原位性乳癌相關復發因子之研究; The Histopathologic Factors and Biologic Markers Associated with Clinical Recurrence in Ductal Carcinoma in Situ of the Breast
25
0
0
全文
(2) 中文摘要 研究目的: 由於目前篩檢性的乳房攝影在全球性的大量運用,使乳房原位癌 ( Ductal carcinoma in situ )的發現率逐年上升,而目前全球對於 零期乳癌病人的治療方式並未獲得一致性的共識,其中包括了乳房保 留手術或乳房全切除手術之選擇和後續的輔助性療法之應用。理論上 而言,原位性乳癌屬未侵犯性癌,為一發展初期的狀況,其癌細胞尚 未突破基底膜 (basement membrane),但臨床上發現病人經完整治療 後,其復發率仍舊維持在 7%至 20%之間。此研究之目的主要是針對零 期乳癌的病人,其中是否有存在特殊之因子能夠預期復發之可能性進 而給予此類病人輔助性治療而達到預防其復發之目的。 研究方法: 此研究是回朔性收集中國醫學大學附設醫院從 1998 年至 2005 年 此 7 年期間共 70 例零期乳癌的病人,全數接受乳房全切除術或是乳 房保留手術,部份病人並於術後接受輔助性放射線治療或荷爾蒙治 療。此研究中根據病人停經與否(premenopausal or postmenopausal period)、腫瘤大小(tumor size)、腫瘤數目(tumor number)、腫瘤 組織分級(histologic grade)、腫瘤組織形態(type)、顯微鈣化的呈 現(microcalcification)、有無組織壞死(necrosis)、有無神經浸潤 (perineyral invasion)、有無淋巴血管侵犯(lymphovascular invasion)及有無腺體異化增生(apocrine metaplasia)等 10 項病理 組織因子及荷爾蒙接受體之狀態(ER 和 PR)和 Her-2/new 的表現等 3 項生化因子進行分析統計研究。 研究結果: 在收集的 70 例零期乳癌的病人當中有 4 位復發,復發率為 5.7% 而平均復發時間為 38.25 個月(範圍 10-23 個月) ,而 70 位病人的平 均年紀為 51.8 歲(範圍 31-89 歲) ,平均追蹤的時間為 35.6 個月(範 圍 9-92 個月) 。在此篇研究當中,停經前原位癌患者似乎增加乳癌復 I.
(3) 發之機會,但根據統計的結果並沒有特別相關的因子能用於預測原位 癌之復發。 研究結論: 根據近期相關的文獻報告 Van Nuys 分級系統在臨床上而言是一 個有用的預測復發的因子,但是此研究當中所分析的十項組織病理因 子及三項生化方面的因子對復發而言都沒有特別的關聯性,不過隨著 分子生物學的進步,許多的因子都正在進行相關的研究,這也是未來 的一個重要方向。. II.
(4) 英文摘要 The Histopathologic Factors and Biologic Markers Associated with Clinical Recurrence in Ductal Carcinoma in Situ of the Breast. Abstract: Aims: Because of widespread use of screening mammography, the incidence of DCIS has risen, and recurrence rate from 7 to 20% are reported after mastectomy or breast conserving surgery with adjuvant radiotherapy in DCIS patients. The prognostic factors should be identified and these patients of DCIS with risk factors should receive appropriate treatment to prevent clinical recurrence. Patients and Methods: The 70 patients of pure DCIS receiving total mastectomy or breast conserving surgery with or without adjuvant radiotherapy after pathology confirmed were enrolled between June 1998 and May 2005 in China Medical University Hospital (CMUH). The status of menses, tumor size, tumor number, histologic grade, type, presence or absence of microcalcification, necrosis, perineural invasion, lymphovascular invasion, apocrine metaplasia, estrogen receptor (ER), progesterone receptor (PR), and HER-2/neu are chosen to analyzed with immunohistochemistry method. Fisher’s exact test and the logistic regression were used for statistical analysis. Results: There was a total of 70 patients with DCIS enrolled in this study. The four of the patients (5.7%, 4/70) had a recurrence with median interval to recurrence of 38.25 months (range 10-83 months). The median age in the 70 patients was 51.8 years (range 31-89 years) and the age at diagnosis of DCIS was 48.35 years ( range 27-86 years). The median length of follow-up was 35.6 months ( range 9-92 months). In this study, the DCIS patients within premenopausal period seem to be associated with increased risk of recurrence. However there were no histopathological or biological factors showing significant relation with recurrence.. III.
(5) Conclusion: Based on the current review, the Van Nuys classification system was a useful predictor for recurrence although there was no significant biological and histopathological difference in our study. In this study, the DCIS patients within premenopausal period seem to be associated with increased risk of recurrence. There is a need of further evaluation of the genetic expression to find the useful predictors for elimination of recurrence in DCIS patients.. IV.
(6) 致. 謝. 辭. 此研究是回朔性收集了中國醫藥大學附設醫院,從 1998 年至 2005 年此 7 年期間共 96 例零期乳癌的病人,根據條件限制,最後共 收集了 70 例原位性乳癌的病人進入此研究。由於零期乳癌的病人在 臨床上收集不易,且研究過程中亦遭遇許多困難。其中因得到許多老 師、教授們的熱心幫忙,且大力支持此研究之目的,使得許多不易解 決之難題,最後皆能迎刃而解,而研究才得以順利完成。故在此特別 提出感謝。 中國醫藥大學. 醫學研究所: 李昭宏 副教授. 中國醫藥大學. 中醫研究所: 陳光偉 所 長. 中國醫藥大學附設醫院 乳房外科: 王惠暢 主 任 彰化基督教醫院. 外科部: 陳達人 教 授. 中國醫藥大學附設醫院. 病理部: 林智一 醫 師. 中山醫學大學. 醫務管理系: 廖宏昌 副教授. V.
(7) 目 一、第一章 前言. 錄 -------------------- 1. 第一節 研究背景及目的 ------------ 1. 二、第二章 研究方法. ----------------- 3. 第一節 研究材料 ------------------ 3 第二節 研究設計 ------------------ 3 第三節 統計方法 ------------------ 5. 三、第三章 研究結果 ------------------ 5 四、第四章 討論 ---------------------- 7 五、第五章 結論與建議 ---------------- 8 六、表一. ---------------------------- 9. 七、表二. ---------------------------- 11. 八、表三. ---------------------------- 12. 九、參考文獻 ------------------------- 13. VI.
(8) 第一章 前言 第一節 研究背景及目的 原位性乳癌( Ductal carcinoma in situ of breast;DCIS)主要是指癌 細胞尚未突破基底膜而且亦未產生基質的侵犯(1)。過去原位性乳癌 是一個鮮少被提及和討論的領域而其大約佔了整體乳癌病患 5%的比 例,但隨著檢查工具的日新月異及全球篩檢性乳房攝影的大量廣泛使 用,原位性乳癌佔整體乳癌病患的比例已大幅提升至 15%到 25%之 間。由於原位性乳癌屬於非侵犯性的零期癌,理論上而言應具有自我 設限之特性,換言之即不具侵犯性,所以治療上應只須全乳房切除即 可達到完全治癒之目的,除此之外亦同時預防其復發。但事實上,有 許多的研究顯示臨床上的復發率,從 15%至 20%都有醫療機構曾報 告過(2.3)。以往原位性乳癌以全乳房切除即可達到治療及預防復發的 目的(4)。此類原位性乳癌在復發時,除了復發為原位性乳癌外,有 一部份病人會形成更嚴重之侵犯性乳癌。目前由於乳房保留手術的進 步,再加上三項大型的臨床研究報告,包括 NSABP. B-17 ,EORTC trail 10853 和 UK DCS 都顯示原位性乳癌的患者,在接受乳房保留 手術之後,再接受輔助性放射線治療亦能達到降低原位性乳癌復發的 機率(5-10) 。所謂的乳房保留手術即切除沿著腫瘤周圍合併大約 1 公 分正常的乳房組織為安全距離 (Free margin),其復發率為 7% 至 9%,而且一半的復發病人可能成為侵犯性乳癌(5.7)。因此,我們為 了降低復發率,也為了給予病人最適當的治療。在臨床上,找出影響 復發的因子,是非常重要的。有促進復發因子的病人,在治療上就可 能需要給予更進一步輔助性的治療。目前為止,己有許多的研究機構 及醫療單位投入大量的人力及物力,致力找出預測復發的因子。而許 多的組織病理因子 (histopathological factors),也己經被研究並發表相 關的文獻報告,包括了腫瘤大小 (tumor size)、核分裂等級 (nuclear grade)、組織型態的變化 (histologic type)、及安全距離的大小 (free margin) 和是否呈現壞死組織 (presence of necrosis) 等和乳癌復發的 關係 (8.11-19)。雖然有很多的報告己發表,但結果卻呈現多樣化, 並沒有一致性的共識。Silverstein 研究團隊發現細胞核分化的程度和 -1-.
(9) 是否呈現 comedo necrosis,對原位性乳癌的病人而言,是非常重要 的預測因子,也就是說如果病人呈現 comedo necrosis,或是呈現高 程度細胞核分化代表病人容易有復發的情形,在治療上需要再加以輔 助性療法。而 S. Roka 等人的研究指出,高程度的細胞核分化 (high nuclear grade) 和呈現荷爾蒙接受體陰性 (negative status of estrogen receptor) 這二項組織病理因子能夠有效的預測原位性乳癌病人復發 的情形。另一方面 S. Stallard 研究顯示,腫瘤位置和乳頭的距離亦是 一個相關因子。但是卻有其他的學者如 Solin 之研究團隊指出,並沒 有發現相關預測復發之因子。可見相關的研究雖多但並未形成一個相 同的共識。根據最近研究 Van Nuys prognostic index (VNPI)提供 了我們一個有用的預測復發工具,其中包括了腫瘤大小、安全距離的 大小、細胞核分化程度和是否呈現 comedo necrosis 有相當的關係。 而第五項因素,病人的年紀也因為其重要性而加入此一分級系統當中 (15.10.20)。另一方面,隨著分子生物科技學的進步,基因科技的發 現,己有大量生物學上的因子有別於傳統組織病理學上所發現的因子 被加入研究當中,包括 estrogen receptor (ER), progesterone receptor (PR), HER-2/neu, p53, Ki-67, bcl-2, E-cadherin, p21 等。相同的,許多 的研究的結果也顯示沒有一定的結論 (21-26)。而在此研究當中,我 們採取了病人停經與否(premenopausal or postmenopausal period)、腫瘤大小(tumor size)、腫瘤數目(tumor number)、腫瘤組織 分級(histologic grade)、腫瘤組織形態(type)、顯微鈣化的呈現 (microcalcification)、有無組織壞死(necrosis)、有無神經浸潤(perineural invasion)、有無淋巴血管侵犯(lymphovascular invasion)及有無腺體異 化增生(apocrine metaplasia)等 10 項因子併入組織病理學因子的研 究。而另外 ER、 PR 和 Her2-reu 等三項因子併入生物學因子的研 究,探討這十三項因子是否能夠有效預測原位性乳癌的病人疾病復發 的可能。. -2-.
(10) 第二章 研究方法 第一節 研究材料 此研究是回朔性收集了中國醫藥大學附設醫院,從 1998 年至 2005 年此 7 年期間共 96 例零期乳癌的病人,此 96 例病人都接受乳房超音 波及乳房攝影的檢查。這些病人當中,如果有合併其他惡性腫瘤或是 之前曾是侵犯性乳癌的病人經治療後又復發原位癌的病人必須排除 在收集的病人之外。另外一方面,如果因侵犯性乳癌而先接受 neoadjuvant 化學治療後,最後轉變成原位癌的病人,也不能納入收 集當中。以上述條件,共收集了 70 例原位性乳癌的病人,而這些病 人都經過病理上的確認,證實是原位性乳癌。此 70 位病人,一部份 接受全乳房切除手術,其餘接受乳房保留手術,而切下的標本經病理 確認,皆保有安全距離,亦表示乳房原位癌完全切除,切除邊緣無發 現殘餘癌細胞。病理標本上經染色確定是屬於 ER 或 PR 陽性的病 人,後續會給予輔助性荷爾蒙治療,即給予藥物 Tamoxifen 輔助治 療。因為許多研究己顯示,如果乳癌病人是屬於 ER 或 PR 陽性的族 群,使用輔助性荷爾蒙治療確實在臨床上會有相當程度的益處 (19.27)。臨床上復發的定義,是指原發性乳癌經治療後,後續追蹤 6 個月以上,又發現乳癌細胞。此 70 個病人所分析的資料都呈現於表 1 及表 2 當中,而這些病人在經過治療後,在前 2 年追踪期中每 3 個 月接受評估及檢查,包括每三個月血清腫瘤指數的高低 (CEA .CA-125.CA-153),而每 6 個月則另外接受胸部放射線檢查及 其他血清生化檢查,而年度檢查則包含全身骨頭掃描、腹部超音波及 對側乳房攝影。而在追蹤 2 年後,後續則只需接受 6 個月期的追踪檢 查。 第二節 研究設計 組織病理學方法:所有的標本都使用免疫染色法(H&E staining ),並 且經過中國醫藥大學病理科醫師確定。分析的因子及結果都詳實記錄 於表 1 及表 2。第一項因子,腫瘤大小(tumor size),主要是根據腫瘤 -3-.
(11) 的最大徑,其分為 4 個分項 (<=1.0m 、 >1 至<=2.0m 、 >2 至<=3.0m 、>3.0m) 。第二項分析因子是腫瘤個數(tumor number), 如個數大於 3 個就分類為多發性(multifocal lesion) 。第三項分析因 子為腫瘤組織分級(histologic grade),主要是根據 Holland 等人的定 義分為低(low)、中(intermediate)、高(high)三種分化等級。低等程度 分化是指單一、圓形或橢圓且細小的染色體並缺少核仁,而高等分化 則是指較差的分化,而且伴隨著大且粗糙的核仁及空泡狀染色質,而 中等分化則是介於低及高之間的程度(28-30)。但是有些原位性乳癌會 同時出現多種分化並存之狀況,此種情形則是採取較高等級的分化。 第四項因子為腫瘤的分類(tumor type),原位性乳癌共分為五類 (solid,papillay,micropapillary,comedo,cribriform) ,有些原位性 乳癌會有 2 至 3 種類型併存,所以此研究主要是根據病理檢查下,取 其較強表現的類型為其代表,而進一步又將其五種次分型再歸類為 comedo 及 non-comedo 兩種類型。Non-comedo type 包含了 solid , papillay,micropapillary 和 cribriform 四種。除此之外此研究分析的 因子亦包含病人停經與否(premenopausal or postmenopausal period)、顯微鈣化的有無(microcalcification)、組織壞死的呈現 (necrosis)、神經(perineural invasion)、淋巴和血管的侵犯 (lymphovascular invasion)及腺體異化增生(apocrine metaplasia)。 生物學方法:此 70 例病人當中,有 3 例未復發的病人其病理檢驗結 果中並未呈現 ER、PR、Her2-/new 之相關資料,故無法納入研究之 中,其餘有 67 位原位性乳癌的病人納入生物統計學因子檢驗統計。 此研究中把 ER、PR、Her2-/new 三個分析因子歸類為陽性及陰性兩 類,而陽性定義為超過 10%的細胞有染色表現(31)。所有的標本都用 免疫組織化學法以 Liquid DAB-Plus Substrate kit (3,3’-diaminobenzidine tetrahydrochloride-plus kit, substrate for horseradish peroxidase)染色而結果呈現出黑褐色沈積。. -4-.
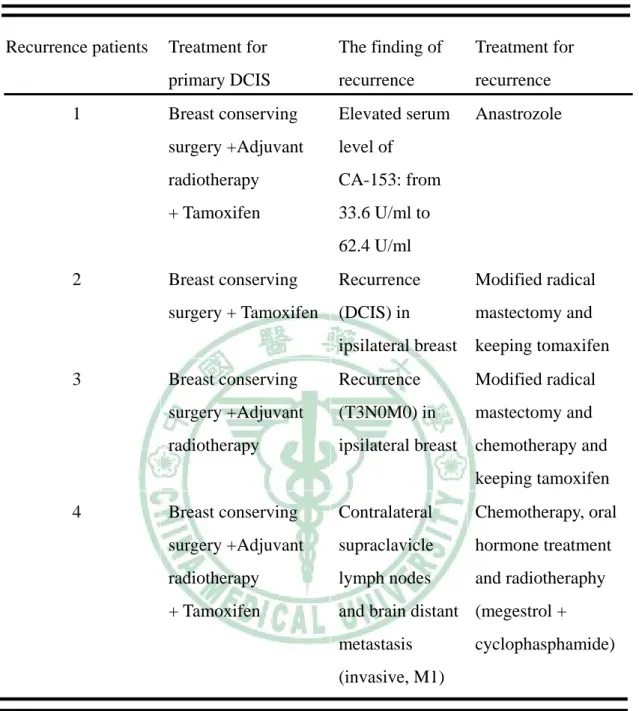
(12) 第三節 統計方法 此研究是以 Fisher`s exact 及 Logistic regression 做為統計分析 法,P 值小於 0.05 定義為有意義之分析結果。 第三章 研究結果 此 70 例病人經過統計的結果都完整呈現於表 1 及表 2,其中 33 個病人接受全乳房切除術而另外 37 個病人接受乳房保留手術,有一 部分病人接受輔助性放射線治療,其餘則未接受放射線治療。這 70 例病人平均年紀為 51.8 歲 (範圍 31-89 歲) ,而診斷出原位性乳癌的 年紀為 48.5 歲(範圍 27-86 歲) 。首先,根據停經與否(premenopausal or postmenopausal period)而分析的結果並未顯現出其為一有意義 的預測復發的因子(OR=0.513,95% C.I. 0.051-5.200, p> 0.05) 。平均 追蹤的時間為 35.6 個月(範圍 9-92 個月) 。70 例病人當中有 4 例復發 (5.7%, 4/70),而平均從治療完成到復發的時間為 38.25 個月(範圍 10-83 個月) 。此 4 例復發病人的資料都呈現於表 3 當中,所有復發 的病人都是之前接受乳房保留手術而後 2 例(50%, 2/4)接受輔助性放 射線治療,另外 2 例(50%, 2/4)沒有接受放射線治療。而此 4 例復發 的乳癌有 1 例仍然是原位癌,另外 3 例則是侵犯性癌。在表 3 中,第 一位復發的病人主要是因為在追蹤期間血清中 CA-153 腫瘤指數由 33.6U/ml 一路攀升至 62.4 U/ml。雖然影像學的檢查並沒有特別發現 有其腫瘤的情況,但在臨床上而言,還是懷疑癌細胞在局部有產生復 發跡象,故此病人並沒有得到病理學上的確認。此位 DCIS 的病人之 前已接受過乳房保留手術合併輔助性放射線治療(5040cGy/28 factious 加上 600 cGy/3 factious)和荷爾蒙治療(tamoxifen) ,因為腫 瘤指數上升將 Tamoxifen 轉換成第三代 AI. (anatrozole)治療,目前腫 瘤指數已有往下之趨勢。第二位病人針對先前之原位性乳癌已接受部 分乳房保留手術及輔助性荷爾蒙治療,而後產生同側乳房局部復發 (DCIS)之後,即接受全乳房切除並且持續服用 Tamoxifen 以維持後 續賀爾蒙治療。而第三位原位性乳癌復發之病人之前亦已接受乳房保 -5-.
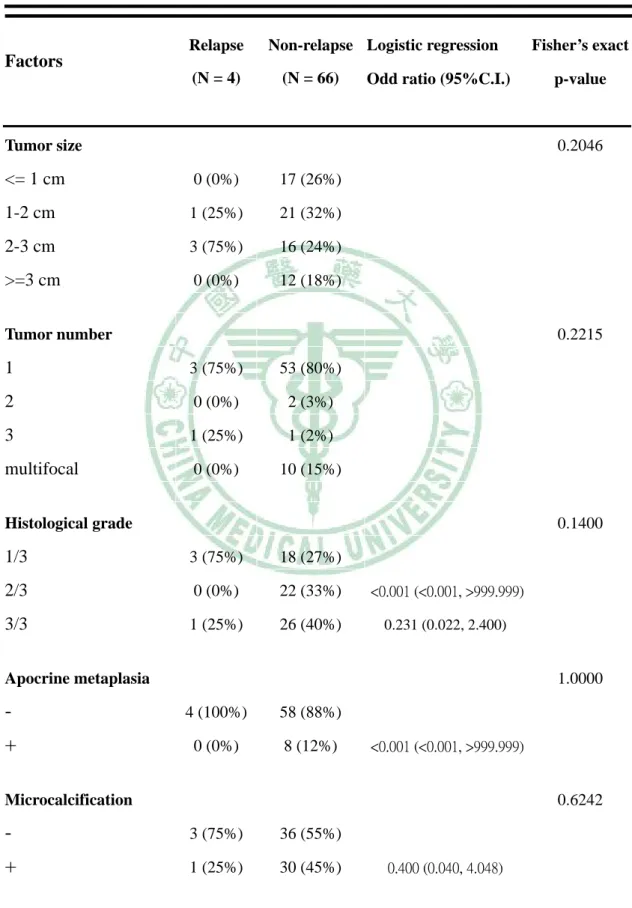
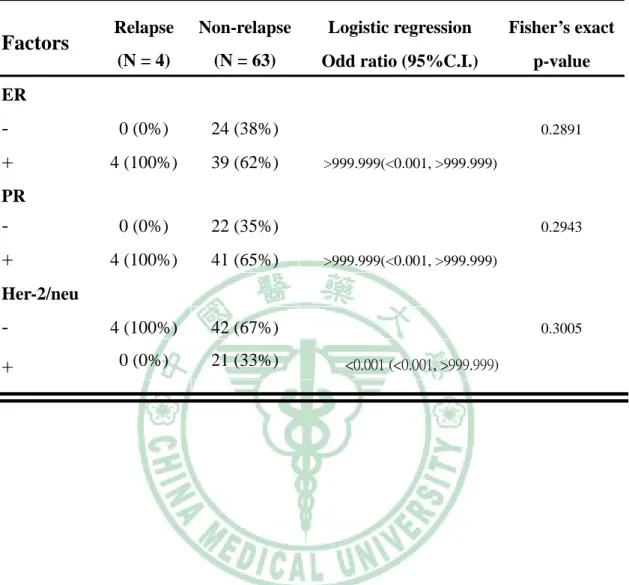
(13) 留手術合併輔助性放射線治療而後復發侵犯性乳癌(T3N0M0) ,即接 受乳房根除性手術並腋下淋巴結清除並且加上化學治療及荷爾蒙治 療(tamoxifen + taxol x 3 cycles)。最後第 4 位復發的病人是屬於遠端轉 移的情況(M1),包括對側鎖骨上淋巴結及腦部轉移。而此位病人之前 也接受乳房保留手術合併輔助性放射線治療,在於復發後接受口服化 療及荷爾蒙治療併放射線治療(megestrol + cyclophasphamide)。至目前 為止,所有的病人都仍存活且持續接受追蹤。 組織病理學因子:此研究所分析的十項組織病理學因子,都完整 呈現於表 1 之中。首先,腫瘤大小(p=0.2046)及腫瘤數目(p=0.2215) 這兩項因子經過統計分析後皆呈現與腫瘤復發並無相關性。就腫瘤組 織分級而言,在 4 例復發病人當中,有三例是屬於低程度的核分化, 而一例屬高程度之核分化,但統計分析後亦無明顯相關(p=0.14)。此 4 例復發病人皆呈現無腺體異化增生(p>0.05),無淋巴血管(p>0.05)神 經侵犯性之情況(p>0.05)。而統計分析後,此三項因子亦和復發無明 顯相關性,另外顯微鈣化的呈現( OR=0.400, 95% C.I. 0.040-4.048, p= 0.6242)及組織壞死( OR=0.547, 95% C.I. 0.054-5.547, p=1.00)亦不能 有效預測腫瘤復發,最後腫瘤型態此因子也和復發並無明顯相關 (p>0.05)。 生物學因子:ER、PR、Her2-/new 的染色情形,經分析結果呈現 於表 2 之中。而因為在未復發此一族群中有三例資料無法得知,故復 發及未復發兩羣是以 4 比 63 進行分析。研究中 4 例復發病人皆呈現 ER 陽性( p=0.2891)、PR 陽性(p=0.2943)、Her2-/new 陰性( p=0.3005), 經統計分析後,此三項生物學因子亦無呈現有意義的結果。 討論:如同前言所說,治療原位性乳癌的治療方式是非常多樣化的, 至目前為止,仍無一定之共識。也由於如此,我們更應該小心挑選出 具有高危險因子的病人,再加以後續的輔助性治療而達到預防復發的 目的。許多研究已顯示核分化的等級、安全距離大小、腫瘤大小、年 紀及腫瘤型態都是非常重要的預測復發的因子(12.32-37)。. -6-.
(14) 第四章 討論 此一研究中四位復發的病例其中有三位是屬於停經前這一組,似 乎代表在年輕的族群中是容易復發的,但經統計分析後並沒有顯現出 有其意義。除此之外,另外有兩個研究報告各表示在年輕族羣中(小 於 40 歲)有較高的復發率(32.38) 。在許多文獻報告中,已說明 USC/VNPI 是一個有效的預測指標。但是在此一研究中包括停經與 否、侵犯程度、腫瘤大小及組織壞死的呈現,經統計分析後,呈現出 和復發沒有明顯相關的結果。另一方面,有些研究報告指出 ER、PR 和 Her2-/new 並不是獨立之預測復發因子(14.20.39) ,但卻有另外的 研究指出 ER 陰性、PR 陰性及 Her2-/new 陽性的病例卻具有較易復發 的特質(40) 。在早期的研究中,Kninght WA 等人即有報告指出,ER 的狀態對復發而言是一個有效的預測因子 (41)。但最近的研究已認 為 ER 的狀態也只是反映出病人對荷爾蒙療法的效用(42.43)。針對此 一研究有兩項重點是值得討論的。第一,本研究所收集的個數相對而 言是屬於較小的羣體,而其中復發的個數亦是如此。在其他大型的研 究中所收集的個數全體都超過百例 (12.21) ,本研究復發率只有 5.7%,由於如此很容易在統計分析上出現偏差,尤其是當所要分析的 因子又再分為更多的次分組(如:腫瘤大小、腫瘤個數)時,分析上 的誤差更加明顯。另外,在此研究中,70 例的病患只要原位性乳癌 在病理染色上出現 ER 或 PR 陽性,即會給予輔助性荷爾蒙療法,或 許也因此在治療上有相當的幫助。相同地,NSABP-17、EORTC 1085-3 和 UKDICIS 三大研究都指出輔助性放射線治療的重要性 (5.10) 。也 因此,此研究中有部份病例可能因接受輔助性放射線治療而導致整體 復發率降低。第二,追蹤時間短亦是影響本研究結果的重要因素。此 70 例病人的平均追蹤時間為 35.6 個月,而 4 例復發病人的平均復發 時間為 38.25 個月。許多的大型研究其追蹤時間都比本研究長達將近 一年左右(12.21.31) 。所以在此研究中顯現出平均復發時間比平均追 蹤時間長,暗示本研究追蹤的時間不夠長,很可能腫瘤復發情形尚未 發生。. -7-.
(15) 第五章 結論與建議 雖然在我們研究中,組織病理學因子並不具預測效用。但我們回 顧很多研究並参考相當多文獻報告指出,Van Nuys 分級系統仍是一 個有用的預測工具。而生物方面的因子,如 ER、PR 和 Her2-/new 皆 與預測復發無相關性。另一方面,基於上述之討論,對於原位性乳癌 之研究勢必要收集更多的病例,增長追蹤的時間方能彌補統計上的誤 差,達到有效的分析。而且輔助性放射線治療及輔助性荷爾蒙治療等 相關因素都應嚴格的限制並加以納入考量,以釐清的真正原因及各相 關獨立之預測因子。隨著分子生物學和基因科學的進步,我們更要把 未來的焦點放在生物學方面的因子,如最近很多研究都分析的 Ki67.P53.bcl-2 等(14.21)。藉著對基因及細胞的完整窺探而更能研究 出預防腫瘤的有效方式。. -8-.
(16) Table 1. Univariate Analysis of Clinical and Histopathological Characteristics Related to Recurrence. Relapse. Non-relapse Logistic regression. Fisher’s exact. Factors (N = 4). (N = 66). Odd ratio (95%C.I.). Tumor size. p-value. 0.2046. <= 1 cm. 0 (0%). 17 (26%). 1-2 cm. 1 (25%). 21 (32%). 2-3 cm. 3 (75%). 16 (24%). >=3 cm. 0 (0%). 12 (18%). Tumor number. 0.2215. 1. 3 (75%). 53 (80%). 2. 0 (0%). 2 (3%). 3. 1 (25%). 1 (2%). multifocal. 0 (0%). 10 (15%). Histological grade. 0.1400. 1/3. 3 (75%). 18 (27%). 2/3. 0 (0%). 22 (33%). <0.001 (<0.001, >999.999). 3/3. 1 (25%). 26 (40%). 0.231 (0.022, 2.400). Apocrine metaplasia. 1.0000. -. 4 (100%). 58 (88%). +. 0 (0%). 8 (12%). <0.001 (<0.001, >999.999). Microcalcification. 0.6242. -. 3 (75%). 36 (55%). +. 1 (25%). 30 (45%). -9-. 0.400 (0.040, 4.048).
(17) Lymphovascular. 1.0000. invasion. -. 4 (100%). 65 (98%). +. 0 (0%). 1 (2%). <0.001 (<0.001, >999.999). Perineural invasion. -. -. 4 (100%). 66 (100%). +. 0 (0%). 0 (0%). -. Necrosis. 1.0000. -. 3 (75%). 41 (62%). +. 1 (25%). 25 (38%). premenopause. 3 (75%). 40 (60%). postmenopause. 1 (25%). 26 (40%). 0.547 (0.054, 5.547). Menses 1.0000 0.513 (0.051, 5.200). Tumor type. 0.3498. comedo. 1 (25%). 35 (53%). non-comedo. 3 (75%). 31 (47%). - 10 -. 0.295 (0.029, 2.987).
(18) Table 2 Univariate Analysis of Biological Characteristics Related to Recurrence Relapse. Non-relapse. Logistic regression. Fisher’s exact. (N = 4). (N = 63). Odd ratio (95%C.I.). p-value. -. 0 (0%). 24 (38%). +. 4 (100%). 39 (62%). -. 0 (0%). 22 (35%). +. 4 (100%). 41 (65%). -. 4 (100%). 42 (67%). +. 0 (0%). 21 (33%). Factors ER. 0.2891 >999.999(<0.001, >999.999). PR 0.2943 >999.999(<0.001, >999.999). Her-2/neu 0.3005 <0.001 (<0.001, >999.999). - 11 -.
(19) Table 3. Detail in 4 recurrences. Recurrence patients. 1. Treatment for. The finding of. Treatment for. primary DCIS. recurrence. recurrence. Breast conserving. Elevated serum. Anastrozole. surgery +Adjuvant. level of. radiotherapy. CA-153: from. + Tamoxifen. 33.6 U/ml to 62.4 U/ml. 2. 3. Breast conserving. Recurrence. Modified radical. surgery + Tamoxifen. (DCIS) in. mastectomy and. ipsilateral breast. keeping tomaxifen. Breast conserving. Recurrence. Modified radical. surgery +Adjuvant. (T3N0M0) in. mastectomy and. radiotherapy. ipsilateral breast. chemotherapy and keeping tamoxifen. 4. Breast conserving. Contralateral. Chemotherapy, oral. surgery +Adjuvant. supraclavicle. hormone treatment. radiotherapy. lymph nodes. and radiotheraphy. + Tamoxifen. and brain distant (megestrol + metastasis (invasive, M1). - 12 -. cyclophasphamide).
(20) References: 1. Tavassoli, F. A. (1998). Ductal carcinoma in situ: introduction of the concept of ductal intraepithelial neoplasia. Mod Pathol 11, 140-154. 2. Silverstein MJ, B. A., Poller DN, Gierson ED, Colburn WJ, Waisman JR, , and P., G. (1995). Ten-year results comparing mastectomy to excision and radiation therapy for ductal carcinoma in situ of the breast. Eur J Cancer 9, 1425-1427. 3. Ernster, V. L., Barclay, J., Kerlikowske, K., Grady, D., and Henderson, C. (1996). Incidence of and treatment for ductal carcinoma in situ of the breast. Jama 275, 913-918. 4. Boyages, J., Delaney, G., and Taylor, R. (1999). Predictors of local recurrence after treatment of ductal carcinoma in situ: a meta-analysis. Cancer 85, 616-628. 5. Julien, J. P., Bijker, N., Fentiman, I. S., Peterse, J. L., Delledonne, V., Rouanet, P., Avril, A., Sylvester, R., Mignolet, F., Bartelink, H., and Van Dongen, J. A. (2000). Radiotherapy in breast-conserving treatment for ductal carcinoma in situ: first results of the EORTC randomised phase III trial 10853. EORTC Breast Cancer Cooperative Group and EORTC Radiotherapy Group. Lancet 355, 528-533. 6. Fisher, B., Costantino, J., Redmond, C., Fisher, E., Margolese, R., Dimitrov, N., Wolmark, N., Wickerham, D. L., Deutsch, M., Ore, L., and et al. (1993). Lumpectomy compared with lumpectomy and radiation therapy for the treatment of intraductal breast cancer. N Engl J Med 328, 1581-1586. 7. Fisher, B., Dignam, J., Wolmark, N., Mamounas, E., Costantino, J., Poller, W., Fisher, E. R., Wickerham, D. L., Deutsch, M., Margolese, R., et al. (1998). Lumpectomy and radiation therapy for the treatment of intraductal breast cancer: findings from National Surgical Adjuvant Breast and Bowel Project B-17. J Clin Oncol 16, 441-452. 8. Fisher, E. R., Dignam, J., Tan-Chiu, E., Costantino, J., Fisher, B., Paik, S., and Wolmark, N. (1999). Pathologic findings from the National Surgical Adjuvant Breast Project (NSABP) eight-year update of Protocol B-17: intraductal carcinoma. Cancer 86, 429-438. 9. George W D, H. J., Cuzick J et al. (2000). Radiotherapy and tamoxifen following. - 13 -.
(21) complete local excision(CLE)in the management of ductal carcinoma in situ (DCIS): preliminary results from the UK DCIS trial. Proc Am Soc Clin Oncol 19, 70a. 10. Houghton, J., George, W. D., Cuzick, J., Duggan, C., Fentiman, I. S., and Spittle, M. (2003). Radiotherapy and tamoxifen in women with completely excised ductal carcinoma in situ of the breast in the UK, Australia, and New Zealand: randomised controlled trial. Lancet 362, 95-102. 11. Kestin, L. L., Goldstein, N. S., Lacerna, M. D., Balasubramaniam, M., Martinez, A. A., Rebner, M., Pettinga, J., Frazier, R. C., and Vicini, F. A. (2000). Factors associated with local recurrence of mammographically detected ductal carcinoma in situ in patients given breast-conserving therapy. Cancer 88, 596-607. 12. Ottesen, G. L., Graversen, H. P., Blichert-Toft, M., Zedeler, K., and Andersen, J. A. (1992). Ductal carcinoma in situ of the female breast. Short-term results of a prospective nationwide study. The Danish Breast Cancer Cooperative Group. Am J Surg Pathol 16, 1183-1196. 13. Ottesen, G. L., Graversen, H. P., Blichert-Toft, M., Christensen, I. J., and Andersen, J. A. (2000). Carcinoma in situ of the female breast. 10 year follow-up results of a prospective nationwide study. Breast Cancer Res Treat 62, 197-210. 14. Ringberg, A., Idvall, I., Ferno, M., Anderson, H., Anagnostaki, L., Boiesen, P., Bondesson, L., Holm, E., Johansson, S., Lindholm, K., et al. (2000). Ipsilateral local recurrence in relation to therapy and morphological characteristics in patients with ductal carcinoma in situ of the breast. Eur J Surg Oncol 26, 444-451. 15. Silverstein, M. J., Poller, D. N., Waisman, J. R., Colburn, W. J., Barth, A., Gierson, E. D., Lewinsky, B., Gamagami, P., and Slamon, D. J. (1995). Prognostic classification of breast ductal carcinoma-in-situ. Lancet 345, 1154-1157. 16. Silverstein, M. J., Lagios, M. D., Groshen, S., Waisman, J. R., Lewinsky, B. S., Martino, S., Gamagami, P., and Colburn, W. J. (1999). The influence of margin width on local control of ductal carcinoma in situ of the breast. N Engl J Med 340, 1455-1461. 17. Solin, L. J., Fourquet, A., Vicini, F. A., Haffty, B., Taylor, M., McCormick, B., McNeese, M., Pierce, L. J., Landmann, C., Olivotto, I. A., et al. (2001).. - 14 -.
(22) Mammographically detected ductal carcinoma in situ of the breast treated with breast-conserving surgery and definitive breast irradiation: long-term outcome and prognostic significance of patient age and margin status. Int J Radiat Oncol Biol Phys 50, 991-1002. 18. Solin, L. J., Kurtz, J., Fourquet, A., Amalric, R., Recht, A., Bornstein, B. A., Kuske, R., Taylor, M., Barrett, W., Fowble, B., et al. (1996). Fifteen-year results of breast-conserving surgery and definitive breast irradiation for the treatment of ductal carcinoma in situ of the breast. J Clin Oncol 14, 754-763. 19. Roka, S., Rudas, M., Taucher, S., Dubsky, P., Bachleitner-Hofmann, T., Kandioler, D., Gnant, M., and Jakesz, R. (2004). High nuclear grade and negative estrogen receptor are significant risk factors for recurrence in DCIS. Eur J Surg Oncol 30, 243-247. 20. Silverstein, M. J., Lagios, M. D., Craig, P. H., Waisman, J. R., Lewinsky, B. S., Colburn, W. J., and Poller, D. N. (1996). A prognostic index for ductal carcinoma in situ of the breast. Cancer 77, 2267-2274. 21. Cornfield, D. B., Palazzo, J. P., Schwartz, G. F., Goonewardene, S. A., Kovatich, A. J., Chervoneva, I., Hyslop, T., and Schwarting, R. (2004). The prognostic significance of multiple morphologic features and biologic markers in ductal carcinoma in situ of the breast: a study of a large cohort of patients treated with surgery alone. Cancer 100, 2317-2327. 22. Eissa, S., Khalifa, A., el-Gharib, A., Salah, N., and Mohamed, M. K. (1997). Multivariate analysis of DNA ploidy, p53, c-erbB-2 proteins, EGFR, and steroid hormone receptors for prediction of poor short term prognosis in breast cancer. Anticancer Res 17, 1417-1423. 23. Zellars, R. C., Hilsenbeck, S. G., Clark, G. M., Allred, D. C., Herman, T. S., Chamness, G. C., and Elledge, R. M. (2000). Prognostic value of p53 for local failure in mastectomy-treated breast cancer patients. J Clin Oncol 18, 1906-1913. 24. Quinn, C. M., Ostrowski, J. L., Harkins, L., Rice, A. J., and Loney, D. P. (1998). Loss of bcl-2 expression in ductal carcinoma in situ of the breast relates to poor histological differentiation and to expression of p53 and c-erbB-2 proteins. Histopathology 33, 531-536.. - 15 -.
(23) 25. Poller, D. N., Roberts, E. C., Bell, J. A., Elston, C. W., Blamey, R. W., and Ellis, I. O. (1993). p53 protein expression in mammary ductal carcinoma in situ: relationship to immunohistochemical expression of estrogen receptor and c-erbB-2 protein. Hum Pathol 24, 463-468. 26. Rudas, M., Neumayer, R., Gnant, M. F., Mittelbock, M., Jakesz, R., and Reiner, A. (1997). p53 protein expression, cell proliferation and steroid hormone receptors in ductal and lobular in situ carcinomas of the breast. Eur J Cancer 33, 39-44. 27. Gandhi, A., Holland, P. A., Knox, W. F., Potten, C. S., and Bundred, N. J. (2000). Effects of a pure antiestrogen on apoptosis and proliferation within human breast ductal carcinoma in situ. Cancer Res 60, 4284-4288. 28. Provenzano, E., Hopper, J. L., Giles, G. G., Marr, G., Venter, D. J., and Armes, J. E. (2004). Histological markers that predict clinical recurrence in ductal carcinoma in situ of the breast: an Australian population-based study. Pathology 36, 221-229. 29. Holland, R., Peterse, J. L., Millis, R. R., Eusebi, V., Faverly, D., van de Vijver, M. J., and Zafrani, B. (1994). Ductal carcinoma in situ: a proposal for a new classification. Semin Diagn Pathol 11, 167-180. 30. Bijker, N., Peterse, J. L., Duchateau, L., Julien, J. P., Fentiman, I. S., Duval, C., Di Palma, S., Simony-Lafontaine, J., de Mascarel, I., and van de Vijver, M. J. (2001). Risk factors for recurrence and metastasis after breast-conserving therapy for ductal carcinoma-in-situ: analysis of European Organization for Research and Treatment of Cancer Trial 10853. J Clin Oncol 19, 2263-2271. 31. Ringberg, A., Anagnostaki, L., Anderson, H., Idvall, I., and Ferno, M. (2001). Cell biological factors in ductal carcinoma in situ (DCIS) of the breast-relationship to ipsilateral local recurrence and histopathological characteristics. Eur J Cancer 37, 1514-1522. 32. Vicini, F. A., Kestin, L. L., Goldstein, N. S., Chen, P. Y., Pettinga, J., Frazier, R. C., and Martinez, A. A. (2000). Impact of young age on outcome in patients with ductal carcinoma-in-situ treated with breast-conserving therapy. J Clin Oncol 18, 296-306. 33. Goldstein, N. S., Kestin, L., and Vicini, F. (2000). Intraductal carcinoma of the breast: pathologic features associated with local recurrence in patients treated with breast-conserving therapy. Am J Surg Pathol 24, 1058-1067.. - 16 -.
(24) 34. Solin, L. J., Fourquet, A., McCormick, B., Haffty, B., Recht, A., Schultz, D. J., Barrett, W., Fowble, B. L., Kuske, R., Taylor, M., and et al. (1994). Salvage treatment for local recurrence following breast-conserving surgery and definitive irradiation for ductal carcinoma in situ (intraductal carcinoma) of the breast. Int J Radiat Oncol Biol Phys 30, 3-9. 35. Poller, D. N., Silverstein, M. J., Galea, M., Locker, A. P., Elston, C. W., Blamey, R. W., and Ellis, I. O. (1994). Ideas in pathology. Ductal carcinoma in situ of the breast: a proposal for a new simplified histological classification association between cellular proliferation and c-erbB-2 protein expression. Mod Pathol 7, 257-262. 36. Schwartz, G. F. (1994). The role of excision and surveillance alone in subclinical DCIS of the breast. Oncology (Williston Park) 8, 21-26; discussion 26-27, 31-22,35. 37. Zafrani, B., Leroyer, A., Fourquet, A., Laurent, M., Trophilme, D., Validire, P., and Sastre-Garau, X. (1994). Mammographically-detected ductal in situ carcinoma of the breast analyzed with a new classification. A study of 127 cases: correlation with estrogen and progesterone receptors, p53 and c-erbB-2 proteins, and proliferative activity. Semin Diagn Pathol 11, 208-214. 38. Van Zee, K. J., Liberman, L., Samli, B., Tran, K. N., McCormick, B., Petrek, J. A., Rosen, P. P., and Borgen, P. I. (1999). Long term follow-up of women with ductal carcinoma in situ treated with breast-conserving surgery: the effect of age. Cancer 86, 1757-1767. 39. Warnberg, F., Nordgren, H., Bergkvist, L., and Holmberg, L. (2001). Tumour markers in breast carcinoma correlate with grade rather than with invasiveness. Br J Cancer 85, 869-874. 40. Provenzano, E., Hopper, J. L., Giles, G. G., Marr, G., Venter, D. J., and Armes, J. E. (2003). Biological markers that predict clinical recurrence in ductal carcinoma in situ of the breast. Eur J Cancer 39, 622-630. 41. Knight, W. A., Livingston, R. B., Gregory, E. J., and McGuire, W. L. (1977). Estrogen receptor as an independent prognostic factor for early recurrence in breast cancer. Cancer Res 37, 4669-4671. 42. Osborne, C. K. (1998). Steroid hormone receptors in breast cancer management. Breast Cancer Res Treat 51, 227-238.. - 17 -.
(25) 43. Elston, C. W., Ellis, I. O., and Pinder, S. E. (1999). Pathological prognostic factors in breast cancer. Crit Rev Oncol Hematol 31, 209-223.. - 18 -.
(26)
數據
相關文件
Malins, “Squamous cell carcinoma arising in the lining of an epidermoid cyst within the sublingual gland—a case report,” British Journal of Oral and Maxillofacial Surgery, vol..
Persons with a phenotype mediated by one of these MC1R genetic variants are at greater risk of UV-induced skin cancers, because pheomelanin not only provides less effective
Loss of vascular content, increase of fat in the bone marrow cavity, and fibrosis showed a linear relation with time after radiation and were considered the end stage of
To evaluate the clinicopathologic features, prognostic factors, and management of patients in the North Chinese population with head and neck squamous cell carcinoma (HNSCC)
The isolated case showed typical features, including fibrocystic breast disease, benign thyroid nodules, and multiple papillomatous lesions in the face and oral cavity, and the
Oral and maxillofacial metastasis of male breast cancer: Report of a rare case and literature review
Less than 1% of all breast cancers occur in male patients, and to date, only 8 cases of metastatic breast adeno- carcinoma to the oral and maxillofacial region in a male patient
Papillary thyroid carcinoma, the commonest histopathologic variant of thyroid cancer, has minimal potential for distant metastasis, and most reported metastatic thyroid carcinomas
Carcinoma ex pleomorphic adenoma (CXPA) is a rare malignant salivary gland tumor, mostly involving the parotid and submandibular glands.. Minor salivary gland involvement is even
