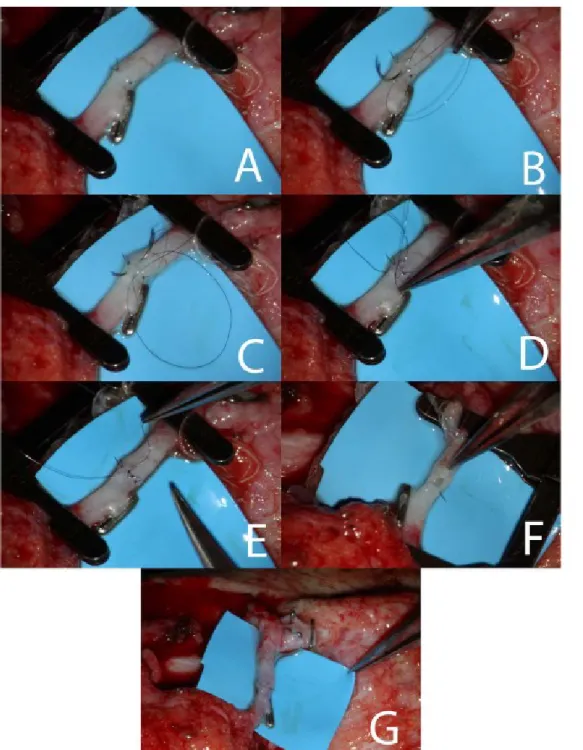
angle (Fig. 1A). Then a loose running suture
LETTER TO THE EDITOR
MICROSURGERY 34:82–84 (2014)
A NOVEL “CONTINUOUS-INTERRUPTED” METHOD FOR
MICROVASCULAR ANASTOMOSIS
Dear Editor,
conventional method of microvascular anastomosis with interrupted sutures is well proven method, with high successful rate. However, this method is time consuming, especially when multiple anastomosis are required. Even though several techniques have been described to mini-mize the time of anastomosis, none of these have been widely accepted.1,2 Vessel anastomosis with a continuous suture has the advantage of being faster than the conven-tional method but due to the high risk of stricture at the anastomotic site is not recommended for microvascular anastomosis.3
Herein, we present a novel method of performing microvascular anastomosis, which combines the advan-tages of the continuous and interrupted sutures. After proper setup of the vessels, the anastomosis begins with the application of two 10-0 sutures at 0 and 180
is applied at the anterior wall of the vessel. Depending on the size of the vessel, usually 3 to 4 passes of the suture are required, creating 2 or 3 loops, respectively. (Figs. 1B and 1C) Then the end of the first suture is tied with the corresponding suture of the opposite site and the knot is cut leaving one suture-loop less (Figs 1D and 1E). The same procedure is repeated for the rest sutures as well as at the posterior vessel wall (Figs. 1F and 1G).
*Correspondence to: Stamatis Sapountzis, Department of Plastic Surgery, China Medical University Hospital/, China Medical University, 2, Yuh-der Road, Taichung, Taiwan. E-mail: ssapountzis@yahoo.com
Received 16 May 2013; Accepted 19 July 2013
Published online 13 September 2013 in Wiley Online Library (wileyonlinelibrary. com). DOI: 10.1002/micr.22174
Ó 2013 Wiley Periodicals, Inc.
T
heWe performed this technique in 30 venous and 15 arterial anastomoses during free tissue transfer. In 15 free flaps, both the arterial and venous anastomoses were performed with the described method, meanwhile in other 15 free flaps, the arterial anastomoses were performed with the conventional method and the venous anastomosis with the “continuous-interrupted” tech-nique. In both of the groups, no complications were noted performing this technique as all the flaps survived well. Furthermore, the same surgeon in anterolateral thigh flap (ALT) flaps performed 20 venous anastomo-ses, 10 with the conventional technique, and 10 with the proposed method in order to compare the time dif-ference between the two methods in vessels with the same size. Statistically significant less time was
required (P < 0.05) for the venous anastomosis with the “continuous-interrupted” method.
The described method for microvascular anastomosis has several advantages. First of all, the application of the sutures can be very precise as the loosely running suture leaves spaces between the vessels, allowing the lumen to be visible without extensive manipulation of the vessel. This is very useful especially when the last suture of the anterior and posterior wall is applied, which with the conventional method there is limited space between the two edges of vessels. Similarly, dur-ing the anastomosis, the posterior vessel wall is always visible, avoiding inadvertent two-wall sewing. Addition-ally, even though the suture is applied continuously, finally tied as the interrupted fashion, hence there is no risk of stenosis at the anastomotic site. Finally, the anas-tomosis is performed faster than the conventional method, as the surgeon saves time applying the sutures with a running manner.
Letter to the Editor 83
Figure 1. A: Anastomosis of the anterior vessel wall. Two interrupted sutures are applied at 00 and 1800 angle. B: Second pass of the
running suture creating the first loop. C: Third pass of the running suture creating the second loop. D: The first running suture has already been tied as interrupted. At this picture the second suture is being tied, leaving the last loop. E: The knot of the second suture has been cut and the last suture of the anterior wall is ready to be tied. F: View of the posterior wall. The vessel lumen is open. G: Successful com-pletion of the anastomosis with no bleeding from the anastomotic site. [Color figure can be viewed in the online issue, which is available at wileyonlinelibrary.com.]
84 Letter to the Editor
STAMATIS SAPOUNTZIS, M.D.* KIDAKORN KIRANANTAWAT, M.D. SEONG YOON LIM, M.D. JOANNIS CONSTANTINIDES, M.D. PEDRO CIUDAD, M.D.
FABIO NICOLI, M.D.
MATTHEW YEO SZE WEI, M.D.
€TOLGA TAHA SONMEZ, M.D., and HUNG CHI CHEN, M.D., M.H.A., FACS Department of Plastic Surgery, China Medical University Hospital, Taichung, Taiwan
REFERENCES
1. Alghoul MS, Gordon CR, Yetman R, Buncke GM, Siemionow M, Afifi AM, Moon WK. From simple interrupted to complex spiral: a systematic review of various suture techniques for microvascular anastomoses. Microsurgery 2011;31:72–80.
2. Lykoudis EG, Spyropoulou GA, Liadakis GN, Papaliodi ET. A new combined “interrupted-continuous” microvascular anastomotic nique. Experimental study and clinical application. J Reconstr surg 2008;24:79–84.
3. Schlechter B, Guyuron B. A comparison of different suture ques for microvascular anastomosis. Ann Plast Surg 1994;33:28–31.