Kaohsiung J Med Sci February 2009 • Vol 25 • No 2 98
Liver abscess is a common intra-abdominal infection that has many possible causative pathogens includ-ing bacterial, fungal or parasitic organisms. In the 1990s, Klebsiella pneumonia (Kp) liver abscess was first described as an emerging disease in Taiwan, and Kp was found to be the leading cause of liver abscess in patients with diabetes [1–4]. Kp is a colonizer of the human gastrointestinal tract and is rarely associated with disease in the normal host. Various diseases have been associated with liver abscess, including biliary tract malignancies, appendicitis, diverticulitis and enteritis [5]. Patients with diabetes mellitus were also found to be more susceptible to Kp-associated
liver abscess and bacteremia. It is well-known that
Streptococcus bovis (Sb) bacteremia offers a diagnostic
marker for the presence of occult colon carcinoma. The ulcerated surface of neoplastic lesions forms a path-way for the microorganism to enter the bloodstream [6]. In addition to Sb, other kinds of colon-colonizing bacteria may enter the blood stream via a similar pathway. Here, we report a case of a patient with dia-betes with recurrent Kp liver abscess who was later confirmed to have an occult sigmoid colonic tumor.
C
ASEP
RESENTATIONThe case was an 82-year-old female with type 2 diabetes mellitus and hypertension, which were con-trolled by regular oral medications for more than 20 years. The first time she was admitted to our hos-pital was on July 10, 2006 for general malaise and fluctuation of self-monitored blood sugar at home. Received: Jul 18, 2008 Accepted: Sep 8, 2008
Address correspondence and reprint requests to: Dr Chien-Yu Lu, Division of Gastroenterology, Department of Internal Medicine, Kaohsiung Medical University Hospital, 100 Tzyou 1stRoad,
Kaohsiung 807, Taiwan.
E-mail: [email protected]
O
CCULT
C
OLON
C
ANCER IN A
P
ATIENT WITH
D
IABETES AND
R
ECURRENT
K
LEBSIELLA
PNEUMONIAE
L
IVER
A
BSCESS
Wen-Hung Hsu,1Fang-Jung Yu,1Chien-Han Chuang,2Chin-Fan Chen,3
Chien-Ting Lee,4and Chien-Yu Lu1,5
1Division of Gastroenterology, Department of Internal Medicine, and 5Faculty of Medicine,
College of Medicine, Kaohsiung Medical University, 2Division of Gastrointestinal and General Surgery,
Department of Surgery, Kaohsiung Medical University Hospital, Kaohsiung, and Departments of
3Surgery and 4Internal Medicine, Pingtung Hospital, Department of Health, Pingtung, Taiwan.
Klebsiella pneumoniae (Kp) is a well-known leading cause of liver abscess in patients with diabetes,
but recurrent Kp liver abscess in such patients within a period of time is seldom seen. Here, we report a patient with diabetes who experienced three episodes of Kp liver abscess within 1 year. The patient was subsequently diagnosed to have an occult sigmoid cancer. The liver abscess did not recur after resection of the colonic tumor. Occult sigmoid colonic cancer may have played an important role in the recurrent Kp liver abscess in our case. Therefore, further investigation of gastrointestinal malignancies, particularly of the colonic tract, is necessary in patients with diabetes and Kp liver abscess.
Key Words:colonic cancer, diabetes mellitus, Klebsiella pneumoniae, liver abscess (Kaohsiung J Med Sci 2009;25:98–103)
Laboratory examination showed leukocytosis and elevated C-reactive protein. Accordingly, abdominal ultrasonography (US) was done to identify the focus of infection and a mixed echoic space-occupying lesion was found over the anterior superior segment of the right hepatic lobe (S8), and which showed as a hypodense lesion on routine abdominal computed tomography (CT) (Figure 1). The liver abscess was confirmed by fine needle aspiration with black-red
pus from a hepatic-occupying lesion. Blood and aspi-rated (drained) abscess cultures showed wild-type
Kp. She was treated with percutaneous transhepatic
abscess drainage and parenteral antibiotic during hos-pitalization. After discharge, an oral antibiotic was prescribed for a total 6 weeks of treatment. Follow-up abdominal US showed the liver abscess was resolved into a residual cystic lesion (Figure 2C).
Unfortunately, this patient developed another two episodes of Kp liver abscess in the following year. In May, 2007, she suffered from intermittent fever with chills for 1 week. Complete blood counts showed leu-kocytosis and mild anemia, but negative stool occult blood test. Abdominal US showed a mixed echoic space-occupying lesion over the posterior superior segment of the right hepatic lobe (S7), which was dif-ferent from the first episode. Liver abscess was diag-nosed by fine needle aspiration of the S7 lesion. Blood and aspirated pus cultures again showed wild-type Kp. A similar therapeutic procedure and complete course of antibiotics were also given. Unexpectedly, 3 months later, the third episode of Kp liver abscess occurred with the presentation of general malaise and inter-mittent fever over 1 week. This time, abdominal US disclosed a mixed echoic space-occupying lesion over Figure 1.Abdominal computed tomography at the first admission
shows a hypodense space-occupying lesion over the S8 area.
A B
C
Figure 2.(A) A heterogeneous space-occupying lesion in the S2 area was found by abdominal ultrasonography. (B) Abdominal com-puted tomography shows a hypodense lesion over the S2 area (arrowhead). (C) Abdominal comcom-puted tomography reveals trace remnants of a previous S8 liver abscess (arrow).
the lateral superior segment of the left hepatic lobe (S2), which was surprisingly different from the previ-ous two episodes (Figure 2). Fine needle aspiration of the S2 liver abscess was performed again, and the aspirated pus culture again showed Kp bacteria. A progressive decline in her hemoglobin level and pos-itive stool occult blood test were found during this admission.
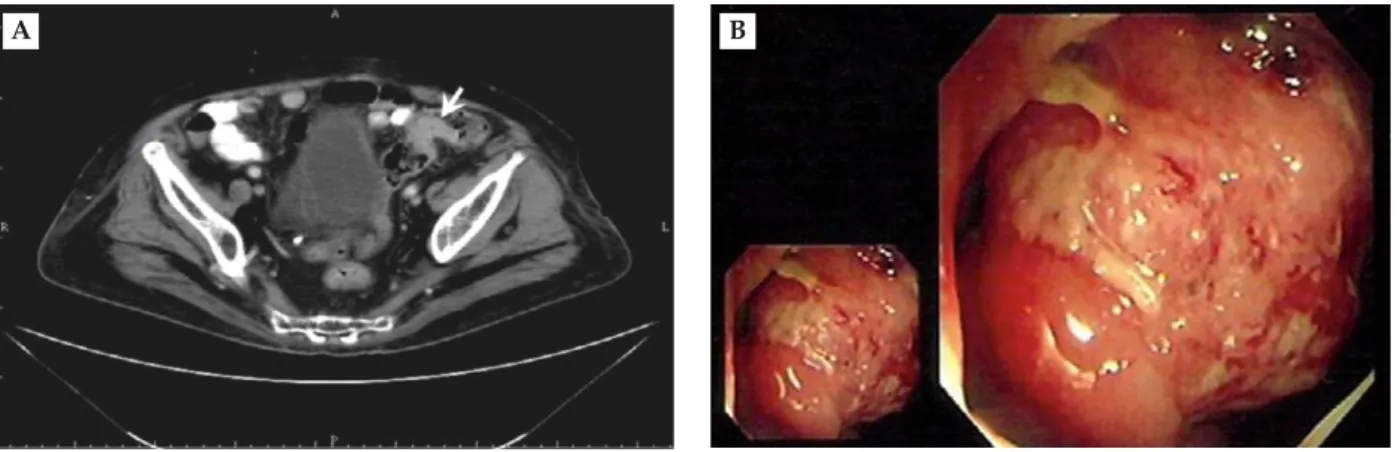
Colonoscopy was advised, but the patient re-fused. Again, abdominal CT with enhancement was arranged, and the scan was extended to the pelvic area to completely evaluate the gastrointestinal tract. Segmental wall thickness over the sigmoid colon was noted on the CT scan (Figure 3). Colonoscopy was strongly advised and colonic adenocarcinoma was confirmed by pathologic biopsy. After controlling the infection, surgical intervention was performed to resect
the sigmoid tumor. During the operation, periabscess liver tissue was collected for pathologic examination to rule out metastatic lesions, and surgical drainage was done incidentally. Postoperative pathology showed stage IIa (T3N0M0) and the tumor had invaded the
serosa; however, lymph nodes were not involved.
D
ISCUSSIONThe clinical course of our patient is summarized in the Table. Diabetes mellitus was well controlled in the last two hospitalizations, as documented by HbA1C levels less than 7%. At the first admission, the patient’s diagnosis was thought to be primary Kp liver abscess because the abdominal CT did not show any other biliary tract or intra-abdominal sources of infection.
A B
Figure 3.(A) Abdominal computed tomography extended to the pelvic area shows segmental wall thickness over the sigmoid colon (arrow). (B) An ulcerated tumor mass was detected by colonoscopy and pathologic biopsy verified adenocarcinoma.
Table.Presentation, location, laboratory data, and treatment of three episodes of liver abscess in our patient Time of diagnosis
July 2006 May 2007 August 2007
HbA1C (%) 8.8 6.8 6.6
Presentations General malaise, Intermittent fever General malaise, unstable blood sugar with chills intermittent fever Location of liver abscess Segment 8 Segment 7 Segment 2
Blood culture Kp Kp No growth
Abscess culture Kp Kp Kp
Hemoglobin (g/dL) 12.6 10.2 9.5
Stool occult blood Not checked Negative Positive
CEA (ng/mL) Not checked Not checked 2.31
Treatment Abscess drainage, Abscess aspiration, Abscess aspiration, cephalosporin* cephalosporin* surgical drainage,
cephalosporin* *Empirical antibiotic with cefotaxime initially, then shifting to cephradine according to culture result and drug sensitivity test. Kp= Klebsiella pneumoniae; CEA = carcinoembryonic antigen.
The patient did not complain of any abdominal symp-toms except for a mild right upper quadrant tender-ness due to the liver abscess. The patient did not report any bowel habit change, tenesmus or bloody stool. The misdiagnosis of sigmoid cancer in the first admission could be attributed to the “routine” abdom-inal CT scan, which does not normally include the pelvic area.
The two subsequent episodes of Kp liver abscess occurred in different hepatic segments within 1 year, which implied that these different episodes may arise from the same portal venous seeding of colon colo-nization [7]. The other findings implicating colonic lesion were that the test of stool occult blood became positive and a decline in hemoglobin levels was noted in the follow-up laboratory data. After resection of sigmoid cancer, no more liver abscess was noted until now.
The association between Sb bacteremia with colonic carcinoma is well known. Several possible mechanisms have been proposed to account for this association. Increased Sb colonization along with disruption of the colonic mucosa may favor Sb bacteremia [6]. More-over, Sb and Kp are both colonizers in the human gas-trointestinal tract. Kp-pathogenic liver abscess is a well-known infectious complication in patients with diabetes [1–4]. Indeed, patients with diabetes are known to show defects in neutrophil chemotaxis and phagocytosis, which are thought to be the most im-portant predisposing factors for Kp-pathogenic liver abscess [8]. Most of these cases were thought to be pri-mary Kp liver abscess because they were free of biliary disease or other intra-abdominal infection. Patients with diabetes who recovered from primary Kp liver abscess after adequate antibiotic treatment have rarely relapsed [2].
Pyogenic liver abscess secondary to malignancy has been reported by Yeh et al [9]. Six patients (11.5%) had colorectal cancers among their 52 studied cases with underlying malignancy. They concluded that pyogenic liver abscess can be a presentation of underlying hepatopancreatobiliary malignant disease before the terminal stage, but carried a poor prognosis compared with non-hepatopancreatobiliary malignant patients [9]. Our patient was a non-hepatopancreatobiliary malignant case and received a good prognosis after surgical resection of sigmoid cancer.
Hiraoka et al reported three cases of Kp liver abscess associated with colon cancer and reviewed
41 pyogenic liver abscess cases in their hospital [10]. Malignant disease occurred in 12 of a total of 41 patients (29.3%) including three cases of colonic can-cers. In their 41 cases, diabetes mellitus was found to be the most commonly associated disease for liver abscess (14/41, 34.1%), and was also the major med-ical disease in our patient. Thirty-two of these 41 patients received liver abscess drainage and 71.9% (23/32) patients were positive for bacteria, with Kp being the most frequent (13/32, 40.6%), followed by
Escherichia coli (6/32, 18.8%). Our patient also had
positive Kp cultures from blood and aspirated pus. Few reports have described Kp liver abscess asso-ciated with diabetic and colonic malignancy [10,11].
Kp liver abscess could be a complication of Kp
bac-teremia, because this organism enters the portal circu-lation from the erosive surface of colonic cancer [12]. Diabetes and colonic malignancies may have syner-gistic effects on the occurrence of Kp liver abscess. To our knowledge, Kp liver abscess associated with colonic neoplasm have been rarely reported [11]. In our case, the characteristic recurrent episodes of liver abscess prompted us to further investigate if there was any underlying predisposing factor.
Kp liver abscess is a common intra-abdominal
infection in patients with diabetes. The real incidence of colonic neoplasms in such cases may be overlooked. Our case with recurrent Kp liver abscess reminded us that colonic cancer may also be present without spe-cific symptoms or laboratory findings. Kp liver abscess could be the only initial presentation of colonic cancer, and CT of the whole abdomen, including the pelvic area, provides an opportunity to detect possible occult colonic lesions.
Many risk factors have been identified for colorectal cancer including aging, high-fat diet, obesity, familial polyposis syndrome and inflammatory bowel disease. Recent evidence indicates metabolic abnormalities such as impaired glucose tolerance and diabetes mel-litus are also associated with increased incidence of colonic adenoma and cancer [13,14]. Insulin resistance and hyperinsulinemia may also play critical roles, but the detailed mechanisms are still being investigated. Accordingly, diabetes mellitus can be thought of as a risk factor for colorectal cancer. In our case, old age and diabetes mellitus were additional prompts to consider further evaluation of colon lesions.
Therefore, we recommend that, when a liver abscess is diagnosed, aggressive evaluation of colonic
occult malignancy is essential, particularly in patients with diabetes.
R
EFERENCES1. Chang SC, Fang CT, Hsueh PR, et al. Klebsiella
pneumo-niae isolates causing liver abscess in Taiwan. Diagn Microbiol Infect Dis 2000;37:279–84.
2. Wang JH, Liu YC, Lee SS, et al. Primary liver abscess due to Klebsiella pneumoniae in Taiwan. Clin Infect Dis 1998;26:1434–8.
3. Lee KT, Wong SR, Sheen PC. Pyogenic liver abscess: an audit of 10 years’ experience and analysis of risk factors. Dig Surg 2001;18:459–66.
4. Yang CC, Chen CY, Lin XZ, et al. Pyogenic liver abscess in Taiwan: emphasis on gas-forming liver abscess in diabetics. Am J Gastroenterol 1993;88:1911–5.
5. Wallack MK, Brown AS, Austrian R, et al. Pyogenic liver abscess secondary to asymptomatic sigmoid divertic-ulitis. Ann Surg 1976;184:241–3.
6. Klein RS, Recco RA, Catalano MT, et al. Association of
Streptococcus bovis with carcinoma of the colon. N Engl J Med 1977;297:800–2.
7. Lai HC, Chan CY, Peng CY, et al. Pyogenic liver abscess associated with large colonic tubulovillous adenoma.
World J Gastroenterol 2006;12:990–2.
8. Delamaire M, Maugendre D, Moreno M, et al. Impaired leucocyte functions in diabetic patients. Diabet Med 1997; 14:29–34.
9. Yeh TS, Jan YY, Jeng LB, et al. Pyogenic liver abscesses in patients with malignant disease: a report of 52 cases treated at a single institution. Arch Surg 1998;133: 242–5.
10. Hiraoka A, Yamashita Y, Uesugi K, et al. Three cases of liver abscesses complicated with colon cancer without liver metastasis: importance of screening for digestive disease. Intern Med 2007;46:2013–7.
11. Weng SW, Liu JW, Chen WJ, et al. Recurrent Klebsiella
pneumoniae liver abscess in a diabetic patient followed
by Streptococcus bovis endocarditis—occult colon tumor plays an important role. Jpn J Infect Dis 2005;58: 70–2.
12. Teitz S, Guidetti-Sharon A, Manor H, et al. Pyogenic liver abscess: warning indicator of silent colonic cancer. Report of a case and review of the literature. Dis Colon
Rectum 1995;38:1220–3.
13. Nilsen TI, Vatten LJ. Prospective study of colorectal cancer risk and physical activity, diabetes, blood glucose and BMI: exploring the hyperinsulinaemia hypothesis.
Br J Cancer 2001;84:417–22.
14. Giovannucci E, Michaud D. The role of obesity and related metabolic disturbances in cancers of the colon, prostate, and pancreas. Gastroenterology 2007; 132:2208–25.
收文日期:97 年 7 月 18 日 接受刊載:97 年 9 月 8 日 通訊作者:盧建宇醫師 高雄醫學大學附設醫院胃腸內科 高雄市三民區自由一路 100 號