Reviewer “A”: None
Reviewer “B”: None
L
EARNINGO
BJECTIVESAfter completing this course, the reader will be able to:
1. Describe the effect of finasteride use on the incidence of prostate cancer and overall cancer. 2. Describe the effect of dutasteride use on the incidence of renal cancer.
3. Explain the relationship between finasteride dosage and risk of prostate cancer and overall cancer risk. This article is available for continuing medical education credit at CME.TheOncologist.com.
CME
CME
ABSTRACT
Background. 5␣-Reductase inhibitors (5ARIs) are com-monly used to treat benign prostate hyperplasia (BPH) by blocking the conversion of testosterone into the more po-tent dihydrotestosterone. This study explored a possible as-sociation between the use of the 5ARIs finasteride and
dutasteride and the subsequent risk of prostate cancer or other cancers.
Methods. We analyzed data from the Taiwanese National Health Insurance system. In a BPH cohort, we identified 1,489 patients with cancer and included them in our study
Correspondence: Chia-Hung Kao, M.D., Institute of Clinical Medicine Science and School of Medicine, College of Medicine, China
Medical University, No. 2, Yuh-Der Road, Taichung 404, Taiwan. Telephone:⫹886 4 22052121 x7412; Fax: ⫹886 4 22336174. e-mail:
[email protected] Received December 26, 2011; accepted for publication March 8, 2012; first published online in The
Oncol-ogist Express on June 20, 2012. ©AlphaMed Press 1083-7159/2012/$20.00/0 http://dx.doi.org/10.1634/theoncolOncol-ogist.2011-0464
T
he
O
ncologist
®O
utcomes
R
esearch
by Chia-Hung Kao on August 13, 2012
www.TheOncologist.alphamedpress.org
group. For the control group, 3 patients without cancer were frequency matched with each BPH case for age, BPH diagno-sis year, index year, and month. Information regarding past 5ARI use was obtained from the Taiwanese National Health Insurance Research Database (NHIRD). Multivariate logistic regression analysis was conducted, and odds ratio (OR) and 95% confidence interval (CI) were estimated.
Results. Finasteride use marginally increased the inci-dence of prostate and overall cancer at a level of statistical significance (prostate cancer: ORⴝ 1.90; 95% CI: 1.00– 3.59; overall cancer: ORⴝ 1.51; 95% CI: 1.00–2.28). Du-tasteride use significantly increased kidney cancer risk
(ORⴝ 9.68, 95% CI: 1.17–80.0). Dosage analysis showed that lower doses of finasteride were associated with higher overall and prostate cancer risks. The major limitation is the lack of important data in the NHIRD, such as prostate cancer histologic grades, smoking habits, alcohol con-sumption, body mass index, socioeconomic status, and family history of cancer.
Conclusions. This population-based nested case-control study suggested that finasteride use may increase prostate and overall cancer risks for patients with BPH. The effects were more prominent for patients using lower doses of fi-nasteride. The Oncologist 2012;17:986 –991
INTRODUCTION
Benign prostate hyperplasia (BPH) is the most common pros-tate disease in aging men, and patients may suffer considerably from related urinary symptoms. Androgens play an essential role in prostatic growth and development [1], but they also contribute to prostate disease pathogenesis [2]. One of the ma-jor roles of 5␣-reductase is to convert testosterone into the more potent dihydrotestosterone and then enhance the andro-genic signal in tissues. Finasteride and dutasteride are two well-known 5␣-reductase inhibitors (5ARIs) that are com-monly used to treat BPH by blocking this conversion. Both agents result in similar prostate gland volume reduction and symptom improvement. Both agents also achieve reductions in the long-term risk of BPH development for symptom progres-sion, acute urinary retention, and BPH-related surgery [3].
A currently debated issue is the use of 5ARIs to prevent prostate cancer [4]. Two landmark large randomized clinical trials, namely the Prostate Cancer Prevention Trial (PCPT) with finasteride and the Reduction by Dutasteride of Prostate Cancer Events (REDUCE) trial, aroused great interest in the public health field [5, 6]. These studies revealed a 23%–25% reduction in prostate cancer incidence when participants used 5ARIs; however, the medication was also found to be associ-ated with an absolute increase in high-grade prostate cancer. Because of this concern, the U.S. Food and Drug Administra-tion has not approved 5ARIs as a chemopreventive agent for prostate cancer.
Globally, a large number of men with BPH are treated with 5ARIs. Thus, even a small magnitude of benefit or hazard has important clinical implications. A large population-based study may help to clarify the controversy. The results from a post hoc analysis of the data in the REDUCE study confirmed the value of dutasteride treatment for reducing the risk of pros-tate cancer in Japanese men [7]. We were interested in explor-ing this issue further, so we conducted the current study usexplor-ing data from the National Health Insurance (NHI) system of Tai-wan. We analyzed the risk for prostate cancer, as well as other individual cancers and overall cancer risk.
METHODS
This study used data retrieved from Taiwan’s National Health Research Institute, which is responsible for managing the NHI Research Database (NHIRD). The NHIRD contains all reim-bursement claim records from 1996 to 2009 for 1 million
ran-domly selected representative insurance holders. Details of this population-based database have been published previ-ously [8].
In this nested case-control study, we first identified pa-tients who had been newly diagnosed with BPH (ICD-9-CM: 600.xx) and followed up between 1996 and 2009; these pa-tients were included in our exposure cohort. We then excluded from this group patients who had been newly diagnosed with cancer (ICD-9-CM 140 –208) before January 1, 2007. We se-lected patients who were newly diagnosed with cancer be-tween 2007 and 2009 as our study sample and used the date of cancer diagnosis as the patient’s index date. To create the com-parison group, each cancer case was matched with three ran-domly selected NHIRD patients without cancer, with frequency matching for age, BPH year, index year, and month. Medication use was defined as a patient having received a drug prescription during the 2 years before his index date. Medication was classified into four groups: none (control), du-tasteride, finasteride, and both.
STATISTICAL ANALYSIS
We used the-square test to compare the distributions of de-mographic characteristics and medication use between the cancer and noncancer groups. We used a multivariate logistic regression model to calculate the odds ratio (OR), namely the ratio of cancer risk for medication users to that for nonusers. Multivariate logistic regression was also used to estimate the 95% confidence interval (CI) and specific cancer risks. We fur-thermore estimated the cancer risk for different dosages of du-tasteride and finasteride.
All analyses were performed using the SAS statistical package, version 9.1 (SAS Institute, Cary, NC). The signifi-cance level was set at p⬍ .05.
RESULTS
The distributions for demographic variables and medication use for the cancer and noncancer groups are shown in Table 1. Among the 1,489 patients with cancer, most were between 65 and 84 years of age (71.0%). The mean age was 72.5⫾ 9.3 years for the cancer group and 72.6⫾ 9.5 years for the non-cancer group. No statistically significant difference emerged for medication use between patients with cancer (2.2% for du-tasteride, 2.6% for finasteride) versus the noncancer control group (1.6% for dutasteride, 1.8% for finasteride).
www.TheOncologist.com
by Chia-Hung Kao on August 13, 2012
www.TheOncologist.alphamedpress.org
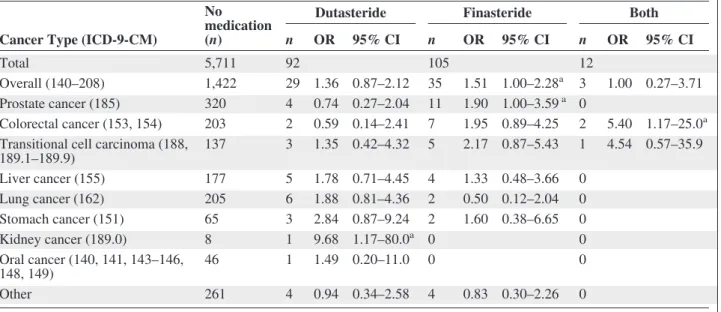
Overall, compared with patients who did not use 5ARIs, patients with BPH who were using finasteride displayed a mar-ginal but significant increase in overall cancer risk (OR⫽ 1.51, 95% CI: 1.00 –2.28; Table 2). The cancer-specific anal-yses showed that finasteride users had a 1.90-fold increased risk (95% CI: 1.00 –3.59) for prostate cancer. For patients who used both medications, the OR was 5.40 (95% CI: 1.17–25.0) for colorectal cancer, indicating that the combined use of the two medications was associated with a substantially increased risk. Dutasteride use was associated with a significant increase in risk for kidney cancer (OR⫽ 9.68, 95% CI: 1.17–80.0; Ta-ble 2).
Furthermore, dosage analysis showed that lower rather than higher doses of finasteride were associated with higher overall cancer risk (OR⫽ 1.96, 95% CI: 1.19–3.22) and pros-tate cancer risk (OR⫽ 2.20, 95% CI: 1.04–4.65) relative to nonmedication users (Table 3).
DISCUSSION
The results of the adjusted analysis from this population-based
overall cancer. Dutasteride use was not related to prostate can-cer risk, but it was associated with a significant increase in kid-ney cancer risk. Dosage analysis showed that lower doses of finasteride were associated with higher prostate and overall cancer risks.
Since 1982, cancer has been the leading cause of death in Taiwan. The age-adjusted incidence rate has increased steadily, and in 2007 it reached 270 new cases per 100,000 population [9]. This trend differs from the U.S. Surveillance Epidemiology and End Results data, which showed that the overall cancer incidence rates in the U.S. decreased by 0.7% per year between 1999 and 2006 [10]. Prostate cancer was the fifth most common cancer in Taiwan in 2008, with the inci-dence rate increasing dramatically by 15.9% between 2002 and 2006 [9]. As in other Asian countries, in Taiwan the adoption of globalized lifestyles and factors related to diet and the envi-ronment have contributed to an increase in cancer rates [11].
Taiwan’s NHI program provides comprehensive health coverage to all citizens. The NHIRD contains ambulatory ser-vice records, hospital serser-vice records, and prescription claims
Table 1. Demographics and medication use of noncancer and cancer groups
Noncancer group Cancer group
p n % n % Total 4,331 1,489 Age, year 1.00 50–64 942 21.3 318 21.4 65–74 1,532 34.6 514 34.5 75–84 1,619 36.5 543 36.5 ⱖ 85 338 7.6 114 7.7 Mean (SD) 72.6 9.5 72.5 9.3 0.89 Occupation 0.002 Publica 444 10.0 177 11.9 Labor 1,770 40.0 645 43.3 Business 1,109 25.0 363 24.4 Low incomeb 32 0.7 6 0.4 Other 1,076 24.3 298 20.0 Urbanizationc 0.44 1 1,179 26.6 417 28.0 2 1,198 27.0 392 26.3 3 733 16.5 254 17.1 4 723 16.3 250 16.8 5 598 13.5 176 11.8 Medication 0.33 Dutasteride 72 1.6 32 2.2 0.18 Finasteride 79 1.8 38 2.6 0.07 a
Government, education, and military.
b
Insured income is lower than the level required for charging premium.
cUrbanization level: 1 indicates the highest level of urbanization and 5 the lowest.
by Chia-Hung Kao on August 13, 2012
www.TheOncologist.alphamedpress.org
underlying populations. We recently used the database to con-duct a cohort study to evaluate the risk of malignancy for pa-tients with end-stage renal disease. That article has been published and presents some interesting findings [12]. The cur-rent study used the same data source but with a diffecur-rent re-search design (nested case-control study) to investigate whether the use of 5ARIs was associated with an increased risk of prostate or other cancers.
Substantial evidence from previous research suggests that androgens influence the development of prostate cancer [13–16]. Studies of BPH treatment incidentally found pre-liminary but inconclusive evidence that the use of 5ARIs may reduce the risk of prostate cancer [17, 18]. The PCPT was the first large-scale primary chemoprevention trial
con-ducted with men at risk for prostate cancer. Its findings sug-gested that finasteride effectively prevented or delayed the occurrence of prostate cancer; however, finasteride use was also found to be associated with a significant increase in the risk of high-grade prostate cancer (Gleason score 7–10) [5]. The REDUCE study later focused on dutasteride and ob-tained similar results. The incidence of prostate cancer was significantly reduced by the use of dutasteride, but users of this drug were at a significantly greater risk for developing high-grade cancer (Gleason score 8 –10) compared with the placebo-controlled group [6]. The REDUCE researchers speculated that this scenario was due to the more frequent early detection of low-grade tumors among the placebo group. A secondary analysis of REDUCE data focused on
Table 2. Adjusted odds ratio (OR) and 95% confidence interval (CI) for cancer type by medication
Cancer Type (ICD-9-CM)
No medication (n)
Dutasteride Finasteride Both
n OR 95% CI n OR 95% CI n OR 95% CI
Total 5,711 92 105 12
Overall (140–208) 1,422 29 1.36 0.87–2.12 35 1.51 1.00–2.28a 3 1.00 0.27–3.71
Prostate cancer (185) 320 4 0.74 0.27–2.04 11 1.90 1.00–3.59a 0
Colorectal cancer (153, 154) 203 2 0.59 0.14–2.41 7 1.95 0.89–4.25 2 5.40 1.17–25.0a
Transitional cell carcinoma (188, 189.1–189.9) 137 3 1.35 0.42–4.32 5 2.17 0.87–5.43 1 4.54 0.57–35.9 Liver cancer (155) 177 5 1.78 0.71–4.45 4 1.33 0.48–3.66 0 Lung cancer (162) 205 6 1.88 0.81–4.36 2 0.50 0.12–2.04 0 Stomach cancer (151) 65 3 2.84 0.87–9.24 2 1.60 0.38–6.65 0 Kidney cancer (189.0) 8 1 9.68 1.17–80.0a 0 0 Oral cancer (140, 141, 143–146, 148, 149) 46 1 1.49 0.20–11.0 0 0 Other 261 4 0.94 0.34–2.58 4 0.83 0.30–2.26 0
Values are adjusted for age and occupation.
ap⬍ .05.
Table 3. Adjusted odds ratio (OR) and 95% confidence interval (CI) of cancer in patients with BPH by medication dosage
Medication dosage
None Low High
n Cases (n) OR 95% CI n Cases (n) OR 95% CI n Cases (n) OR 95% CI
All cancer None 5,711 1,422 1.00 Reference 67 26 1.96 1.19–3.22a 38 9 0.91 0.43–1.92 Low 55 17 1.34 0.75–2.38 6 1 0.59 0.07–5.07 1 0 High 37 12 1.38 0.69–2.77 4 2 3.22 0.45–23.0 1 0 Prostate cancer None 5,711 320 1.00 Reference 67 8 2.20 1.04–4.65b 38 3 1.40 0.42–4.57 Low 55 1 0.32 0.04–2.31 6 0 1 0 High 37 3 1.35 0.41–4.42 4 0 1 0
Values are adjusted for age and occupation. Median daily medication dosages are as follows: low dutasteride,⬍2 mg; high dutasteride,ⱖ2 mg; low finasteride, ⬍0.2 mg; high finasteride, ⱖ 0.2 mg.
ap⬍ .01. bp⬍ .05.
www.TheOncologist.com
by Chia-Hung Kao on August 13, 2012
www.TheOncologist.alphamedpress.org
the outcomes of BPH and found that dutasteride was asso-ciated with a decreased risk of BPH progression [19].
The 5ARIs are known to exert a prolonged adverse effect on sexual function, with erectile dysfunction or diminished libido be-ing reported by a subset of men [20]. Extensive research has at-tempted to evaluate the risks and chemopreventive benefits of 5ARIs, but to date consensus is lacking on which drug is the most promising chemopreventive agent [4, 21, 22]. In addition, physi-cians may not readily accept the use of chemopreventive agents for prostate cancer [23].
The current study did not find a chemopreventive effect for either finasteride or dutasteride regarding prostate cancer. On the contrary, we observed more prostate cancer cases among finasteride users, with a marginal statistical significance. Un-fortunately, the limitations of the data available in the NHIRD meant that we were unable to differentiate between cases of low- versus high-grade cancer. A prior Taiwanese study as-sessed the pathologic features of prostate cancer and found higher percentages of high-grade cancer (Gleason score 7 or higher): 90.6% and 72.9% for the largest tumor and second largest tumor, respectively [24]. The PCPT analyzed data from cases in the U.S., with the majority of patients being white. For the PCPT cancer cases, a Gleason score of 7 or higher was noted in 47.8% and 29.4% of the finasteride and placebo groups, respectively [5]. The discrepancy between our results and those of the PCPT may possibly be explained by a higher percentage of patients in our study who had Gleason scores of 7–10. If this was the case, the statistical results would have un-deremphasized the chemopreventive effect of finasteride on low-grade prostate cancer, while highlighting the possible risk of finasteride use in the development of high-grade prostate cancer. We also found prostate cancer to be the most common cancer among the finasteride users, accounting for 31.4% (11/35) of all cancer cases in this group. In contrast, only 22.5% (320/1,422) of patients with cancer who were not treated with 5ARI (control group) had prostate cancer. The ob-vious difference in the prostate cancer risk between the two groups paralleled the difference in overall cancer risk between the two groups.
The other unexpected finding among our patients with BPH was a significantly higher risk for kidney cancer in the dutasteride users. The kidneys express 5␣-reductase type I [25], and an as-yet undetermined mechanism may account for the relationship between dutasteride use and kidney cancer risk. However, when we visually inspected the original data, we could identify only eight cases of kidney cancer in the no-5ARI group and only one case in the dutasteride group. When the number of cases is so small, even minimal effects influence the statistical results dramatically, leading to potentially spuri-ous conclusions. In addition, we could not find any descrip-tions or discussions in the literature on plausible mechanisms for a cause-and-effect relationship between dutasteride use and kidney cancer. We thus concluded that the statistical difference between our study and control groups for kidney cancer inci-dence was likely to be a spurious finding.
The same problem was evident in our findings for the
in-nasteride and dutasteride appeared to be associated with a significant increase in risk of colorectal cancer. However, these results were statistically unreliable because of the ex-tremely small sample size (n⫽ 12), with a minimal number of colorectal cancer cases (n⫽ 2; Table 2).
Another finding of the current research was that lower doses (⬍0.2 mg per day) rather than higher doses of finasteride were related to the risk of prostate cancer and all other cancers (Table 3). This finding suggests that the possible chemopre-ventive effect of finasteride requires the medication to be ad-ministered in higher doses to counterbalance the risk factor associated with lower doses.
Strengths of the current study included its use of popula-tion-based data and NHIRD records rather than self-reported drug use. However, certain limitations should be mentioned. First, important data were missing from the NHIRD, including the histologic grade of prostate cancer and detailed demo-graphic information such as smoking habits, alcohol consump-tion, body mass index, socioeconomic status, and family history of cancer. These are major risk factors for multiple can-cers and may be indirectly associated with 5ARI use. How-ever, because the NHIRD covers a highly representative sample of Taiwan’s general population and the reimbursement policy is universally the same, it is unlikely that these factors would have affected the prescription of 5ARIs.
Second, the evidence derived from a nested case-control study is generally lower in quality than that from randomized trials because a nested case-control study design is subject to many biases related to adjustments for confounding variables. Despite our meticulous study design with adequate control of confounding factors, a key limitation is that bias could remain if unmeasured or unknown confounders were present.
Third, the diagnoses recorded in NHI claims primarily serve the purpose of administrative billing and do not undergo verification for scientific purposes. We were unable to contact the patients directly to enquire on their use of 5ARIs because all beneficiaries listed on the NHIRD are protected by ano-nymity. Furthermore, our analysis was unable to consider pre-scriptions for 5ARIs issued before 1996. This omission could have led to an underestimation of the cumulative dosage and may have weakened the observed association. However, data on the prescription of 5ARIs and cancer diagnosis were reliable.
In conclusion, this population-based nested case-control study did not find a chemopreventive role of 5ARIs for pros-tate cancer. On the contrary, our results suggested that low doses of finasteride may actually increase the risk of prostate cancer. Possible underlying mechanisms for such an associa-tion have yet to be investigated and identified. Further large population-based studies or large-scale randomized clinical trials to confirm our findings are mandatory before any definite conclusions can be drawn.
ACKNOWLEDGMENTS
This work was supported by the China Medical University Hospital (DMR-100-110 and DMR-101-080), the Taiwan
by Chia-Hung Kao on August 13, 2012
www.TheOncologist.alphamedpress.org
Department of Health Cancer Research Center for Excellence (DOH101-TD-C-111-005).
AUTHORCONTRIBUTIONS
Conception/Design: Ji-An Liang, Chia-Hung Kao, Li-Min Sun, Ming-Chia Lin, Shih-Ni Chang, Fung-Chang Sung, Chih-Hsin Muo
Provision of study material or patients: Ji-An Liang, Chia-Hung Kao, Li-Min Sun, Ming-Chia Lin, Shih-Ni Chang, Fung-Chang Sung, Chih-Hsin Muo
Collection and/or assembly of data: Ji-An Liang, Chia-Hung Kao, Li-Min Sun, Ming-Chia Lin, Shih-Ni Chang, Fung-Chang Sung, Chih-Hsin Muo
Data analysis and interpretation: Ji-An Liang, Chia-Hung Kao, Li-Min Sun, Ming-Chia Lin, Shih-Ni Chang, Fung-Chang Sung, Chih-Hsin Muo
Manuscript writing: Ji-An Liang, Chia-Hung Kao, Li-Min Sun, Ming-Chia Lin, Shih-Ni Chang, Fung-Chang Sung, Chih-Hsin Muo Final approval of manuscript: Chia-Hung Kao, Li-Min Sun, Ming-Chia Lin,
Shih-Ni Chang, Fung-Chang Sung, Chih-Hsin Muo, Ji-An Liang
REFERENCES
1. Pritchard CC, Nelson PS. Gene expression profiling
in the developing prostate. Differentiation 2008;76: 624 – 640.
2. Nelson PS, Clegg N, Arnold H et al. The program of
androgen-responsive genes in neoplastic prostate epithe-lium. Proc Natl Acad Sci U S A 2002;99:11890 –11895.
3. Nickel JC. Comparison of clinical trials with
finas-teride and dutasfinas-teride. Rev Urol 2004;6:S31–S39.
4. Theoret MR, Ning YM, Zhang JJ, et al. The risks and
benefits of 5␣-reductase inhibitors for prostate-cancer prevention. N Engl J Med 2011;365:97–99.
5. Thompson IM, Goodman PJ, Tangen CM et al. The
influence of finasteride on the development of prostate cancer. N Engl J Med 2003;349:215–224.
6. Andriole GL, Bostwick DG, Brawley OW et al.
Ef-fect of dutasteride on the risk of prostate cancer. N Engl J Med 2010;362:1192–1202.
7. Akaza H, Kanetake H, Tsukamoto T et al. Efficacy
and safety of dutasteride on prostate cancer risk reduc-tion in Asian men: the results from the REDUCE study. Jpn J Clin Oncol 2011;41:417– 423.
8. Lu JF, Hsiao WC. Does universal health insurance
make health care unaffordable? Lessons from Taiwan. Health Aff (Millwood) 2003;22:77– 88.
9. Cancer Statistics Annual Report. Taiwan Cancer
Registry. Available at http://tcr.cph.ntu.edu.tw/main. php?Page⫽N2. Accessed November 16, 2011.
10. Edwards BK, Ward E, Kohler BA et al. Annual
re-port to the nation on the status of cancer, 1975–2006, fea-turing colorectal cancer trends and impact of interventions (risk factors, screening, and treatment) to reduce future rates. Cancer 2010;116:544 –573.
11. Sim HG, Cheng CW. Changing demography of
prostate cancer in Asia. Eur J Cancer 2005;41:834 – 845.
12. Liang JA, Sun LM, Yeh JJ et al. The association
between malignancy and end-stage renal disease in Tai-wan. Jpn J Clin Oncol 2011;41:752–757.
13. Ross RK, Bernstein L, Lobo RA et al.
5-Alpha-reductase activity and risk of prostate cancer among Jap-anese and US white and black males. Lancet 1992;339: 887– 889.
14. Giovannucci E, Stampfer MJ, Krithivas K et al.
The CAG repeat within the androgen receptor gene and its relationship to prostate cancer. Proc Natl Acad Sci U S A 1997;94:3320 –3323.
15. Hsing AW, Reichardt JK, Stanczyk FZ. Hormones
and prostate cancer: current perspectives and future di-rections. Prostate 2002;52:213–235.
16. Rittmaster RS. 5alpha-reductase inhibitors in
be-nign prostatic hyperplasia and prostate cancer risk reduc-tion. Best Pract Res Clin Endocrinol Metab 2008;22: 389 – 402.
17. Andriole GL, Guess HA, Epstein JI et al. Treatment
with finasteride preserves usefulness of prostate specific antigen in the detection of prostate cancer: results of a randomized, double-blind, placebo controlled clinical trial. Urology 1998;52:195–202.
18. Andriole GL, Bautista M, Crawford D et al.
Pros-tate cancer (CAP) detection in the medical therapy of prostatic symptoms (MTOPS) trial. Abstract presented at: American Urological Association Annual Meeting, April 26 –May 1 2003, Chicago, IL.
19. Roehrborn CG, Nickel JC, Andriole GL et al.
Du-tasteride improves outcomes of benign prostatic hyper-plasia when evaluated for prostate cancer risk reduction: secondary analysis of the REduction by DUtasteride of prostate Cancer Events (REDUCE) trial. Urology 2011; 78:641– 646.
20. Traish AM, Hassani J, Guay AT et al. Adverse side
effects of 5␣-reductase inhibitors therapy: persistent di-minished libido and erectile dysfunction and depression in a subset of patients. J Sex Med 2011;8:872– 884.
21. Hamilton RJ, Freedland SJ. 5-␣ reductase
inhibi-tors and prostate cancer prevention: where do we turn now? BMC Med 2011;9:105.
22. Parekh DJ. Prostate cancer prevention with 5
al-pha-reductase inhibitors. Recent Results Cancer Res 2011;188:109 –114.
23. Hamilton RJ, Kahwati LC, Kinsinger LS.
Knowl-edge and use of finasteride for the prevention of prostate cancer. Cancer Epidemiol Biomarkers Prev 2010;19: 2164 –2171.
24. Chuang AY, Chang SJ, Horng CF et al. Study of
prostate cancer pathologic features in Chinese popula-tions. Urology 2007;69:915–920.
25. Gormley GJ. Finasteride: a clinical review.
Biomed Pharmacother 1995;49:319 –324.
See the accompanying commentary on pages 888 – 890 of this issue.
www.TheOncologist.com
by Chia-Hung Kao on August 13, 2012
www.TheOncologist.alphamedpress.org
DOI: 10.1634/theoncologist.2011-0464
2012;17;986-991; originally published online June 20, 2012;
The Oncologist
Chih-Hsin Muo and Chia-Hung Kao
Ji-An Liang, Li-Min Sun, Ming-Chia Lin, Shih-Ni Chang, Fung-Chang Sung,
Prostate Hyperplasia
Inhibitors Did Not Decrease Prostate Cancer Risk in Patients with Benign
This information is current as of August 13, 2012
& Services
Updated Information
http://theoncologist.alphamedpress.org/content/17/7/986
including high-resolution figures, can be found at:
by Chia-Hung Kao on August 13, 2012
www.TheOncologist.alphamedpress.org