行政院國家科學委員會專題研究計畫 成果報告
常壓性水腦之腦部血流量及化學分子移轉: 以腦化學移轉
造影及腦血流量圖作為治療適應症及療效之評估
計畫類別: 個別型計畫 計畫編號: NSC91-2314-B-002-341- 執行期間: 91 年 08 月 01 日至 92 年 12 月 31 日 執行單位: 國立臺灣大學醫學院外科 計畫主持人: 杜永光 計畫參與人員: 廖漢文 報告類型: 精簡報告 報告附件: 出席國際會議研究心得報告及發表論文 處理方式: 本計畫可公開查詢中 華 民 國 93 年 7 月 1 日
Report of # NSC91-3214-B-002-341
Cerebral Blood Flow and Chemical Shifting in Normal
Pressure Hydrocephalus:
Evaluation of Therapeutic Indication and Efficacy by
Chemical Imaging and Blood Flow Mapping
Yong-Kwang Tu, Dar-Min Lai and Hon-Man Liu*
Department of Neurosurgery and Department of Medical Imaging* School of Medicine and Hospital
National Taiwan University Taipei, Taiwan
Key Words: Normal Pressure Hydrocephalus, Regional Cerebral Blood Flow, Chemical Shifting Imaging, Magnetic Resonance Spectroscopy, Ventriculo-peritoneal Shunting
Introduction:
Normal pressure hydrocephalus (NPH) resulted from cerebrovascular accidents, head injury or other causes is a common disease among aged patients. This disease is characterized by the presence of symptoms of diffused brain dysfunction without those of intracranial hypertension. Deterioration of mental function, manifested initially as impairment of memory, insidiously progresses to confusion and severe deterioration of intellectual function, associate with disturbance of gait and bladder control. Because of the similar clinical manifestation and imaging finding on CT or MR, it is very difficult to differentiate this disease from brain atrophy or Alzheimer’s disease. Shunting procedure to drain cerebrospinal fluid (CSF) in NPH patients may effectively reverse these clinical problems, however, if the differential diagnosis is not properly made this surgery sometimes become unnecessary or even harmful.
Various tests have been investigated for the differentiation of these conditions, yet none was proven to be ideal. Demonstration of CSF circulation dynamics by cisternography with isotope intrathecal injection or employing CT and MR technique was tried but the results were equivocal. One recent study of regional blood flow measurement showed that both conditions caused the reduction of flow over the periventricular areas of the brain but the results of cerebrovascular reactivity are different between NPH and brain atrophy. Thus, we hypothesize that in a reversible clinical condition such as NPH, although rCBF is depleted due to the pressure effect from dilated ventricles, neuronal metabolic activity should remain normal or
suboptimal. On the contrary, both rCBF and neuronal metabolic activity should be very low in the irreversible condition of brain atrophy.
In vivo proton magnetic resonance spectroscopy allows noninvasive evaluation of brain metabolism on patients with neurological disease. During the past 3 years, we conducted two studies to evaluate the biochemical changes of the brain
parenchyma with proton magnetic resonance spectroscopy (H-MRS) and the changes of regional cerebral blood flow (rCBF) in patients with moderate head injury and intracerebral hemorrhage. We demonstrate a good correlation among H-MRS, rCBF and patients clinical outcome in these two diseases. Recently, we are able to apply imaging software to reconstruct proton single voxel spectroscopy into chemical shifting imaging (CSI). With this technique, rCBF mapping can be
Material and Methods:
1. General protocol
From August 2002 to July 2003, a total of 25 patients with the clinical diagnosis of NHP were selected to enter this study. Before and after the ventriculo-peritoneal shunting procedure, all the patients received the following studies: (1) magnetic resonance imaging (MRI) to analyze the ventricular size of the patients and the extension of edema at the periventricular white. (2) Magnetic resonance
spectroscopy (MRS) to analyze the chemical content and metabolism of the brain tissue and convert it into Chemical shifting imaging (CSI) to access the degree of brain atrophy and neuronal death. (3) Measuring of regional cerebral blood flow (rCBF) with Xenon enhance computed tomography (Xenon /CT) to detect the ischemic changes at the periventricular whitematter. (4) Evaluation of Karnoffsky scale, qualified gait measurement and hydrocephalus scale of the patient to analyze the prognosis of the patients with shunt surgery.
These studies were performed before the shunt surgery and at a month after the surgery. Additional evaluations of Karnoffsky scale, qualified gait measurement and hydrocephalus scale were performed at 3 months after the shunt surgery.
2. Selection of the patients
The inclusion criteria of the patients were: (1) Age between 45-75 years old of either sex. (2) Patients with clinical manifestations as unsteady gait, urinary
incontinence, and mental retardation. (3) Routine CT scan of the patient revealed enlarge d ventricular system with transependymal absorption of the cerebrospinal. However, patients with brain tumor to cause obstructive hydrocephalus will be excluded. (4) Patients enrolled in this study should have good consciousness to be cooperative during all the diagnostic procedure. (5) Patients with a history of previous surgery for clipping of intracranial aneurysm or implantation of cardiac pacemaker should be excluded. (6) Patients with poor pulmonary function or using ventilator should be excluded.
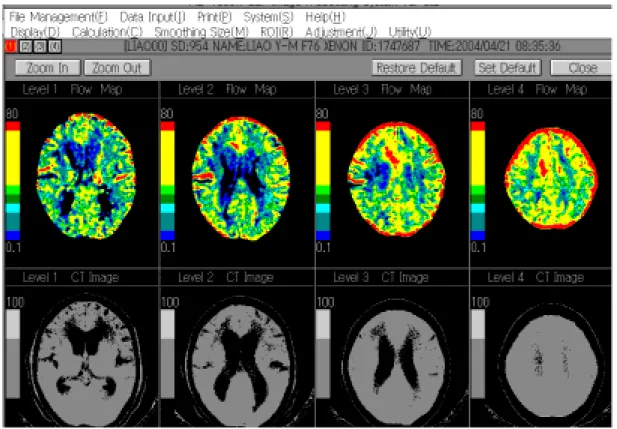
3. Measurement of regional cerebral blood flow.
Xenon enhanced CT method by the using of a Picker 1200SX CT scanner was adopted in this study for the measurement of cerebral blood flow. The patients underwent this measurement were fasted for 2 hours and their blood pressure, hematocrit and pulmonary function were checked. A mask was applied to allow the
patient to inhale room air for baseline measurement. The average of data from two consecutive baseline CT studies was used as the baseline data to minimize error. Then, the inhaled air was shifted to a mixture of 30% xenon, 30% oxygen and 40% room air. Three sets of CT scan were taken at 1 minute, 3 minute and 5 minutes after the
inhalation of this gas mixture to obtain the wash-in and wash-out curve of xenon gas. Regions of interest (ROIs) with a diameter of 1 cm were selected on 4 different axial cuts of the CT scan. A total of 16 ROIs were selected from various corresponding
anatomical locations of both hemispheres including: frontal cortex, temporal cortex, parietal cortex, occipital cortex, white matter anterior to the frontal horn, white matter medial to the frontal horn, white matter lateral to the frontal horn.
The concentration of xenon calculate from the CT number of various ROIs was obtained. According to Fick’s principle and Kety-Schmidt equation described
elsewhere, software formulated for the calculation of rCBF was applied. In addition to the calculated rCBF from different ROIs, a flow map was
generated from color scale. This flow map was used for the comparison to MRI and CSI.
4. Magnetic resonance spectroscopy an chemical shifting imaging
In the present study, a GE signa 1.5T MRI system and a Proton Brain Exam PROBE Spectroscopy software were used for proton MRS. An additional low-pass birdcage resonator was also used for the detection of proton at the frequency of 89-MHz. A self-shielded gradient coil is applied on the patient’s head during the procedure. The areas corresponding the ROIs chosen in xenon CT/CBF study are also selected as areas of interest (AOIs) in the study for MRS and CSI. The volume of each AOI is designed as 1.5x1.5x1.5mm voxel. Thus, each ROI in the flow study will be inside its AOI of CSI study.
Two TE acquisition techniques are used for regional MRS analysis: (1) LongTE acquisition (TR: 1 sec, TE: 135 or270msec.) for the detection of choline (Cho), creatine(Cr) and N-acetyl aspartate (NAA). (2) Short TE acquisition (TR:1 sec, TE:30 msec) for glutamine and glutamate. After obtaining proton-MRS, the automatic MAP shim software will formulate an orthogonal scout image. This image will store in an UNIX workstation and through two processes of Fourier transfer and summation of peak areas by Gassian function, the chemical changes in each AOI will be transfer into image. This image can again overlapping with MRI to show the chemical metabolism in various anatomical location of the brain.
6. Data analysis
The differences of changes of rCBF on the ROIs, the CSI on the AOIs, gait analysis, hydrocephalus scale and Karnoffsky scale of the patients at before the surgery and 1 month after the surgery are tested with Scheffe-F-test. The correlation among rCBF, CSI and the patient’s outcome are tested by ANOVA.
Results:
A total of 25 patients were enrolled during the study period. There were 16 males and 9 females. Their age ranged from 58 to 81. The average preoperative qualified gait analysis was 22.6 + 0.7 and average hydrocephalus scale was 8.01 + 2.95. Regional cerebral blood flow measurement before the surgery was 18.5 + 9.3 ml/100gm/min at the periventricular white matter and 28.9 + 11.3 ml/100gm/min at the frontal cortex. The preoperative CSI study revealed a 55.8 + 21 4 % reduction of the NAA at the periventricular white matter. According to this result, the studied patents were further divided into two groups: (A) Patients with >40% NAA reduction and (B) Patients with <40 % NAA reduction. The average NAA reduction in group A was 70.3 + 18.9 % and 29.3+10.1 % in group B (p=0.037). The calculated rCBF at periventricular white in these two subgroup were 27.7 + 9.3 ml/100gm/min in group A and 33.7 +10.5 ml/100gm/min (p=0.31).
The postoperative qualified gait analysis was 67.3 + 20.1 in group A and 35.6 + 10.4 in group B (p=0.033) and the average hydrocephalus scale was 6.72 + 2.14 in group A and 3.32 +1.51 in Group B (p=0.025).
Discussion:
From this preliminary report, the patients presenting with the triad of
hydrocephalus had a generally reduced rCBF. However, there are different degrees of reduction of the NAA level detected by MRS. The patients with flow reduction as well as NAA reduction had a poorer clinical outcome (group A). This phenomena probably indicating an irreversible change, i.e. brain atrophy, in this group of patients. On the other hand, patients with rCBF reduction and a high NAA level probably has some degree of ischemia caused by the compression from dilated ventricle, however, most of the neuron are vital and this change can be reversed by shunting procedure. We wish that through this study we would develop a reliable method for the differentiation of these two diseases of similar clinical manifestation but entirely different prognosis.