Prolonged Effect of Botulinum Toxin Injection in the Treatment of
Cricopharyngeal Dysphagia: Case Report and Literature Review
Ming-Jang Chiu, MD, PhD,
1Yeun-Chung Chang, MD,
2and Tzu-Yu Hsiao, MD, PhD
31
Department of Neurology,2Department of Medical Imaging,3Department of Otolaryngology, National Taiwan University Hospital, College of Medicine, National Taiwan University, Taipei, Taiwan
Abstract. Cricopharyngeus (CP) muscle spasm can
lead to severe dysphagia. Myotomy of the CP muscle
was the treatment of choice. Recently, botulinum
toxin type A (BtxA) has been used for CP spasm. It
usuallybrings improvement in deglutition but most
patients require reinjection in 3–5 months. We report
a 35-year-old man who had an arteriovenous
mal-formation hemorrhage in the brain stem resulting in
CP spasm and consequentlysevere dy
sphagia. He
received BtxA injection and deglutition and nutrition
remained good one year after treatment. A literature
review analyzing 28 patients and our patient showed
negative correlations between age and BtxA dose and
between age and duration. Efficacywas positively
correlated with duration and BtxA dose was
posi-tivelycorrelated with pretreatment severity. In
con-clusion, physicians would use higher doses on
pa-tients with more severe cases but use lower doses on
older patients. Those who obtained better
post-treatment results would enjoylonger effective
dura-tion. Thus, the effective duration of the BtxA is
multifactorial.
Key words: Botulinum toxin type A —
Crico-pharyngeus muscle spasm — Dysphagia —
Deglu-tition — DegluDeglu-tition disorders.
Botulinum toxin type A (BtxA) is of significant
therapeutic value in the management of a varietyof
hyperkinetic disorders such as blepharospasm,
tor-ticollis, writer’s cramp, orofacial dystonia, and
spasmodic dysphonia [1]. It is also efficacious in the
treatment of facial nerve disorders such as synkinesis
or hemifacial spasm. It has also been applied in the
treatment of esophageal motilitydisorders such as
achalasia, hypertensive lower esophageal sphincter,
and upper esophageal sphincter spasm [2,3,4].
Dys-phagia due to hyperactivity of the upper esophageal
sphincter (UES), more specificallythe cricophary
n-geal (CP) muscle, can be seen in a varietyof
neu-rological
disorders
such
as
cerebral
vascular
accidents, amyotrophic lateral sclerosis, multiple
sclerosis, acoustic neuroma, and Parkinson’s disease.
It can also occur after surgical procedures for the
head and neck such as in resections for
oropha-ryngeal and supraglottic carcinoma as a
1
result of
iatrogenic injuryto the pharyngeal or recurrent
la-ryngeal nerves. Some causes of dysphagia are
idio-pathic [4–7]. Traditionally, surgical myotomy of the
CP muscle is the treatment of choice for
hyperac-tivityof the UES due to various causes [8,9].
However, CP myotomy is invasive and is not always
effective [8]. BtxA was introduced in 1989 by
Schneider et al. [4] for patients with spasticity,
hypertonus, or delayed relaxation of the UES. The
intervention usuallybrings improvement in
degluti-tion but most patients require reinjecdegluti-tion in 3–5
months [5]. We report a patient with a brain stem
stroke who was left with CP sphincter spasm and
consequentlysevere dy
sphagia. He received BtxA
injection and deglutition and nutrition remained
good one year after injection. This is unusually long
for BtxA treatment in terms of its mode of action in
which neuromuscular transmission is
usuallyre-stored within 3–4 months. Thus, we did a literature
review to explore factors affecting the efficacyand
duration of BtxA treatment.
Correspondence to: Tzu-Yu Hsiao, M.D., Department of Otolar-yngology, National Taiwan University Hospital, 7, Chung-Shan S. Rd., Taipei, 100, Taiwan. Telephone: 886-2-23123456 ext. 5214; Fax: 886-2-23410905; E-mail: [email protected]
Case Report
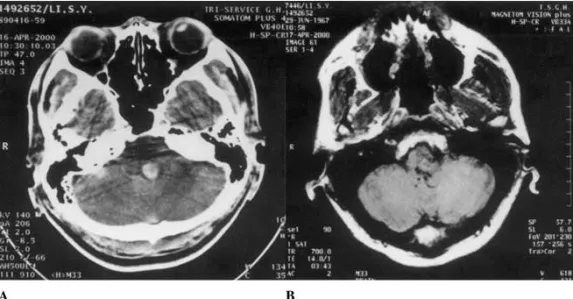
The patient was a 35-year-old man who suffered from severe dys-phagia with a disabilityrating scale (DRS) score of 4 [4] for about one and a half years after an episode of acute consciousness im-pairment from an arteriovenous malformation (AVM) hemorrhage in the left posterior pontomedulla (Fig. 1A,B). He received emer-gencysurgeryfor decompression and removal of blood clots. After the surgery, he gradually regained consciousness and motor func-tions. However, he was left with severe swallowing disturbance and required nasogastric tube feeding. Afterward, he had a significant bodyweight loss from a premorbid baseline of 73–74 kg to 66 kg (bodyheight = 175 cm). The neurological examination on ad-mission revealed leftward gaze palsy, left abducens palsy, and left peripheral-type facial palsy. Mild dysarthria with minimal hyp-ernasalitywas noted. Mild vocal cord palsyon the left side was also observed during laryngoscope examination. Hemihypoesthesia to pinprick and thermal stimulation over the right side of his body was also detected. No definite motor deficits, including weakness, muscle tone change, or abnormal tendon reflex, were detected. He could not drink even 20–30 ml of water without having to spit it out. Videofluoroscopic swallowing study(VFSS) showed almost no passage of barium into the esophagus. It showed severe dysphagia
with lower pharyngeal constrictor dysfunction or upper esophageal spasm. With written informed consent from the patient we per-formed an intrasphincteric BtxA injection.
About two weeks after the injection, the patient started oral feedings. He could drink small swallows of water and eat semisolid food such as pudding (DRS: 2). His swallowing con-tinued to improve and he could eat solid food the third week (DRS: 1). His bodyweight returned to 74 kg two months after the treatment (DRS: 0–1 ) and remained around 72 kg. At the one-year followup, his neurological condition was stable. He could eat and swallow almost normallyexcept for hard solid food at a rapid speed (DRS: 0–1). He had no complications such as acid regurgitation or belching from aerophagia. He received an-other VFSS about 10 months after the injection of BtxA (de-scribed below).
BtxA Injection Method
BtxA was obtained from Dysport (IPSEN, Berkshire, UK) as freeze-dried lyophilized preparation. For clinical use, BtxA ac-tivityis defined in units, 1 unit representing the estimated median lethal dose for mice. Shortlybefore use, the toxin was dissolved with 2.5 ml of 0.9% sterile saline solution (without preservative), equivalent to 500 units. Under general anesthesia and direct lar-yngoscopic guidance, the bulk of the CP muscle was clearly identified. Botulinum toxin 0.6 ml, containing an equivalent dose of about 120 units of Dysport per site, was injected into the left and right lateral sides and the dorsomedial part of the muscle (Fig. 2).
VFSS
VFSS was performed with thin barium (5 ml), thick barium (5 ml), and paste barium (5 ml) in the lateral view and thin barium (5 ml) in the anterior–posterior view. The preinjection VFSS (about 3 months prior to the injection) showed almost no passage of barium into the esophagus with occasional pharyngeal–oral reflux, and laryngeal penetration (Fig. 2A). There was no aspiration. Poor contractilityof the lower pharyngeal segment with massive move-ment was also noted. VFSS showed a severe dysphagia with lower pharyngeal constrictor dysfunction or upper esophageal spasm. Fig. 1. A Preoperation cranial computed tomographyshows a hematoma in the left posterior pons. B The postoperation magnetic resonance imaging of the head reveals an arteriovenous malformation in the left pontomedulla.
Fig. 2. Under laryngoscopic view, the cricoid (C), esophageal lumen (E), and bulk of the cricopharyngeal muscle (CP) are clearly visible. The asterisks indicate the three injection sites.
The first postinjection VFSS (about one month after the injection) revealed left-side predominant bilateral passage into the esophagus but no pharyngeal–oral reflux or pharyngeal–nasal reflux. The second postinjection VFSS (about 10 months after the injection) showed left predominant passage into the esophagus with mild oropharyngeal dysphagia (Fig. 2B).
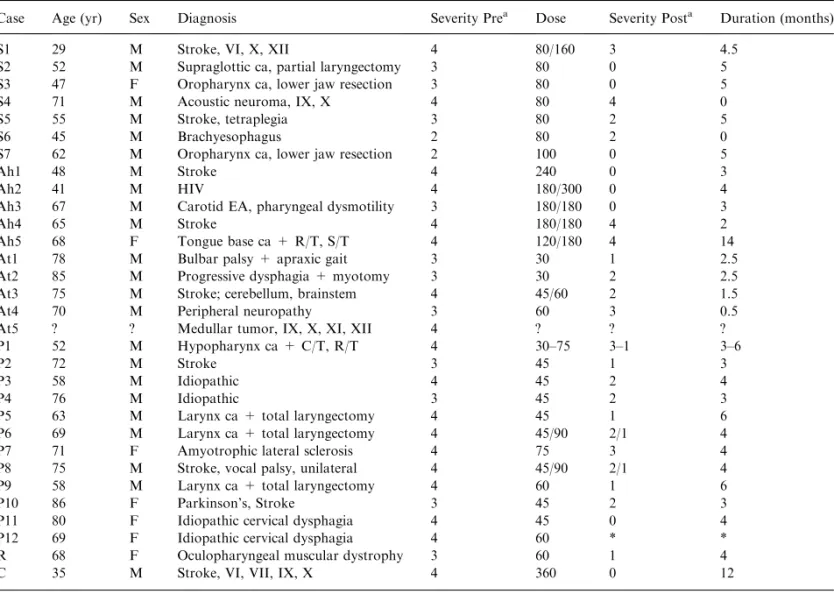
We reviewed the literature, focusing on the efficacyof the BtxA injection and duration of effects. For this purpose, we searched MEDLINE using keywords cricopharyngeus, cricopha-ryngeal muscle, spasm, spasticity, hypertonus, dysphagia, deglu-tition disorder, swallowing disorder and BtxA; we found 7 reported series or cases reports [4,5,10–14]. We analyzed 28 of 30 cases from 5 reports [4,10–12,14] in which there was detailed in-formation on clinical diagnosis, severity, injection dose, efficacy, and duration of response to BtxA intervention. Together with our patient, 29 cases were subjected to further analysis (Table 1). The clinical severityof dysphagia was transformed into Schneider’s 5-point scale (0–4) DRS [4] for comparison. In Schneider’s DRS, score 0 indicates normal function, patient without complaints; score 1: no functional impairment, but subjective dysphagia when swallowing solid and/or liquid foods; score 2: mild functional impairment for solid and/or liquid food; score 3: marked disa-bilitywith moderate aspiration; and score 4: severe functional impairment with complete inabilityto swallow, considerable as-piration, and pneumonia. The efficacywas computed bysub-tracting the post-treatment DRS score from the pre-treatment score. Doses were transformed into Dysport equivalent units with
the ratio of Dysport:Botox = 3:1 [15, 16]. In cases with multiple treatments, the dose with the longest effective duration was used for analysis.
Results
Descriptive statistics were reviewed in 6 women and
23 men with an average age of 62.8 ± 14.6 years. The
mean pretreatment DRS score was 3.48 ± 0.63 and
mean post-treatment DRS score 1.48 ± 1.30 with a
mean Dysport equivalent dose of 110.2 ± 79.1 units.
The mean effective duration was 4.2 ± 2.9 months
with a mean efficacyof 2.00 ± 1.34 change in DRS
score. For exploring efficacyin patients with different
clinical diagnoses, patients were further categorized
into three groups; Group 1, patients with
cerebro-vascular diseases, i.e., strokes (n = 10); Group 2,
patients with malignancies in the tongue base,
oro-pharynx, hypooro-pharynx, supraglottis, or larynx who
suffered peripheral nerve injuries after surgeryin the
upper neck (n = 13); Group 3 consisted of patients
Fig. 3. A Videofluoroscopic swallowing study(VFSS) about 3 months prior to injection shows almost no passage of barium into the esophagus, pharyngeal– oral reflux, and mild laryngeal penetration. There is no aspiration. Poor contractilityof the lower pharyngeal segment with massive movement is noted. B VFSS, about 10 months after the injection shows left pre-dominant passage into esophagus with a mild oropharyngeal dysphagia and minimal laryngeal penetration.
with other causes such as idiopathic dysphagia
(n = 6). A Kruskal–Wallis test showed no significant
differences in the three groups for age, pretreatment
DRS score, post-treatment DRS score, efficacy, dose
of BtxA applied, and effective duration. However,
Spearman rho correlation showed that age was
neg-ativelycorrelated with the dose of BtxA (r =
)0.598,
p
< 0.0001) and with duration of efficacy(r =
)0.463, p = 0.006). Efficacywas positivelycorrelated
with duration of efficacy(r = 0.448, p = 0.007). Dose
was not significantlycorrelated with efficacyor
du-ration but it was positivelycorrelated with the
pre-treatment DRS score (r = 0.370, p = 0.024). In other
words, although physicians used higher doses in more
severe cases, theyalso tended to use lower doses on
older patients, probablybecause the elderlyhad
de-creased muscle mass. The elderlyseemed to have
shorter effective duration. Those who obtained better
post-treatment results enjoyed longer duration of
effectiveness.
Discussion
UES spasm can have serious consequences leading to
complete inabilityto swallow, as in our case. BtxA
has been demonstrated to be therapeutic for CP
muscle spasm and hypertonicity. It can be used in
evaluating patients for permanent treatment such as
CP myotomy [5].
BtxA binds to the motor nerve terminal with
its heavychain [17], which is selective for cholinergic
nerve terminals. It is then internalized via endocytosis
[18], forming a vesicle inside the nerve terminal and
releasing its light chain into the cytoplasm [19]. It
blocks acetylcholine release by cleaving SNAP-25, a
cytoplasmic protein on the cell membrane, for release
of this transmitter [20]. Paralysis occurs as the
com-plete loss of miniature endplate potential starts.
Therefore, the therapeutic effects of muscle weakness
are usuallyevident after a certain latencyranging
from a few days to 2–3 weeks. Chemical denervation
Table 1. Data from 31 patients with CP dysphagia
Case Age (yr) Sex Diagnosis Severity Prea Dose SeverityPosta Duration (months)
S1 29 M Stroke, VI, X, XII 4 80/160 3 4.5
S2 52 M Supraglottic ca, partial laryngectomy 3 80 0 5
S3 47 F Oropharynx ca, lower jaw resection 3 80 0 5
S4 71 M Acoustic neuroma, IX, X 4 80 4 0
S5 55 M Stroke, tetraplegia 3 80 2 5
S6 45 M Brachyesophagus 2 80 2 0
S7 62 M Oropharynx ca, lower jaw resection 2 100 0 5
Ah1 48 M Stroke 4 240 0 3
Ah2 41 M HIV 4 180/300 0 4
Ah3 67 M Carotid EA, pharyngeal dysmotility 3 180/180 0 3
Ah4 65 M Stroke 4 180/180 4 2
Ah5 68 F Tongue base ca + R/T, S/T 4 120/180 4 14
At1 78 M Bulbar palsy+ apraxic gait 3 30 1 2.5
At2 85 M Progressive dysphagia + myotomy 3 30 2 2.5
At3 75 M Stroke; cerebellum, brainstem 4 45/60 2 1.5
At4 70 M Peripheral neuropathy3 60 3 0.5
At5 ? ? Medullar tumor, IX, X, XI, XII 4 ? ? ?
P1 52 M Hypopharynx ca + C/T, R/T 4 30–75 3–1 3–6
P2 72 M Stroke 3 45 1 3
P3 58 M Idiopathic 4 45 2 4
P4 76 M Idiopathic 3 45 2 3
P5 63 M Larynx ca + total laryngectomy 4 45 1 6
P6 69 M Larynx ca + total laryngectomy 4 45/90 2/1 4
P7 71 F Amyotrophic lateral sclerosis 4 75 3 4
P8 75 M Stroke, vocal palsy, unilateral 4 45/90 2/1 4
P9 58 M Larynx ca + total laryngectomy 4 60 1 6
P10 86 F Parkinson’s, Stroke 3 45 2 3
P11 80 F Idiopathic cervical dysphagia 4 45 0 4
P12 69 F Idiopathic cervical dysphagia 4 60 * *
R 68 F Oculopharyngeal muscular dystrophy 3 60 1 4
C 35 M Stroke, VI, VII, IX, X 4 360 0 12
?: not specified; *: lost followup; Dose: Dysport equivalent units (Dysport : Botox = 3:1).
aSeverityfollowing S: Schneider [4]; Ah: Ahsan [11]; At: Atkinson [10]; P: Parameswaran [12]; R: Restivo [14]; C: Chiu; ca: carcinoma; C/T: chemotherapy; R/T: radiotherapy; S/T: surgery; EA: endarterectomy.
of the neuromuscular junction byBtxA results in an
expansion of the end-plate region and growth
stim-ulation of collateral axonal sprouts [21]. A nerve
sprout eventuallyestablishes a new neuromuscular
junction, and muscle activitygraduallyreturns. But
evidence also suggests the new nerve sprout retracts
and the original junction returns to functionality[22].
Theoretically, effects are not permanent, lasting an
average of 3–4 months, which is the time needed for
re-establishing new neuromuscular junctions and
muscle activity. Our patient maintained good
deglu-tition for more than one year after BtxA injection. He
was the second youngest patient in our analysis and
responded verywell to the BtxA injection of 360
Dysport units. Although our patient received the
highest dose of BtxA among all reviewed cases, the
relation between the dose and duration of efficacy
was not substantiated bystatistics. Some cases in our
reviewed series used doses of BtxA up to 240 (Case
Ah1) or 300 (Case Ah2) units but theysustained a
duration of about 3–4 months (Table 1). Thus, the
unusuallyprolonged duration of effectiveness cannot
be fullyelucidated just through the denervation and
sprouting of the motor endplate. Other possible
mechanisms should be considered.
In our patient, the lesion involved the dorsal
pontomedulla affecting the corticoreticular tract and
fibers leading to the dorsal recticulospinal tract, which
is of crucial importance in the facilitation of the
in-hibitoryfunction from cortical neurons. The influence
of cortical motor areas over tone is
principallymedi-ated bya powerful mechanism in the bulbar reticular
formation. Loss of inhibitoryinfluence from the
cor-ticoreticular tract leaves the facilitating effects of the
ventromedial reticular formation unopposed [23]. In
this situation, severe spasticitywith hy
pertonia is
greatest in the antigravityor postural-maintaining
muscles (composed of mainlyslow fibers) such as the
closure maintaining CP muscle. Reduction of muscle
tone following treatment with BtxA results from effects
of muscle denervation as well as inhibition of the
fus-iform system and muscle spindle [24]. Motor
innver-vation of the intrafusal muscle fibers comes from
small-diameter motor neurons, called gamma motor neurons
to distinguish them from the large-diameter alpha
motor neurons. The gamma motor neurons provide a
mechanism for adjusting the sensitivityof the muscle
spindles. When a muscle is stretched, e.g., the CP
muscle is stretched during passage of a bolus coming
down from the oropharynx, the Ia afferents in the
muscle increase their firing rates leading to excitation
of the alpha motor neurons and contraction of the
muscle via the reflex arc. The activation of gamma
motor neurons causes increased intensityor lowered
threshold of the sensoryafferents’ firing from the
in-trafusal spindles. This coactivation of alpha and
gamma motor neurons serves as a feedback
mecha-nism from muscle spindles to reinforce the activation
of the alpha motor neurons. The swallowing peristaltic
waves come down from the oropharynx and the upper
pharynx to the CP muscle. The CP orifice completes
the bolus passage through three steps. First is
relaxa-tion and opening of the orifice. At this point, an
ab-normal hyperactive stretch reflex of the muscle would
impede the relaxation and thus prevent opening of the
orifice. Second, after the opening, the CP muscle
con-tracts and closes the orifice. Finally, it returns to the
resting state [25]. In the human CP muscle, the
hori-zontal inner layer contains more slow fibers while the
outer oblique layer contains more fast fibers [26].
In-terestingly, sprouting is generally slower in fast-twitch
muscles, which are more crucial in the stretch reflex,
than in slow-twitch muscles with predominantlytype I
fibers [27]. Thus, muscle-fiber-type specificity unique in
human CP muscle could be an additional factor in
prolonged effectiveness.
In conclusion, the effective duration of BtxA
injection in relieving CP spasm is multifactorial,
es-peciallyin cases with brain stem stroke. It differs
from a simple denervation–reinnervation process as
in cases of hemifacial spasm. It also differs from
hyperkinetic disorders such as spasmodic dysphonia
in that hypertonia results from rigidity but not
spasticity. It also differs from spastic paresis, which
occurs in areas other than the CP muscle where
fiber-type specificity is not seen. A prolonged effect has
also been seen in upper [11] and lower esophagus
spasm [28]. Further studyon the mechanism is still
necessaryto clarifythis interesting and important
phenomenon.
References
1. Jankovic J, Brin MF: Therapeutic use of botulinum toxin. N Engl J Med 324:1186–1192, 1991
2. Pasricha PJ, Ravich WJ, Hendrix TR, Sostre S, Jones B, Kalloo AN: Intrasphincteric botulinum toxin for the treat-ment of achalasia. N Engl J Med 332:774–778, 1995 3. Jones MP: Botulinum toxin in hypertensive lower esophageal
sphincter. Am J Gastroenterol 91:1283–1284, 1996
4. Schneider J, Thumfart W, Potoschnig C, Eckel HE: Treat-ment of dysfunction of the cricopharyngeal muscle with botulinum A toxin: introduction of a new, noninvasive method. Ann Otol Rhinol Laryngol 103:31–35, 1994 5. Blitzer A, Brin MF: Use of botulinum toxin for diagnosis
and management of cricopharyngeal achalasia. Otolaryngol Head Neck Surg 116:328–329, 1997
6. Blitzer A: Cricopharyngeal muscle spasm and dysphagia. Op Tech Otolaryngol Head Neck Surg 8:191–192, 1997
7. Born LJ, Harned RH, Rillers LF, Peiffer RF, QuigleyEM: Cricopharyngeal dysfunction in Parkinson’s disease: role in dysphagia and response to myotomy. Mov Disord 11:53–58, 1996
8. Mackenna JA, Dedo HH: Cricopharyngeal myotomy: indi-cations and technique. Ann Otol Rhinol Laryngol 101:216– 221, 1992
9. St. GuilyJ, Perie S, Willig T: Swallowing disorders in mus-cular disease: functional assessment and indication of crico-pharyngeal myotomy. Ear Nose Throat J 73:34–40, 1994 10. Atkinson SI, Rees J: Botulinum toxin for circopharyngeal
dysphagia: Case reports of CT guided injection. J Otolar-yngol 26:273–276, 1997
11. Ahsan SF, Meleca RJ, Dworkin JP: Botulinum toxin injec-tion of the cricopharyngeus muscle for the treatment of dysphagia. Otolaryngol Head Neck Surg 122:691–695, 2000 12. Parameswaran MS, Soliman AM: Endoscopic botulinum
toxin injection for cricopharyngeal dysphagia. Ann Otol Rhinol Laryngol 111:871–874, 2002
13. Restivo DA, Plameri A, Marchese–Ragona R: Botulinum toxin for cricopharyngeal dysfunction in Parkinson’s disease. N Engl J Med 346:1174–1175, 2002
14. Restivo DA, Marchese–Ragona R, Staffieri A, de Grandis D: Successful botulinum toxin treatment of dysphagia in oculopharyngeal muscular dystrophy. Gastroenterology 119:1416, 2000
15. Marion ME, SheehyM, Sangla S, Soulayrol S: Dose standardization of botulinum toxin. Lancet 59:102–103, 1995 16. Odergren T, Hjaltasaon H, Kaakkola S, Solders G, Hanko J, Fehling C, et al.: A double blind, randomized parallel group studyto investigate the dose equivalence of Dysport and Botox in the treatment of cervical dystonia. J Neurol Neu-rosurg Psychiatry 64:6–12, 1998
17. Brandypadhyay S, Clark AW, Desgupta BR, Sathyamoor-thyV: Role of the heavyand light chain of botulinum neu-rotoxin in neuromuscular paralysis. J Biol Chem 262:2660– 2663, 1987
18. Black JD, DollyJO: Interaction of125I-labeled botulinum neurotoxins with nerve terminals. II. Autoradiographic evi-dence for its uptake into motor nerves byacceptor-mediated endocytosis. J Cell Biol 103:535–544, 1986
19. Coffield JA, Considine RV, Simpson LL: The site and mechanism of action of botulinum neurotoxin. In: Jankovic J, Hallet M (eds.): Therapy with Botulinum Toxin. New York: Marcel Dekker, 1994, pp 3–13
20. Blasi J, Chapman ER, Link E, et al.: Botulinum neurotoxin A selectivelycleaves the synaptic protein SNAP-25. Nature 365:160–163, 1993
21. Alderson K, Holds JB, Anderson RL. Botulinum-induced alteration of nerve–muscle interactions in the human orbi-cularis oculi following treatment for blepharospasm. Neu-rology 41:1800–1805, 1991
22. de Paiva A, Meunier FA, Molgo J, Aoki KR, DollyJO: Functional repair of motor endplates after botulinum neu-rotoxin type A poisoning: biphasic switch of synaptic activity between nerve sprouts and their parent terminals. Proc Natl Acad Sci USA 96:3200–3205, 1999
23. Brown P: Pathophysiology of spasticity. J Neurol Neurosurg Psychiatry 57:773–777, 1994
24. On AY, Kirazli Y, Kismali B, Aksit R: Mechanisms of ac-tion of phenol block and botulinus toxin type A in relieving spasticity: electrophysiologic investigation and follow-up. Am J Phys Med Rehabil 78:344–349, 1999
25. Duchen LW: Changes in the electron microscope structure of slow and fast skeletal muscle fibres of the mouse after local injection of botulinum toxin. J Neurol Sci 14:61–71, 1971 26. Lund WS: The function of the cricopharyngeal sphincter
during swallowing. Acta Otolaryngol 59:497–510, 1964 27. Mu L, Sanders I: Muscle fiber-type distribution pattern in
the human cricopharyngeus muscle. Dysphagia 17:87–96, 2002
28. D’Onofrio V, Miletto P, Leandro G, Iaguinto G: Long-term follow-up of achalasia patients treated with botulinum toxin. Dig Liver Dis 34:105–110, 2002