Choroidal Vasculopathy: A Case Control Study
Hui-Chen Cheng1,2, Jorn-Hon Liu1,2,3, Shui-Mei Lee1,2, Po-Kang Lin1,2,4,5*
1 Department of Ophthalmology, School of Medicine, National Yang-Ming University, Taipei, Taiwan, 2 Department of Ophthalmology, Taipei Veterans General Hospital,
Taipei, Taiwan, 3 Department of Ophthalmology, Cheng Hsin Rehabilitation Medical Center, Taipei, Taiwan, 4 Graduate Institute of Biomedical Electronics and
Bioinformatics, National Taiwan University, Taipei, Taiwan,5 Biomedical Electronics Translational Research Center, National Chiao Tung University, Hsinchu, Taiwan
Abstract
Purpose:To determine whether elevated plasma homocysteine and serum high sensitivity C-reactive protein (hsCRP) levels, two established risk factors of vascular diseases, are associated with polypoidal choroidal vasculopathy (PCV).
Design:Retrospective case-control study.
Methods:One hundred and nineteen consecutive patients with PCV and 119 matched controls were enrolled in a tertiary hospital from September 2008 to June 2013. Plasma homocysteine and serum hsCRP levels were measured. Associations among plasma homocysteine, serum hsCRP levels and PCV were further evaluated using multivariable logistic regression analysis.
Results: The median plasma homocysteine level was significantly higher in patients with PCV than in the controls (12.20mmol/L vs. 9.80mmol/L, p,0.001). The median serum hsCRP level was slightly higher in the PCV group (0.16 mg/dl vs. 0.11 mg/dl in control group, p = 0.07). After multivariable logistic regression analysis, each 1mmol/L increase of plasma homocysteine was associated with a 1.5-fold increase in likelihood of having PCV (OR, 1.54; 95% confidence interval (CI), 1.33–1.79, p,0.001).
Conclusions:Hyperhomocysteinemia was associated with PCV and might play a role in the pathogenesis of PCV.
Citation: Cheng H-C, Liu J-H, Lee S-M, Lin P-K (2014) Hyperhomocysteinemia in Patients with Polypoidal Choroidal Vasculopathy: A Case Control Study. PLoS ONE 9(10): e110818. doi:10.1371/journal.pone.0110818
Editor: Alfred S. Lewin, University of Florida, United States of America
Received June 1, 2014; Accepted September 22, 2014; Published October 22, 2014
Copyright: ß 2014 Cheng et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Data Availability: The authors confirm that all data underlying the findings are fully available without restriction. All relevant data are within the paper and its Supporting Information files.
Funding: The authors would like to thank the National Science Council of the Republic of China, Taiwan, for supporting this research under Contract No. NSC101-2220-E-010-001. This work was also supported by the ‘‘Aim for the Top University Plan’’ of the National Chiao Tung University and Ministry of Education, Taiwan, R. O. C. The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript. Competing Interests: The authors have declared that no competing interests exist.
* Email: pklin123@hotmail.com
Introduction
Polypoidal choroidal vasculopathy (PCV), first proposed by Yannuzzi et al, [1] is characterized by an inner choroidal vascular network ending in an aneurysmal bulge, visible clinically as a reddish orange, polyp-like structure. The affected eye typically presents with multiple recurrent serous or hemorrhagic detach-ments of the retinal pigment epithelium (RPE) [1,2]. The diagnostic features of PCV are the presence of subretinal nodular hyperfluorescence (the polyps), which may be associated with branching vascular networks in fundus indocyanine green angiography (ICGA) [3]. In earlier reports, PCV accounts for 20–50% of cases manifesting as exudative age-related macular degeneration (AMD) in Asia, compared to approximately 10% in patients of Western descent [2,4–6]. However, PCV has been proposed as a distinct disease entity with its characteristic polypoidal structures and branching vascular networks, which is different from choroidal neovascularization (CNV) of AMD [7]. PCV tends to present at a younger age compared to exudative
AMD, with a male preponderance and more frequently in black or Asian patients [1,2,8,9]. Although the pathogenesis of PCV remains largely unknown, there have been several pathological reports that have noted inner choroidal vessel abnormalities with arteriosclerosis in PCV, possibly indicating an association with vascular diseases [10–12].
Homocysteine is a naturally occurring sulfur-containing amino acid that is produced during the metabolism of methionine. High plasma levels of homocysteine have been identified as an independent risk factor of vascular diseases, such as cardiovascular disease and stroke, dementia and Alzheimer’s disease [13–15]. Elevated plasma homocysteine levels are also observed in patients with retinal vascular occlusion diseases, pseudoexfoliative glauco-ma and diabetic retinopathy [16–19]. Patients with AMD glauco-may also present with elevated plasma homocysteine levels but results are inconsistent [20,21].
C-reactive protein (CRP) is a systemic inflammatory biomarker and a risk factor of cardiovascular disease [22].Kikuchi et al [23] found a significant association between elevated high sensitivity
CRP (hsCRP) levels and PCV in the Japanese, and concluded that inflammatory processes were involved in the pathogenesis of PCV. However, further correlations need to be elucidated.
From the clinical manifestations and pathological reports, we propose a hypothesis that PCV is a vascular disorder related to arteriosclerosis, which may be associated with the risk factors of vascular diseases. The purpose of this study is to determine whether elevated plasma homocysteine and serum hsCRP levels, two established risk factors of vascular diseases, are associated with PCV.
Materials and Methods Study subjects
The authors conducted a case-control study with retrospective recruitment of study subjects from a tertiary hospital between September 2008 and June 2013. The study protocol adhered to the tenets of the Declaration of Helsinki. It was approved by the Institutional Review Board of the Taipei Veterans General Hospital. Though the requirement for informed consent was waived by the approving IRB, verbal informed consent was obtained and recorded on the medical chart.
Patients diagnosed with PCV were recruited consecutively during the study period. The control group included subjects who were undergoing routine physical examinations or follow-up for diseases other than AMD, retinal vascular disease, diabetic retinopathy or glaucoma. Each case was then matched with one control subject on age and gender. All study subjects were of Chinese ethnicity.
Exclusion criteria included subjects without data of plasma homocysteine level, significant comorbidity that could confuse the clinical picture, such as retinal vascular occlusion, uveitis, trauma-related eye disease, other neovascular maculopathies, and media opacities preventing adequate fundus examination. Subjects with renal dysfunction, defined as having a serum creatinine level more than 1.5 mg/dl or having a history of renal failure, and a history of taking vitamin supplements, were also excluded due to their effect on plasma homocysteine [24,25].
All participants received a complete ophthalmic examination consisting of best-corrected visual acuity, slit lamp biomicroscopy and fundoscopy. Fundus photography with fluorescein angiogra-phy (FA) taken with a fundus camera (CF-60 UD, Canon Inc., Tokyo, Japan) and ICGA (Heidelberg Retina Angiograph II, Heidelberg Engineering, Heidelberg, Germany) were performed through dilated pupils in all case subjects. The retinal images were all reviewed by two retina specialist (P.K.L. and J.H.L) in a masked fashion. Only subjects with characteristic polyp-like choroidal vessel dilatation (polypoidal lesions or polyps) on ICGA were diagnosed to have PCV [26]. The diagnosis was confirmed when both of them had come to an agreement. Location of PCV was divided into extrafoveal, juxtafoval (within 200mm of the fovea), subfoveal and peripapillary area (within one disc diameter of the optic disc) [27].
Data including age, gender, lifestyle factors of smoking and alcohol consumption, medication histories, medical histories of hypertension, diabetes mellitus (DM), coronary artery disease, cerebrovascular event and renal dysfunction were obtained from all subjects.
Total plasma homocysteine analysis
Fasting venous blood samples were obtained in the sitting position and collected in test tubes containing heparin. The samples were immediately centrifuged at 4uC, and the plasma homocysteine levels were measured by automated
chemilumines-cent immunoassay (ADVIA Centaur system, Siemens, East Walpole, MA, USA), with a sensitivity of 0.5mmol/L and a total coefficient of variation (CV) of 6.8% at 4.9mmol/L, 3.9% at 61.6mmol/L. This assay correlates well with other assays, including fluorescent polarization immunoassay and high-perfor-mance liquid chromatography (HPLC) [28].
High sensitivity C-reactive protein (hsCRP) analysis
Venous blood samples were obtained and collected in serum-separation tubes. Serum hsCRP was measured by rate nephelom-etry on an automated nephelometer (Immage 800, Beckman Coulter, Fullerton, CA, USA). This hsCRP assay, with an analytical sensitivity of 0.2 mg/L and a total coefficient of variation (CV) of 5.17% at 0.79 mg/L, and 3.8% at 13.4 mg/L, has been shown to correlate well with other commonly used assays [29].
Hyperhomocysteinemia and elevated hsCRP level were defined as levels above the 95th percentile of the control group.
Statistical analysis
Continuous and categorical variables in demographic and medical characteristics were compared between PCV cases and control subjects using Student’st-test and Pearson’s chi-square test, respectively. Plasma homocysteine and serum hsCRP levels were presented as median (interquartile range) and compared to controls using the Mann-Whitney U test because homocysteine and hsCRP levels were not normally distributed.
Multivariable logistic regression models were used to evaluate whether or not PCV was associated with plasma homocysteine or serum hsCRP. All odds ratios (ORs) were adjusted for age, gender, lifestyle factors (smoking and alcohol consumption) and medical histories (hypertension, DM, coronary artery disease, cerebrovas-cular event).
SPSS for Windows version 18 (SPSS Inc, Chicago, Illinois, USA) was used for these calculations. All reported P values were based on 2-sided tests and a P value of less than 0.05 was considered to be statistically significant.
Results
One hundred and twenty-four case subjects were enrolled initially. Three patients were excluded due to renal dysfunction and two were excluded due to revised diagnosis of CNV with AMD. Finally, a total of 119 patients with PCV and 119 matched controls were enrolled in this study.
The mean age was 72.1613.0 years in the PCV group and 69.3610.9 years in the control group, with a male preponderance (74.8%) in both groups. There were no statistically significant differences in age, gender, medical histories of hypertension, DM, coronary artery disease, cerebrovascular event and lifestyle factors including smoking and alcohol consumption between case subjects and controls (Table 1).
The median plasma homocysteine level was significantly higher in the PCV group (median, 12.20mmol/L; interquartile range, 9.67–16.66mmol/L) than in the control group (median, 9.80mmol/L; interquartile range, 8.13–11.26mmol/L; p, 0.001). The homocysteine evaluation can be further categorized into subgroup with DM and without DM. The plasma homo-csyteine level of PCV patients with DM was significantly higher than controls with DM (p = 0.001). Also, the plasma homocsyteine level of PCV patients without DM was significantly higher than controls without DM (p,0.001). The median serum hsCRP level was slightly higher in the PCV group (median, 0.16 mg/dl; interquartile range, 0.06–0.30 mg/dl) than in the control group
(median, 0.11 mg/dl; interquartile range, 0.06–0.25 mg/dl, p = 0.07) (Table 2).
The 95th percentile of the homocysteine level in the control group was 13.26mmol/L. Of the 119 PCV patients, 47 (39.5%) patients exceeded this cutoff value, compared with 5 of 119 (4.2%) patients in the control group (p,0.001). The 95thpercentile of the hsCRP level in the control group was 0.70 mg/dl. In the PCV group, 13 of 118 (11.1%) patients exceeded the cutoff value, compared with 6 of 113 (5.4%) patients in the control group (p = 0.12) (Table S1).
After stratified by genders, both males and females of the PCV group had significantly higher plasma homocysteine levels (p, 0.001 in male and p = 0.02 in female) and proportions of hyperhomocysteinemia (p,0.001 in male and p = 0.02 in female), compared to those of the controls. The results of hsCRP levels were generally insignificant except for the higher proportions of elevated hsCRP in female (26.7% vs 3.4% in controls, p = 0.01) (Table 2 and Table S1). If we stratified the homocysteine levels into tertiles, significantly higher proportion of PCV patients had homocysteine levels in the highest tertile, compared to controls (67.2% vs. 32.8% in controls, p,0.001) (Table 3).
In the multivariable logistic regression analysis, after adjusting for age, gender, hypertension, DM, coronary artery disease, cerebrovascular event, smoking and alcohol consumption, it was observed that elevated plasma homocysteine levels were signifi-cantly associated with an increasing risk of PCV (OR, 1.54; 95% confidence interval (CI), 1.33–1.79, p,0.001), but not the hsCRP (OR, 1.82; 95% CI 0.61–5.45, p = 0.29). If we defined hyperhomocysteinemia and elevated hsCRP as levels above the 95th percentile of the control group, hyperhomocysteinemia is still significantly associated with PCV (OR, 22.04; 95% CI 7.05–68.92, p,0.001) in the multivariable logistic regression analysis, but not with the elevated hsCRP (OR, 2.45; 95% CI 0.75–7.94, p = 0.14). Moreover, people in the highest tertile of homocysteine had an approximately 9-fold increased risk of PCV (OR, 8.84; 95% CI 3.68–21.21, p,0.001) in the regression model (Table 3).
Of the 119 PCV patients, 17 (14.3%) had bilateral involvement, 49 (41.2%) had right-side involvement and 53 (44.5%) had left-side involvement. Comparing the bilateral involvement with unilateral involvement of PCV, no statistically significant differences in plasma homocysteine levels, serum hsCRP levels, age, gender,
lifestyle factors, or medical histories were noted between the two groups.
Of the 136 eyes with PCV, PCV lesions were found in the extrafoveal area in 74 (54.4%) eyes, juxtafoveal in 51 (37.5%) eyes, subfoveal in 9 (6.6%) eyes and peripapillary in 2 (1.5%) eyes. Branching vascular network was noted in 130 (95.6%) eyes. Eighty-one (59.6%) eyes had serous pigment epithelial detachment (PED), 16 (11.8%) eyes had hemorrhagic PED, 51 (37.5%) eyes had subretinal fluid and 20 (14.7%) eyes had subretinal hemorrhage.
Discussion
In our study, total plasma homocysteine levels were significantly higher in the PCV group than in the control group (median, 12.20mmol/L vs 9.80mmol/L in controls, p,0.001). On a multivariable logistic regression analysis, each 1mmol/L increase of plasma homocysteine was associated with a 1.5-fold increase in the likelihood of having PCV (OR, 1.54; 95% CI, 1.33–1.79, p, 0.001). Hyperhomocysteinemia, defined as levels above the 95th percentile of the control group, remained a relevant factor for PCV after regression analysis (OR, 22.04; 95% CI 7.05–68.92, p, 0.001). The increase in risk was also significant for the highest tertile of homocysteine for PCV (OR, 8.84; 95% CI 3.68–21.21, p,0.001). Hyperhomocysteinemia was identified to be associated with PCV in this study. However, whether the plasma homocys-teine contributes to direct toxicity on the pathogenesis of PCV or acts as a disease marker needs to be further determined.
The pathogenesis of PCV remains largely unknown. Possible association with systemic cardiovascular risk factors, such as hypertension, has been proposed [30]. The histopathology studies of PCV also showed inner choroidal vessel abnormalities with arteriosclerosis change [10–12,31]. A significant proportion of PCV patients in our study had hypertension or coronary artery disease (47.1% and 17.6%, respectively), provided additional evidence of the association between PCV and arteriosclerosis. Homocysteine is a potent excitatory neurotransmitter that binds to the N-methyl-D-aspartate (NMDA) receptor and leads to oxidative stress, cytoplasmic calcium influx, cellular apoptosis, and endo-thelial dysfunction, which contributes to atherogenesis [32]. Given the observation that PCV was a choroidal vessel abnormality with arteriosclerosis change, the toxic effect of hyperhomocysteinemia on vessel may contribute to the pathogenesis of PCV.
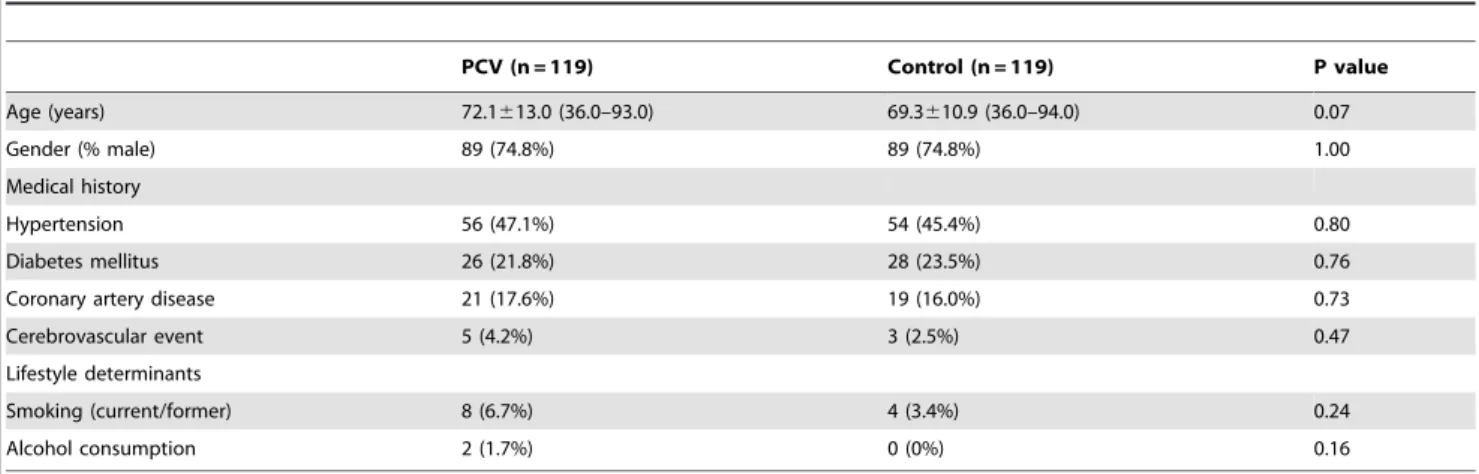
Table 1. Basic characteristics of patients with polypoidal choroidal vasculopathy and the control subjects.
PCV (n = 119) Control (n = 119) P value Age (years) 72.1613.0 (36.0–93.0) 69.3610.9 (36.0–94.0) 0.07 Gender (% male) 89 (74.8%) 89 (74.8%) 1.00 Medical history Hypertension 56 (47.1%) 54 (45.4%) 0.80 Diabetes mellitus 26 (21.8%) 28 (23.5%) 0.76
Coronary artery disease 21 (17.6%) 19 (16.0%) 0.73
Cerebrovascular event 5 (4.2%) 3 (2.5%) 0.47
Lifestyle determinants
Smoking (current/former) 8 (6.7%) 4 (3.4%) 0.24
Alcohol consumption 2 (1.7%) 0 (0%) 0.16
PCV, polypoidal choroidal vasculopathy;
Continuous variables are presented as mean 6 standard deviation (range) and compared using Student’s t-test. Categorical variables were presented as numbers (percentage) and compared using Pearson’s chi-square test. doi:10.1371/journal.pone.0110818.t001
Kondo et al [33] identify the elastin gene, a potent and specific regulator of the migration and proliferation of vascular smooth muscle cells, is a susceptible gene for PCV. The dysfunction of this signaling may lead to the development of vascular diseases such as arteriosclerosis [34]. The disruption of vascular elastin has also been proven to lead to aneurysm formation on animal model [35]. We proposed that elastin gene variation, which may be associated with the loss of function of vascular smooth muscle cells and the elastic layer of the vessel walls, together with homocysteine-mediated oxidative stress and endothelial dysfunction, and intraluminal pressure dysregulation, may lead to the final endpoint of choroidal aneurysmal bulging in PCV.
After stratified by gender, the plasma homocysteine level was found to be significantly different between male and female in our study (median, 13.91 umol/L in male with PCV vs. 9.29 umol/L in female with PCV, p,0.001). The trend was similar in both case and control subjects. After puberty, males have higher plasma homocysteine levels than females, with a gender difference in plasma homocysteine of approximately 2mmol/L [24]. The male-female difference has been attributed to sex differences in muscle mass, circulating sex hormones, and it may possibly modify the contribution of the methylenetetrahydrofolate reductase (MTHFR) mutation to homocysteine concentrations [36]. In our study, there were only 30 females in the PCV group, and they had a significantly lower rate of coronary artery disease compared to the males (3.3% in female vs. 22.5% in male p = 0.02). This may suggest different contributions to the pathogenesis in females with PCV, but further study is required given the small female sample size in this study.
Kikuchi et al [23] have found a significantly increasing risk for the highest quartile of hsCRP for PCV in Japanese. However, we found no significant difference in serum hsCRP levels between the PCV and control groups in our study. Although a higher proportion of elevated hsCRP seemed to be observed in females with PCV (p = 0.01), the small sample size precluded further analysis. From a previous report, focal aggregates of chronic inflammatory cells have been shown in the PCV specimens [37]. The discrepancy in the study results of hsCRP in PCV may suggest the role of chronic inflammation in the pathogenesis of PCV.
There were some limitations in this study. First, it was a retrospective case-control study in a single medical center. Second, MTHFR polymorphism, serum cobalamin and folate levels were not checked, which might influence plasma homocysteine levels [24]. However, the subjects in this study were all well-nourished and people who had history of taking vitamin supplements were excluded to prevent their effect on plasma homocysteine levels. Third, the median plasma homocysteine level (12.20mmol/L) in the PCV group was within the conventional definition of normal range (,15mmol/L). However, plasma homocysteine level may be affected by many factors including age, gender, ethnicity, nutritional status, lifestyle, and disease [24]. Reference intervals should be established for different populations or even different laboratories [24]. Considering the relative small sample size and heterogeneous characteristics in this study, the reference upper-limit was calculated as level above the 95th percentile for presumed healthy individuals. If we used conventional definition of hyperhomocysteinemia (.15mmol/L), 40 (33.6%) PCV patients still had elevated plasma homocysteine level, compared to 1 subject (0.8%) in the control group (p,0.001). The association still existed in the male group (43.8% in PCV vs 1.1% in controls, p,0.001) but not in the female group (3.3% in PCV vs 0% in controls, p = 0.31). After adjusting for age, gender, hypertension, DM, coronary artery disease, cerebrovascular event, smoking and
Table 2. Plasma homocysteine and serum C-reactive protein levels in overall and different genders of patients with polypoidal choroidal vasculopathy and th e control subjects. Overall Male Female PCV (n = 119) Control (n = 119) P value PCV (n = 89) Control (n = 89) P value PCV (n = 30) Control (n = 30) P value Homocysteine ( m mol/L) 1 2.20 (9.67–16.66) 9.80 (8.13–11.26) , 0.001 1 3.91 (11.43–17.65) 10.48 (8.86–11.91) , 0.001 9.29 (7.70–11.11) 8.18 (7.31–9.00) 0.02 hsCRP (mg/dl) a 0.16 (0.06–0.30) 0 .11 (0.06–0.25) 0.07 0.17 (0.06–0.30) 0.11 (0.06–0.24) 0.14 0.15 (0.06–0.42) 0.09 (0.06–0.26) 0.22 hsCRP, high sensitivity C-reactive protein; PCV, polypoidal choroidal vasculopathy Continuous variables are presented as median (interquartile range) a nd compared using the Mann-Whitney U test. aOnly 1 17 patients of PCV and 1 12 control subjects received examination o f the serum hsCRP level. doi:10.1371/journal.pone. 0110818.t002
alcohol consumption, conventional hyperhomocysteinemia (. 15mmol/L) is still significantly associated with PCV (OR, 64.55; 95% CI 9.79–567.73, p,0.001) in the multivariable logistic regression analysis.
In conclusion, our study showed hyperhomocysteinemia was significantly associated with PCV. The results also supported PCV might be related to arteriosclerosis. Further prospective controlled trials with large sample sizes are needed to improve our understanding of the role of hyperhomocysteinemia in PCV.
Supporting Information
Table S1 Proportions of hyperhomocysteinemia and
elevated C-reactive protein levels in overall patients and
different genders of patients with polypoidal choroidal vasculopathy and the control subjects.
(DOC)
Acknowledgments
The authors thank Ling-Chen Tai (Biostatistics Task Force and Division of General Surgery, Department of Surgery, Taipei-Veterans General Hospital) for help with statistical analysis.
Author Contributions
Conceived and designed the experiments: HCC JHL SML PKL. Performed the experiments: HCC JHL SML PKL. Analyzed the data: HCC JHL SML PKL. Contributed reagents/materials/analysis tools: HCC JHL SML PKL. Wrote the paper: HCC JHL SML PKL.
References
1. Yannuzzi LA, Sorenson J, Spaide RF, Lipson B (1990) Idiopathic polypoidal choroidal vasculopathy (IPCV). Retina 10: 1–8.
2. Yannuzzi LA, Wong DW, Sforzolini BS, Goldbaum M, Tang KC, et al. (1999) Polypoidal choroidal vasculopathy and neovascularized age-related macular degeneration. Arch Ophthalmol 117: 1503–1510.
3. Spaide RF, Yannuzzi LA, Slakter JS, Sorenson J, Orlach DA (1995) Indocyanine green videoangiography of idiopathic polypoidal choroidal vasculopathy. Retina 15: 100–110.
4. Liu Y, Wen F, Huang S, Luo G, Yan H, et al. (2007) Subtype lesions of neovascular age-related macular degeneration in Chinese patients. Graefes Arch Clin Exp Ophthalmol 245: 1441–1445.
5. Scassellati-Sforzolini B, Mariotti C, Bryan R, Yannuzzi LA, Giuliani M, et al. (2001) Polypoidal choroidal vasculopathy in Italy. Retina 21: 121–125. 6. Maruko I, Iida T, Saito M, Nagayama D, Saito K (2007) Clinical characteristics
of exudative agerelated macular degeneration in Japanese patients. Am -J Ophthalmol 144: 15–22.
7. Ciardella AP, Donsoff IM, Yannuzzi LA (2002) Polypoidal choroidal vasculo-pathy. Ophthalmol Clin North Am 15: 537–554.
8. Sho K, Takahashi K, Yamada H, Wada M, Nagai Y, et al. (2003) Polypoidal choroidal vasculopathy: incidence, demographic features, and clinical charac-teristics. Arch Ophthalmol 121: 1392–1396.
9. Laude A, Cackett PD, Vithana EN, Yeo IY, Wong D, et al. (2010) Polypoidal choroidal vasculopathy and neovascular age-related macular degeneration: same or different disease? Prog Retin Eye Res 29: 19–29.
10. Okubo A, Sameshima M, Uemura A, Kanda S, Ohba N (2002) Clinicopath-ological correlation of polypoidal choroidal vasculopathy revealed by ultrastruc-tural study. Br J Ophthalmol 86: 1093–1098.
11. Kuroiwa S, Tateiwa H, Hisatomi T, Ishibashi T, Yoshimura N (2004) Pathological features of surgically excised polypoidal choroidal vasculopathy membranes. Clin Experiment Ophthalmol 32: 297–302.
12. Nakashizuka H, Mitsumata M, Okisaka S, Shimada H, Kawamura A, et al. (2008) Clinicopathologic findings in polypoidal choroidal vasculopathy. Invest Ophthalmol Vis Sci 49: 4729–4737.
13. Clarke R, Daly L, Robinson K, Naughten E, Cahalane S, et al. (1991) Hyperhomocysteinemia: an independent risk factor for vascular disease. N Engl J Med 324: 1149–1155.
14. (2002) Homocysteine and risk of ischemic heart disease and stroke: a meta-analysis. JAMA 288: 2015–2022.
15. Seshadri S, Beiser A, Selhub J, Jacques PF, Rosenberg IH, et al. (2002) Plasma homocysteine as a risk factor for dementia and Alzheimer’s disease. N Engl J Med 346: 476–483.
16. Cahill MT, Stinnett SS, Fekrat S (2003) Meta-analysis of plasma homocysteine, serum folate, serum vitamin B(12), and thermolabile MTHFR genotype as risk factors for retinal vascular occlusive disease. Am J Ophthalmol 136: 1136–1150. 17. Aydemir O, Turkcuoglu P, Guler M, Celiker U, Ustundag B, et al. (2008) Plasma and vitreous homocysteine concentrations in patients with proliferative diabetic retinopathy. Retina 28: 741–743.
18. McGimpsey SJ, Woodside JV, Cardwell C, Cahill M, Chakravarthy U (2009) Homocysteine, methylenetetrahydrofolate reductase C677T polymorphism, and risk of retinal vein occlusion: a meta-analysis. Ophthalmology 116: 1778–1787 e1771.
19. Turgut B, Kaya M, Arslan S, Demir T, Guler M, et al. (2010) Levels of circulating homocysteine, vitamin B6, vitamin B12, and folate in different types of open-angle glaucoma. Clin Interv Aging 5: 133–139.
20. Wu KH, Tan AG, Rochtchina E, Favaloro EJ, Williams A, et al. (2007) Circulating inflammatory markers and hemostatic factors in age-related maculopathy: a population-based case-control study. Invest Ophthalmol Vis Sci 48: 1983–1988.
21. Rochtchina E, Wang JJ, Flood VM, Mitchell P (2007) Elevated serum homocysteine, low serum vitamin B12, folate, and age-related macular degeneration: the Blue Mountains Eye Study. Am J Ophthalmol 143: 344–346. 22. Ridker PM (2001) High-sensitivity C-reactive protein: potential adjunct for global risk assessment in the primary prevention of cardiovascular disease. Circulation 103: 1813–1818.
23. Kikuchi M, Nakamura M, Ishikawa K, Suzuki T, Nishihara H, et al. (2007) Elevated C-reactive protein levels in patients with polypoidal choroidal
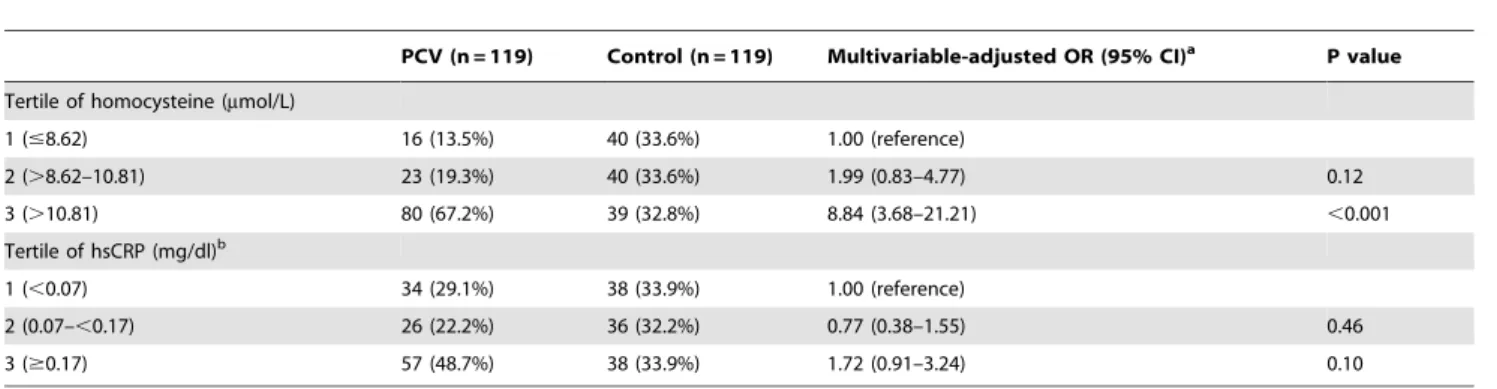
Table 3. Distribution of polypoidal choroidal vasculopathy cases and controls within tertiles of homocysteine and C-reactive protein levels.
PCV (n = 119) Control (n = 119) Multivariable-adjusted OR (95% CI)a P value
Tertile of homocysteine (mmol/L)
1 (#8.62) 16 (13.5%) 40 (33.6%) 1.00 (reference) 2 (.8.62–10.81) 23 (19.3%) 40 (33.6%) 1.99 (0.83–4.77) 0.12 3 (.10.81) 80 (67.2%) 39 (32.8%) 8.84 (3.68–21.21) ,0.001 Tertile of hsCRP (mg/dl)b 1 (,0.07) 34 (29.1%) 38 (33.9%) 1.00 (reference) 2 (0.07–,0.17) 26 (22.2%) 36 (32.2%) 0.77 (0.38–1.55) 0.46 3 ($0.17) 57 (48.7%) 38 (33.9%) 1.72 (0.91–3.24) 0.10
CI, confidence interval; hsCRP, high sensitivity C-reactive protein; OR, odds ratio; PCV, polypoidal choroidal vasculopathy Categorical variables were presented as numbers (percentage).
a
Adjusted for age, gender, hypertension, diabetes mellitus, coronary artery disease, cerebrovascular event, smoking and alcohol consumption. b
Only 117 patients of PCV and 112 control subjects received examination of the serum hsCRP level. doi:10.1371/journal.pone.0110818.t003
vasculopathy and patients with neovascular age-related macular degeneration. Ophthalmology 114: 1722–1727.
24. Refsum H, Smith AD, Ueland PM, Nexo E, Clarke R, et al. (2004) Facts and recommendations about total homocysteine determinations: an expert opinion. Clin Chem 50: 3–32.
25. (2005) Dose-dependent effects of folic acid on blood concentrations of homocysteine: a meta-analysis of the randomized trials. Am J Clin Nutr 82: 806–812.
26. (2005) [Criteria for diagnosis of polypoidal choroidal vasculopathy]. Nippon Ganka Gakkai Zasshi 109: 417–427.
27. Cackett P, Wong D, Yeo I (2009) A classification system for polypoidal choroidal vasculopathy. Retina 29: 187–191.
28. Tewari PC, Zhang B, Bluestein BI (2004) Analytical and clinical evaluation of the Bayer ADVIA Centaur homocysteine assay. Clin Chim Acta 342: 171–178. 29. Ng MK, Liu PY, Williams AJ, Nakhla S, Ly LP, et al. (2002) Prospective study of effect of androgens on serum inflammatory markers in men. Arterioscler Thromb Vasc Biol 22: 1136–1141.
30. Ross RD, Gitter KA, Cohen G, Schomaker KS (1996) Idiopathic polypoidal choroidal vasculopathy associated with retinal arterial macroaneurysm and hypertensive retinopathy. Retina 16: 105–111.
31. Nakajima M, Yuzawa M, Shimada H, Mori R (2004) Correlation between indocyanine green angiographic findings and histopathology of polypoidal choroidal vasculopathy. Jpn J Ophthalmol 48: 249–255.
32. McCully KS (2009) Chemical pathology of homocysteine. IV. Excitotoxicity, oxidative stress, endothelial dysfunction, and inflammation. Ann Clin Lab Sci 39: 219–232.
33. Kondo N, Honda S, Ishibashi K, Tsukahara Y, Negi A (2008) Elastin gene polymorphisms in neovascular age-related macular degeneration and polypoidal choroidal vasculopathy. Invest Ophthalmol Vis Sci 49: 1101–1105.
34. Karnik SK, Brooke BS, Bayes-Genis A, Sorensen L, Wythe JD, et al. (2003) A critical role for elastin signaling in vascular morphogenesis and disease. Development 130: 411–423.
35. Hoh BL, Rabinov JD, Pryor JC, Ogilvy CS (2004) A modified technique for using elastase to create saccular aneurysms in animals that histologically and hemodynamically resemble aneurysms in human. Acta Neurochir (Wien) 146: 705–711.
36. Russo GT, Friso S, Jacques PF, Rogers G, Cucinotta D, et al. (2003) Age and gender affect the relation between methylenetetrahydrofolate reductase C677T genotype and fasting plasma homocysteine concentrations in the Framingham Offspring Study Cohort. J Nutr 133: 3416–3421.
37. Rosa RH, Jr., Davis JL, Eifrig CW (2002) Clinicopathologic reports, case reports, and small case series: clinicopathologic correlation of idiopathic polypoidal choroidal vasculopathy. Arch Ophthalmol 120: 502–508.