Analysis of changes to the anterior chest wall after the Nuss
procedure
—an objective measurement of pectus excavatum
Pei-Yeh Chang
a, Chaur-Hsiang Chang
b, Jin-Yao Lai
a,
Jeng-Chang Chen
a, Der-Baau Perng
b, Qi Zeng
c,⁎
a
Division of Pediatric Surgery, Department of Surgery, Chang Gung Memorial Hospital, Chang-Gung University, College of Medicine, Taoyuan, Taiwan
b
Department of Industrial Engineering and Management, National Chiao Tung University, Hsinchu, Taiwan
c
Department of Pediatric Surgery, Beijing Children Hospital, Capital Medical University, Beijing 100045, China
Received 20 July 2009; accepted 31 July 2009
Key words: Pectus excavatum; Nuss procedure; Anthropometry; Thoracic wall; Surgical outcome Abstract
Introduction: We report a noninvasive method for recording the deviation of the anterior chest wall (ACW) in patients with pectus excavatum before and after the insertion and removal of a Nuss bar. Patients and Method: All patients undergoing the Nuss procedure at our institutions between June 2008 and February 2009 were enrolled in this study. A thermal plastic strip was used to cast the ACW at the skin level along the area corresponding to the tract of the inserted bar. The height of the ACW was defined as the perpendicular length from the xiphoid process to the transverse line drawn between the 2 midaxillary points. Results: Bar insertion caused a significant increase in ACW height and width. Bar removal reduced the corrective effects in terms of a significant decrease in ACW height; at the same time, an increase in ACW width was noted.
Conclusion: Feature extraction and analyses of permanent contour casts of the ACW help to understand immediate changes in the ACW after the Nuss procedure and may assist in the design of the bar at insertion. The Nuss bar in situ helped to maintain cosmetic benefits to the ACW.
© 2009 Elsevier Inc. All rights reserved.
Most patients with pectus excavatum (PE) can be diagnosed within the first 2 years of life[1]. The severity of funnel chest varies widely, even with an asymmetric chest wall deformity. We used a plastic strip to cast the surface contour of the anterior chest wall (ACW) as a record of the corrective efficacy of the Nuss procedure for PE. This method allows repeated measurements over time, minimiz-ing the need for radiographic evaluation. The benefit of
longitudinal follow-up is that it improves our understanding of the natural history of this disorder, and the efficacy of any modified Nuss procedure can be assessed more accurately.
1. Methods
1.1. Patients
All PE patients who underwent Nuss procedures at either of the participating institutions between June 2008 and
Presented at the 42nd Annual Meeting of the Pacific Association of Pediatric Surgeons, Hong Kong, China, May 10-14, 2009.
⁎ Corresponding author. Tel.: +86 13801371712; fax: +86 10 68011503. E-mail address:zengqi-1@163.com(Q. Zeng).
www.elsevier.com/locate/jpedsurg
0022-3468/$– see front matter © 2009 Elsevier Inc. All rights reserved. doi:10.1016/j.jpedsurg.2009.07.053
February 2009 were enrolled in this study. The study protocol was explained to the patients and their families and approved by the ethics committees of our institutions (institutional review board 97-2410B).
1.2. Measurement
The ACW was cast using a 3-mm-thick strip of thermal plastic (Orthoplast Splint; DePuy Casting, a branch of Johnson-Johnson). A 45.7 × 60.9-cm Orthoplast sheet was cut into strips measuring 10 mm × 60.9 cm using a press machine. The strip was quite plastic in hot water (water temperature was approximately between 60°C and 80°C when the plastic strip was dipped into the basin). After allowing the strip to cool to approximately between 35°C and 40°C, it was positioned and taped to the supine patient's ACW from the posterior axillary line, crossing the left incision line, depressed sternum, and right incision line to the contralateral posterior axillary line (Fig. 1).
This line was well correlated with the tract of the Nuss bar. The points corresponding to the xiphoid process and
both incisions and axillary lines were marked on the strip for later analyses. After the strip solidified (in approximately 10 min), it was removed from the ACW and kept as a permanent record. The strip then was scanned to obtain a 2-dimensional chest wall contour. The measurement was repeated 1 day before and after surgery for bar insertion or removal. None of our patients experienced minor burns or skin trauma due to the strip in our study.
1.3. Calculations
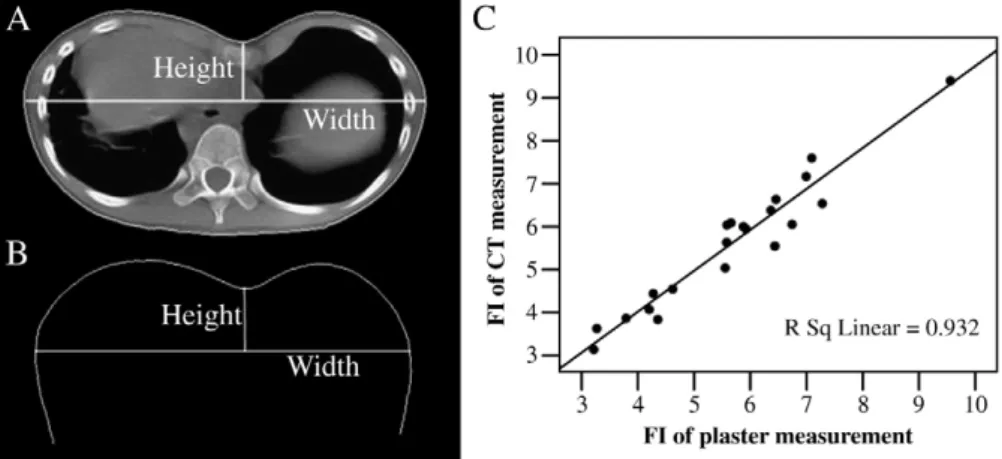
The width of the ACW was defined as the distance between the 2 midaxillary points, or the widest dimension of the chest wall. The height of the ACW was defined as the perpendicular length from the xiphoid process to the line drawn between the 2 midaxillary points. The funnel index (FI) was defined as the width of the ACW divided by its height (Fig. 2), representing the severity of PE in this study. To compare data for different plastic strips, we divided the width of ACW into 65 equidistant points and calculated the perpendicular height from each point to the relative point on
Fig. 1 A, A thermal plastic strip was taped to the ACW to obtain a permanent contour. B, The strip represents a cross-sectional view of the ACW at the sternal end. C, Image obtained from scanning the strip.
Fig. 2 The FI was defined as the width divided by the height of the depressed area at the sternal end. A, Measurements obtained from a CT image. B, Measurements obtained from plastic strip images. C, The correlation coefficient for FI measurements obtained from plastic strips and CT images in 21 PE patients was 0.932.
the contour of the ACW. Then, we used the average width and height data for the 79 patients to construct chest wall contours before and after insertion of the Nuss bar (Fig. 3), and we used the average width and height data of 26 patients to construct the chest wall contours before and after bar removal (Fig. 4).
1.4. Statistics
The correlations between height, width, and FI obtained from both the plastic strips and the equivalent computed tomography (CT) image contours were compared using Pearson correlation coefficient. Paired-sample Student's t tests were performed to detect changes in ACW contour immediately after inserting or removing the Nuss bar.
2. Results
2.1. Demographic data
Seventy-nine patients (62 males, 17 females) ranging in age from 3 to 16 years (mean, 7.95 ± 4.12 years) had bars inserted. Another 26 patients (18 males and 8 females) ranging in age from 6 to 17 years (mean, 8.12 ± 4.73 years) had bars removed. No patient had both insertion and removal data.
2.2. Chest wall changes after the Nuss procedure
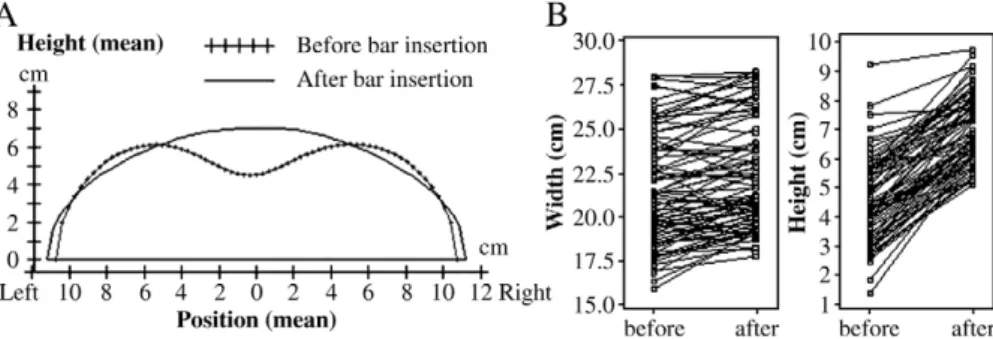
We compared the changes in the shape of the ACW before and after insertion or removal of the Nuss bar. The elevation of the depressed sternal end was accompanied by bilateral depression of the costicartilage junction area, which is prominent preoperatively, as shown inFig. 3andTable 1. The average elevation of the sternal end was 2.49 cm. Immediately after removing the bar, the xiphoid process was depressed an average of 1.12 cm, as shown inFig. 4andTable 2. The chest wall was significantly wider (1.61 cm) after bar removal.
2.3. Reliability of the plastic strip measurement
Before bar insertion, the ACW was measured from both CT images and plastic strips in 21 patients. These data of the FI were used to study the reliability of the plastic strip measurement. The group included 16 males and 5 females, ranging in age from 3.5 to 15 years (mean, 8.82 ± 3.33 years). Measurements obtained via CT and plastic strips were strongly correlated (Fig. 2C).
3. Discussion and conclusion
In the Nuss procedure, both insertion and removal of the bar create new stresses and strains on the chest wall. To
Fig. 3 A, Changes in the contour of the ACW after bar insertion. The shapes represent the mean width and height changes in 79 patients. B, A ladder plot of the width and height changes before and after insertion. Paired-sample t tests for both width and height changes before and after insertion were significant (Pb .001, paired t test).
Fig. 4 A, Changes in the contour of the ACW after bar removal. The curves represent the mean width and height changes in 26 patients. B, A ladder plot of the width and height changes before and after bar removal. Paired-sample t tests for both the width and height changes before and after removal were significant (Pb .001, paired t test).
obtain the best and most persistent cosmetic result after bar removal, it is necessary to determine the optimal Nuss procedure, including the number, shape, and location of the bars. It is also necessary to determine how long the bar must be kept in place to avoid recurrence. Currently, no consensus has been reached regarding the elective removal of metallic implants in children[2], and it is unclear whether adult and pediatric patients exhibit the same chest wall changes after bar removal. In addition, the cosmetic outcome of modified Nuss procedures (ie, using tailored asymmetric bars when treating asymmetric patients) requires objective evaluation. To resolve these various issues, a method to obtain objective measurements is required. This preliminary study reports a simple technique to record ACW changes in PE patients after surgical correction.
Until now, the success of a Nuss procedure has been based on a subjective evaluation by the surgeons or answers to a questionnaire by the patients or their parents. Although CT allows an objective evaluation of sternal elevation [3], irradiation makes this modality less than ideal for long-term follow-up, which requires multiple measurements. Optical measurement of the torso can give 2-dimensional images of the chest wall deformity without radiation exposure[4], but these methods require sophisticated software and equipment. From a cosmetic perspective, direct anthropometric mea-surements of the ACW are 1-dimensional and insufficient for assessing all chest wall changes [5]. In contrast, feature extraction and analysis of molded plastic strips have been used to record head shape changes during early infancy with some success[6,7].
Three definite landmarks are monitored during the long-term follow-up of PE: the 2 incision wounds and the tip of the xiphoid process. These landmarks can also be monitored by placing a plastic strip across the chest wall. Although the plastic strip method does not represent bony
changes in the chest wall, it records surface changes in the ACW, which are of greatest concern to the patient. In addition, measurements using this method were strongly correlated with CT measurements.
Sternal elevation is expected after inserting the metal bar, regardless of the severity of chest depression or age, whereas the counterforce causes downward displacement of the chest wall upon bar exit from the intrapleural space, which is corresponding to the costocartilage junction[8].Fig. 3shows mean patient dimensions before and after inserting the Nuss bar. An increased width is expected because the bar adds thickness to the chest wall.
We also observed significant recoil of the sternal end after removing the bar, showing that the bar maintains the chest wall contour in a better shape before removal. Chest wall growth during the 2 to 3 years in which the bar was in place did not fully adapt to the force exerted by the bar. If the chest wall shape is satisfactory to the surgeons and the patient/ parents before removing the bar, then the small decrease in the height of the sternum upon removal is generally imperceptible or acceptable. In some cases, however, it may be necessary to compensate for the recoil of the chest wall after removing the bar by slightly overcorrecting at the time of insertion.
The increase in width accompanying the recoil of the elevated sternum may be due to the sudden release of the restriction of the chest wall caused by bar removal. The restriction of chest wall growth caused by mechanical constraints, such as protective outerwear, has been reported
[9]. Chest wall restriction was also observed on CT after bar removal in our patients. Thus, long-term longitudinal follow-up is necessary to understand dynamic changes in the chest wall, which result from the balance between the growth capability of the ACW and the force exerted upon it by the bar.
Table 1 Measurements before and after bar insertion (n = 79)
Variables Width (cm) Height (cm)
Mean SD Range Mean SD Range
Before 21.44 3.17 15.90 to 28.02 4.53 1.44 1.36 to 9.23
After 22.38 3.08 17.73 to 28.30 7.03 1.17 5.09 to 9.76
Paired difference 0.94 1.45 −3.27 to 4.00 2.49 1.08 0.16 to 5.60
P b.001 b.001
Table 2 Measurements before and after bar removal (n = 26)
Variables Width (cm) Height (cm)
Mean SD Range Mean SD Range
Before 22.70 2.87 18.59 to 28.02 8.86 1.34 6.41 to 11.16
After 24.31 2.66 20.36 to 29.31 7.73 1.15 5.68 to 9.60
Paired difference 1.61 0.88 −0.08 to 3.64 −1.12 0.60 −2.26 to −0.07
References
[1] Fonkalsrud EW. Current management of pectus excavatum. World J Surg 2003;27:502-8.
[2] Peterson HA. Metallic implant removal in children. J Pediatr Orthop 2005;25:107-15.
[3] Nakagawa Y, Uemura S, Nakaoka T, et al. Evaluation of the Nuss procedure using pre- and postoperative computed tomographic index. J Pediatr Surg 2008;42:518-21.
[4] Poncet P, Kravarusic D, Richart T, et al. Clinical impact of optical imaging with 3-D reconstruction of torso topography in common anterior chest wall anomalies. J Pediatr Surg 2007;42: 898-903.
[5] Brigato RR, Cam pos JR, Jatene FB, et al. Pectus excavatum: evaluation of Nuss technique by objective methods. Interact Cardiovasc Thorac Surg 2008;7:1084-8.
[6] Chang NC, Chang PY, Perng DB, et al. Feature extraction and analysis of head ring images. Chin J Med Biol Eng 2000;20:83-91.
[7] Van Vilmmeren LA, Takken T, Van Adrichem LNA, et al. Plagioce-phalometry: a non-invasive method to quantify asymmetry of the skull; a reliability study. Eur J Pediatr 2006;165:149-57.
[8] Chang PY, Hsu ZY, Chen DP, et al. Preliminary analysis of the forces on the thoracic cage of patients with pectus excavatum after the Nuss procedure. Clin Biomech 2008;23:881-5.
[9] Gonzalez J, Coast JR, Lawler JM, et al. A chest wall restrictor to study effects on pulmonary function and exercise. The energetics of restrictive breathing. Respiration 1999;66:188-94.