Development of Sustained Attention Assessed Using
the Continuous Performance Test among Children
6-15 Years of Age
Chaucer C. H. Lin,
1,2Chuhsing K. Hsiao,
1and Wei J. Chen
1,3Received October 13, 1998; revision received April 13, 1999; accepted April 15, 1999
The Continuous Performance Test (CPT) is a widely used measure of sustained attention, which may rely on the efficiency of cognitive inhibition. We examined the relationships of age and sex with CPT performance among 341 randomly selected school children 6-15 years of age. Multiple regression analyses revealed that the hit rate, false alarm rate, and sensitivity of both the undegraded and the degraded CPT were associated with age by a quadratic relationship. The age-development curves for the hit rate and sensitivity were convex, whereas that for the false alarm rate was concave. Sex was associated with the hit rate and sensitivity on the degraded CPT only. Our findings are consistent with the hypothesis that sustained attention develops during the primary school ages. The data reported are essential for identifying children with conditions associated with sustained attention deficit, such as attention-deficit hyperactivity disorder, as well as those at an increased risk for developing schizophrenia.
The Continuous Performance Test (CPT; Rosvold, Mirsky, Sarason, Bransome, & Beck, 1956) has been widely used as a measure of sustained attention deficits in children with attention-deficit hyperactivity disorder (ADHD; Chee, Logan, Schachar, Lindsay, & Wachsmuth,
1989; Hooks, Milich, & Lorch, 1994; Seidel & Joschko, 1990) and those at high risk for schizophrenia (Cornblatt & Erlenmeyer-Kimling, 1985; Nuechterlein, 1983; Rutschmann, Cornblatt, & Erlenmeyer-Kimling, 1977). The CPT requires participants to respond to predesignated targets among stimuli that are presented at a rapid fixed rate. The discrimination vigilance task of the CPT may consist of a single stimulus (CPT-X, single character or number as the target) or two successive stimuli (CPT-AX, a character or number preceded by another charac-ter or number as the target). The difficulty level of the 1 Institute of Epidemiology, College of Public Health, National Taiwan
University, Taipei, Taiwan.
2Taipei City Psychiatric Center, Taipei, Taiwan.
3 Address all correspondence to Wei J. Chen, Institute of Epidemiology,
College of Public Health, National Taiwan University, Room 1545, 1 Jen-Ai Road, Sec. 1, Taipei 100, Taiwan. E-mail: weijen@ha.mc.ntu. edu.tw.
CPT can be raised further by blurring the stimuli (de-graded CPT; Nuechterlein, 1983) or using a relative tar-get (CPT-identical version or CPT-IP; Cornblatt, Risch, Paris, Friedman, & Erlenmeyer-Kimling, 1988).
CPT performance depends on the task variables of the test and the indexes used. The performance indexes of the CPT have evolved from the hit rate or the false alarm rate alone to indexes derived from signal detection theory (sensitivity and response criterion; Swets, 1973). The commonality of sensitivity and response criterion in-dexes across different CPT versions is supported by the results of the principal component analysis and the fact that the hit rate of conventional CPT correlates moder-ately with that of the degraded CPT (Nuechterlein, 1983). Earlier studies emphasized that a decrease in sensitivity over time was the clearest index for sustained attention deficit (Davies & Parasuraman, 1982). Thus, the CPT usually requires a long duration. However, many studies detected sustained attention deficit in children with ADHD and children of schizophrenic mothers on the basis of in-dexes of overall vigilance performance, especially signal detection indexes, with tests conducted in a relatively short period of time.
403
009l-0627/99/1000-0403$16.00/0 © 1999 Plenum Publishing Corporation
Corkum and Siegel (1993) noted that only about half of CPT studies comparing children with ADHD and nor-mal controls reported significant differences in the tradi-tional indexes of the CPT; that is, omission errors (Horn, Wagner, & Ialongo, 1989; O'Dougherty & Nuechterlein, 1984; Sykes, Douglas, & Morgenstern, 1973; Sykes, Douglas, Weiss, & Minde, 1971) and commission errors (Horn et al., 1989; O'Dougherty & Nuechterlein, 1984; Shapiro & Garfinkel, 1986; Sykes et al., 1971). Of four studies reporting signal detection indexes, however, three found that children with ADHD have a significantly lower sensitivity (d') than controls (O'Dougherty &
Nuechterlein, 1984; Sostek, Buchsbaum, & Rapoport, 1980; Tarnowski, Prinz, & Nay, 1986). The only study reporting significant differences between children with ADHD and children who are normal for all indexes was one that applied the degraded CPT (O'Dougherty & Nuechterlein, 1984). Nevertheless, when the results of 26 studies were put together in a meta-analysis, children with ADHD were found to perform significantly worse than normal controls on the CPT in terms of both com-mission and ocom-mission errors as well as signal-detection indexes (Losier, McGrath, & Klein, 1996). For individual studies, however, CPT versions with excessive demand on attention, short display time, and relatively short in-terstimuli intervals could best differentiate children with ADHD from children who do not have ADHD (Corkum & Siegei, 1993).
Studies using the CPT-X or CPT-AX did not find significant differences between children of schizophrenic mothers and children of normal mothers (Asarnow, Steffy, MacCrimmon, & Cleghorn, 1977; Cohler, Grunebaum, Weiss, Gamer, & Gallant, 1977; Cornblatt & Erlenmeyer-Kimling, 1984; Herman, Mirsky, Ricks, & Gallant, 1977); only studies using the degraded CPT or CPT-IP could de-tect sustained attention deficits in the children of schizoph-renic mothers (Cornblatt & Erlenmeyer-Kimling, 1985; Nuechterlein, Parasuraman, & Jiang, 1983; Rutschmann et al., 1977). However, CPT versions with short (2-5 min) sessions can reveal perceptual sensitivity deficits in chil-dren of schizophrenic mothers if the stimuli are highly degraded (Nuechterlein, 1983).
CPT deficits in schizophrenia patients or those who are at higher risk for schizophrenia strongly suggest that brain abnormalities underlie attentional dysfunctions in schizophrenia. Positron emission tomography (PET) stud-ies of the CPT reported by Buchsbaum et al. (1990) have shown that performance of this task activates the frontal lobes, and schizophrenia patients showed decreased meta-bolic activity in the prefrontal cortex and a reduction of normally lateralized activity in the temporoparietal region, as compared with nonschizophrenic people. More recent
PET studies also suggested that patients with schizophre-nia have patterns of brain blood flow abnormalities that are consistent with difficulty in focusing attention, which might reflect the functional substrata of the anatomic ab-normalities (Andreasen, Swazye, O'Leary, & Nopoulos, 1995). The sustained attention deficits measured by the CPT was considered a facet of cognitive inhibition (Lencz, Raine, Benishay, Mills, & Bird, 1995). The dysfunction of cognitive inhibition has been postulated to explain symp-toms of schizophrenia (Braff, 1993) and schizotypy (Beech & Claridge, 1987). The efficiency of cognitive in-hibition was also hypothesized to change with age during childhood and hence leads to developmental changes on performance of neuropsychological tests (Harnishfeger & Pope, 1996), such as the CPT.
The effect of age on CPT performance has been demonstrated in both nonclinical children (Greenberg & Waldman, 1993; Levy, 1980; Seidel & Joschko, 1990) and children with ADHD (O'Dougherty & Nuechterlein, 1984; Seidel & Joschko, 1990). A nonlinear developmen-tal trend of CPT performance was noted by Levy (1980) and Greenberg and Waldman (1993). The effect of age was also noted on the brain potential components during the CPT (Friedman, Boltri, Vaughan, & Erlenmeyer-Kimling, 1985). The rapid developmental changes in sustained at-tention among children present difficulty in interpreting CPT performance. A well-established age norm for CPT performance is thus essential for classifying children as having sustained attention deficits. Although several stud-ies have reported CPT performance indexes in nonclinical children, their utility was limited because the study sam-ples were small (Halperin et al., 1988; Seidel & Joschko, 1990), were composed of only boys (Halperin, Sharma, Greenblatt, & Schwartz, 1991), included a re-stricted age range (Mirsky, Anthony, Duncan, Ahearn, & Kellam, 1991), or had unsatisfactory test completion rates (Levy, 1980). Only Greenberg and Waldman's study (1993) of 775 children, aged 6-16 years, was ideal in de-scribing CPT normal values for children. However, the stimuli used in that study were two easily discriminated visual shapes with one of them designated as the target, which was different from the CPT versions used in many previous studies.
Our previous study (Chen, Hsiao, Hsiao, & Hwu, 1998) found that the undegraded CPT '1-9' results of adults were comparable with results of other studies. Thus, it is worthwhile to establish a norm for that version of CPT in children. In our previous study of 345 adults and 115 junior high school students (Chen, Hsiao et al., 1998), we found a decline in CPT performance with age and a better performance on CPT for men than for women in the adult sample. However, such relationships between CPT
performance and age as well as gender were not noted in the student sample, probably because of the limited age range (13-15 years-old). Based on the results of previous studies (Greenberg & Waldman, 1993; Levy, 1980) and our previous adult sample, we hypothesized that CPT per-formance might develop with age in a nonlinear fashion that reaches a plateau around adolescence. In this study, we expanded the student sample to include 233 primary school students 6-13 years of age and investigated the effects of age and gender on CPT performance in the en-larged sample. Two versions of the CPT, the undegraded 1-9 task and the 25% degraded 1-9 task, were adminis-tered. Both conventional indexes and indexes derived from signal detection theory of the CPT, as well as the relation-ship between these indexes and demographic features, are reported.
METHOD
Participants
The study group was composed of primary (aged 6-13 years) and junior high (aged 6-13-15 years) school stu-dents sampled from two schools in Chinshan Township, which is a 60 min drive north of Taipei, Taiwan. The pop-ulation of the township was about 18,000 in 1993, For the junior high school students, 118 were sampled randomly from the 1,178 students enrolled in the Chinshan Junior High School in 1994. The selection criteria and results on the degraded and undegraded CPT were previously de-scribed (Chen, Hsiao et al., 1998). Among the participants, 3 failed to complete the test (1 due to absence and 2 due to transfer to other schools). Thus, only 115 junior high school students were included in this study.
To evaluate the developmental trend of CPT per-formance in children, we expanded the student sample by recruiting primary school children in the next year. A systematic sampling procedure was carried out using 1995 student lists from all classes of the Chinmei Pri-mary School, which was randomly selected from four of its kind in the township. One out of every 3 students from each of 22 classes was selected. We thus sampled 251 of the 749 students. Among the sampled students, 11 (5 from the first grade, 2 from the second grade, 3 from the third grade, and 1 from the fourth grade) refused to participate in the study, and 7 (1 from the first grade, 1 from the sec-ond grade, 2 from the third grade, 1 from the fourth grade, and 2 from the fifth grade) had transferred to other schools by the time of data collection. The remaining 233 students completed the tests. Data of both sessions of the CPT for 6 students (2 in the second grade and 4 in the third grade) and that of the degraded session for 1 student (in the third
grade) were lost in the data-managing process. Thus, there were 226 primary school students with complete data. In all, there were 341 students (167 boys and 174 girls), aged 6-15 years, in the present study. No students in this study were screened for specific psychopathology. Taiwanese was these students' native tongue but Mandarin was the official language used in the schools. In addition, students began learning mathematics with Arabic numbers in their first year in the primary school, so they were able to work with Arabic numbers well.
Test Procedures
All children participating in this study completed two CPT sessions (the undegraded followed by the degraded test). Tests were conducted in the health care room at the schools, after a written informed consent form signed by the student and one of his or her parents was obtained. We used a CPT machine from Sunrise Systems (model version 2.20, Pembroke, MA). The testing procedure has been described in detail elsewhere (Chen, Hsiao, et al., 1998; Chen, Hsiao, & Lin, 1997). Briefly, numbers from 0 to 9 were randomly presented for 50 ms each, at a rate of one per second. The probability of critical stimulus was set at 10%. Each student undertook two CPT sessions; the un-degraded 1-9 task and the un-degraded 1-9 task. During the undegraded session, students responded to the target stim-ulus (the number 9 preceded by the number 1) by pressing a button. A total of 341 trials, 31 of them targets, were presented over a period of 5 min. During the degraded session, a pattern of snow was used to toggle background and foreground dots so that the image was not distinct. The further stimulus encoding and analysis processes of the de-graded CPT demand a substantial allocation of attentional capacity (Nuechterlein, 1983). Standardized instructions were given in Mandarin before the test to make sure that the students understood the rules. The undegraded session was administered first and then the degraded session. Each session of the test began with 2 min of practice (repeated if students required). The rater, who sat or stood at an oblique angle to the student, could monitor the student's perfor-mance through a computer monitor and make sure that the student knew how to press the button correctly. Once a test began, no rewards or cues were given to the student.
The signal-detection indexes of CPT performance were derived from the hit rate (rate of response to target trials) and false alarm rate (rate of response to nontarget trials; Nuechterlein, 1991; Swets, 1973). The sensitivity index (d') reflects the degree to which the frequency dis-tribution of the internal perceptual evidence generated by signal trials is separated from that generated by nonsignal or noise trials, whereas the response criterion index (In t)
assesses the amount of perceptual evidence an individual requires prior to making a decision to respond to a stimu-lus as a signal. The d' was calculated as z(h) — z(f), where z denotes the normal deviate, h denotes the hit rate, and / denotes the false alarm rate. In cases where the hit rate was 100% or the false alarm rate was 0%, h and f were calculated as 2-1/s and 1 — 2- 1 / n, where 5 denotes num-ber of target trials and n denotes the numnum-ber of nontarget trials (Davies & Parasuraman, 1982). The In t was calcu-lated as In{y[z(h)]/y[z(f)]}, where y is the ordinate of the normal distribution. Variables extraneous to the intended comparison (d1), such as differences in motivation or in
cooperativeness between the groups, would yield differ-ences in the response criterion rather than in d'.
RESULTS
All analyses were performed with the SAS computer package (SAS Institute, 1989). The univariate procedure was used to describe the general distribution of these data. The effects of sex and age on CPT performance indexes were initially assessed by a multivariate analysis of vari-ance (MANOVA) in order to reduce Type I error. A uni-variate two-way analysis of variance (ANOVA) was then performed. The relationships between age and the CPT performance indexes were first plotted and then investi-gated further with multiple regression. The log-likelihood ratio test was used to select the model that best fit the data. A p value of less than .05 was considered significant.
Among the 341 children, 167 (49%) were boys and 174 (51%) were girls. The distributions of the CPT perfor-mance indexes of both the undegraded and degraded ses-sions by age are shown in Table I. For both the undegraded
and degraded CPT, the hit rate and d' increased with age, whereas the false alarm rate decreased with age. The re-sponse criteria of both sessions showed no obvious trend with age. The main effect of age in a MANOVA was highly significant, F(9, 321) = 42.16, p < 0.01, and that of sex was of marginal significance, F(8, 314) = 1.79, p = 0.08. The following two-way ANOVAs revealed that age influenced all CPT performance indexes except In t on the undegraded CPT, F(9, 330) = 1.84, p = 0.06. Sex had no significant influence on any of the undergraded CPT indexes, but had a significant effect on the hit rate, F(l, 330) = 6.25, p = 0.01, and d', F(1, 330) = 3.97, p = 0.05, of the degraded test.
We then regressed individual CPT performance in-dexes on age (coded as continuous) and sex (coded as 0 for boys and 1 for girls) to assess the linear effects of these variables. Similar to the results of the ANOVAs, age had significant effects on the hit rate, false alarm rate, and d' of both sessions and In t of the degraded session (all ps < 0.05; Table II). Sex also had a significant effect on the hit rate and d' of the degraded CPT. All the R2s of the total
model for each fitted model were significantly greater than zero (Table II). The partial R2s of sex in the models of hit
rate and d' of the undegraded CPT and false alarm rate and In ft of both CPT versions were very small (ranging from 0.000 to 0.002) and not significant, except for that in the models of hit rate (0.02), F(2, 338) = 10.62, p < 0.01, and d' (0.02), F(2, 338) = 9.64, p < 0.01, of the degraded CPT, which were significant. Given the small values of the partial R2s of sex, the partial R2s of age
in these models were very close to the R2s of the total
model and were all significant. The effect estimates and the log likelihood of each model are also presented in Table II.
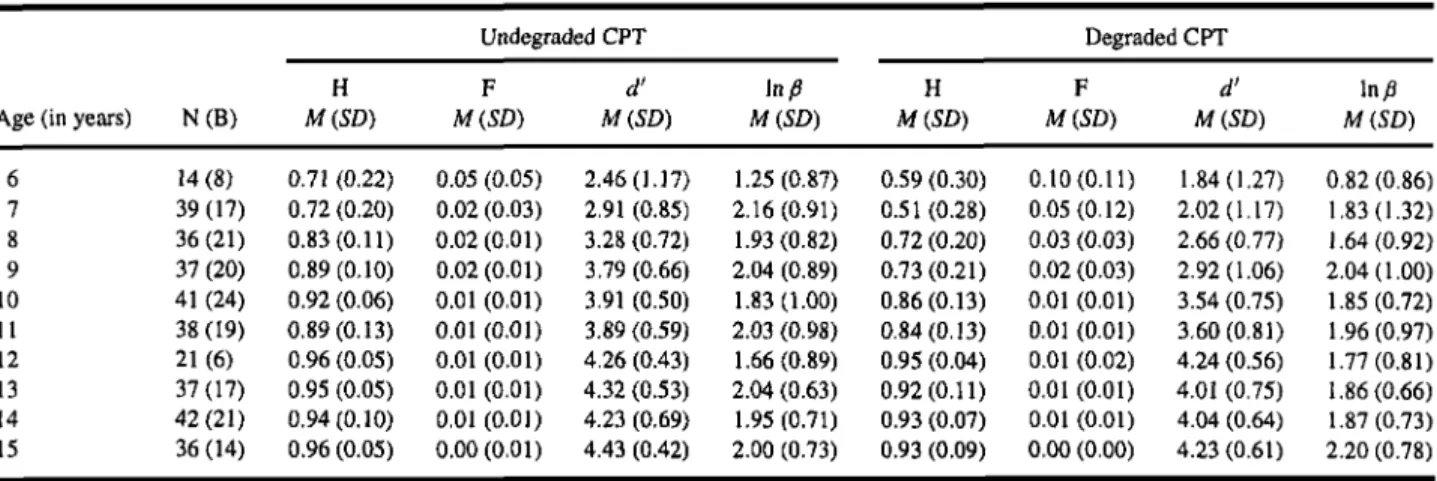
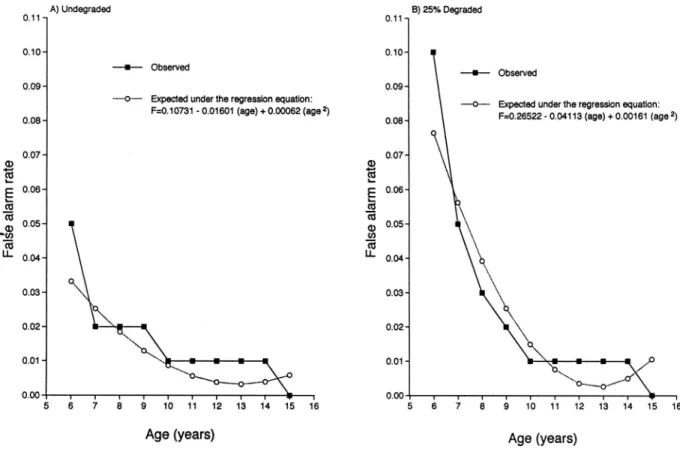
Table I. Means (and Standard Deviations) of CPT Indexes in Children of Different Ages Undegraded CPT
Age (in years)
6 7 8 9 10 11 12 13 14 15 N(B) 14(8) 39(17) 36(21) 37 (20) 41 (24) 38(19) 21(6) 37(17) 42(21) 36 (14) H M(SD) 0.71 (0.22) 0.72 (0.20) 0.83(0.11) 0.89(0.10) 0.92 (0.06) 0.89(0.13) 0.96 (0.05) 0.95 (0.05) 0.94(0.10) 0.96 (0.05) F M(SD) 0.05 (0.05) 0.02 (0.03) 0.02(0.01) 0.02 (0.01) 0.01 (0.01) 0.01 (0.01) 0.01 (0.01) 0.01 (0.01) 0.01 (0.01) 0.00(0.01)
d'
M (SD) 2.46(1.17) 2.91 (0.85) 3.28 (0.72) 3.79 (0.66) 3.91 (0.50) 3.89 (0.59) 4.26 (0.43) 4.32 (0.53) 4.23 (0.69) 4.43 (0.42) In b M (SD) 1.25(0.87) 2.16(0.91) 1.93(0.82) 2.04 (0.89) 1.83(1.00) 2.03 (0.98) 1.66(0.89) 2.04 (0.63) 1.95 (0.71) 2.00 (0.73) Degraded CPT H M (SD) 0.59 (0.30) 0.51(0.28) 0.72 (0.20) 0.73(0.21) 0.86(0.13) 0.84(0.13) 0.95 (0.04) 0.92(0.11) 0.93 (0.07) 0.93 (0.09) F M (SD) 0.10(0.11) 0.05(0.12) 0.03 (0.03) 0.02 (0.03) 0.01 (0.01) 0.01 (0.01) 0.01 (0.02) 0.01 (0.01) 0.01 (0.01) 0.00 (0.00)d'
M (SD) 1.84(1.27) 2.02(1.17) 2.66 (0.77) 2.92(1.06) 3.54 (0.75) 3.60(0.81) 4.24 (0.56) 4.01 (0.75) 4.04 (0.64) 4.23 (0.61) In b M (SD) 0.82 (0.86) 1.83(1.32) 1.64(0.92) 2.04(1.00) 1.85(0.72) 1.96(0.97) 1.77(0.81) 1.86(0.66) 1.87(0.73) 2.20 (0.78)Note. CPT = Continuous Performance Test; N = number of participants; B = number of boys; H = hit rate; F = false alarm rate; d' = sensitivity;
Fig. 1. Observed and expected age distributions of the hit rates on the undegraded (A) and degraded (B) Continuous Performance Test (CPT) in 341 nonclinical children. Curves of expected data from the degraded CPT are plotted for both sexes separately.
Because the pattern of relationships between these indexes (including the hit rate, sensitivity, and the false alarm rate) and age revealed a possible nonlinear rela-tionship (the solid lines in Figs. 1-3), a quadratic term of age was added to the regression models (called quadratic model hereafter) for further analysis. Age and quadratic
age remained in all the models except that for the In y. For the hit rate and d' in the degraded CPT, sex remained in the models in addition to age and quadratic age (Table II). All the R2s of the total model for each fitted model were
significantly greater than zero (Table II). The partial
R2s of quadratic age was 0.04 for d', F(2, 338) = 25.2,
Table II. Regression Coefficients (Standard Errors), Total Model R2s, and Model Selecting Indexes for Hit Rate, False Alarm Rate, and Sensitivity
in the Undegraded and Degraded CPT
Undegraded CPT Model Linear model Age Sex LL() R2 Quadratic mode) Age Sex Age2 LL1 R2 L R T ( x 2 , d f , p ) H 0.025 (0.002) — 721 0.25 (F(1, 339) = 115.1)* 0.132(0.020) — -0.005 (0.001) 734 0.31 (F<2, 338) = 75.5)* 26, 1, <0.00l F(x10-2) -0.258 (0.035) — 1,366 0.13 (F (1,339) = 52.2)* -1.606 (0.314) — 0.062 (0.014) 1,375 0.18(F(2, 338) = 36.7)* 18. 1. <0.001 d1 0.185(0.013) — 132 0.36 (F (1,339) =192.5)* 0.764 (0.116) — -0.027 (0.005) 145 0.41 (F (2.338)= 115.7)* 26, 1, <0.001 Degraded CPT H 0.046 (0.004) -0.064 (0.020) 582 0.34 (F(2, 338) = 86.7)* 0.195 (0.031) -0.061 (0.019) -0.007 (0.001) 593 0.38 (F (3, 337) = 69.2)* 22, 1, <0.001 F(xl0- 2) -0.634(0.101) — 1,014 0.11(F(1, 339) = 39.8)* -4.113 (0.887) — 0.161(0.041) 1,022 0.14 (F(2. 338) = 28.5)* 16. 1. <0.001 d1 0.272 (0.017) -0.286 (0.094) 49 0.43 (F(2. 338) = 128.5)* 0.098 (0.149) -0.270(0.091) -0.033 (0.007) 60 0.47 (F (3. 337) = 98.7)* 22, 1, <0.001
Note. CPT = Continuous Performance Test; LLn = log likelihood of the model n; LRT = -2LL0 + 2LL1 . Em-dashes indicate that the variable was not in the model. All regression coefficients listed
arc significant at 0.05 level. *p <0.01.
Fig. 2. Observed and expected age distributions of sensitivity on the undegraded (A) and degraded (B) Continuous Performance Test (CPT) in 341 nonclinical children. Curves of expected data from the degraded CPT are plotted for both sexes separately.
p < 0.01; 0.06 for hit rate, F(2, 338) = 27.0, p < 0.01; and 0.05 for false alarm rate, F(2, 338) = 18.6, p < 0.01, of the undegraded CPT and 0.04 for d', F(3, 337) = 23.2, p < 0.01; 0.04 for hit rate, F(3, 337) = 23.4, p < 0.01; and 0.04 for false alarm rate, F(2, 338) = 15.6, p < 0.01, of the degraded CPT. The partial R2s of sex for hit rate and d' of the degraded CPT was 0.02, F(3, 337) = 10.13, p < 0.01, and 0.01, F(3, 337) = 8.75, p < 0.01, respectively. Given the small values of the partial R2s of sex and quadratic age, the partial R2s of age in these
mod-els were very close to the R2s of the total model and were
all significant. The effect estimates and the log likelihood of each model are also presented in Table II.
Comparing the quadratic models with the linear mod-els, the log-likelihood ratio test (LRT) revealed that the quadratic models fit the data better. For the hit rate and d', the coefficients of the quadratic terms in the models were negative, indicating that these two indexes increased with age initially but would reach a maximum later (the dot-ted lines in Figs. 1 and 2). By letting the derivative of the quadratic regression equations equal zero, we calculated that the values of the hit rate and d' on the undegraded CPT
would reach a maximum at 13.2 and 14.1 years of age, respectively, whereas those of the degraded test would reach a maximum value at 13.9 and 14.7 years of age, respectively. For the false alarm rate, coefficients of the quadratic term in the models were positive, indicating that the false alarm rate decreased with age initially and would reach a minimum later (the dotted lines in Fig. 3); the age at which the false alarm rate would reach the minimum was calculated as 13.0 years for the undegraded CPT and 12.8 years for the degraded CPT. Because we coded girls as 1 and boys as 0 in our analyses, the significant negative coefficients of sex in the models of hit rate and d' on the degraded CPT indicated that girls had worse performance than boys on these two indexes.
DISCUSSION
There are several features of this study that make it more appropriate than previous studies for providing normative data for CPT performance in children. First, the sample had sufficient numbers of children (36 to 42)
Fig. 3. Observed and expected age distributions of the false alarm rates on the undegraded (A) and degraded (B) Continuous Performance Test in 341 nonclinical children.
in all age groups except the 6-year-old and 12-year-old groups (14 and 21, respectively). The numbers of boys and girls were balanced in most of the age levels. The reported indexes included traditional ones (the hit rate and the false alarm rate) and those derived from signal detection theory (sensitivity and response criterion). These data provided an opportunity to examine the developmental changes of performance on CPTs of different difficulty levels and the effects of age and sex on the performance.
Our finding that CPT performance improves with age, especially in the age range of 6 to 12 years, is con-sistent with the hypothesis that cognitive inhibition deve-lops during the primary school years (Bjorklund & Harnishfeger, 1990). In particular, the trends of increasing hit rate and d' with age were similar to those reported by Seidel and Joschko (1990) and O'Dougherty and Nuechterlein (1984), despite the differences in the task variables used in these studies. Cross-study comparabil-ity was noted for the undegraded CPT by comparing the data in this study with those from studies using different versions. For example, Chee et al. (1989) reported a hit rate of 0.91 and a false alarm rate of 0.013 on the unde-graded CPT-X (display time = 200 ms) for 36 control
children (mean age = 8.5 years), which were similar to the values of the 37 9-year-old children in our study (hit rate = 0.89 and false alarm rate = 0.02). The slight, though not significant, decrease in hit rate and increase in false alarm rate in our data might be due to the memory load of the CPT 1-9 and the shorter display time (50 ms in this study).
With sufficient numbers of children in each age level, we further applied multiple regression to investigate the relationships between age and these indexes, which have seldom been reported. In investigating the nonlinear re-lationship between age and these CPT indexes, we de-cided to use the quadratic polynomial model for data fit-ting rather than the exponential models applied by Levy (1980). The main reason for our choice was that an ex-ponential model would not be consistent with the trends of these indexes among adults; in a previous study (Chen, Hsiao et al., 1998) we found that the hit rate and d' de-creased with age, whereas the false alarm rate inde-creased with age in adults.
The results of multiple regression analysis indicated that there was indeed a nonlinear relationship, that is, a quadratic term, between age and CPT performance indexes
except for the response criterion. This was consistent with the results of Greenberg and Waldman (1993), in which the performance on a two-shape version of the CPT de-veloped in a nonlinear manner, changing rapidly in early childhood and leveling off during late childhood and ado-lescence. On the basis of the predicted convex curves, the hit rate and sensitivity would reach their maximum values at somewhat higher ages for the degraded session than for the undegraded session, which indicates that the ability to sustain attention in the degraded session may need more time to mature. Because there are no data available on CPT performance of children aged 16 to 19 years, the validity of these predictions can only be assessed by showing that CPT performance of young adults is poorer than that of 15-year-old children: Among a community sample of 345 adults, aged 20 to 65 years, we found that the means (SDs) of these indexes for the 20- to 24-year-old age group were 0.94 (0.11) for the hit rate and 4.45 (0.56) for sensitiv-ity in the undegraded session, and 0.86 (0.13) and 3.77 (0.83) in the degraded session (Chen, Hsiao et al., 1998). These values further decreased in the 25- to 29-year-old age group to 0.90 (0.14), 4.20 (0.90), 0.83 (0.19), and 3.65 (1.00), respectively. Results of multiple regression among these adults also showed that the hit rate and d' decreased as age increased. Taken together, the results are consistent with the prediction of a convex curve for the age-related changes in the hit rate and d' of the CPT. Similarly, the trend of the false alarm rate increasing with age among adults (Chen, Hsiao et al., 1998) is consistent with the prediction of a concave curve for the age-related changes in the false alarm rate.
The significant relationship between age and false alarm rate noted on multiple regression analysis is consis-tent with the results of Levy (1980) and O'Dougherty and Nuechterlein (1984). However, Seidel and Joschko (1990) reported that the effect of age on the false alarm rate was nonsignificant. Nevertheless, their analyses revealed that younger children had a higher false alarm rate in a pro-longed 15-min CPT. The inconsistency of the effect of age on the false alarm rate cannot be easily explained by the sample size, age of children, or CPT versions used. Because the commission errors reported in these reports may be a mixture of different error types, reflecting either impulsivity or inattention (Halperin et al., 1988), more specifically defined indexes are needed to assess the dif-ferent deficits and their relationships to age.
The results of this study indicate that, in addition to age, sex is also associated with performance on the de-graded CPT. Girls had a worse performance than boys in the hit rate and sensitivity of the degraded CPT, which is consistent with the results of our previous adult sam-ple (Chen, Hsiao et al., 1998). However, previous studies
reported either no gender differences in CPT perform-ance (Levy, 1980; Seidel and Joschko, 1990) or that boys made more omission and commission errors than girls (Greenberg & Waldman, 1993). The inconsistency might be due to the use of different versions of the CPT. Our re-sults from both adult and child samples indicate that a gen-der difference in signal discrimination during vigilance can be demonstrated only when processing demands are increased. These findings were consistent with the similar gender differences in brain potential components during CPT (Friedman et al., 1985). The gender difference noted might be related to differences in processing strategies, physiological differences during cognitive activity shown by studies of cerebral blood flow (Gur et al., 1982), en-docrinological differences (MacLusky & Naftolin, 1981), or even physical differences. Further research is warranted to clarify these possible factors for gender differences in CPT performance. Until then, gender of participants should not be ignored in interpreting the degraded CPT performance.
The age-specific distributions of the CPT perfor-mance indexes obtained in this study should make it pos-sible for us to choose a suitable threshold for classifying a child's performance as normal or deficit. However, the task is complicated by the fact that some of the degraded indexes are affected further by sex. Thus, to classify a child as having deficits in these CPT performance indexes or to compare these indexes among distinct groups of children, a method of standardization with adjustment for age and sex (Chen, Liu et al., 1998; Saykin et al., 1991) should be applied. The data presented in this article are valuable for this purpose.
ACKNOWLEDGMENTS
This work was supported by research grants from the National Science Council, Taiwan (NSC83-0412-B-002-310, NSC84-2331-B-002-187, and NSC85-2332-B-002-269). We acknowledge the assistance of Li-Ling Hsiao and Yu-Hei Chang in administrating the CPT. We also thank teachers and staff of the health care rooms at Chinshan Junior High School and Chinmei Primary School for their help in providing us with a facility for conducting the tests.
REFERENCES
Andreasen, N. C., Swazye, V., O'Leary, D. S., & Nopoulos, P. (1995). Abnormalities in midline attentional circuitry in schizophrenia: Evi-dence from magnetic resonance and positron emission tomography.
Asarnow, R. F., Steffy, R. A., MacCrimmon, D. J., & Cleghorn, J. M. (1977). An attentional assessment of foster children at risk for schizophrenia. Journal of Abnormal Psychology, 86, 267-275. Beech, A., & Claridge, G. (1987). Individual differences in negative
priming: Relations with schizotypal personality traits. British
Jour-nal of Psychology, 78, 349-356.
Bjorklund, D. F., & Harnishfeger, K. K. (1990). The resources construct in cognitive development: Diverse sources of evidence and a theory of inefficient inhibition [Special Issue: Limited resource models of cognitive development]. Developmental Review, 10, 48-71. Braff, D. L. (1993). Information processing and attention dysfunctions
of schizophrenia. Schizophrenia Bulletin, 19, 233-259.
Buchsbaum, M. S., Nuechterlein, K. H., Haier, R. J., Wu, J., Sicotte, N., Hazlett, E., Asarnow, R. F., Potkin, S., & Guich, S. (1990). Glucose metabolic rate in normals and schizophrenics during the Continu-ous Performance Test assessed by positron emission tomography.
British Journal of Psychiatry, 156, 216-227.
Chee, P., Logan, G., Schachar, R., Lindsay, P., & Wachsmuth, R. (1989). Effects of event rate and display time on sustained attention in hyperactive, normal, and control children. Journal of Abnormal
Child Psychology, 17, 371-391.
Chen, W. J., Hsiao, C. K., Hsiao, L.-L., & Hwu, H.-G. (1998). Per-formance of the Continuous PerPer-formance Test among community samples. Schizophrenia Bulletin, 24,163-174.
Chen, W. J., Hsiao, C. K., & Lin, C. C. H. (1997). Schizotypy in com-munity samples: The three-factor structure and correlation with sustained attention. Journal of Abnormal Psychology, 106, 649-654.
Chen, W. J., Liu, S. K., Chang, C. J., Lien, Y. J., Chang, Y. H., & Hwu, H. G. (1998). Sustained attention deficit and schizotypal person-ality features in nonpsychotic relatives of schizophrenic patients.
American Journal of Psychiatry, 155, 1214-1220.
Cohler, B. J., Grunebaum, H. U., Weiss, J. L., Gamer, E., & Gallant, D. H. (1977). Disturbances of attention among schizophrenic, depressed and well mothers and their children. Journal of Child Psychology
and Psychiatry, 18, 115-135.
Corkum, P. V., & Siegel, L. S. (1993). Is the Continuous Performance Task a valuable research tool for use with children with attention-deficit-hyperactivity disorder? Journal of Child Psychology and
Psychiatry and Allied Disciplines, 34, 1217-1239.
Cornblatt, B. A., & Erlenmeyer-Kimling, L. (1984). Early attentional predictors of adolescent behavioral disturbances in children at risk for schizophrenia. In N. F. Watt, E. J. Anthony, L. C. Wynne, & J. E. Rolf (Eds.), Children at risk for schizophrenia: A
longitudi-nal perspective (pp. 198-211). New York: Cambridge University
Press.
Cornblatt, B. A., & Erlenmeyer-Kimling, L. (1985). Global attentional deviance as a marker of risk for schizophrenia: Specificity and pre-dictive validity. Journal of Abnormal Psychology, 94, 470-486. Cornblatt, B. A., Risch, N. J., Fans, G., Friedman, D., &
Erlenmeyer-Kimling, L. (1988). The Continuous Performance Test, identical pairs version (CPT-IP): I. New findings about sustained attention in normal families. Psychiatry Research, 26, 223-238.
Davies, D. R., & Parasuraman, R. (1982). The psychology of vigilance. London: Academic Press.
Dykman, R. A., Ackerman, P. T, & Oglesby, D. M. (1979). Selective and sustained attention in hyperactive, learning-disabled, and nor-mal boys. The Journal of Nervous and Mental Disease, 167, 288-297.
Friedman, D., Boltri, J., Vaughan, H., & Erlenmeyer-Kimling, L. (1985). Effects of age and sex on the endogenous brain potential compo-nents during two continuous performance tasks. Psychophysiology,
22, 440-452.
Greenberg, L. M., & Waldman, I. D. (1993). Developmental normative data on the Test of Variables of Attention (TOVA). The Journal of
Child Psychology and Psychiatry and Allied Disciplines, 34,
1019-1030.
Gur, R. C., Gur, R. E., Obrist, W. D., Hungerbuhler, J. P., Younkin, D., Rosen, A. D., Skolnick, B. E., & Reivich, M. (1982, August). Sex
and handedness differences in cerebral blood flow during rest and cognitive activity. Science, 217, 659-661.
Halperin, J. M., Sharma, V., Greenblatt, E., & Schwartz, S. T. (1991). Assessment of the Continuous Performance Test: Reliability and validity in a nonreferred sample. Psychological Assessment, 3, 603-608.
Halperin, J. M., Wolf, L. E., Pascualvaca, D. M., Newcorn, J. H., Healy, J. M., O'Brien, J. D., Morgenstein, A., & Young, J. G. (1988). Differ-ential assessment of attention and impulsivity in children. Journal
of the American Academy of Child and Adolescent Psychiatry, 27,
326-329.
Harnishfeger, K. K., & Pope, R. S. (1996). Intending to forget: The development of cognitive inhibition in directed forgetting. Journal
of Experimental Child Psychology, 62, 292-315.
Herman, J., Mirsky, A. F, Ricks, N. C., & Gallant, D. (1977). Be-havioral and electrographic measures of attention in children at risk for schizophrenia. Journal of Abnormal Psychology, 86,
27-33.
Hooks, K., Milich, R., & Lorch, E. P. (1994). Sustained and selective at-tention in boys with atat-tention deficit hyperactivity disorder. Journal
of Clinical Child Psychology, 23, 69-77.
Horn, W. F., Wagner, A. E., & lalongo, N. (1989). Sex differences in school aged children with pervasive attention deficit hyperac-tivity disorder. Journal of Abnormal Child Psychology, 17, 109-125.
Lencz, T., Raine, A., Benishay, D. S., Mills, S., & Bird, L. (1995). Neu-ropsychological abnormalities associated with schizotypal person-ality. In A. Raine, T. Lencz, & S. A. Mednick (Eds.), Schizotypal
personality (pp. 289-328). New York: Cambridge University
Press.
Levy, F. (1980). The development of sustained attention (vigilance) in children: Some normative data. Journal of Child Psychology and
Psychiatry and Allied Disciplines, 21, 77-84.
Losier, B. J., McGrath, P. J., & Klein, R. M. (1996). Error patterns on the Continuous Performance Test in non-medicated and medicated samples of children with and without ADHD: A meta-analysis re-view. Journal of Child Psychology and Psychiatry and Allied
Dis-ciplines, 37, 971-987.
MacLusky, N. J., & Naftolin, F. (1981, March). Sexual differentiation of the central nervous system. Science, 211, 1294-1302.
Mirsky, A. F, Anthony, B. J., Duncan, C. C., Ahearn, M. B., & Kellam, S. G. (1991). Analysis of the elements of attention: A neuropsycho-logical approach. Neuropsychology Review, 2, 109-145. Nuechterlein, K. H. (1983). Signal detection in vigilance tasks and
be-havioral attributes among offspring of schizophrenic mothers and among hyperactive children. Journal of Abnormal Psychology, 92, 4-28.
Nuechterlein, K. H. (1991). Vigilance in schizophrenia and related dis-orders. In S. R. Steinhauer, J. H. Gruzelier, & J. Zubin (Eds.),
Handbook of schizophrenia (Vol. 5, pp. 397-433). Amsterdam, The
Netherlands: Elsevier.
Nuechterlein, K. H., Parasuraman, R., & Jiang, Q. (1983, April). Visual sustained attention: Image degradation produces rapid sensitivity decrement over time. Science, 220, 327-329.
O'Dougherty, M., & Nuechterlein, K. H. (1984). Hyperactive and hy-poxic children: Signal detection, sustained attention, and behavior.
Journal of Abnormal Psychology, 93, 178-191.
Rosvold, H. E., Mirsky, A. F., Sarason, I., Bransome, E. D. J., & Beck, L. H. (1956). A Continuous Performance Test of brain damage.
Journal of Consulting Psychology, 20, 343-350.
Rutschmann, J., Cornblatt, B., & Erlenmeyer-Kimling, L. (1977). Sus-tained attention in children at risk for schizophrenia: Report on a Continuous Performance Test. Archive of General Psychiatry, 34, 571-575.
SAS Institute, Inc. (1989). SAS/STAT User's Guide, Version 6. Cary, NC: SAS Institute.
Saykin, A. J., Gur, R. C., Gur, R. E., Mozley, P. D., Mozley, L. H., Resnick, S. M., Kester, D. B., & Stafiniak, P. (1991). Neu-ropsychological function in schizophrenia: Selective impairment
in memory and learning. Archive of General Psychiatry, 48, 618-624.
Seidel, W. T., & Joschko, M. (1990). Evidence of difficulties in sustained attention in children with ADDH. Journal of Abnormal Child
Psy-chology, 18, 217-229.
Shapiro, S. K., & Garfinkel, B. D. (1986). The occurrence of behav-ior disorders in children: The interdependence of attention deficit disorder and conduct disorder. Journal of the American Academy
of Child Psychiatry, 25, 809-819.
Sostek, A. J., Buchsbaum, M. S., & Rapoport, J. L. (1980). Effects of amphetamine on vigilance performance in normal and hyper-active children. Journal of Abnormal Child Psychology, 8, 491-500.
Swets, J. A. (1973, December). The relative operating characteristic in psychology: A technique for isolating effects of response bias finds wide use in the study of perception and cognition. Science, 182, 990-1001.
Sykes, D. H., Douglas, V. I., & Morgenstem, G. (1973). Sustained at-tention in hyperactive children. Journal of Child Psychology and
Psychiatry, 14, 213-220.
Sykes, D. H., Douglas, V. I., Weiss, G., & Minde, K. K. (1971). Attention in hyperactive children and the effect of methylphenidate. Journal
of Child Psychology and Psychiatry, 12, 129-139.
Tarnowski, K. J., Prinz, R. J., & Nay, S. M. (1986). Comparative analysis of attentional deficits in hyperactive and learning-disabled children.