論文題目:藥事服務的經濟效益 - 以重症加護病房為例 作 者:黃靖雅1 郝宏恕2 謝右文1,3 蔡輝彥1,3 所屬機構及單位: 1中國醫藥大學附設醫院 藥劑部 2中國醫藥大學 公共衛生學院 醫務管理學系 3中國醫藥大學藥 藥學院 藥學系 聯 絡 人:黃靖雅 地 址:台中市育德路 2 號 電 話:22062121 ext 2263 作者介紹: 黃靖雅 中國醫藥大學附設醫院 藥劑部 臨床藥師/ 中國醫藥大學 藥學院藥學系 兼任講師 郝宏恕 中國醫藥大學 公共衛生學院醫務管理學系 副教授 謝右文 中國醫藥大學附設醫院 藥劑部 部主任/ 中國醫藥大學 藥學院藥學系 助理教授 蔡輝彥 中國醫藥大學附設醫院 院長室 顧問/ 中國醫藥大學 藥學院藥學系 榮譽教授
摘 要 美國重症醫學會指出藥師是重症照護團隊不可或缺的角色,因為藥師的加入可以 預防藥物不良事件之發生並且降低照護的費用。藥師參與病房照護對於醫療品質的提升 方面,國內外的文獻報告相當多,但就國內藥師在醫院提供住院病人藥事服務,是否 對於醫療花費造成影響則極少有相關研究發表。 本研究利用不同時段,在個案醫院內科加護病房藥師人力配置的差異,探討其中 藥物費用、平均入住加護病房的天數是否有所差異。本研究使用 SAS (9.1 版) 套裝軟體進 行描述性統計、卡方檢定、t-檢定、變異數分析及複迴歸分析。 研究結果顯示,研究組及對照組在性別、年齡、入住及離開加護病房時之 APACHE II Score、病房佔床率,或是在提供醫療照護之醫師年資、護理人員職級上皆無明顯差異 之基礎下,研究組每人每日平均藥費可節省 894 元,而在加護病房入住天數方面則降 低了 0.67 天。由以上研究結果證實藥師對於醫療團隊的貢獻不僅在提升醫療品質,在評 估用藥的經濟效益以及節省醫療照顧費用的角色亦將更顯重要。 關鍵字:臨床藥學、加護病房、健康經濟學、效益評估
壹、前言 近十年來,台灣醫療體系對於藥師提供藥事服務的要求由早期的調劑、確認藥品 正確性及交付藥品,發展至現今強調以病人為導向之團隊服務,我們可以察覺到國內 藥師在醫療團隊中的角色有很大的變化,社會及醫療團隊要求藥師提供的服務也不同 於以往。醫院藥師與醫療團隊在這幾年中藉由不斷的溝通及相互學習,已建立相當良好 的互動模式,藥師提供醫療團隊相關的藥物建議,協助其他醫療人員的進階升等課程 並參與團隊查房,這些貢獻已深獲醫療團隊成員的肯定。除了因應醫療評鑑之要求,加 護病房主任及護理長也認為藥師參與病房照顧可以提供其他醫療人員必要的協助,希 望加護病房能派駐藥師參與團隊。這樣的需求帶給醫院管理者一個新的思考—藥師需提 供多少時數的病房照顧,才能使品質及經濟層面的考量皆呈現正面的意義,因此,除 了提升用藥品質外,我們也想知道在藥師提供藥事照顧的同時是否也提供了經濟效益。 綜觀國內就藥師在醫院提供住院病人藥事服務是否影響醫療花費,鑑於人力配置的限 制而困難執行此類評估,故極少有本土的研究數據被發表。為了瞭解藥師提供藥事照顧 的效益,本研究以個案醫院為例,回溯性的探討藥師參與重症病房內照護服務的時間 與醫療花費之間的相關性。 貳、研究方法 本研究以個案醫院內科加護病房為研究對象,在 94 年 10 月以前,藥師實際在內科 加護病房內提供照護的時間為每星期一次的教學查房,而 10 月份以後則每日參與病房 查房及病患照護,並即時提供醫療團隊藥物相關的治療建議及諮詢。研究時間為 94 年 10-12 月,而對照研究時間為 93 年 10-12 月,在這 2 個時段內科加護病房入住人數共有 440 人,此間由同一位藥師負責藥事照顧業務。因考慮患者死亡前這一段時間內的醫療 花費會極劇增加,所以排除死亡患者,另外考慮到入住少於 2 天的病人,藥師參與其 藥療照護的時間過短,故亦將入住加護病房少於 2 天的患者,排除於研究對象之外, 最後納入研究人數為 260 人。 兩組分別收集研究期間內收住病人之年齡、性別、疾病嚴重度、病人診斷分布情況, 計算病房住院人日、佔床率、平均加護病房住院日、加護病房病人回住率及藥物花費,將 兩組之各項資料進行分析比對並統計其差異程度。
本研究採用 SAS 套裝統計軟體(9.1 版)進行雙變項及複廻歸分析,分析兩組(藥師有 /無參與每日查房)患者特性、疾病嚴重度及病房照護品質上是否有所差異,並探討影響 入住加護病房天數及藥物費用之相關因素。 參、結果 依納入研究數據顯示,兩組患者在基本特質方面包括性別、年齡、入住期間主要診 斷項次、入住及離開加護病房之 APACHE II Score 皆分佈平均無顯著差異。96%病人離 開加護病房時之 APACHE II Score 小於 19 分,顯示兩組病人在離開加護病房時皆處於 疾病穩定的狀態,且未有 48 小時內回住情形。其次是兩組病人在未扣除排除對象之前, 佔床率分別為 64.8%及 62.8%,也就是說除了藥師參與病房內照護的時間有差異外,其 護理人力與病人數配置的比例是幾近相同的。主治醫師特質是指病患所屬之主治醫師的 個人資歷,即其升任主治醫師至研究其間之年資,兩階段主治醫師之平均年資分別為 7.72 年及 6.71 年,未有統計上顯著差異。另外在護理人員資歷方面,兩組護理師資歷分 佈率亦無顯著差異。 在分析此兩時段內之藥物費用差異以每人每天消耗之藥物費用來看,對照組平均 藥物費用為 4,253 元,研究組則為 3,359 元,若僅就藥物費用觀察,顯示每人每天可節 省 894 元。(表 1) 另以加護病房每人每日平均藥物費用為依變項,病人及病房等影響照 護費用因素為自變項進行複迴歸分析,探討影響加護病房藥物費用之相關因素時可以 發現,主要影響藥物費用的因素仍在於患者的疾病嚴重程度 (p<0.05),其次則為患者之 年齡 (p<0.1)。(表 2) 依據文獻指出,藥師參與照護團隊並提供藥事照顧,最明顯的經濟效益在於住院 天數的縮短而非藥物費用的節省(Dooley 等,2004),因此本研究亦就加護病房入住天 數的差異進行分析。在入住天數的分析方面,排除僅入住一天及入住 21 天以上之患者, 避免入住天數差距過大造成統計結果向左或向右偏差。對照組之平均入住天數為 6.15 天 研究組為 5.48 天,差異為 0.67 天,若依當時每日內科加護病房健康保險局之基本住院 給付費用 9,800 元計算,每位入住患者可因藥師投予照護的時間差異,節省 6,566 元之 病房費用。再以加護病房平均住院日為依變項,病人及病房等影響照護費用因素為自變
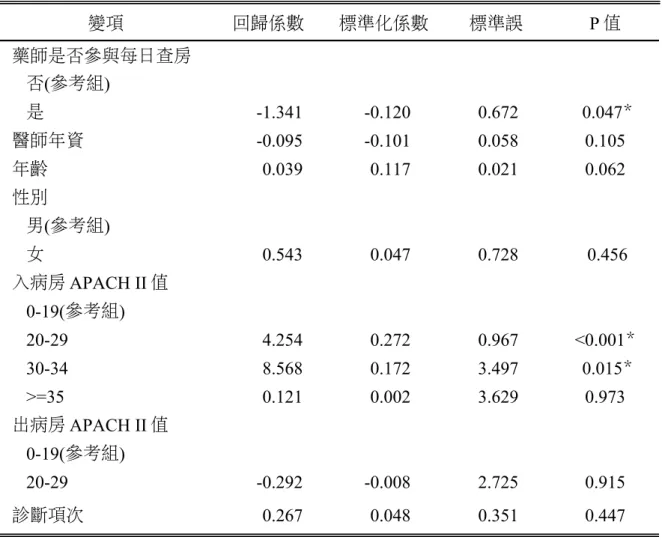
項,進行複迴歸分析,探討影響加護病房入住天數之相關因素時可以發現,主要影響 入住天數的因素仍在於患者入住時的疾病嚴重程度 (p<0.05),其次為藥師是否參與每日 查房 (p<0.05),再者則為患者之年齡 (p<0.1)。(表 3) 肆、討論 對照研究期間藥師提供每週 4 小時的病房內照護,佔週工作時數的 9.5%,以藥師 平均薪資每月 50,000 元計算,依花費時間換算成其支付的薪資每月為 4,750 元,而研究 組藥師提供每週 20 小時的病房內照護,佔週工作時數的 47.6%,同樣依花費時間來換 算則每個月需支付的薪資為 23,800 元,故每個月支付藥師的薪資差異為 19,050 元。 兩組間每人日 ICU 藥費差異 894 元,而平均加護病房入住天數降低 0.67 天。依此 結果顯示,藥物費用在病房 80% 佔床率的前提下,每個月可減少的費用為 472,032 元, 而在入住天數縮短方面,以每月平均收住 70 名病患計算,可降低病房費用達 459,620 元,合計共節省 931,652 元之醫療花費。若將節省之費用與因增加藥事照護時數所增加 的藥師薪資相除,可得到其效益/費用比率為 48.9:1,當加護病房佔床率為滿床的狀況 時,則將因減少入住天數,增加每月收住病患,其經濟效果將更加的顯著。 藥師就用藥的安全性及適切性進行評估,目的是使病人不要因為疾病以外的原因 而延長住院日數,以經濟效益的層面來看,藥師提供藥事服務在醫療資源方面可以降 低藥物不良事件的發生率、縮短住院日數並節省病患照顧費用。另外,若以社會資源的 面向來看,縮短住院日數所帶來的經濟價值,則涵蓋了個人或家庭生產力的增加、病人 健康對於患者本人及家人的意義等,舉凡感知及經濟上皆存在其不可忽視的價值。 本研究以加護病房提供之藥事服務為例,就醫療提供者之觀點進行成本花費及資 源節省的評估,為藥師參與藥事服務呈現的經濟效益提供本土研究的數據,期能拋磚 引玉看到更多的相關研究,進而使醫療提供者及政策制定者能取得足夠的參考數據, 擬定品質與效益兼具的醫療資源政策。 伍、參考文獻
1. ASHP Continuity of Care Task Force. Continuity of care in medication management: review of issues and considerations for pharmacy. American Journal of Health-System Pharmacy. 2005 Aug 15; 62(16):1714-20.
2. Curtis JR. Cook DJ. Wall RJ. et.al., Intensive care unit quality improvement: a "how-to" guide for the interdisciplinary team. Critical Care Medicine. 2006 Jan; 34(1):211-8. 3. Reader TW, Flin R, Mearns K, et.al., Developing a team performance framework for the
intensive care unit. Critical Care Medicine. 2009 May; 37(5):1787-93.
4. Dooley MJ. Allen KM. Doecke CJ. et.al., A prospective multicentre study of pharmacist initiated changes to drug therapy and patient management in acute care government funded hospitals. British Journal of Clinical Pharmacology. 2004 Apr; 57(4):513-21. 5. Drummond M, et al., chp 3. Critical assessment of economic evaluation; Method for the
economic evaluation of health care programmes. 3rd.ed. Oxford University press. 2005. 6. Horn E. Jacobi J. The critical care clinical pharmacist: evolution of an essential team
member. Critical Care Medicine. 2006 Mar; 34(3 Suppl):S46-51.
7. Kane-Gill SL, Jacobi J, Rothschild JM. Adverse drug events in intensive care units: risk factors, impact, and the role of team care. Critical Care Medicine. 2010 Jun; 38(6 Suppl):S83-9.
8. Kane-Gill S, Reddy P, Gupta SR et.al., Guidelines for pharmacoeconomic and outcomes research fellowship training programs: joint guidelines from the american college of clinical pharmacy and the international society of pharmacoeconomics and outcomes research. Pharmacotherapy. 2008 Dec; 28(12):1552.
9. Negrini D. Sheppard L. Mills GH. et.al., International Programme for Resource Use in Critical Care (IPOC)--a methodology and initial results of cost and provision in four European countries. Acta Anaesthesiologica Scandinavica. 2006 Jan; 50(1):72-9.
10. Gasperino J. The Leapfrog initiative for intensive care unit physician staffing and its impact on intensive care unit performance: A narrative review. Health Policy. 2011 Mar 23.
11. Schumock GT. Butler MG. Meek PD. et.al., 2002 Task Force on Economic Evaluation of Clinical Pharmacy Services of the American College of Clinical Pharmacy. Evidence of the economic benefit of clinical pharmacy services: 1996-2000. Pharmacotherapy. 2003 Jan; 23(1):113-32.
12. Anderson SV, Schumock GT. Evaluation and justification of clinical pharmacy services. Expert Rev Pharmacoecon Outcomes Res. 2009 Dec; 9(6):539-45.
13. Seferian EG. Afessa B. Demographic and clinical variation of adult intensive care unit utilization from a geographically defined population. Critical Care Medicine. 2006 Aug; 34(8):2113-9.
14. Sirio CA. Critical care performance measurement: the time has come for all. Critical Care Medicine. 2006 May; 34(5):1538-9.
15. Erntoft S. Pharmaceutical priority setting and the use of health economic evaluations: a systematic literature review. Value Health. 2011 Jun; 14(4):587-99.
陸、附表 表 1 每人每日平均藥物費用及加護病房平均入住天數差異性分析 變項 93 年 94 年 t-test p 值 平均值 標準差 平均值 標準差 每日平均藥費 4253.1 4146.5 3358.6 4045.8 0.0826* ICU 入住天數 6.1509 5.029 5.4803 4.2984 0.2516 *p< 0.1 表 2 病人因素及病房因素與平均藥物費用之相關性 變項 回歸係數 標準化係數 標準誤 P 值 藥師是否參與每日查房 否(參考組) 是 -711.083 -0.034 1333.668 0.594 醫師年資 -161.521 -0.091 115.350 0.163 年齡 -74.132 -0.116 41.674 0.077 性別 男(參考組) 女 -1170.666 -0.054 1434.952 0.415 入病房 APACH II 值 0-19(參考組) 20-29 -2085.223 -0.071 1980.863 0.294 30-34 -15025.000 -0.160 6971.583 0.032 >=35 -290.595 -0.003 7143.369 0.968 出病房 APACH II 值 0-19(參考組) 20-29 21761.000 0.298 5364.273 <0.001* 診斷項次 783.831 0.075 691.039 0.258 ICU 天數 -209.114 -0.111 128.947 0.106 *p<0.05
表 3 病人因素及病房因素與平均加護病房入住天數之相關性 變項 回歸係數 標準化係數 標準誤 P 值 藥師是否參與每日查房 否(參考組) 是 -1.341 -0.120 0.672 0.047* 醫師年資 -0.095 -0.101 0.058 0.105 年齡 0.039 0.117 0.021 0.062 性別 男(參考組) 女 0.543 0.047 0.728 0.456 入病房 APACH II 值 0-19(參考組) 20-29 4.254 0.272 0.967 <0.001* 30-34 8.568 0.172 3.497 0.015* >=35 0.121 0.002 3.629 0.973 出病房 APACH II 值 0-19(參考組) 20-29 -0.292 -0.008 2.725 0.915 診斷項次 0.267 0.048 0.351 0.447 *p<0.05
Abstract
Background: The U.S. SCCM (Society of Critical Care Medicine) distinctly states the importance of the role of pharmacists in the critical care team. The involvement of pharmacists can prevent adverse drug events and reduce costs of care. Many reports from both domestic and overseas on improvement of quality of medical services from inpatient pharmaceutical care can be found. However, there are limited published articles on economic-based impacts of pharmacists’ intervention in Taiwan.
Methods: The study drew upon the two types in manpower allocations of pharmacists in an MICU that explored the variations in average drug expenditures and their length of stay. Independent t test was performed to investigate difference of drug expenditures and LOS. Microsoft SAS 9.1 was employed in the analysis of the data.
Results: There is no significant difference between the study and control group with regards to age, sex, bed occupancy rate, seniority of attending physicians and nurses or APACH II scores of admission to and discharge from the MICU. Therefore, observations based simply on medication expenses revealed a daily savings of NT 894 per individual. As length of stay, have a reduction of 0.67 day.
Discussions: Aside from improving quality of medical services and in medication safety, the above results further ascertained the contributions of pharmacists to the ICU medical team. The importance of the roles of pharmacists in the appraisal of medical economic benefits is apparent.