行政院國家科學委員會補助專題研究計畫
█ 成 果 報 告
□ 期中進度報告
(計畫名稱)
發展醫學生問題導向學習評估工具並分析影響表現的因子
計畫類別:█ 個別型計畫 □ 整合型計畫
計畫編號:NSC 96-2516-S-039-002- (3/3)
本年度計畫執行期間:2007 年 08 月 01 日至 2008 年 07 月 31 日
總計畫執行期間:2005 年 08 月 01 日至 2008 年 07 月 31 日
計畫主持人:林妍如
共同主持人:陳家玉
計畫參與人員:陸希平、許彤筵
成果報告類型(依經費核定清單規定繳交):□精簡報告
█完整報告
本成果報告包括以下應繳交之附件:
□赴國外出差或研習心得報告一份
□赴大陸地區出差或研習心得報告一份
□出席國際學術會議心得報告及發表之論文各一份
□國際合作研究計畫國外研究報告書一份
處理方式:除產學合作研究計畫、提升產業技術及人才培育研究計畫、
列管計畫及下列情形者外,得立即公開查詢
□涉及專利或其他智慧財產權,□一年□二年後可公開查詢
執行單位:中國醫藥大學
中 華 民 國 2008 年 10 月 31 日
摘 要
問題導向學習 (PBL)係以學員小組討論實際案例為中心的學習方式,並以分析、解釋 與解決問題為目標。這種學習模式已廣泛施行於國內外各大醫學院多年,許多因子會影響 學員在PBL 中的表現與學習成效。 試圖找出評估學員在 PBL 學習表現中的重要面向,進而建立評估學員在 PBL 學習表 現的工具。以及評量學員在PBL 學習表現工具的主客觀性,信效度及可行性。接下來分析 學員個體的個性特質如何影響問題導向學習的效果,進而對於日後學員的分組與老師的選 擇提供較佳的預測模式。 以中部某一醫學大學93 年度 124 位醫學系五年級學生為研究樣本,在 PBL 課程後進 行學員同儕評估,學員個性自評量表 (Big-5 44 項短問卷),以及學業成績(前 4 年)等資料 的收集,以了解學員個性與知識特質對 PBL 學習表現的影響。 針對PBL 表現同儕及導師對學員的評估經主成份分析 (Eigenvalue >1) 分別得到 5 個 (分別命名為控制領導、協助/協同、遵守規定、觀察思索與妥協),及 2 個(堅持與權變) 可 命名的主成份(根據因素負荷量判斷)。將此評量構面與 PBL 學員個性及知識特質間進行分 析顯示學員的守紀律個性特質與知識水準和其在PBL 課程中的控制領導角色扮演呈現正相 關 (p<0.05),而學員的交際性個性特質與其在 PBL 課程表現中的協助協同與遵守規定呈統 計明顯之正相關(p<0.05)。另外,學員想像力的個性特質則與其在 PBL 課程中表現遵守規 定的角色有統計明顯的正相關(p<0.05)。 本研究結果證明醫學生部份個性特質及知識水準與醫學生在 PBL 課程中表現的差異 性,此可提供醫學教育者在實施PBL 課程時,從學員本身特質來規劃其在團體中的角色, 並提供教師在學員表現上一套完整而客觀的方法。未來需更多資料與更長的時間觀察這些 因素間的因果相關性。 關鍵詞: 問題導向學習,醫學教育,個性特質,學習表現。Abstract
Problem based learning (PBL), a student-centered and small group discussion approach to analyze, explain and solve the problem. This learning model has been implemented in all medical universities in Taiwan for years. There are many factors being reported to influence the performance in the PBL course. To discover how the personality, knowledge, and tutors’ performance would influence the performance of medical students in the PBL curriculum.
A total of 124 undergraduate medical students participated in this survey. The personality was self-assessed by 44-itemed Big Five factors. The knowledge was assessed by their score point average (SPA) in the previous four years at the medical school. The performances of students in PBL curriculum were assessed by peers and tutors, with the use of two newly developed, reliable and validated evaluation sheets. The specialists content validity and the consistency reliability of related measures were tested.
The principal components (Eigenvalue >1) of the PBL performance evaluated by peers or tutors were analyzed as five (control/lead, assist/coordinate, obey rules, observe/think and compromise) and two (insist on rules vs flexible) major independent factors respectively. The specialists (n=5) content validity coefficient (Vi) for the PBL evaluation sheet (5-point scale) ranged from 0.8 to 0.95 (p<0.05). The consistency reliabilities of the Big-Five personality questionnaire were analyzed and deleted discordant items (Crobach’s Alpha= 0.67 to 0.82 after selection). The relationships between the personality/knowledge characters and the PBL performance, analyzed by stepwise regression, showed that the conscientiousness personality and knowledge (SPA) are positively related to the control/lead character in PBL, and the extraversion is positively related to the obey-rule character in PBL. The agreeableness and conscientiousness personality are positively related to the SPA.
The knowledge and personality characters appear to influence the performances of students in PBL. The students PBL performance evaluated by peers have more discriminate power than these evaluated by tutors. More samples will be required to get more reliable results. Implications are drawn regarding the future development and application of this assessment tools in medical schools.
Keywords: problem-based learning, medical education, personality factors, learning outcome
Preface
Introduction ………. 5
Methodology ………. 5
Results ……… 7
Discussions ………10
Conclusion ……… 12
References ………. 14
Acknowledgement ……… 17
Introduction
Problem based learning (PBL), a pedagogic concept using problems in context through
student-centered and small group discussion approach, has been adopted in varying extents for years in all eleven medical institutes in Taiwan. Much evidence have shown that a number of factors can seriously affect student performance in PBL courses, such as the design of PBL scenarios, characters of the tutors or the students’ attitudes and efforts.
Methodology
Study subjectsTo examine how the personal characters or knowledge base of the Taiwanese medical students influence their performance in a hybrid-PBL curriculum. A total of 309 (234 male, 75 female) high-school entry undergraduate medical students participated in this survey.
Instruments
Self-assessed personal traits were presented in a 44-item questionnaire with a Big- Five factor structure. Knowledge base was assessed by the score point average (SPA) based on their previous four- year education in the medical school. Peer-assessed performance of students in PBL curriculum was carried out using a well-developed, reliable, and validated evaluation form.
Big-five personality factors Paper-and-pencil measures were included in our study to evaluate the personality variables. The Big five personality test, a modified form of the Myers-Briggs Type Indicator (MBTI), has been used worldwide for over 10 years in many research fields with satisfactory reliability and validity. It includes the following five dimensions: 1) extraversion vs. introversion. Extraversion means a person is talkative, sociable, and assertive. 2) agreeableness vs. antagonism. Agreeableness means a person is good natured, cooperative, and trusting. 3) conscientiousness vs. undirectedness. Conscientiousness means a person is
responsible, orderly, and dependable. 4) neuroticism vs. emotional stability. Neuroticism means a person is anxious, prone to depression, and worries a lot. When this score was reversed in the following analysis, it was renamed “emotional stability.” And 5) open to experience vs. not open to experience. Openness means a person is imaginative, independent minded, and has ability to think divergently. A modified 44-item questionnaire was used and the items were scored on a Likert 5-point scale ranging from 5, strongly agree to 1, strongly disagree. The “negative” trait items were reverse-scored so that high scores indicate more positive traits.
Peer evaluation of student performance Students evaluated their peers in each group at the end of this course. The assessment had two major dimensions: first, contributions to group missions and goals; second, interpersonal skills which were verified by five tutors
well-experienced in PBL before performing the survey.
Peer evaluation of student performance- missions and goals The achievement of missions and goals in group learning task often relates to the following characters of
content-related role-play: 1) The initiator-contributor, who often suggests new ideas or sorts out directions in the course of PBL discussion. For example, the initiator may challenge: “How do we treat pulmonary emphysema patients who are refractory to medical treatment”. In response to the question, a contributor may suggest the flow of direction by asking: “It is reasonable to consider the lung volume reduction surgery or pulmonary transplantation”. 2) The answer
seeker/giver, who tends to seek or offer a correct answer to a question in the PBL tutorial
discussion. For example, an answer seeker may ask simple and direct question: “ What’s the normal pH value of a human arterial blood sample?” The answer giver will respond directly with an answer. 3) The opinion seeker, who tends to challenge and/or offer comments to add more values to the information. For example, an opinion seeker may comment: “Some reports in the literature emphasize the value of video-assisted thoracic surgery, in the treatment of empyema”. They may also respond to further such comment: “Evaluation using evidence-based principles (level of evidence, level of recommendation) shows the level of understanding of their learning results.” 4) The elaborator, who explain a concept by actual and adequate examples or metaphors. For example an elaborator may respond to a question such as: “What is lung compliance?” by elaborating as the following “You can think of the lung as a balloon. If you can blow the balloon up easily, its compliance is said to be high.”5) The coordinator, who can summarize different opinions within a group to formulate a consensus. For example, during debates about treatment options for urethral stones, the coordinator may weigh the condition of this patient and the proposed treatment plans, and then describes a cost-effectiveness treatment strategy for the benefit of the patient. 6) The orientator, who can direct the pace and issues effectively to help members adequately adhering to the proper course of learning. 7) The evaluator, who comments on the contents and process of learning and offer feedback for further improvement as an
individual or as a group. 8) The energizer, who showed enthusiasm and passion in the group process via facilitation and encouragement and persistently helped the group to reach consensus within the group. 9) The scribe, who records the content and process of learning during the discussion. A scribe may also prepare reports or summaries on behalf of the group.
Peer evaluation of student performance- interpersonal skills 1) Encourager. A member
who encourages and appreciates other colleagues’ comments or attitudes. 2) Harmonizer. A member who intervenes in the conflict or disagreement between other members. 3) Compromiser. A member who maintains group harmony. 4) Gatekeeper. A member who maintains the balance
of opinion expression among members. 5) Standard setter. A member who reminds the other members of the need to meet the goals and follow the rules. This behavior is usually observed at the feedback stage. 6) Group observer. A member who analyzes the interactions of the members, and this is also observed at the feedback stage.
Peer evaluation of student performance Two points or 1.5 points were added to the score of any student rated “the best” or “second best,” respectively, in a particular item. The score of each student for a particular item was the sum of the scores given by their peers. Then the group sum for each item was calculated, and the ratio of each student score for an item to the group score for that item was calculated to correct for inter-group differences in response (standardization).
Score point average (SPA) SPA over the last 4 years at the university was used. The grades (scores) were separated on the basis of content courses (e.g., basic and clinical medical courses) and method courses involving memory (e.g., anatomy), operation (e.g., chemistry lab course), and reasoning (e.g., physics). These scores were weighted on the basis of the number of teaching hours, and the average score of the above three groups of subjects for every student was calculated for analysis.
Analyses and statistics
Internal consistency reliability was measured in the Big-five personality evaluation. Content and construct validity of the PBL evaluation sheets were tested. PBL performance (peers evaluation) and SPA were subjected to principal components analysis. The mean and standard deviation of scores was determined. The response rate was defined as the ratio of the number of respondents to the total number of members in this group. The purpose of the ratio of the scores used in the peer evaluation, described above, was to minimize differences in response rates between groups. Simple correlation between items of the revised evaluation sheets, between peer evaluations and Big-five personality or SPA were obtained. Big-five personality factors and SPA were used to predict student’s performance (rated by peers and the tutor). Factors were included or excluded step-by-step in this analysis. The statistical tests were performed by using SPSS 13.0 and Excel for Windows XP.
Results
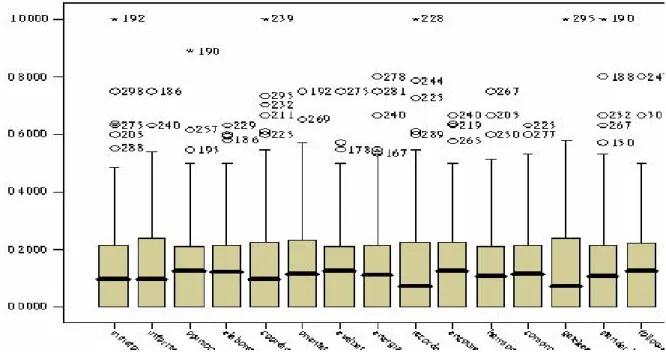
Descriptive Statistics for PBL Performance (Fig. 1)
Peer-evaluated PBL performance scores were standardised and ranged from 0 to 0.63 (elaborator and compromiser) to 1.00 (information seeker, coordinator, recorder, gatekeeper and standard setter), with the median value ranging from 0.095 to 0.139. Response rates for the 44 groups ranged from 0.75 (recorder) to 0.85 (opinion seeker).
Figure 1. Boxplot distribution (Boxplot) of scores of peer evaluation (n = 309). Descriptive Statistics of Big Five Personality Factors (Fig. 2) and SPA (Table 1)
Two hundred and sixty-three students (85.1%) completed the Big Five personality questionnaire. The mean and standard deviation of each item and dimension (before exclusion of items) is listed in Figure 2. Three hundred and one students (97.5%) had SPA information, and the mean value and standard deviation was 77.5 ± 7.2 (range, 60.2- 90.7) (Table 1).
Reliability of the Big Five Personality Questionnaire
The Cronbach’s alpha values of the original 44-item, 5-dimension questionnaire ranged from 0.6594 to 0.7662. These values increased from 0.7008 to 0.7662 after deletion of 2 items. The reliability of this questionnaire improved after this deletion, and the revised data could be applied to subsequent correlative study on the students’ PBL performance.
Table 1. Descriptive statistics of SPA (n=301) (97.5%)
Total score (∑ Score * credit hrs)
Dimensions Minimum Maximum Mean±SD
No. credit hrs. Average score (range) Common/memory 511 807 697±59 9 77.4 (56.8-89.7) Calculate/reasoning 791 1273 1061±93 14 75.7(56.5-90.9) Common/operation 572 721 673±29 8 84.1(71.5-90.1) Basic/memory 3097 4960 4128±446 53 77.9(58.4-93.6) Basic/operation 608 798 737±35 9 81.9(67.6-88.7) Clinical/memory 1504 2205 1928±148 25 77.1(60.2-88.2) Total 7104 10701 9148±78 118 77.5 (60.2-90.7)
Evaluations
One hundred and 21 students effectively completed the test-retest reliability test of PBL
performance by peer evaluation. These ranged from 0.4889 (compromiser) to 0.8282 (initiator).
Content Validity of the PBL Performance Evaluation Sheet The content validity (Vi) of the
15-item PBL performance evaluation sheet (from 5 evaluators) ranged from 0.80 to 0.95 (significantly powerful at the 0.05 level). The mean score of each item (using a Likert 5-point scale) ranged from 4.2 to 4.8, with standard deviation of 0.45 to 0.84.
Factor Analysis of the PBL Performance Peer-evaluation Sheets
Factor analysis identified 4 mutually independent principal factors: assist-coordinate (PC No. 1) with 7 highly correlated items in which the loading values ranged from 0.439 (information seeker) to 0.758 (coordinator), control-lead (PC No.2) with 5 highly correlated items in which the loading values ranged from 0.578 (elaborator) to 0.762 (opinion seeker), written organisation (PC No.3) with 2 related items named recorder (0.850) and follower (0.491) and compromise-comply (PC No. 4) with only 1 related item (compromiser, loading value 0.829).
Factor Analysis of the SPA
Factor analysis of SPA found only 1 principal component (loading value ranging from 0.163 to 0.214). In Taiwan, most medical schools still use the written test, which mainly assesses the content knowledge of students, to determine the performance of their students. This score may therefore not properly reflect their true abilities in the tested subject. Thus, a variety of abilities, such as operational, reasoning or calculation, which should be emphasised in some experimental or specific basic sciences (such as physics, calculus) courses, cannot be measured through these tests.
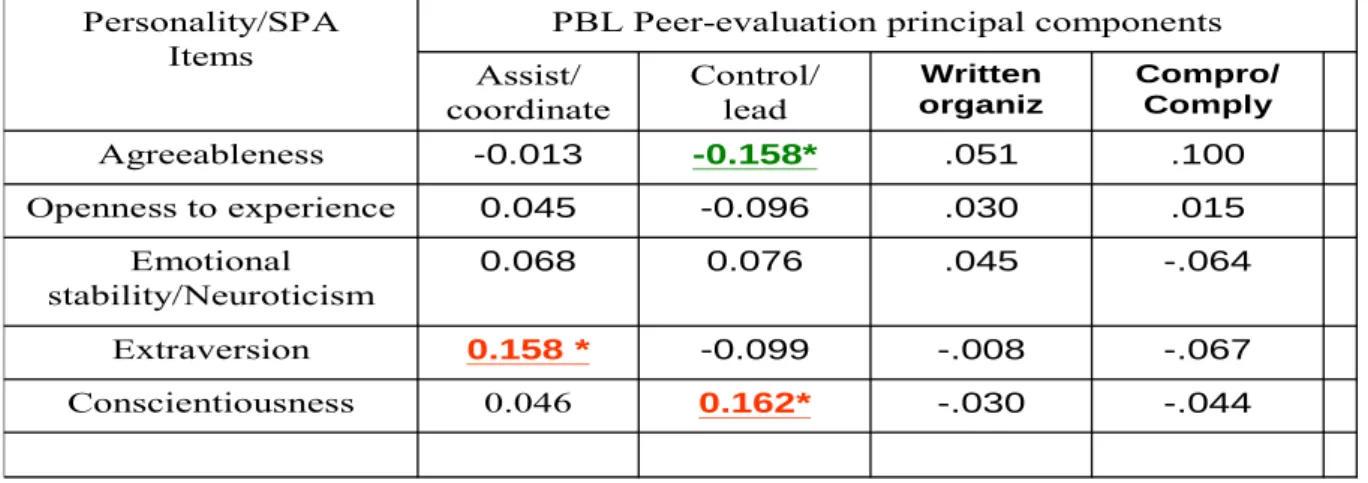
Simple and Stepwise Regression Between the Personality/SPA and PBL Performance (Table 2 and 3)
Simple correlation between personality/SPA and peer-evaluated performance (Table 2) showed that “extraversion” and “openness to experience” were positively related to the
“assist-coordinate” characteristic in PBL performance, and “conscientiousness” was positively related to the “control/lead” characteristic in PBL performance (P <0.05). The SPA was
positively related to “assist-coordinate” and the “control-lead” characteristic in PBL performance (P <0.05). The “agreeableness” was negatively correlated with the “control-lead” characteristic in PBL performance (P <0.05). After stepwise regression between the Big Five
and each component of PBL performance, only the correlation between conscientiousness and control/lead and between extraversion and assist/coordinate remained significant (Table 3).
Table 2. Relationship between personality/SPA and peer-evaluated student performance
Table 3. Stepwise regression between personality and peer-evaluated student performance
Discussions
PBL Performance Evaluation
Our studies modified the role play in the small group learning in previous literature to design a new evaluation sheet of students’ PBL performance in the medical school. In our present study, the 15- item evaluation sheet has been verified by five specialists in the field of medical
education. To test the α-value stability of these evaluation sheets, we proceed a test-retest
.022 .045 .443* .161* GPA principal components -.044 -.030 .162* -.021 Conscientiousness -.067 -.008 -.037 .158* Extraversion -.064 .045 .048 .092 Emotional stability/Neuroticism .015 .030 -.040 .132* Openness to experience .100 .051 -.145* .004 Agreeableness Compro/ Comply Written organiz Control/ lead Assist/ coordinate
PBL Peer-evaluation principal components Personality/SPA Items -.044 -.030 0.162* 0.046 Conscientiousness -.067 -.008 -0.099 0.158 * Extraversion -.064 .045 0.076 0.068 Emotional stability/Neuroticism .015 .030 -0.096 0.045 Openness to experience .100 .051 -0.158* -0.013 Agreeableness Compro/ Comply Written organiz Control/ lead Assist/ coordinate
PBL Peer-evaluation principal components Personality/SPA
reliability evaluation since this year, and the preliminary results were satisfactory.
Then we performed factor analysis about these 15 role play item to extract four mutually independent principal components (PCs). These PCs can be properly named according to their factors components and loadings as described in the Fig. 3. In our proceeding studies, we have collected much more samples for similar analysis and noted that the previous classification and nomenclature of these PCs was consistent and reliable. Our results disclose the multidimensional factor structure of PBL performance. We think that this carefully constructed evaluation sheet is not only a tool for conducting an objective and multidimensional assessment but also a means of reminding the members in this course to regulate their roles.
The other important benefit of PC analysis is the subtraction and mutually independent variables will make the subsequent comparison between their correlations with many other variables, such as personality or knowledge characteristics, simpler and more reliable.
Furthermore, we found that (not described in this paper) peer evaluation provides more valuable and discriminative information about student performance than our previous literature about the tutor evaluation. Tutors, and to a lesser extent peers, in PBL curricula are usually reluctant to give low scores to students and thus tend to give higher, less discriminative scores than is justified.
The other benefit of establishing this PBL performance evaluation is achieving feedback from self and group members. Reviewing in literature, students in the PBL can not only learn the concepts of PBL through feedback evaluation using this evaluation sheet after the course, but also learn more objective evaluation methods in this course.
Personality vs. PBL performance
Research has shown a linkage between personality and performance8, 30 and between knowledge and performance of pre- and post-graduates.23,34 Our results described how to modify the
personality (Big-five) evaluation sheets and their correlations with the PBL performance. In this study we used the investigated sample for items selection/deletion in the same dimension. We delete only a very small number of “discordant” items to get better consistent reliability (the higher Cronbach's alpha value in the Table II). In this study we also found that some personality characteristics, such as conscientiousness and extraversion, can influence performance.
The negative correlation between the agreeableness and control/lead performance in PBL is puzzling, yet may be explained that “respect others’ opinion” might obstacle the control of session in PBL, and that will lead to be recognized as a weaker control/lead performance. Through this and our ongoing studies, we can establish and compare these databases and realize the influences of personality not only in the individual student's performance of the PBL, but
also the group dynamics and their future career development. These results can provide us guidelines to help the students not only in the PBL courses but also in other aspects of their learning in the school.
Knowledge vs. PBL performance
There were still some study limitations in this study. Grade point average (GPA) has been widely applied as the students'knowledge indicator in previous literature. In this study we used the score point average (SPA) to replace the GPA because there were cultural differences between the Asian and Euro-American countries. We realized the differences between the subjects, some of them emphasize the ability of reasoning and calculation (such as calculus and physics), some others emphasize the ability of memory (anatomy), and some others emphasize the ability of operation (experiment or bedside practice).
However, since most of the course in the Asian countries still use written test as one of the important methods to evaluate the students'performance, thus the PCs would be difficult to extract not because of the contents of the courses themselves, but the methods of evaluation. In our school, the curriculum reform has been undergoing, including the reform of evaluation
method. Content knowledge would not be the only determinant to evaluate the ability of a student, but also the ability of search, integration, application and actual operation, which would be
replace the former as the main criteria for evaluation.
The other limitations in this study are the number and the representatives of these samples are insufficient. Now we have proceeded a 3 year medical education research project supported by the National Science Council in Taiwan and has recruited this study as one of the important missions in these years. We collaborate with two other medical schools in Taiwan and investigate more medical students for the future survey. In our proceeding study we have added the tutor and self evaluation to compare the reliability of the peers'evaluation, and this “360 degree
assessment" by all related members will be more objective.
Conclusion
In this study we developed a new evaluation sheet for PBL performance. In the future, we should perform related activities: 1) Compare results between different PBL curricula (focused on basic, clinical, or other topics). 2) Collect more samples from other students taking the same course. 3) Collect samples from other medical schools and compare their differences. 4) Develop methods to evaluate inter-group differences. Group dynamics (such as leaderless group discussion [LGD] dynamics) or demonstrations of individual abilities (such as ability to analyze cases and simulate
interviews) should be recorded for evaluation by third-party specialists. We believe that a reliable and valid method of evaluation of PBL as well as predictive models of individual performance or future career success can be developed in the future with the use of personality, knowledge, and other variables such as the tutor characteristics. Through these models, group composition can be optimized so as to lead to the most effective group dynamics.
References
1. Walters MR. Problem-based learning within endocrine physiology lectures. Adv Physio Edu 2001; 25: 225-7.
2. Dolmans DH, Gijselaers WH, Moust JH, et al. Trends in research on the tutor in
problem-based learning: conclusions and implications for educational practice and research. Med Teacher 2002; 24: 173-80.
3. Michel MC, Bischoff A, Jakobs KH. Comparison of problem and lecture based pharmacology teaching. Trends Pharmacol Sci 2002; 23:168-70.
4. Epstein RJ. Learning from the problems of problem-based learning. BMC Medical Education. 2004; 4: 1.
5. Armstrong EG, Machkey M, Spear SJ. Medical education as a process management problem. Acad Med 2004; 79: 721-8.
6. Carrera LI, Tellez TE, D’Ottavio AE. Implementing a problem-based learning curriculum in an Argentinean medical school: implications for developing countries. Acad Med 2003; 78: 798-801.
7. Newton H. Telemedicine in educational settings. Nursing standard 2003; 17: 75-8.
8. Morgan J, Whelan L. Problem based learning: pyrexia of unknown origin? Accid & Emerg Nurs 2003; 11: 131-40.
9. Ogrinc G, Headrick LA, Mutha S, et al. A framework for teaching medical students and residents about practice-based learning and improvement, synthesized from a literature review. Acad Med 2003; 78:748-56.
10. Wood DF. Problem based learning. BMJ 2003; 326: 328-30.
11. Stratman E, Dyer J. Problem-based learning: an approach to dermatology resident education. Arch Dermatol 2002; 138: 1299-302.
12. Beard JD, Robinson J, Smout J. Problem-based learning for surgical trainees. Ann Royal Coll Surg Engl 2002; 84: 227-9.
13. Williams B. Developing critical reflection for professional practice through problem-based learning. J Adv Nurs 2001; 34: 27-34.
14. Azer SA. Problem-based learning. Challenges, barriers and outcome issues. Saudi Medical J 2001; 22: 389-97.
15. Azer SA. Problem-based learning. A critical review of its educational objectives and the rationale for its use. Saudi Med J 2001; 22: 299-305.
16. Johnston AK, Tinning RS. Meeting the challenge of problem-based learning: developing the facilitators. Nurse Edu Today 2001; 21:161-9.
17. Doran GA. Reviewing the role of educational domains and problem-based learning in dental curricula. Part I. SADJ 2000; 55: 433-5.
18. Price A, Price B. Problem-based learning in clinical practice facilitating critical thinking. JNSD 2000;16: 257-64.
19. Haith-Cooper M. Problem-based learning within health professional education. What is the role of the lecturer? A review of the literature. Nurs Edu Today 2000; 20: 267-72.
21. Spencer JA, Jordan RK. Learner centered approaches in medical education. BMJ 1999; 318: 1280-3.
22. Sweeney G. The challenge for basic science education in problem-based medical curricula. Clin Invest Med 1999; 22: 15-22.
23. Maudsley G. Do we all mean the same thing by “problem-based learning?” a review of the concepts and a formulation of the ground rules. Acad Med 1999; 74: 178-85.
24. Zeitz HJ. Problem based learning: development of a new strategy for effective continuing medical education. Allergy & Asthma Proc 1999; 20: 317-21.
25. Casassus P, Kivon R, Gagnayre R, d’Ivernois JF. An initial experiment in hematology isstuction using the problem based learning method in third year medical training in France. Hematology & Cell Therapy. 1999; 41: 137-44.
26. Luh, SP. The definition, classification, and casualty relationship of disease: from the medical logical viewpoint. Med Edu 1999; 3: 399-404.
27. Luh, SP. Creation of Small Group Teaching. Med Edu 1999; 3: 416-18.
28. Luh, SP. The Diagnostic Process, from the Medical Logical Viewpoint. Med Edu 2000; 4: 198-205.
29. Luh, SP, Wang, NP, Yang PM. Screening Blood donations for hepatitis C in central Africa: analysis of a risk and cost based decision tree. Med Edu 2003;7: 74-78.
30. Luh SP, Su HC. The importance of small group problem based learning in medical technical-occupational education. Med Edu 2002; 6: 348-52.
31. Luh SP, Chen JY. The application of evidence based medicine. Chung-Shan Med J 2004 (in press).
32. Luh SP, Chen JY, Chou MC. The role of students and tutors in the PBL. J Med Edu 2004 (in press).
33. Luh SP, Chen JY, Chou MC. The logical thinking of history taking and diagnostic reasoning. J Med Edu 2004 (in press).
34. Luh SP, Lin YR, Chen JY, Chou MC. The application of item response theory. J Med Edu 2004 (in press).
35. Das M, Mpofu DFS, Hasan MY, Stewart TS. Student perceptions of tutor skills in problem based learning tutorials. Med Edu 2002; 36: 272-8.
36. Roche WP, Scheetz AP, Dane FC, Parish DC, O’Shea JT. Medical students’ attitudes in a PBL curriculum: trust, altruism, and cynicism. Acad Med 2003; 78: 398-402.
37. Eshach H, Bitterman H. From case-based reasoning to problem based learning. Acad Med 2003; 78: 491-7.
38. Doman T, Bosthuizen H, Cordingley L, Hidder S, Hadifield J, Scherphier A. Evaluation of self directed clinical education: validation of an instrument. Med Edu 2004; 38: 670-7. 39. McLean M. What can we learn from facilitator and student perceptions of facilitation skills
and roles in the first year of a problem based learning curriculum? BMC Med Edu 2003; 3: 9-14.
40. Correa BB, Pinto PR, Rendas AB. How do learning issues relate with content in a problem-based learning pathophysiology course? Adv Physio Edu 2003; 27: 62-9.
41. Leung KK, Lue BH, Lee MB. Development of a teaching style inventory for tutor evaluation in problem-based learning. Med Edu 2003; 37: 410-6.
42. Zeithaml VA, Bitner MJ. Service marketing integrating customer focus across the firm. McGram-Hill Companies, Inc. 2nd Ed, 2002, Boston.
43. 余民寧. 試題反應理論的介紹 (一): 測驗理論的發展趨勢. 研習資訊 1991;8(6): 13-18. 44. 余民寧. 試題反應理論的介紹 (二): 基本概念與假設. 研習資訊 1992;9(1):5-9.
45. 余民寧. 試題反應理論的介紹 (三): 試題反應模式及估計. 研習資訊 1992;9(2):6-10. 46. 吳孟勳, 李富民: A research on applying fuzzy set theory and item response theory to
Acknowledgement
The authors gratefully acknowledge the project support from the Taiwan
NSC-95-2516-S-040-003, and sincerely our great honors to achieve the“Best Poster" awards (No. BP-11) in the 4th APMEC, Year 2007 in Singapore.
Publication in the three-year periods
1. Luh SP, Yu MN, Tsao TCY, Chen JY., 2007. The Influence of Personality and Knowledge on the Performance of Medical Students in the Problem Based Learning Curricula.測驗學刊 2008(in press). (TSSCI).
2. Luh SP, Yu MN, Lin YR, Chou MJ, Chou MC, Chen JY., 2007 Sep. A study on the personal traits and knowledge base of Taiwan medical students following problem-based learning instructions. Ann Acad Med Singap, 36(9):743-50. (SCI)
3. Luh SP, Lin YR, Chen JY., 2007 Sep. Application of Big-Five Personality Questionnaire Survey for Medical Students: Pilot Investigation. RESEARCHES IN MEDICAL
EDUCATION, 6(9):863-866 873.
4. 陸希平。醫學教育未來發展重要趨勢- 2007 亞太國際醫學教育之重要資訊 (上)。西北醫 學教育 2008 (in press).
5. 陸希平。醫學教育未來發展重要趨勢- 2007 亞太國際醫學教育之重要資訊 (下)。西北醫 學教育 2008 (in press).
6. Luh SP, Wang BR, Chen JY., 2006 Jun. Problem Based Learning.醫學教育,10(2):89-97. 7. Luh SP, Lin YR, Chen JY., 2005 Jun. Content validity and factor analysis of the peer
evaluation sheet for problem based learning performance. 醫學教育,9(2):138-48.