An Innovative VR-based Vestibular Rehabilitation System
Shih-Ching Yeh1, Pa-Chun Wang2, Yen-Po Hung1, Chia-Huang Chang3, Shuya Chen4, Mu-Chun Su1, Hsueh-Lin Chen5 1Department of Computer Science and Information Engineering, National Central University, Taoyuan, Taiwan
2 Department of otolaryngology, Cathay General Hospital, Taipei, Taiwan 3Outcomes Research Unit, Cathay Medical Research Institute, Taipei, Taiwan
4Department of Physical Therapy, China Medical University 5Industrial Technology Research Institute, ITRI
Abstract
Dizziness caused by peripheral vestibular nerve disease might lead to the imbalance of center of gravity, which in turn might affect the quality of daily life. Vestibular function rehabilitation exercise is thought to be able to improve the symptom of dizziness effectively. However, since rehabilitation process is boring, lacks of challenges and adaptive training contents and lacks of assessment method based on exercise analysis, the effectiveness of rehabilitation exercise is thus reduced. In this research, Cawthorne-Cooksey vestibular rehabilitation training exercise in clinical use was modified as an innovative interactive rehabilitation training system in which stereo imagimg, interactive technology and game technology were applied. In this research, clinical test (17 subjects, 6 training sessions) has been successfully carried out, during the experimental process, the task performance data, the time-history of the deviation distribution of center of gravity and subjective feeling questionnaire survey data of the patient is completely measured and recorded. The experimental result has verified the functionalities of this system, in the mean time, through the task performance evaluation and the analysis of level of balance, the medical effect of this system in assisting the patient to perform dizziness rehabilitation training has been proved, and the clinical observation also shows that the patient has higher willingness and motive to use such new system to perform rehabilitation.
Keywords: Virtual reality, rehabilitation, vertigo, vestibular dysfunction
I. INTRODUCTION
Dizziness is defined as: the sensation of motion when no motion is occurring relative to earth’s gravity [1]. It could lead to the difficulty of the patient in maintaining space recognition and body gesture. As a result, the loss of balance of center of gravity of the patient might prevent from performing lots of daily activities and the quality of daily life of the patient might get lost [2],
Vestibular rehabilitation was thought to be able to improve the symptom of dizziness effectively [3]. Among those, Cawthorne-Cooksey exercise has been proved to be able to improve the balancing capability and reduce the occurrence frequency of dizziness. For those patients whose vestibular function was already disabled, replacement
exercise function could be provided [4]. However, such exercise is boring, and is lack of challengeable and adaptive training content available to perform customized therapy. Therefore, the rehabilitation effect of rehabilitation exercise is limited.
In the related research, Uttama Lahiri[5] has used virtual reality to let children in autism dialogue with person of virtual reality to assist the therapy and monitor in real time the response of the patient. Sergei V [6] has used haptic gloves with force feedback to let patient do repeated Reach–Touch or Placing the ball or tea cup in the virtual environment for performing the rehabilitation of patient with Hemiparetic Upper Extremity. In the introduction of information simulation aid in vestibular function rehabilitation, Cheng [7] et al. has developed a set of virtual reality computer aided software for vestibular rehabilitation exercise, accompanied with electronic eye vibration chart and gesture balancer, to train the balancing function of vestibular system of the patient. Brain Port [8] has developed a set of physiological feedback system for dizziness patient with the loss of vestibular function, and the system can measure the neck gesture of the patient, then the electric stimulus placed on the tip of the tongue will guide the patient for the training.
In this research, for the Cawthorne-Cooksey vestibular rehabilitation exercise, virtual reality technology is used to develop the training system. The system can assist the patient to perform dizziness rehabilitation training, in the mean time, clinical measurement and record are made for the patient’s time history of the deviation distribution of center of gravity and task performance data. Meanwhile, survey questionnaire is used to measure the subjective feeling of the patient so as to understand further patient’s acceptance on new technology and to assess patient’s psychological factor.
II. METHODOLOGIES
The rehabilitation system contains two sub-systems: training system and assessment system. Training system will follow the design of Cawthorne-Cooksey exercise. Multi-dimensional information of the patient in the process can be completely recorded to facilitate the subsequent analysis and
assessment. Sensor technology is used to measure the time history of the trace of center of gravity for the patient under different statuses for subsequent analysis and assessment. A. Training system
Head movement task:
The main objective of this task is to urge the patient to have the eye look at a fixed object while the head is rotating. During the conduction process of the task, the head of the patient must rotate up and down or left and right, and the eye must look at the red square at the center of the screen. When the head rotates to the extent that only the remaining light of the eye can be used to look at the square, number will appear around the square, and the patient must read out the number. When the head rotates once and the number appears called one round, and there are 20 rounds in one game. This task has used large screen produced by ultra short focus projector, and optical ball tracking system has been used to trace the head rotation angle accurately. The entire task system is as shown in Figure 1.
Figure 1 The operation situationof head-move task Difficulty level of this system will be set up: The number of seconds of the number display:
The length of the display second limits the time for a patient to complete the task, and shorter second means that the eye of the patient will need faster focus to the location where the number appears.
Count of number display: When the count of number displayed each time is increased, it means that the time for single round of task performed by the patient will be extended accordingly too, and the possibility of the generation of dizziness on the patient will be enhanced too, in the mean time, the difficulty is also enhanced.
Multi-dimensional information:
Task performance (Count of right
answer/total count of questions).
Specific direction task performance (Count of right answer in specific direction/total count of question in specific direction). Eye movement task:
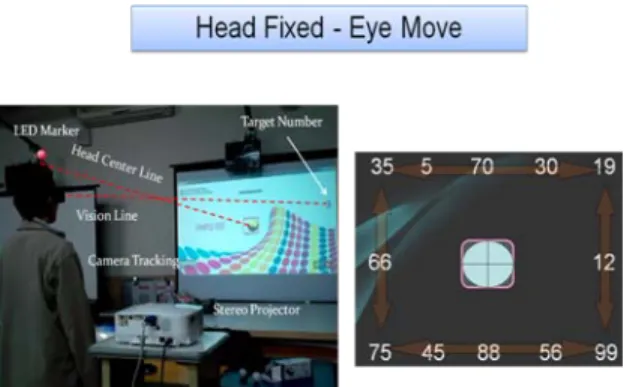
The main objective of this task is to urge the patient to move the eye to the border of the vision while the head is not rotating. During the process, the head of the patient must be fixed, but the eyeball must move up and down and left and right to read the number appear at the border of the vision. These number will appear at the edge of the screen according to clockwise or counter-clockwise, and this direction is set up in the very beginning of the game. When each one number appears is called one round, and there are 25 rounds in one game. During the process, if the tennis ball in the game deviates away from the red square due to head rotation , the game will then sound to alarm, and that round will be judged automatically as wrong. In order to cover all the scope of the vision, this task has used the large game screen produced by ultra short focus projector, in the mean time, image type optical ball tracking system is used to trace accurately if the head has rotation exceeding the allowable scope. The entire task system is as shown in Figure 2.
Figure 2 Operation situation and screen of eye-move task Difficulty level of this system will be set up: The number of seconds of the number display:
The length of the second display will limit the task finishing time by the patient, that is, shorter number of seconds means that the eye of the patient needs faster focus onto the appearance location of the number, hence, if the dizziness occurs to the patient, the patient will then need longer time of judgment, and different display number of second will lead to different level of difficulty on the patient. Multi-dimensional information:
Task performance (Count of right
answer/total count of questions). Limb and body extension task:
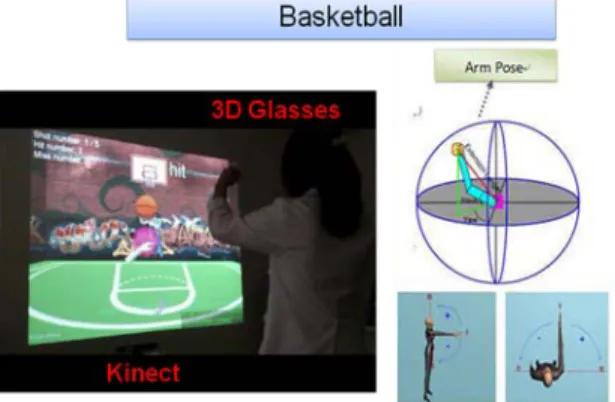
The main objective of this task is to urge the patient to raise the arms and extend them to certain point in the space. During the process, there are three balls exit in the scene, one is red ball R, one is yellow ball Y, and another one is ball B. Ball Y represents the location of the hand of the patient, next, hand is need to moved to the location of B ball, finally move to R ball location that appears at different location of the three dimensional space, The scene is projected by ultra short focus 3D projector, and the patient will use 3D glasses to sense virtual scene with depths. This system has used Microsoft Kinect to perform action tracking. The entire system is as shown in Figure 3.
Figure 3 Operation situation of the extension task Difficulty level of this system will be set up: Ball holding time: The shorter the time, the
patient will have the need to perform faster arm extension exercise, and it means that the dizziness will be easier to be triggered. Count of ball throwing: The higher of the
count of ball throwing, the longer the time of experiments to be carried out, and if the patient’s vestibular capability is not sufficient to cope with it, dizziness will then be generated.
Distance and angle: The upper arm gesture is decided by upper arm extension length, pitch and yaw that are based on the shoulder as the origin.
Selection of left and right hand: Whether the patient uses left hand or right hand to throw the ball can be selected.
Multi-dimensional physiological performance information:
Task performance (Finishing time/finishing proportion).
Upper arm gesture (point of ball catching) position-time history data.
Limb and body coordination task:
The main objective of this task is to urge the patient to perform the activity with limb and body coordination characteristic in both arms. During the
process, the patient is going to use both arms to touch ball in different locations in the virtual scenes, and the ball will be thrown to the spatial field of another arm due to the touch from the patient, and the ball throwing and catching will be repeated in such way. The environment setup was same as Limb and body extension task. This system also uses Microsoft Kinect and the patient can interact through action tracking and virtual scene. The entire system is as shown in Figure 4.
Figure 4 Operation situation of the coordination task Difficulty level of this system will be set up: Drop range radius: when the radius is larger,
the patient hand exercise range will be larger too, in the mean time, the patient will need better coordination capability.
Count of ball throwing and catching: The larger the count of ball throwing and catching means longer experiment carry-out time, and when the patient’s vestibular capability is insufficient, it will then generate dizziness. Ball speed: The patient needs better vestibular
function so as to be able to use faster exercise speed to cope with ball of faster movement speed.
Multi-dimensional physiological performance information:
Task performance (Finishing time/finishing proportion).
Position-time history data of the exercise tracking of upper arm gesture (Shoulder, elbow and wrist).
B. Assessment system
• The assessment system is, at the period before and after the rehabilitation therapy process of each stage, to assess the balance performance and improvement situation of the patient. We have used the pressure sensor device possessed by WiiFit to measure the historical data of the center of gravity of the patient in real time so as to set up the database and to carry out the subsequent balancing performance analysis. Before and after each time of rehabilitation, the
patient should, without the assistance of standing from the medical care personnel, stand on WiiFit for 20 seconds with both eyes opened so that the historical data of center of gravity of the patient can be measured. The entire assessment system is as shown in Figure 5.
Figure 5 Wiifit usage and real time display of center of gravity C. Experiment Design
TABLE I Characteristics of Participants
Mean (SD value)
Participants, (n, %) 17 (100)
Age (years) 56.71 (19.85)
<60 9
≥60 8
Gender 8 male / 9 female
Height (cm) 165.67 (7.24)
Weight (kg) 65.07 12.52)
The case taking standard is adult patient (age>=18) that is diagnosed as having chronic vestibular dysfunction and can be done with balance rehabilitation. The case arrangement standards are feeling, recognition and language hindrance will hinder them from using the computer interface, following experimental oral command or finishing the survey questionnaire. The therapists meeting the project standards are occupational therapists or physical therapists currently in practice.
This clinical research experiment has recruited 17 participants, those will follow modified Cawthorne-Cooksey exercises test(MCCET) and the command, and each subject will finish six training sessions within four weeks.
In order to assess the patient’s self-performance and improvement situation, before and after the carry-out of exercise, WiiFit is usually used to measure the clinical historical data of the distribution of center of gravity of the body. After finishing all the rehabilitation practices, we will ask the patient to fill out generalized questionnaire regarding their feeling.
III. DISSCUSSION A. Performance assessment
TABLE II Improvement of MCCET
MCCE
Score (base line) session 2 (post-test) session 6 value p Effect size
Eye (15.97) 83.29 (12.33) 89.25 0.01 0.41 Head (13.67) 75.20 (11.31) 81.59 0.21 0.49 Stretch (23.19) 70.88 (14.96) 85.73 0.03 0.74 Ball (13.74) 57.67 (11.93) 68.89 0.02 0.85 Significance Level = 0.05
For the game task, we have treated the first training session as the practice of the game to waive patient’s progress due to learning and familiarity of the game, the second session is used as baseline, and the sixth training session is used as post-test. TABLE II shows the average performance in the rehabilitation game from 17 patients. Through statistical analysis is shows significance in three items.
In eye-move task, the patient progress rate is 15/17 = 88.34 %, with level of improvement of 6.68%.
In head-move task, the proportion of patient in progress is about 11/17 = 64.71 %, with level of improvement of 7.83%.
In limb and body extension task, the patient with progress is 13/17 = 76.47 %, with level of improvement of 17.32%.
In limb and body coordination task, the patient with progress is 13/17 = 76.47 %, and the level of improvement is 16.29%.
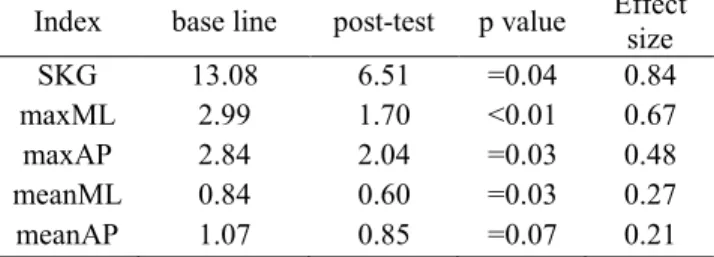
B. Analysis and measurement of level of balance The time history data can analyze five important balancing indexes: envelope line area SKG value (SKG index), maximal X and Y shifts (maxML and maxAP indexes), average X and Y shifts per second (meanML and meanAP indexes). Cristiane [9] pointed out that the calculation of the envelope area of the patient is one important index to assess the rehabilitation improvement situation of the patient.
We have used the pre-test data in the first therapy session as the entire pre-test value, and the pre-test data of the last session as the post-test value. We also used statistical analysis to verify if there is significant difference between pre-test and post-test, except meanAP, the rest four indexes all show significance (as shown in TABLE III).
TABLE III Postugraphy Measurements Following MCCE Index base line post-test p value Effect size
SKG 13.08 6.51 =0.04 0.84
maxML 2.99 1.70 <0.01 0.67
maxAP 2.84 2.04 =0.03 0.48
meanML 0.84 0.60 =0.03 0.27
Significance Level = 0.05
For SKG envelope area, the proportion of patient with progress is 11/17 = 64.7 %, with level of improvement of 50.26 %. In the index of maxML / maxAP, 15/12 out of 17 patients are show progress, and the proportion of patient with progress is 88.24% / 70.59%, the level of improvement is 42.9% / 27.9%.
For the index of meanML / meanAP, 13/14 out of 17 patients show progress, the proportion of patient with progress is 76.5% / 82.4%, with level of improvement of 27.63% / 20.26%.
IV. CONCLUSIONS
In this research, an innovative vestibular rehabilitation system derived from Cawthorne-Cooksey training exercise was developed via virtual reality technologies in which stereo imaging, motion tracking and 3D games were utilized. Besides, sensing technologies was used to develop new-type assessment method for assessing the level of balance. Further, a clinical experiment was conducted and 17 subjects were recruited for the participation of the test. According to the result, we found that this exercise generally has better improvement on dizziness caused by no head rotation of head rotation of small amplitude.
In the future, the subjective perception data of the patients collected in this research will be further analyzed, besides this system will be used continuously to investigate how to enhance the rehabilitation performance for the dizziness caused by larger amplitude of head swing.
V. ACKNOWLEDGEMENT
We are grateful for the support of the National Science Council, Taiwan, under NSC 100-2221-E-008-043- & NSC 100-2631-S-008-001, and Microsoft in Taiwan.
VI. REFERENCE
[1] Monsell EM, Balkany TA, Gates GA, et al. “Committee on hearing and equilibrium guidelines for the diagnosis and evaluation of therapy in Meniere's disease”, Otolaryngol Head Neck Surg 1995;113:186-7. [2] Gauchard GC, Jeandel C, Perrin PP. Physical and Sporting Activities
Improve Vestibular Afferent Usage and Balance in Elderly Human Subjects. Gerontology 2001;47:263-270.
[3] Michael C. Schubert, Susan L. Whitney, From Cawthorne-Cooksey to Biotechnology: Where We Have Been and Where We Are Headed in Vestibular Rehabilitation? JNPT 2010 June, Volume 34.
[4] Schubert MC, Whitney SL. From Cawthorne-Cooksey to biotechnology: where we have been and where we are headed in vestibular rehabilitation? J Neurol Phys Ther. 2010;34(2):62-3.
[5] Uttama Lahiri, Zachary Warren, Nilanjan Sarkar, “Design of a Gaze-Sensitive Virtual Social Interactive System for Children With Autism” , IEEE TRANSACTIONS ON NEURAL SYSTEMS AND REHABILITATION ENGINEERING, VOL. 19, NO. 4, AUGUST 2011.
[6] Sergei V. Adamovich, Gerard G, et al. “Incorporating Haptic Effects Into Three-Dimensional Virtual Environments to Train the Hemiparetic Upper Extremity“, IEEE TRANSACTIONS ON NEURAL SYSTEMS AND REHABILITATION ENGINEERING, VOL. 17, NO. 5, OCTOBER 2009.
[7] Chin-I Huang, “Human Vestibular Based (HVB) Senseless Maneuver Optimal Washout Filter Design for VR-based Motion Simulator”, IEEE International Conference on Systems, Man, and Cybernetics, 200 [8] Brain Port , “Efficacy of electrotactile vestibular substitution in patients with bilateral vestibular and central balance loss”, IEEE Conference of Engineering in Medicine and Biology Society, 2006
[9] Cristiane Akemi Kasse, Graziela Gaspar Santana, Renata Coelho Scharlach, Juliana Maria Gazzola, Fatima Cristina Barreiro Branco, Flavia Dona, ”Vestibular rehabilitation exercises in acute vertigo”, Braz J Otorhinolaryngol, 76(5):623-9, 2010.