Physical activity has been shown empirically to have great benefits for physical health1,2and psy-chological functioning.3,4 Healthcare providers increasingly recommend regular physical activity
as an appropriate treatment to improve physical and psychological health for people with mental illness.5 Individuals with anxiety disorders have been shown to have higher levels of state and trait
Roles of State and Trait Anxiety in Physical
Activity Participation for Adults with
Anxiety Disorders
Wei-Fen Ma,1Wen-Jiuan Yen,2Wan-Chen Chen,3Hsiu-Ju Chang,4Xuan-Yi Huang,1 Hsien-Yuan Lane5*
Background/Purpose: Physical activity has benefits for reducing levels of anxiety. However, factors that
affect physical activity participation for individuals with anxiety disorders have not been well studied. Here, we aimed to clarify the roles of state and trait anxiety in physical activity participation by examining relationships among seven major study variables in Taiwanese adults with anxiety disorders.
Methods: A multi-site, cross-sectional explanatory design was used. Data were collected using one
inter-view and five self-administered questionnaires. The sample included 144 Taiwanese adults diagnosed with anxiety disorders.
Results: State and trait anxiety were significantly correlated with most of the study variables. Physical
activity participation by subjects with anxiety disorders was significantly correlated with state anxiety, ben-efits of activity, self-efficacy for activity, and social support for activity. When age, sex, and education were controlled in the analysis, state anxiety was associated significantly and negatively with physical activity, benefits of activity, and self-efficacy for activity, and was correlated positively with barriers to activity. Trait anxiety was found to be correlated significantly and negatively with benefits of activity and self-efficacy for activity, and correlated positively with barriers to activity.
Conclusion: State anxiety demonstrated greater power than trait anxiety in its relationship with physical
activity. These findings suggest that clinical mental health professionals should consider state anxiety when encouraging Taiwanese adults with anxiety disorders to engage in physical activity. [J Formos Med Assoc 2009;108(6):481–492]
Key Words: anxiety disorders, physical activity, state anxiety, trait anxiety
©2009 Elsevier & Formosan Medical Association
. . . .
1School of Nursing and Nursing Department, and 5Department of Psychiatry and Institute of Clinical Medical Science,
China Medical University and Hospital, 2College of Nursing, Chung-Shan Medical University, Taichung, 3Department of
Education, National Chengchi University, and 4College of Nursing, Taipei Medical University, Taipei, Taiwan.
Received: July 30, 2008 Revised: August 19, 2008 Accepted: January 7, 2009
*Correspondence to: Dr Hsien-Yuan Lane, Department of Psychiatry and Institute of
Clinical Medical Science, China Medical University and Hospital, 91 Hsueh-Shih Road, Taichung 404, Taiwan.
anxiety than the general population.6–8These find-ings suggest key questions about the roles of state and trait anxiety as they relate to physical activity participation for Taiwanese adults with anxiety disorders.
The relationships between anxiety and behav-ior outcomes have been described in Spielberger’s Cross-Sectional Model of Anxiety.9This model pro-poses that state anxiety causes behavioral reac-tions directly through defense mechanisms and adaptive processes to avoid stressful situations.8,9 In addition, trait anxiety directly influences one’s cognitive appraisal, which has an impact on how an individual perceives stressful situations.9This model led the authors to consider that state and trait anxiety may have a profound influence on physical activity behavior, especially for individ-uals with anxiety disorders.
Physical activity has been shown in a meta-analysis to help reduce levels of anxiety,10 not only by its impact on biological systems,11,12but also by improving emotional status,13especially when exercise gives people relief and time away from daily worries.14These effects are profoundly significant for the moderate symptoms of indi-viduals with generalized anxiety disorder (GAD) and panic disorder,15and participating in regular physical activity has been found to be especially meaningful and important for individuals with anxiety disorders.16Nevertheless, the motivation, facilitators and inhibitors of physical activity par-ticipation for individuals with anxiety disorders have not been fully documented. To promote better health for those with anxiety disorders, by encouraging them to engage in physical activity, the roles of state and trait anxiety need clarifica-tion. This is particularly true for Taiwanese adults with anxiety, because these issues have not been studied in this population.
This study was guided by Pender et al’s17 re-vised Health Promotion Model (HPM), which inte-grates constructs from Becker’s Health Belief Model, Ajzen and Fishbein’s Theory of Reasoned Action, Bandura’s Social Cognitive Theory, and Prochaska and DiClemente’s Transtheoretical Model. The re-vised HPM predicts health-promoting behavior,
and has been tested for predicting physical activity in general populations.13,18,19 Pender et al’s re-vised HPM has been used to show that the physi-cal activity of general populations is significantly affected by four factors: benefits of activity; barri-ers to activity; self-efficacy for activity; and social support for activity.17For example, physical activ-ity in a Taiwanese general population was shown to be correlated positively with perceived benefits of activity in a sample of 400 workers,20which was also demonstrated in 125 US college students.21 In addition, participation in physical activity was determined largely by self-efficacy for activity in both Western4,22and Taiwanese populations,20and influenced positively by social support for activity in general populations of adults from Western countries.23–25In contrast, barriers to physical ac-tivity have been shown often to hinder Taiwanese adolescents from engaging in physical activity.26
Together, these findings raise two key questions. Do these same four factors that influence physi-cal activity for the general population correlate with participation in physical activity for people with anxiety disorders? Do state and trait anxiety also relate to these four factors and influence par-ticipation in physical activity? To help Taiwanese clients with anxiety disorders reduce anxiety lev-els, mental healthcare providers need additional evidence that state and trait anxiety are indeed related to levels of physical activity and factors that influence physical activity participation in this population.
Our objective was to clarify the roles of state and trait anxiety in physical activity participation of Taiwanese adults with anxiety disorders, by ex-amining the relationships among seven variables: state anxiety, trait anxiety, levels of physical activ-ity participation, benefits of activactiv-ity, barriers to activity, self-efficacy for activity, and social sup-port for activity. Our hypothesis was that increased levels of state and trait anxiety were associated significantly with decreased levels of physical ac-tivity participation, with decreased levels of ben-efits of activity, self-efficacy for activity, and social support for activity, as well as increased levels of barriers to activity.
Subjects and Methods
Research design and study subjects
A cross-sectional explanatory design was used to select a convenience sample from five study sites: three psychiatric clinics in the city of Taichung, one counseling center in Taoyuan County, and one psychiatric clinic in the city of Taipei. Cri-teria for selection included non-hospitalized men and women, aged 20–60 years, diagnosed with anxiety disorders by clinical psychiatrists, able to verbally communicate, and who agreed to par-ticipate in this study. Subjects meeting these cri-teria were identified by psychiatrists at the study sites using the Structured Clinical Interview from the Diagnostic and Statistical Manual of Mental Disorders.27 Individuals were excluded if they were diagnosed with schizophrenia, mood dis-order, impaired cognitive function, or physical disability.
The sample size was estimated using nQuery Advisor 6.01 (Statistical Solutions, Boston, MA, USA). This software calculated a sample size of 81–118 based on correlation coefficients between physical activity and six anxiety- and physical-activity-related variables found in a pilot study of 18 adults with anxiety disorders, a power of 0.80, α = 0.05, and a two-tailed test of significance. Allowing for a 15% dropout rate, the total sample size needed was 135. Of the 150 individuals who participated in this study, 144 (96%) completed all questionnaires. The study sample included 72 patients with GAD, 48 with panic disorder and agoraphobia (PDA), 13 with obsessive-compulsive disorder (OCD), six with posttraumatic stress dis-order (PTSD), and five with social phobia (SP). The final power for this study, based on correlation coefficients of six variables to physical activity, was 87–96%.
Instruments
Data for this study were collected using six instruments: the Demographic Inventory (DI), the State-Trait Anxiety Inventory form Y (STAI-Y), the Exercise Benefits/Barriers Scale (EBBS), the Exercise Confidence Survey (ECS), the Social Support and
Exercise Survey (SSE), and the Past Year Regular Physical Activity Checklist (PYRPAC).
Measures of state anxiety, trait anxiety, self-efficacy, social support (STAI-Y, ECS, SSE) were translated from English into Mandarin Chinese and back-translated to satisfy both semantic and cultural equivalence requirements.28,29The mea-sure of exercise benefits and barriers (EBBS) used for this study was translated previously from English into Chinese.18The measure of physical activity (PYRPAC) was modified by the authors from existing Chinese measures of physical activ-ity to accommodate the cultural background and specific age range of the study subjects.
DI
Demographic data on study subjects included nine items: age, sex, education, marital status, job status, income adequacy, self-reported monthly income, anti-anxiety medication, and anxiety disorder diagnosis.
STAI-Y
State and trait anxiety were defined according to Spielberger.8State anxiety is the temporary dimen-sion of anxiety that is related to stress responses, and trait anxiety is the character dimension of anxiety that is related to the long-term stability of personality. The STAI-Y is a self-administered questionnaire that measures subjective feelings of state and trait anxiety. The STAI-Y includes 40 items rated on a 4-point Likert-type scale from 1 (not at all) to 4 (very much). The STAI-Y has two subscales that assess state anxiety (Y1, 20 items) and trait anxiety (Y2, 20 items). Total STAI-Y scores can range from 40 to 160, with higher scores in-dicating higher anxiety. The two subscales have been shown to have satisfactory reliability and validity.8For the current research, the 2-week test– retest reliability of the Chinese version of the STAI-Y was shown, in a pilot study of 18 Taiwanese adults with anxiety disorders, to be 0.63 for state anxiety and 0.92 for trait anxiety. The lower reli-ability for state anxiety in the pilot study was likely explained by fluctuations in individuals’ feelings with changing life events.8For the present study,
Cronbach’s α coefficients were 0.92 and 0.90 for trait and state anxiety subscales, respectively.
EBBS
Benefits of activity have been defined as an indi-vidual’s subjective knowledge or experience re-garding the advantages of physical activity,30and barriers to activity as the perceived limitations to physical activity.30The EBBS has two subscales that measure benefits of activity (29 items) and barri-ers to activity (14 items). EBBS items are rated on a 4-point, forced-choice, Likert-type format scale from 4 (strongly agree) to 1 (strongly disagree). Scores on the benefits subscale can range from 29 to 116, and on the barriers (limitations) sub-scale from 14 to 56. Higher scores on the bene-fits subscale indicate more perceived benebene-fits of exercise. Higher scores on the barriers subscale indicate more perceived barriers to exercise. The original EBBS was reported to have good 2-week test–retest reliability, internal consistency, and construct validity.30 The Chinese version of the EBBS was reported to have good test–retest and internal consistency reliability.18In the pilot study for the current research, the 2-week test–retest coefficients for the Chinese version of the EBBS benefits and barriers subscales were 0.87 and 0.87, respectively. Cronbach’s α coefficients for the ben-efits and barriers subscales in the present study were 0.92 and 0.84, respectively.
ECS
Self-efficacy for activity was defined as one’s confi-dence in the ability to engage in physical activity.31 The ECS measures self-efficacy for activity and con-sists of 12 items rated on a 5-point Likert-type scale from 1 (I know I cannot) to 5 (I know I can). ECS scores can range from 12 to 60, with higher scores indicating greater confidence in one’s ability to engage in physical activity. The ECS was reported to have acceptable 2-week test–retest reliability, inter-nal consistency reliability, criterion-related validity, and construct validity.31In the pilot study for the current research, the Chinese version of the ECS had a 2-week test–retest coefficient of 0.73. Cronbach’s α coefficient for the present study was 0.90.
SSE
Social support for activity was defined as an in-dividual’s cognitive appraisal of being reliably supported by family members and friends when performing physical activity.32The SSE measures social support for activity during the preceding 3 months. The SSE consists of 13 items with re-sponses rated on a 5-point Likert-type scale from 1 (none) to 5 (very often). Each item has two re-sponses: one indicating support from family (or members of the subject’s household) and the other indicating support from friends. SSE scores can range from 26 to 130, with higher scores indicat-ing greater social support for performindicat-ing physi-cal activity. The SSE was reported to have good 2-week test–retest reliability, internal consistency reliability, criterion-related validity, and construct validity by principal-components factor analysis.32 In the pilot study for the current research, the Chinese version of the SSE had a 2-week test– retest coefficient of 0.89. Cronbach’s α coefficient for the present study was 0.89.
PYRPAC
The definition of physical activity for the present study was an individual’s regular performance of moderate physical activity during the past year. The PYRPAC was modified from the 12-item Past Year Regular Physical Exercise Questionnaire (PYRPEQ), which has been used to measure reg-ular leisure-time physical exercise for Taiwanese elders,18and from 19 physical activities identified as most likely to be performed by 504 Taiwanese adults.33Drawing on these studies, we added 13 items to the PYRPEQ and changed its format from self- to interviewer-administered to create the 25-item PYRPAC, plus three open-ended 25-items at the end. The PYRPAC was then evaluated and found to measure accurately regular physical activity for Taiwanese adults with anxiety disorders.
To quantify the information collected in the PYRPAC, all data were recorded as energy expen-diture, using metabolic equivalent units (METs). One MET is equal to 3.5 mL O2/kg/min.34 The METs for each physical activity were recorded as described previously.35,36Higher METs indicated
greater amounts of regular physical activity. In the pilot study for the current research, the PYRPAC had a 2-week test–retest coefficient of 0.70 and a correlation coefficient of 0.68 (p< 0.001) when compared with a 7-day physical activity recall.
Procedure and ethical consideration
The present study was approved by the Institutional Review Boards at the study sites. Subjects signed informed consent that explained the study pur-poses, data collection procedures, potential risks and benefits of participation, and protection of confidentiality by ensuring the anonymity of their responses. Potential risks for subjects included fatigue and anxiety or discomfort caused by the subject matter and length of the questionnaires. To minimize these risks, subjects were told that they could rest at any time, they were not pressured to complete the questionnaires within a time limit, and they could omit any items that made them feel uncomfortable.
Data were collected during July 2004 and July 2006 using interviewer- and self-administered questionnaires. To recruit subjects, the first au-thor provided exclusion and inclusion criteria to the managers and staff members at the five study sites. Patients meeting the study criteria were iden-tified by study-site psychiatrists who informed the authors. The researcher met with these potential participants in a quiet room to explain the study purposes and to describe the rights, benefits and risks of participation. After participants signed the consent form, the researcher gave them a copy of the consent form and a pack of questionnaires. Subjects were then interviewed individually by the researcher using the PYRPAC to measure levels of physical activity. The remaining questionnaires were then explained, and subjects completed them alone. Each subject took 25–60 minutes to com-plete the questionnaires.
Data analysis
Descriptive statistics were used to explain demo-graphic data and major variables. Levine’s test was used to examine the assumption of homogeneity of variance (HOV) among groups. Differences by
study sites and by types of anxiety disorder were tested by analysis of variance (ANOVA) and Scheffe’s test. Levine’s test was used to examine differences among groups, and post hoc tests using Dunnett’s C test were used to examine the data for variables that did not satisfy the HOV. Pearson’s r correlation was used to test relationships among study variables for the two groups. Linear regres-sion was used to examine relationships of state and trait anxiety to other study variables by con-trolling for age, sex and education.
Results
Subject characteristics
Of 144 Taiwanese adults in the study sample, 55 (38.2%) were male, and 89 (61.8%) were female. They had a mean age of 35.96± 10.79 years (range, 20–60 years), with 45.8% (n= 66) who were sin-gle and 43.8% (n= 63) who were married. One hundred and thirty-three subjects (92.3%) had completed a high school education. Eighty-two subjects (56.9%) reported adequate income to meet their needs, and only 55 (38.2%) were cur-rently taking medicine to control anxiety. The av-erage state and trait anxiety scores were 46.62 and 55.42, respectively. The details of these study variables are shown in Table 1.
Differences among subjects by type of anxiety disorder
Subjects with different types of anxiety disorders differed significantly with regard to state anxiety, trait anxiety, benefits of activity, and self-efficacy for activity (Table 2). Post hoc test outcomes showed that subjects with SP had significantly higher state and trait anxiety levels than subjects with other anxiety disorders. On the other hand, sub-jects with PDA showed significantly higher self-efficacy for activity than subjects with GAD and SP. Subjects with different types of anxiety disor-der did not differ significantly in terms of physi-cal activity participation, perceived benefits of activity, perceived barriers to activity, and social support for activity.
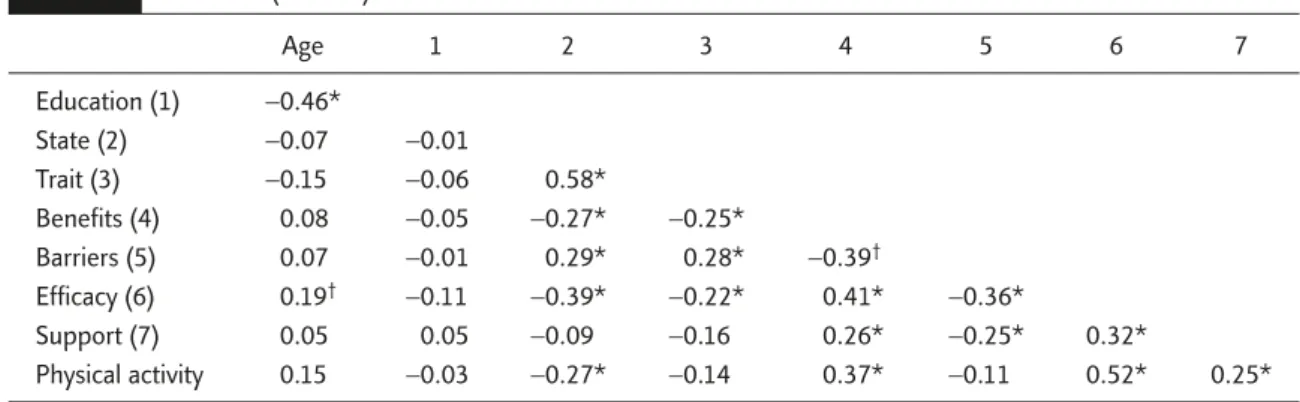
Correlations of physical activity participation with physical-activity factors and anxiety
Physical activity participation for subjects with anxiety disorders was correlated significantly with state anxiety, benefits of activity, self-efficacy for activity, and social support for activity (Table 3). In addition, state and trait anxiety were correlated significantly with most of the variables that influ-enced physical activity participation.
Linear regression analysis for state and trait anxiety by potential confounders
To clarify the role of anxiety in participation in physical activity, we used linear regression analysis to examine potential confounders between state anxiety and physical activity and factors that in-fluenced participation in physical activity. When age, sex and education were controlled in the analy-sis, state anxiety was associated significantly and negatively with physical activity, benefits of ac-tivity, and self-efficacy for acac-tivity, and was corre-lated positively with barriers to activity. Table 4 presents detailed information about relationships between state anxiety and other variables when potential confounders were controlled.
Using a similar analysis as for state anxiety, trait anxiety was found to be correlated signifi-cantly and negatively with benefits of activity and self-efficacy for activity, and correlated posi-tively with barriers to activity when age, sex and education were controlled. The results of linear
regression analysis for trait anxiety by control-ling for potential confounders are summarized in Table 5.
Discussion
Our results show that state anxiety had greater power than trait anxiety in its relationship with physical activity. State anxiety was correlated sig-nificantly and negatively with physical activity for our subjects with anxiety disorders, but trait anx-iety was not associated significantly with phy-sical activity. State anxiety, by definition,8is the response to stress from life events postulated to affect behaviors. It was reasonable to assume, therefore, that subjects with higher state anxiety would have engaged in less physical activity, be-cause they faced problems or stresses in their lives. This assumption is supported by results of a 4-year follow-up study on 7281 young adult women whose physical activity levels decreased during key life events such as getting married and having children.37
In contrast, a 2-year randomized controlled trial38found that higher life stress was related to greater participation in physical activity among an intervention group of 184 women and 154 men. These results suggest that higher stress sup-ports greater physical activity participation because physical activity is perceived as a way to help deal Table 1. Scales used to measure variables and their descriptive statistics (n= 144)
Variable Scale n Mean SD IQR Range
Age DI 144 35.96 10.79 17.75 10–60
Education DI 144 13.43 3.25 4.0 18
State anxiety STAI-Y1 144 46.62 9.45 14 23–74
Trait anxiety STAI-Y2 144 55.42 7.53 9.5 33–76
Benefits EBBS-benefits 144 85.01 9.99 7.75 58–113
Barriers EBBS-barriers 144 29.76 4.61 4 17–40
Efficacy ECS 144 31.17 11.67 17.5 12–60
Social support SSE 143 43.29 13.78 21 20–78
Physical activity PYRPAC 144 23.52 21.16 18.8 0.39–127.69
IQR = 75thquartile minus 25thquartile; DI = demographic inventory; STAI-Y = State-Trait Anxiety Inventory form Y; EBBS = Exercise Benefits/Barriers Scale; ECS = Exercise Confidence Survey; SSE = Social Support and Exercise Survey; PYRPAC = Past Year Regular Physical Activity Checklist.
with life stress. Similarly, 32,229 employed adults who participated in moderate physical activity were about half as likely to perceive stress as those who did not exercise.39Coping skills for life stress may differ in working people or healthy young adults from those in individuals with anxiety disorders.
Our findings also showed that physical ac-tivity was correlated significantly and positively with study variables that influenced physical ac-tivity, i.e. the benefits of, self-efficacy for, and social support for physical activity. These out-comes are consistent with the predicted outout-comes Table 2. Differences among subjects with different types of anxiety disorders (n= 144)
Variable Disorder type n Mean SD F Scheffe’s test
State anxiety GAD 72 48.72 8.55 4.617* SP, OCD†
PDA 48 47.98 10.06 SP, PDA†
OCD 13 47.92 8.15 SP, PTSD†
PTSD 6 41.33 6.74 SP, GAD†
SP 5 63.80 8.70
Trait anxiety GAD 72 54.82 7.09 5.094* SP, PTSD†
PDA 48 55.17 7.59
OCD 13 59.08 5.38
PTSD 6 48.17 7.94
SP 5 65.60 5.77
Benefits GAD 72 85.11 9.43 3.202† No differences
PDA 48 86.40 8.54
OCD 13 78.31 13.19
PTSD 6 92.50 9.22
SP 5 78.80 14.52
Barriers GAD 72 30.15 4.68 2.368 No differences
PDA 48 29.33 3.99
OCD 13 30.08 4.48
PTSD 6 25.17 5.42
SP 5 32.80 6.14
Self-efficacy GAD 72 28.61 10.36 3.919* PDA, SP†
PDA 48 35.71 12.71 PDA, GAD†
OCD 13 30.00 12.95
PTSD 6 35.50 5.79
SP 5 22.40 5.68
Social support GAD 71 43.29 13.78 0.930 No differences
PDA 48 42.69 14.05
OCD 13 42.15 14.72
PTSD 6 53.50 10.86
SP 5 40.20 8.89
Physical activity GAD 72 22.21 21.97 1.368 No differences
PDA 48 28.64 22.81
OCD 13 15.51 13.09
PTSD 6 18.33 10.91
SP 5 20.37 6.86
*p< 0.01; †p< 0.05. GAD = generalized anxiety disorder; PDA = panic disorder and agoraphobia; OCD = obsessive-compulsive disorder; PTSD = posttraumatic stress disorder; SP = social phobia.
of Pender et al’s17 revised HPM, except for the variable of barriers to activity. Our results are also supported by previous studies that have shown that physical activity is correlated significantly
and positively with the benefits of activity,21and that the higher the perceived benefits of activity, the higher the levels of physical activity.5,40Other support comes from evidence that self-efficacy Table 3. Pearson’s r correlations of physical activity with selected variables for subjects with anxiety
disorders (n= 144) Age 1 2 3 4 5 6 7 Education (1) −0.46* State (2) −0.07 −0.01 Trait (3) −0.15 −0.06 0.58* Benefits (4) 0.08 −0.05 −0.27* −0.25* Barriers (5) 0.07 −0.01 0.29* 0.28* −0.39† Efficacy (6) 0.19† −0.11 −0.39* −0.22* 0.41* −0.36* Support (7) 0.05 0.05 −0.09 −0.16 0.26* −0.25* 0.32* Physical activity 0.15 −0.03 −0.27* −0.14 0.37* −0.11 0.52* 0.25* *p< 0.01; †p< 0.05.
Table 4. Summary of linear regression analysis for state anxiety by age, sex and education
Outcome variable Control b Beta t Adjusted R2 F
Physical activity Beta 39.09 2.45* 0.09 4.66†
State anxiety −0.53 −0.24 −2.95†
Age 0.41 0.21 2.30*
Sex −5.56 −0.13 −1.58
Education 0.34 0.05 0.59
Benefits of activity Beta 96.35 12.50‡ 0.06 3.09*
State anxiety −0.29 −0.27 −3.33†
Age 0.03 0.04 0.38
Sex 1.75 0.09 1.03
Education −0.09 −0.03 −0.32
Barriers to activity Beta 20.16 5.70‡ 0.07 3.50†
State anxiety 0.14 0.30 3.60‡
Age 0.05 0.12 1.27
Sex −0.11 −0.01 −0.14
Education 0.07 0.05 0.56
Efficacy for activity Beta 55.63 6.74‡ 0.21 10.21‡
State anxiety −0.43 −0.35 −4.58‡
Age 0.19 0.18 2.08*
Sex −5.39 −0.23 −2.96†
Education −0.14 −0.04 −0.46
Support for activity Beta 40.32 3.66‡ −0.01 0.56
State anxiety −0.12 −0.09 −0.99
Age 0.11 0.08 0.86
Sex 0.28 0.01 0.12
Education 0.35 0.08 0.87
and social support for activity are the most com-mon factors that influence physical activity.22,41 Our results also showed that state anxiety was re-lated significantly to three of the four factors that influence physical activity. These results suggest that future studies might consider state anxiety as a cognitive variable for benefits of, barriers to, efficacy for, and support for activity in a model to predict physical activity. The results of model testing might fill gaps in our knowledge about direct and indirect influences on physical activity in patients with anxiety disorders.
We found that subjects with different types of anxiety disorders differed in most of the variables that we examined, which indicates that individu-als with different types of anxiety disorders vary
with regard to participation in physical activity. For example, subjects with PTSD had significantly lower levels of trait anxiety than others. In addi-tion, subjects with SP had significantly higher state anxiety than others. To obtain more insightful and stable data, we suggest that future researchers se-lect and group subjects based on similar types of anxiety. For example, subjects with GAD, PDA, OCD and SP should be grouped separately from those with PTSD for trait anxiety, and subjects with GAD, PDA, OCD and PTSD should be grouped separately from those with SP for state anxiety. When individuals with anxiety disorders are en-couraged to engage in physical activity, those with GAD and SP need more interventions to increase self-efficacy for activity, since our study showed Table 5. Summary of linear regression analysis for trait anxiety by age, sex and education
Outcome variable Control b Beta t Adjusted R2 F
Physical activity Beta 29.24 1.52 0.05 2.75*
Trait anxiety −0.29 −0.10 −1.24
Age 0.43 0.22 2.35*
Sex −6.85 −0.16 −1.91
Education 0.43 0.07 0.72
Benefits of activity Beta 101.07 11.08† 0.04 2.52*
Trait anxiety −0.33 −0.25 −2.97‡
Age 0.03 0.03 0.29
Sex 1.15 0.06 0.68
Education −0.05 −0.02 −0.18
Barriers to activity Beta 16.68 4.02† 0.07 3.54‡
Trait anxiety 0.18 0.30 3.62†
Age 0.06 0.13 1.42
Sex 0.17 0.02 0.23
Education 0.05 0.04 0.41
Efficacy for activity Beta 50.70 4.97† 0.12 5.78†
Trait anxiety −0.28 −0.18 −2.28*
Age 0.20 0.19 2.09*
Sex −6.39 −.27 −3.37‡
Education −0.07 −0.02 −0.23
Support for activity Beta 50.39 3.93† 0.00 1.11
Trait anxiety −0.28 −0.15 −1.78
Age 0.09 0.07 0.71
Sex 0.10 0.01 0.04
Education 0.36 0.09 0.91
that such individuals had significantly lower self-efficacy scores for activity than others did.
The results of this study showed a significant relationship between age and self-efficacy for ac-tivity. In addition, this result was compromised by the gender imbalance in our sample (two-thirds female). To determine whether other sociodemo-graphic variables were confounders for anxiety variables, we controlled for these variables and other physical activity-related variables and found no change in the significant relationships of state and trait anxiety to other study variables. We also found that trait anxiety was associated significantly with benefits of, barriers to, and self-efficacy for activity. To test for direct and indirect effects of individual characteristics such as personal data and trait anxiety on physical activity behavior, future research should include a larger sample size.
Study limitations
The generalizability of our results has some limita-tions. First, the data were collected from Taiwanese adults, aged 20–60 years, who were receiving ser-vices in mental health clinics for anxiety disorders. Thus, our results may not be applicable to people younger than 20 or older than 60 years, living in other countries with different cultures, or with other mental diseases or disorders. Second, the information was obtained from questionnaires and interviews, which may have bias related to memory capacity, personal influences or opinions, and social desirability. Third, subjects were re-cruited by convenience sampling. Thus, outcomes cannot be generalized for individuals diagnosed with anxiety disorders who did not participate or who were attending other clinics. Fourth, this study is limited by using a cross-sectional design to explore relationships between anxiety, physi-cal activity, and four factors that influence phy-sical activity. Interpretation of results must be made cautiously, because an explanatory design explains only the most fundamental relationships among variables. To investigate better causality and changes in variables over time, a cohort study or experimental design should be used in future studies.
Relevance to clinical application
The wellbeing of individuals with mental illness is promoted by the World Health Organization,42 and mental wellbeing has been associated with increased participation in physical activity. Physical activity is also correlated positively with psycho-logical benefits, including a greater sense of well-being, absence of negative emotion during exercise, positive impression of physical status, and feelings of relaxation after activity.21Furthermore, physical activity is associated significantly with a decreased prevalence of anxiety disorders for individuals with mental illness.16,43For these reasons, men-tal health clinicians should develop guidelines to promote physical activity participation by first dealing with the higher levels of state and trait anxiety in populations with anxiety disorders.
When encouraging individuals with anxiety disorders to engage in physical activity, clinicians should also emphasize the benefits of activity (e.g. decreased anxiety levels), improve patients’ self-efficacy for activity (e.g. conduct small groups in clinics for sharing successful experiences in regu-lar physical activity), and develop social support for activity (e.g. help enlist family members or friends who can join subjects in the activity).
Here, perceived barriers to activity were not correlated significantly with physical activity. This outcome differed from that of other studies, in which barriers to activity were usually related neg-atively to physical activity.44Our findings on bar-riers to activity suggest that clinicians might not need to consider barriers when promoting in-creased levels of physical activity for people with anxiety disorders.
Conclusion
This is believed to be the first study to demon-strate correlations among state anxiety, trait anx-iety, physical activity and factors that influence physical activity in Taiwanese adults with anxiety disorders. The results are consistent with previous reports that physical activity is correlated well with most of its influencing variables. This study
suggests that clinical mental health professionals should emphasize state anxiety when encouraging these clients to engage in physical activity.
References
1. Elley C, Arroll B. Review: aerobic exercise reduces systolic and diastolic blood pressure in adults. ACP J Club 2002; 137:109.
2. Fransson EI, Alfredsson LS, de Faire UH, et al. Leisure time, occupational and household physical activity, and risk factors for cardiovascular disease in working men and women: the WOLF study. Scand J Public Health 2003; 31:324–33.
3. Berger BG, Owen DR. Relation of low and moderate inten-sity exercise with acute mood change in college joggers.
Percept Mot Skills 1998;87:611–21.
4. D’Alonzo KT, Stevenson JS, Davis SE. Outcomes of a pro-gram to enhance exercise self-efficacy and improve fitness in Black and Hispanic college-age women. Res Nurs Health 2004;27:357–69.
5. Schmitz N, Kruse J, Kugler J. The association between physical exercises and health-related quality of life in sub-jects with mental disorders: results from a cross-sectional survey. Prev Med 2004;39:1200–7.
6. McLean PD, Woody SR. Anxiety Disorders in Adults. New York: Oxford University Press, 2001.
7. Spano L. The relationship between exercise and anxiety, obsessive-compulsiveness, and narcissism. Pers Individ Dif 2001;30:87–93.
8. Spielberger CD. State-Trait Anxiety Inventory. Mountain View, CA: Consulting Psychologists Press, 1983. 9. Spielberger CD. Anxiety and Behavior. New York: Academic
Press, 1966.
10. Petruzzello SJ, Landers DM, Hatfield BD, et al. A meta-analysis on the anxiety-reducing effects of acute and chronic exercise. Sports Med 1991;11:143–82.
11. Goldfarb AH, Hatfield BD, Potts J, et al. Beta-endorphin time course response to intensity of exercise: effect of training status. Int J Sports Med 1991;12:264–8. 12. Hoffmann P. The endorphin hypothesis. In: Morgan WP,
ed. Physical Activity and Mental Health. Washington: Taylor & Francis, 1997:163–77.
13. Stutts W. Physical activity determinants in adults: perceived benefits, barriers, and self efficacy. AAOHN J 2002;50: 499–507.
14. Breus MJ, O’Connor PJ. Exercise-induced anxiolysis: a test of the “time out” hypothesis in high anxious females. Med
Sci Sports Exerc 1998;30:1107–12.
15. Paluska SA, Schwenk TL. Physical activity and mental health: current concepts. Sports Med 2000;29:167–80. 16. Goodwin RD. Association between physical activity and
mental disorders among adults in the United States. Prev
Med 2003;36:698–703.
17. Pender NJ, Murdaugh CL, Parsons MA. Health Promotion
in Nursing Practice. NJ: Prentice Hall, 2006.
18. Chen CH. Physical Exercise and Sense of Well-being
among Chinese Elderly in Taiwan. Austin, Texas: University
of Texas at Austin, 1995. [Dissertation]
19. Wu TY, Ronis DL, Pender N, et al. Development of ques-tionnaires to measure physical activity cognitions among Taiwanese adolescents. Pre Med 2002;35:54–64. 20. Kao Y, Huang Y. Determinants of exercise behavior in adults:
a path analysis. J Nurs Res 2000;8:435–46. [In Chinese] 21. Barrows PL. Exercise Participation and the Relationship
to Depressive Symptomatology, Motives, Barriers, and Perceived Benefits of Exercise Participation in College Students. Texas: Texas Tech University, 2003. [Dissertation]
22. Miller KH, Ogletree RJ, Welshimer K. Impact of activity behaviors on physical activity identity and self-efficacy.
Am J Health Behav 2002;26:323–30.
23. Courneya K, Plotnikoff R, Hotz S, et al. Predicting exercise stage transitions over two consecutive 6-month periods: a test of the theory of planned behaviour in a population-based sample. Br J Health Psychol 2001;6:135–50. 24. Dowda M, Ainsworth BE, Addy CL, et al. Correlates of
physical activity among U.S. young adults, 18 to 30 years of age, from NHANES III. Ann Behav Med 2003;26:15–23. 25. Giles-Corti B, Donovan RJ. Socioeconomic status differ-ences in recreational physical activity levels and real and perceived access to a supportive physical environment.
Prev Med 2002;35:601–11.
26. Wu TY, Pender N. Determinants of physical activity among Taiwanese adolescents: an application of the Health Pro-motion Model. Res Nurs Health 2002;25:25–36. 27. American Psychiatric Association. Diagnostic and Statistical
Manual of Mental Disorders: DSM-IV-TR (4th Rev. ed.).
Washington, DC: American Psychiatric Association, 2000. 28. Corless IB, Nicholas PK, Nokes KM. Issues in cross-culture quality-of-life research. J Nurs Scholarsh 2001;33:15–20. 29. Varricchio CG. Measurement issues concerning linguistic
translations. In: Frank-Stromborg M, Olsen S, eds.
Instru-ment for Clinical Health Care Research. Boston: Jones
and Bartlett, 1997:54–63.
30. Sechrist KR, Walker SN, Pender NJ. Development and psychometric evaluation of the exercise benefits/barriers scale. Res Nurs Health 1987;10:357–65.
31. Sallis JF, Pinski RB, Grossman RM, et al. The development of self-efficacy scales for health-related diet and exercise behaviors. Health Educ Res 1988;3:283–92.
32. Sallis JF, Grossman RM, Pinski RB, et al. The development of scales to measure social support for diet and exercise behaviors. Prev Med 1987;16:825–36.
33. Li BX. The Stage of Exercise, Physical Activity and their
Determinants: A Study of the Middle-aged from the Chungshan District in Taipei. Taipei: National Taiwan
Normal University, 2001. [Dissertation]
34. American College of Sports Medicine. ACSM’s Resource
Manual for Guidelines for Exercise Testing and Prescription.
35. Ainsworth BE, Haskell WL, Leon AS, et al. Compendium of physical activities: classification of energy costs of human physical activities. Med Sci Sports Exerc 1993;25:71–80. 36. Montoye HJ, Kemper HCG, Saris WHM, et al. Measuring
Physical Activity and Energy Expenditure. Champaign, IL:
Human Kinetics, 1996.
37. Brown WJ, Trost SG. Life transitions and changing physical activity patterns in young women. Am J Prev Med 2003; 25:140–3.
38. Johnson-Kozlow MF, Sallis JF, Calfas KJ. Does life stress moderate the effects of a physical activity intervention?
Psychol Health 2004;19:479–89.
39. Aldana SG, Sutton LD, Jacobson BH, et al. Relationships between leisure time physical activity and perceived stress.
Percept Mot Skills 1996;82:315–21.
40. Smits JAJ, Zvolensky MJ. Emotional vulnerability as a func-tion of physical activity among individuals with panic disorder. Depress Anxiety 2006;23:102–6.
41. Lewis BA, Marcus BH, Pate RR, et al. Psychosocial media-tors of physical activity behavior among adults and children.
Am J Prev Med 2002;23:26–35.
42. World Health Organization. World Health Report 2001.
Mental Health: New Understanding, New Hope. Geneva:
World Health Organization, 2001.
43. Ng F, Dodd S, Berk M. The effects of physical activity in the acute treatment of bipolar disorder: a pilot study.
J Affect Disord 2007;101:259–62.
44. Knapen J, Vermeersch J, Van Coppenalle H, et al. The physical self-concept in patients with depressive and anxiety disorders. Int J Ther Rehabil 2007;14:30–5.