Kaohsiung J Med Sci October 2005 • Vol 21 • No 10 441 Tooth transposition is defined as the positional interchange
of two adjacent teeth, particularly of the roots, or the development or eruption of a tooth in a position normally occupied by a non-adjacent tooth [1–3]. This dental anomaly, described as an interchange in the position of two permanent teeth within the same quadrant of the dental arch, is considered a relatively rare anomaly of unknown origin [4]. We need to exercise caution when diagnosing this condition, in order to avoid confusing it with mere ectopic eruption. In transposition, there is an exchange of positioning, thereby reversing the sequence in the mouth. Ectopic eruption is a broad category referring to any abnormal or aberrant eruptive position taken by a tooth. Tooth transposition, therefore, must be considered a subdivision of ectopic eruption: tooth transposition is an example of ectopic eruption, but few ectopic eruptions are tooth transpositions [5].
Tooth transposition is often accompanied by other dental anomalies. Hypodontia, developmentally missing, small or peg-shaped maxillary lateral incisors, severe rotations and malpositions of adjacent teeth, retained deciduous teeth, dilacerations, and malformation of other teeth have
C
ANINE
T
RANSPOSITION
Yu-Chuan Tseng,1 Hong-Po Chang,1,2 and Tsau-Mau Chou2
1
Department of Orthodontics, Kaohsiung Medical University Chun-Ho Memorial Hospital, Kaohsiung Medical University, and 2College of Dental Medicine,
Kaohsiung Medical University, Kaohsiung, Taiwan.
Transposition is described as an interchange in the position of two teeth within the same quadrant of the dental arch. Canine transposition is reportedly the most common transposition in human dentition. The incidence of maxillary canine-premolar transposition is reported to be 0.135–0.510%. Although the exact mechanism of canine transposition is unclear, it seems to be closely related to genetically influenced, retained deciduous canine, and a history of trauma. In this article, we focus on the classification, incidence, etiology, and treatment modalities of tooth transposition. We hope this information will help clinicians treating patients with this kind of dental anomaly.
Key Words: canine transposition (Kaohsiung J Med Sci 2005;21:441–7)
Received: April 15, 2005 Accepted: August 11, 2005 Address correspondence and reprint requests to: Dr. Hong-Po Chang, College of Dental Medicine, Kaohsiung Medical University, 100 Shih-Chuan 1st Road, Kaohsiung 80708, Taiwan.
E-mail: [email protected]
most frequently been reported in conjunction with transposition [4–8]. Canine transposition has been reported to be the most common transposition found in the human dentition [9,10].
C
LASSIFICATIONA distinction is made between complete and incomplete transposition. In complete transposition, both the crowns and the entire root structures of the involved teeth are found parallel to their transposed position (Figure 1). In incomplete transposition (also called pseudo or partial transposition), the crowns may be transposed, while the root apices remain in their normal positions (Figure 2) [4,11–13]. Alternatively, the crowns may be in the correct order, while the root apices are transposed. Thus, the two involved teeth overlap and their long axes cross each other. In addition, the crowns and roots of the two involved teeth may completely superimpose each other on normally projected radiographs.
Transpositions are classified according to Peck and Peck’s classification [14]: maxillary canine–first premolar (Mx.C.P1), maxillary canine–lateral incisor (Mx.C.I2), maxillary canine–first molar site (Mx.C to M1), maxillary lateral incisor–central incisor (Mx.I2.I1), maxillary canine– central incisor site (Mx.C to I1), and mandibular lateral
incisor–canine (Mn.I2.C). Aberrant positioning of the maxillary canine is a feature of four of the five types of maxillary tooth transpositions, the exception being the special situation of lateral–central incisor transposition. The maxillary permanent canine is the tooth most frequently involved in transposition. The canine shows the highest incidence of transposition with the first premolar, less often with the lateral incisor, rarely with the central incisor, and extremely rarely with the second premolar or first molar [3, 4,8,14].
Two of the five types of maxillary tooth transpositions cannot truly be defined as transpositions. Canine–first molar and canine–central incisor site “transpositions” represent extreme displacement and should, instead, be called ectopic eruptions [6] or transpositions of an extensive degree [15]. Joshi and Bhatt also used the term “extreme distal migration” to describe maxillary canine eruption distal to the second premolar [16]. Displacement of the tooth from one quadrant across the midline to the other side or physiologic migration of an unerupted tooth across the midline in the absence of pathology or trauma is referred to as transmigration [17], and has been reported in the mandibular and the maxillary arches. However, these should be considered ectopically erupted teeth, not transpositions [4].
I
NCIDENCE ANDE
PIDEMIOLOGYThe incidence of maxillary canine–premolar transposition is reported to be 0.135–0.510% [6,7]. In Japanese, the reported prevalence of tooth transposition is 0.065% in the general population [18,19] and 0.660% in orthodontic patients [18, 20]. Yilmaz et al found a prevalence of tooth transposition of 0.380% in a Turkish population [12]. Burnett reported that the prevalence of MxC.P1 transposition was 0.510% in an African population [21]. Buenviaje and Rapp reported a prevalence of transposed teeth of 0.080% in a population of 2,439 children aged 2–12 years [22]. In other reports, the frequency of transposition involving the mandibular canine and lateral incisor among 13,712 children aged 8–9 years was 0.030% [3,23].
Maxillary tooth transposition most frequently involves the canine with the first premolar, and less frequently involves the lateral incisor [2,6,24,25]. Females present with approximately 60% more transposition than males [6,14]. Most maxillary transpositions are unilateral with a higher involvement of the left side, particularly in canine–lateral incisor transposition [6,14,16]. Left-side predominance is suggested in unilateral cases [1,2,5,6,13,14,16]. Laterality is not uncommon in the expression of other orofacial anomalies. Subject handedness is not related to the side of
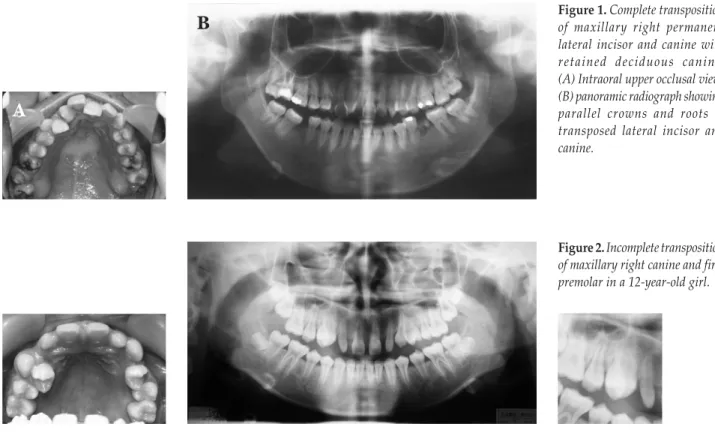
Figure 1. Complete transposition of maxillary right permanent lateral incisor and canine with retained deciduous canine. (A) Intraoral upper occlusal view; (B) panoramic radiograph showing parallel crowns and roots of transposed lateral incisor and canine.
Figure 2. Incomplete transposition of maxillary right canine and first premolar in a 12-year-old girl.
B
the transposition in unilateral cases [2]. Interestingly, transposition has never been observed in both jaws simultaneously, nor is transposition known to occur in the deciduous dentition [4,7]. A high incidence of associated dental anomalies, such as missing or small maxillary lateral incisors, missing second premolars, retained deciduous canines, impacted permanent canines and central incisors, and severe rotation of the adjacent premolars, is observed on the side of the transposition [1,2,5–7].
E
TIOLOGYThe etiology of tooth transposition is the subject of controversy and is still not completely understood. Suggestions outline various scenarios, which include variation in embryologic development, early loss of primary teeth, and prolonged retention of primary teeth [26]. Several theories have been proposed to explain the phenomenon. Multifactorial genetic factors and an interchange in the position of the developing dental lamina of the involved teeth are suggested causes [6].
A thorough review of the etiology of canine tooth transposition was carried out by Peck and Peck [14]. They found evidence to suggest that the maxillary canine–first
premolar transposition is genetically influenced [1,14,27– 29]. A polygenic cause is supported by the increased frequency of associated dental anomalies (Figures 3 and 4), such as tooth agenesis and peg-shaped lateral incisors, bilateral occurrence, familial occurrence, and significant differences between male and female prevalence. Heredity was offered as a possible explanation for this anomaly, especially when reported bilaterally in siblings [1,5].
Another theory suggests that a retained deciduous canine, observed in a large number of canine transpositions, might be the primary cause of the displacement and migration of the permanent canine from its normal path of eruption. Although not a true transposition, this migration theory may help to explain those extreme cases in which the canine erupts in the position of the central incisor, second premolar, or first molar [6]. Because retention of deciduous canines and lateral incisors is reported in most cases of canine transposition and impaction, it has been suggested that the long-term retention of deciduous teeth may be the primary cause of displacement of the permanent tooth from its normal path of eruption. Whether prolonged retention of a deciduous tooth causes displacement of its successor, or an abnormal path of eruption is the reason for retention of the deciduous tooth, is a matter of speculation [4].
Figure 4. Complete transposition of maxillary right permanent canine and first premolar. (A) Intraoral upper occlusal view; (B) panoramic radiograph showing parallel crowns and roots of transposed canine and first premolar. Note the congenital missing of lower left second premolar.
Figure 3. Bilateral complete
transposition of maxillary right permanent canine and first premolar. (A) Intraoral upper occlusal view; (B) panoramic radiograph showing congenital absence of upper and lower right lateral incisors.
B
A
B
Although patients with a transposed canine seem to have an increased prevalence of other dental anomalies, and there is a gender bias, we are unable to determine whether or not canine transposition has a genetic etiology. It is still unclear if transposition results from formation of tooth germs in an ectopic position, or if transposition results from the displacement of the follicle and tooth germ following formation. Bone pathology, such as cyst formation, may also cause displacement and transposition of the tooth. The etiology of the maxillary canine to lateral transposition appears to be adventitious. This kind of transposition results principally from dentofacial trauma in the deciduous dentition and subsequent permanent tooth drift [1,14], although a genetic basis for some occurrences cannot be totally excluded [30,31]. A history of trauma is often present, resulting in the distal disruption of the developing lateral incisor tooth germ. This leads to mesial migration of the canine. Trauma to the deciduous teeth has also been suggested as a factor in the etiology of transposition in reported cases where dilacerations of the permanent incisor roots were found adjacent to transposed teeth [4,6].
The canine transposes to the site of the central incisor by mesial migration. This occurs when the central incisor is lost (usually due to trauma) or displaced (e.g. by a supernumerary tooth). Yilmaz et al found a 50% history of trauma in maxillary canine to central incisor site transposition [12]. Therefore, the maxillary canine should be regularly monitored after trauma or early loss of maxillary central incisors [13]. On rare occasions, extreme distal migration of the canine to the site of the first molar has occurred when the deciduous canine is retained or the upper first permanent molar is lost early. In the mandible, when canine to lateral incisor transposition occurs, the deciduous canine is often retained and other dental anomalies may be present. The position of the lateral incisor and its often severe rotation suggests that this tooth migrates around an ectopic mandibular canine. In the mandible, the distal migration of the lateral incisor appears to be the primary reason for the developing transposition [4].
T
REATMENTC
ONSIDERATIONSFor discussion, treatment will be divided into interceptive and definitive treatment, although it is important to recognize that the two often overlap clinically. When cases of incipient transposition are detected early, they can sometimes be treated interceptively. When seen at later stages, the positions
of the root apices are important for decisions concerning where to move the transposed teeth [32].
Interceptive treatment
Early diagnosis of a developing transposition is based on thorough intraoral examination, followed by complete radiographic analysis, preferably between the ages of 6 and 8 years. This is especially important for early detection of malposed mandibular permanent lateral incisors. When incipient transposition is detected early enough, interceptive treatment should be initiated to remove retained mandibular deciduous teeth and guide the ectopic lateral incisor to its normal place in the arch. The space for the mandibular canine should be maintained while awaiting its eruption. This interceptive procedure will prevent the full development of transposition with the erupting permanent canine [2]. In the years after the age of 10, interception of a mandibular canine to lateral incisor transposition becomes far more difficult, because, during these years, the transposition tends to develop naturally into a total positional interchange of the affected teeth [3].
Definitive treatment
In definitive treatment, a number of factors need to be considered. These factors include the underlying malocclusion and the degree of crowding, the occlusion (both static and dynamic), the esthetic, the position of the root apices, patient motivation and suitability for treatment, length of treatment time, and the form of retention. There are three main options for definitive treatment: extraction of one of the transposed teeth, alignment of the teeth in the transposed position, and orthodontic movement of the teeth to their correct positions [33,34].
For Mx.C.P1 transposition, if the cuspid root lies distal to the first bicuspid root, the transposition should be accepted. Normally, a pleasing appearance can be achieved by leaving the teeth in the transposed position with less than ideal function. Some enamel reduction of the bicuspid palatal cusp is normally needed. Buccal root torque of the bicuspid is helpful, as it improves esthetics and reduces the need for enamel reduction. The crown–root angulation on the facial surface of the maxillary cuspids and maxillary first bicuspids is different, and, therefore, not as much buccal root torque can be added to the bicuspids compared with the cuspids [35]. The malocclusion should be considered on its own merits. Crowding, or the need for overjet reduction, presents the opportunity for correction of the transposition and malocclusion by extraction of the first premolars [7].
In Mx.C.I2 transposition, there are two problems to overcome: the ability of the lateral incisor to function as a canine and the ability to disguise the canine and lateral incisor as each other. The upper lateral incisor is less favorable for “canine guidance”, as its root is usually thin and short. Hence, conversion to group function may be suggested for non-extraction cases. Camouflage of the upper canine often requires grinding of its tip, a combination of grinding and adding composite resin, or a porcelain veneer. The canine has a broader and higher gingival contour, compared with the lateral incisor, so this may make the esthetic result pleasing in those with a high smile line [7].
In mandibular canine to lateral incisor transposition, the transposed lateral incisor in the lower arch is often extracted. However, in a spaced arch, or non-extraction case, its retention in the transposed position can be accepted with little detriment to esthetics or function [7,36]. If the mandibular canine and lateral incisor have already erupted in their transposed position, correction to their normal position should not usually be attempted because dense compact bone occupies its buccolingual thickness. Alignment in their transposed position with reshaping of the incisal surfaces will not damage the teeth or supporting structures and will present an acceptable esthetic result. The teeth are correctly rotated and aligned in their transposed positions, and a mandibular anterior fixed retainer is bonded, following severing of the gingival supracrestal fibers of the rotated teeth [4,8].
D
ISCUSSIONAlthough there is no definitive explanation for the development of transposition, several theories have been suggested. One theory suggests that an interchange in position of tooth buds during the very early stages of tooth development is responsible for this anomaly. The second, a more acceptable explanation, is that the developing tooth migrates from its normal path during the course of eruption. However, a genetic etiology was strongly supported by Peck and Peck [1], and by Nelson [27].
The tooth most commonly transposed, the maxillary canine, starts its long pre-eruptive migration high above the premolars. It has been suggested that the maxillary canines may change their usual downward direction of eruption and migrate mesially to be transposed with the lateral incisor or distally to be transposed with the first premolar. The eruption of the maxillary canine in the position of the
central incisor or the second premolar is further offered as evidence that canine migration is, in fact, the cause of transposition [8].
The orthodontic correction of complete transposition is complex. The key to success is to treat early, because treatment can be accomplished with fewer possibilities of injuring the surrounding tissue. Careful observation of bitewing radiographs is essential for early diagnosis and treatment of these transpositions. Early intervention is recommended, with more limited treatment options available as time progresses. Early diagnosis of the atypical eruption pattern usually offers the option of orthodontic movement of the displaced teeth into normal arch alignment. If teeth are repositioned, there is a strong tendency for relapse requiring a long retention period. Early identification of the problem before the permanent canines and first premolar erupt tends to optimize tooth movements in achieving acceptable alignment, while minimizing severe arch collapse and asymmetry. During treatment, the possibility of damaging teeth, especially the roots and supporting structures, should be carefully considered. The main difficulties in correcting altered tooth position with maxillary canine–premolar transposition are avoiding root interference and resorption and controlling root inclination of the transposed teeth [37]. In particular, the width of the alveolus is usually insufficient for the roots of the teeth to pass labio-palatally. Root resorption may then occur as a result of compression and friction during the correction. Thinning of the labial alveolus and mucosa may result in clefting and recession of the gingiva, particularly if it is inflamed [7].
Chattopadhyay and Srinivas found a male predominance in their transposition sample [5], which is distinctly different from earlier reports from India and elsewhere [1]. We believe that, because most of the previous samples were from orthodontic clinics, a high female count could be expected because more females than males seek orthodontic treatment. Shapira et al found a high prevalence of agenesis of third molars, impacted maxillary canine, and maxillary canine– premolar transposition in patients with Down’s syndrome [29]. These anomalies should not be seen as separate, independent entities, but as associated phenomena: underdevelopment of the upper jaw, delayed dental development, reduction in teeth number and size, and the associated altered path of canine eruption. No explanation other than genetics is immediately available to explain why the Mx.C.P1 transposition should represent another phenotypic expression of this trisomy.
Transposition of the maxillary canine and the second premolar is a fairly common tooth malposition in children
with cleft lip, palate, or both. Among the abnormalities in number, size, and shape of teeth, transposition is important to take into consideration in planning a patient’s overall dental care and orthodontic treatment [24].
In conclusion, canine transposition is considered to be the most common transposition found in human dentition. Early clinical examination of children, before reaching 10 years of age, is recommended to detect developmental anomalies. Once transposition has occurred, careful orthodontic assess-ment must be carried out to correct the malocclusion in a manner that produces the best esthetic and functional result.
R
EFERENCES1. Peck L, Peck S. Maxillary canine – first premolar transposition, associated dental anomalies and genetic basis. Angle Orthod 1993;63:99–109.
2. Plunkett DJ, Dysart PS, Kardos TB, Herbison GP. A study of transposed canines in a sample of orthodontic patients. Br J Orthod 1998;25:203–8.
3. Peck S, Peck L, Hirsh G. Mandibular lateral incisor – canine transposition in monozygotic twins. J Dent Child 1997;64:409–13. 4. Shapira Y, Kuftinec MM. Tooth transposition—a review of the literature and treatment considerations. Angle Orthod 1989;59: 271–6.
5. Chattopadhyay A, Srinivas K. Transposition of teeth and genetic etiology. Angle Orthod 1996;66:147–52.
6. Shapira Y, Kuftinec MM. Maxillary tooth transpositions: Characteristic features and accompanying dental anomalies. Am J Orthod Dentofac Orthop 2001;119:127–34.
7. Weeks EC, Power SM. The presentations and management of transposed teeth. Br Dent J 1996;181:421–4.
8. Shapira Y, Kuftinec MM. Orthodontic management of mandibular canine – incisor transposition. Am J Orthod 1983; 83:271–6.
9. Mader C, Konzelman JL. Transposition of teeth. J Am Dent Assoc 1979;98:412–43.
10. Nestel E, Walsh JS. Substitution of a transposed premolar for a congentially absent lateral incisor. Am J Orthod Dentofac Orthop 1988;93:395–9.
11. Wasserstein A, Tzur B, Brezniak N. Incomplete canine transposition and maxillary central incisor impaction: a case report. Am J Orthod Dentofac Orthop 1997;111:635–9. 12. Yilmaz HH, Türkkahraman H, Sayin MÖ. Prevalence of tooth
transposition and associated dental anomalies in a Turkish population. Dentomaxillofac Radiol 2005;34:32–5.
13. Türkkahraman H, Sayin MÖ, Yilmaz HH. Maxillary canine transposition to incisor site: a rare condition. Angle Orthod 2005;75:280–3.
14. Peck S, Peck L. Classification of maxillary tooth transpositions. Am J Orthod Dentofac Orthop 1995;107:505–17.
15. Shanmuhasuntharam P, Thong YL. Extreme distal migration of maxillary canine. Br Dent J 1990;168:73–4.
16. Joshi MR, Bhatt NA. Canine transposition. Oral Surg Oral Med Oral Pathol 1971;31:49–54.
17. Rebellato J, Schable B. Treatment of a patient with an impacted transmigrant mandibular canine and a palatally impacted maxillary canine. Angle Orthod 2003;73:328–36.
18. Sato K, Yokozeki M, Takagi T, Moriyama K. An orthodontic case of transposition of the upper right canine and first premolar. Angle Orthod 2002;72:275–8.
19. Asakura S, Okamito T, Tamoto H, et al. Forty cases of tooth transposition. Dent Outlook 1958;15:979–86.
20. Yoshida S, Suzuki A, Ito K, Tanne K. Current status of migrated tooth and clinical consideration for the orthodontic treatment. J Hiroshima Univ Dent Soc. 1995; 27:266–74.
21. Burnett SE. Prevalence of maxillary canine – first premolar transposition in a composite African sample. Angle Orthod 1999;69:187–9.
22. Buenviaje TM, Rapp R. Dental anomalies in children: a clinical and radiographic survey. J Dent Child 1984;51:42–6. 23. Bradley EJ, Bell RA. Eruptive malposition of the mandibular
permanent lateral incisor: three case reports. Pediatr Dent 1990;12:380–7.
24. Ranta R. Tooth germ transposition: report of cases. J Dent Child 1989;56:366–70.
25. Yaillen DM. Early identification and correction of transposed teeth. Angle Orthod 1990;60:73–7.
26. Parker WS. Transposed premolar, canines, and lateral incisors. Am J Orthod Dentofac Orthop 1990;97:431–48.
27. Nelson GC. Maxillary canine – third premolar transposition in a prehistoric from Santa Cruz Island, California. Am J Phy Anthropol 1992;88:135–44.
28. Burnwtt SE, Weets JD. Maxillary canine – premolar transposition in two Native American skeletal samples from New Mexico. Am J Phy Anthropol 2001;116:45–50.
29. Shapira J, Chaushu S, Becker A. Prevalence of tooth transposition, third molar agnesis, and maxillary canine impaction in individuals with Down Syndrome. Angle Orthod 2000;70:290–6.
30. Maia FA. Orthodontic correction of a transposed maxillary canine and lateral incisor. Angle Orthod 2000;70:339–48. 31. Peck S, Peck L, Kataja M. Mandibular lateral – canine
transposition, concomitant dental anomalies, and genetic control. Angle Orthod 1998;68:455–66.
32. Laptook T, Silling G. Canine transposition–approaches to treatment. J Am Dent Assoc 1983;107:746–8.
33. Lai HH, Chang HF. Analysis of tooth transposition. J Taiwan Assoc Orthod 2004;16:38–43.
34. Shapira Y, Kuftinec MM. Maxillary canine – lateral incisor transposition? Orthodontic management. Am J Orthod Dentofac Orthop 1989;95:439–44.
35. Bennett JC, McLaughlin RP. Orthodontic management of the dentition with the preadjusted appliance. London: Mosby, 2001: 153–90.
36. Liberman MA, Gazit E. Cuspid transposition and treatment timing. Angle Orthod 1983;53:143–5.
37. Bocchiere A, Braga G. Correction of a bilateral canine – first premolar transposition in the late mixed dentition. Am J Orthod Dentofac Orthop 2002;121:120–8.