Perinatal and Infant Health Outcomes among Neonates Born to
Aboriginal Parents in Taiwan
YU-HSUN CHANG1, PAU-CHUNG CHEN2, CHIA-JUNG HSIEH2, SUH-FANG JENG3, HUA-FANG LIAO3,
YI-NING SU4, SHIO-JEAN LIN5, HUNG-CHIEH CHOU6, YI-PING LIN2, WU-SHIUN HSIEH6
Background: Poor health outcomes among neonates born to aborigines has been reported in many countries. This study was aimed to examine the nationwide characteristics of live births, adverse birth outcomes, and age-specific mortality among neonates born to non-aboriginal and aboriginal parents in Taiwan.
Methods: All neonates born alive during the period of 2000 to 2003 in Taiwan were included. The adverse birth outcomes including low birth weight, preterm, and small-for-gestational-age births, and age-specific mortality were obtained. Logistic regression analysis was used to estimate odds ratios for parental ethnicity in relation to birth outcomes, while Cox’s proportional hazards regression models were used to estimate hazard ratios for parental ethnicity in relation to age-specific infant deaths.
Results: A total of 947,317 live births were included that consisted of 9,381 born to aboriginal mothers, 6,429 born to aboriginal fathers, and 15,354 born to aboriginal parents. There was a gradual increase in the risk of having a baby with low birth weight, preterm, or small for gestational age born to the four parental aboriginal ethnicity groups: non-aboriginal parents, aboriginal mother only, aboriginal father only, and aboriginal parents. Similar trends were also found for early neonatal, neonatal, and infant mortalities after stratification of residential areas. The neonates born to both aboriginal parents with residence in rural or mountain areas were at highest risk of adverse birth outcomes and age-specific mortality.
Conclusions: Our results demonstrated that aboriginality and residential area are important risk factors for adverse perinatal and infant outcomes. (Acta Paediatr Tw 2007; 48:135-40)
Key words: perinatal outcome, infant outcome, aborigines
INTRODUCTION
Poor perinatal and infant outcomes among aborigines have been reported in many countries.1-6 Aboriginality
used to be considered as a risk factor, but this concept has been challenged. Previous studies reported that aboriginality per se may lose its association with adverse outcomes after adjusting the confounding factors.7,8 Their
Department of Pediatrics, Buddhist Tzu Chi General Hospital1, Hualien; Institute of Occupational Medicine and Industrial
Hygiene, National Taiwan University College of Public Health2, Taipei; School and Graduate Institute of Physical Therapy,
National Taiwan University College of Medicine3, Taipei; Graduate Institute of Clinical Medicine, National Taiwan
University College of Medicine, and Department of Medical Genetics, National Taiwan University Hospital4, Taipei;
Department of Pediatrics, National Cheng-Kung University Hospital, National Cheng-Kung University College of Medicine5,
Tainan; Department of Pediatrics, National Taiwan University Hospital and National Taiwan University College of Medicine6, Taipei, Taiwan.
Received: November 17, 2006. Revised: April 11, 2007. Accepted: June 5, 2007.
Address reprint requests to: Dr. Wu-Shiun HSIEH, Department of Pediatrics, National Taiwan University Hospital and National Taiwan University College of Medicine, No.7, Chung-Shan South Road, Taipei 100, Taiwan.
T E L : 886-2-2312-3456 ext. 5067 FAX : 886-2-2393-4749
results may be questionable due to relative smaller sample size and inappropriate patient selection based on a single hospital study. In addition to aboriginality, other factors including poorer socioeconomic status and malnutrition, and health-damaging behaviors such as smoking and alcohol drinking, may also contribute to the adverse outcomes.7-11
to have lower life expectancy, higher infant mortality, and higher morbidity rates associated with many health problems.12,13 However, after the implementation of the
National Health Insurance (NHI) in Taiwan since 1995, the people in Taiwan including the aborigines have received medical care conveniently and universally.14, 15 NHI provides pregnant women with regular prenatal
and intrapartum care services. In addition, it also provides follow-up neonatal care service and the nationwide vaccination programs for pediatric population.14-16
Improvement of the medical care in aboriginal areas has been considered to be one of NHI’s best achievements. Despite the utilization of the services by aboriginal pregnant women having increased, utilization of the neonatal care service may have regional difference, especially in the rural or mountain areas.14-16 Lower NHI
coverage rate and difficulties in access to medical resources due to traveling time and traveling distance are problems in aboriginal health care.17
This study was aimed to illustrate the characteristics of live births, adverse birth outcomes, and age-specific mortality among neonates born to non-aborigines and aboriginal parents in Taiwan. We also analyzed the impact of residency on perinatal and infant health outcome in aborigines based on a nationwide database.
MATERIALS AND METHODS Data sources
We used the birth certificate registration data with the information of birth outcomes and potential risk factors from the Ministry of Interior in Taiwan. The Children Welfare Act18 mandates birth registration by an obstetrician
or midwife within 10 days for live births for which work has been implemented since October of 1994. The certificate form contains child and parental information. The former include parental indigenes, national identification number, date of birth, education, marital status, and residence. The latter include neonatal identification number, date of birth, birth weight, gestational age, parity, singleton or multiple births, delivery institute, and the information on obstetrician or midwife.
Death certificate registration data is maintained by the Department of Health in Taiwan. The deathcertificate information has been computerized since 1971 in Taiwan consists of national identification number, dates of birth and death, education, residency, and cause of death. The causeof death is systematically coded according to the ninthrevision of the International Classification of Diseases (ICD-9).
Study population
There were a total of 1,017,257 live births registered between 2000 and 2003 in Taiwan. After excluding births to parents with missing ethnicity data (20,633, 2.0%) and those with missing data in covariates (49, 307, 4.8%), a total of 947,317 live births were included for analysis. Then, each neonatal identification number was linked to the death certificate registration data. This study was approved by the National Taiwan University College of Public Health Ethics Review Board, Taipei, Taiwan.
Definitions of birth outcomes and infant deaths
Low birth weight refers to babies with birth weight below 2,500 g and preterm as babies born before 37 completed weeks (259 days) of gestation, as measured from the first day of the last menstrual period. Small for gestational age is defined as birth weight falling below the 10th percentile of the appropriate gestation age-specific birth weight distribution in Taiwan.19 Neonatal deaths
refer to deaths that occurred during the first 28 days of life. They are subdivided into early neonatal deaths, occurring during the first seven days of life, and late neonatal deaths, occurring from the seventh through the 28th day of life. Postneonatal deaths refer to deaths after the 28 completed days through the first year of life, while infant deaths refer to deaths during the first year of life.20
Statistical analyses
Logistic regression models were used to estimate crude and adjusted odds ratios (ORs) and their 95% confidence intervals (CIs) of adverse birth outcomes according to parental indigenes (plain or mountain indigenes and others), while Cox’s proportional hazards regression models were used to estimate crude and adjusted hazard ratios (HRs) and their 95% CIs for age-specific mortalities. Several risk factors of adverse birth outcomes and infant mortalities, which potentially modify or confound the relationship between parental ethnicity and adverse birth outcomes and infant moralities, were examined and controlled. Marital status (married and unmarried), maternal age (<20, 20-24, 25-29, 30-34, and 35 y), paternal age (<25, 25-29, 30-34, 35-39, and 40 y), parental education ( 6, 7-9, 10-12, and 13 y), residential area (urban, suburban, rural, and mountain), parity (primipara and multipara), infant sex (male and female), and plurality (singleton, twin and triplet) were taken into account in the models for low birth weight and preterm births and age-specific infant mortalities. However, infant sex was not entered into the models for small for gestational age births. All statistical analyses were performed using SAS software 8.0.
RESULTS
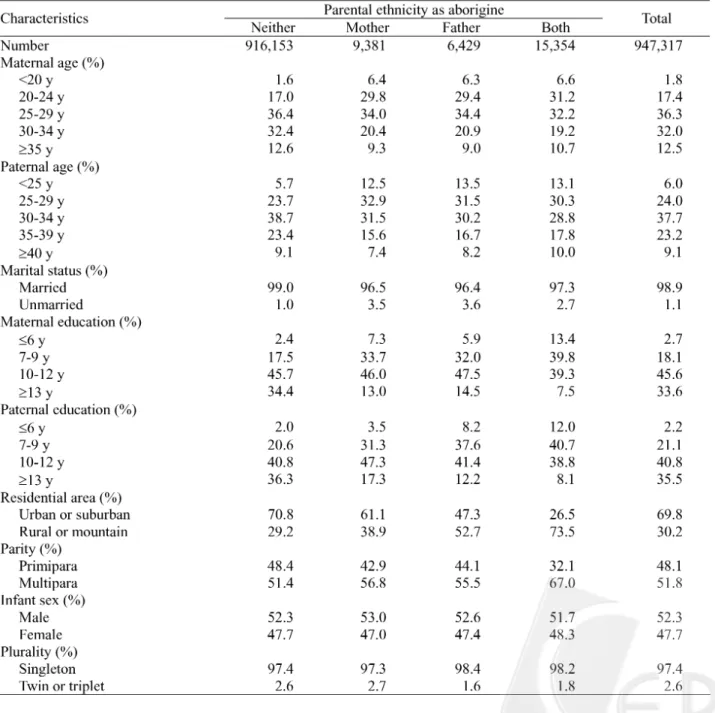
Table 1 shows characteristics of live births according to parental aboriginal ethnicity: neither (n = 916,153), mother only (n = 9,381), father only (n = 6,429), and both (n = 15,354). Comparing to non-aboriginal parents, aboriginal parents were younger, of lower educational levels, and more multiparous. A higher proportion of them gave births in unmarried status and resided in rural or mountain areas. There were fewer twin and triplet babies born to paternal aborigines and aboriginal parents
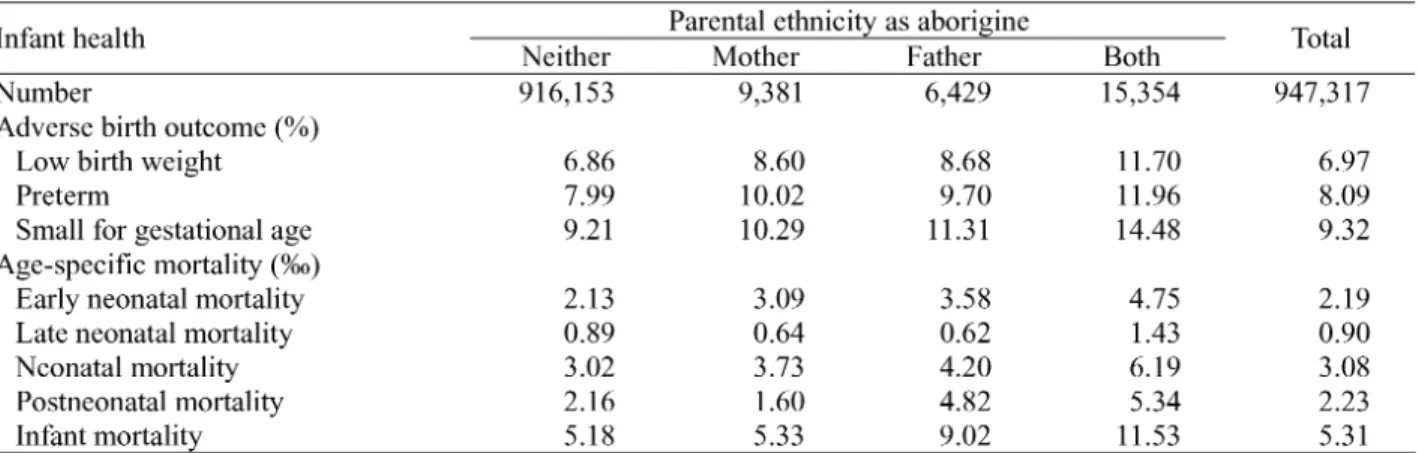
than to non-aboriginal parents and maternal aborigines. Table 2 shows adverse birth outcomes and age-specific infant mortalities of live births according to their parental aboriginal ethnicity. There was a gradual increase in low birth weight and small-for-gestational-age babies born to the four parental aboriginal ethnicity groups: non-aboriginal parents, aboriginal mother only, aboriginal father only and aboriginal parents, while aboriginal parents were more likely to have preterm babies than non-aboriginal parents. Similar trends were found for age-specific infant mortalities, with the exception
of late neonatal and postneonatal mortalities. Table 3 shows adjusted odds ratios for adverse birth outcomes and age-specific infant mortalities of live births according to their parental aboriginal ethnicity. There was a gradual increase in the risk of having a baby with low birth weight, preterm, or small for gestational age born to the four parental aboriginal ethnicity groups: non-aboriginal parents, aboriginal mother only, aboriginal father only, and aboriginal parents. Similar trends were noted for early neonatal, neonatal, and infant mortalities, and the results remained the same even after stratification of residential areas (Table 4).
DISCUSSION
Health care among aboriginal pregnant women and their newborn infants are important public health issues around the world. The current study explored the perinatal characters among Taiwanese aboriginal parents to identify
the contributing factors to perinatal outcomes. Like other aborigines around the world, the aboriginal women in Taiwan suffer from similar problems, i.e., more teenage pregnancy, less education, and more unmarried status.
3,4,7,21 The teenager pregnancy ratio of Taiwanese
aborigines was similar to those of American Indians and Alaska natives, and yet was lower than those of Canadian Inuits and Indians, and of Australian aborigines.
3,4,7 The ratio of school attainment more than thirteen
years in aboriginal mothers was highest in the US, but it was lower in Taiwan and in Canada.3,4 The ratio of
single aboriginal mothers was lowest in Taiwan. The relative disparities between aboriginal and non-aboriginal women changed little over recent decades in Western countries, although the absolute rate differences diminished substantially.3,4,7,8 Compared to
other North American women, aboriginal women experience poorer birth outcomes, such as higher rates of stillbirth, prematurity and low-birth-weight infants.
aboriginal women are thought to be partly attributed to their disadvantaged socioeconomic status. The high prevalence of smoking, poor nutrition, a previous premature infant and bacterial vaginosis in midgestation in these mothers may also contribute the adverse perinatal outcomes.7 In addition, there were much higher risks
of infant death resulting from sudden infant death and infections among both Inuit and Indian infants.3,7 We
found that neonates born to aboriginal parents in Taiwan had higher prevalence rates of preterm, low birth weight, and small-for-gestational-age births. Except for late neonatal mortality rate, these infants had unfavorable neonatal and infant outcomes, too. After adjusting for the confounding factors such as parental ages, education, marital status, parity, infant sex, and plurality, the neonates born to aboriginal parents suffered from the highest risk of adverse birth outcomes and age-specific mortality (Table 3). The causes of death in early neonatal, neonatal and infant mortality were similar among four different groups in our study. Perinatal events such as low birth weight and immaturity-related neonatal death and congenital anomaly mainly contributed to increased early neonatal mortalities; accident and injury events are important causes of postneonatal mortality (data not shown). Both maternal and perinatal factors may together contribute to the adverse perinatal and infant outcomes in our study. These results suggest an urgent need to improve access to and quality of obstetric and perinatal care among aborigines. The adverse health outcomes
among the neonates born to aboriginal fatrher may attribute to poorer socioeconomic status. Further improvement in socioeconomic conditions among aborigines is also mandated in Taiwan.
Residential factor may play an important role in the prevalence of perinatal and infant outcomes. Baldwin et al. found that receipt of an inadequate pattern of prenatal care was significantly higher for rural than for urban mothers of American Indians and Alaska Native infants.4 Rates of inadequate prenatal care in both groups
were over twice than that for Whites. The post neonatal death rates among American Indians and Alaska Native infants were also more than twice that of Whites. They suggested that this situation may be due to the interference with women’s receipt of prenatal care by some barriers such as greater distances from health services, and limited transportation systems in rural areas. Similarly, the neonates born to parents residing in rural or mountain areas suffered from higher risks of adverse birth outcomes and age-specific mortality than those of parents residing in urban or suburban areas, in our study. In addition, the neonates born to aboriginal parents residing in rural or mountain areas were associated with the highest risk of adverse birth outcomes and age-specific mortality. Nevertheless, the neonates born to maternal aborigines only showed similar outcome in late neonatal and postneonatal mortalities compared to the infants born to non-aboriginal parents. Furthermore, the risks for adverse birth outcomes such as small for gestational age
and infant mortality were also comparable between groups. Except for the similar ratio of residency in urban and suburban areas, factors that may contribute to these favorable birth outcomes require more investigation. Several limitations in our study design merit consideration. First, we used the nationwide database that included incomplete socioeconomic information. This may affect the adverse birth and neonatal outcomes. Second, some aboriginal cultures and practices such as smoking, alcohol drinking, and betel nut chewing that may affect these outcomes were not analyzed in this study. Third, the causes of deaths could not be specified due to coding limitation. Finally, we tested several outcomes or mortalities and, then, may inflate type I errors. This would not have a significant impact on our findings about the biologically related outcomes and their consequent mortalities. However, this study was the first to analyze the nationwide database on birth outcomes and age-specific infant mortalities among the aborigines and the non-aborigines in Taiwan.
In conclusion, this study has provided important information on the perinatal and infant health outcomes among neonates born to aboriginal parents in Taiwan. Improvement of obstetric care and a reduction in preterm births is necessary to enhance perinatal and infant health outcomes among the aborigines. The government should also provide more evenly distributed medical and educational resources, and convenient transport systems, especially in the rural and mountain areas. Furthermore, public health policies for improvement in healthier lifestyle such as decreasing smoking habit, alcohol consumption, substance abuse, and prevention of accident events, sudden infant death and infection-related deaths are also important to improve health outcomes for the aborigines. ACKNOWLEDEGMENTS: This study was supported by the grants (BHP-PHRC-92-4 and DOH93-HP-1702) awarded by the Bureau of Health Promotion, Department of Health, Taiwan, and by a grant awarded by the Preterm Baby Foundation, R.O.C., and by the grant TCRD 96-35 awarded by the Buddhist Tzu Chi General Hospital.
REFERENCES
1. Matthias GS, Morgan G. Aboriginal and non-aboriginal perinatal deaths in Darwin: a comparative view. Med J Aust 1992; 156:533-7.
2. Mohsin M, Bauman AE, Jalaludin B. The influence of an-tenatal and maternal factors on stillbirths and neonatal deaths in New South Wales, Australia. J Biosoc Sci 2006;
38:643-57.
3. Luo ZC, Wilkins R, Platt RW, Kramer MS. For the Fetal and Infant Health Study Group of the Canadian Perinatal Sur-veillance System. Risks of adverse pregnancy outcomes among Inuit and North American Indian women in Quebec, 1985-97. Paediatr Perinat Epidemiol 2004; 18:40-50. 4. Baldwin LM, Grossman DC, Casey S, et al. Perinatal and
infant health among rural and urban American Indians/Alaska Natives. Am J Public Health 2002; 92:1491-7.
5. Corry M. Is birthweight an appropriate health-outcome mea-sure for Torres Strait Islander babies? Aust N Z J Public Health 2000; 24:60-3.
6. Smith RM, Smith PA, McKinnon M, Gracey M. Birthweights and growth of infants in five Aboriginal communities. Aust N Z J Public Health 2000; 24:124-35.
7. Wenman WM, Joffres MR, Tataryn IV, Edmonton Perin-atal Infections Group. A prospective cohort study of pregnan-cy risk factors and birth outcomes in Aboriginal women. CMAJ 2004; 171:585-9.
8. Panaretto KS, Muller R, Patole S, Watson D, Whitehall JS. Is being Aboriginal or Torres Strait Islander a risk factor for poor neonatal outcome in a tertiary referral unit in North Queensland? J Paediatr Child Health 2002; 38:16-22. 9. Yang MS, Ko YC, Wen JK. Prevalences and related
fac-tors of substances use in female aborigines in southern Taiwan. Kaohsiung J Med Sci 1996; 12:634-40.
10. Yang MS, Chang FT, Chen SS, Lee CH, Ko YC. Betel quid chewing and risk of adverse pregnancy outcomes among aborigines in southern Taiwan. Public Health 1999; 113:189-92.
11. Colditz PB, Shannon C. Indigenous neonatal outcomes: What do we expect? J Paediatr Child Health 2002; 38:4-5. 12. Wen CP, Tsai SP, Shih YT, Chung WSI. Bridging the gap in life expectancy of the Aborigines in Taiwan. Int J Epide-miol 2004; 33:320-7.
13. Knobel HH, Yang WS, Ho MS. Urban-rural and regional differences in infant mortality in Taiwan. Soc Sci Med 1994;
39:815-22.
14. Chen LM, Wen SW, Li CY. The impact of national health insurance on the utilization of health care services by preg-nant women: the case in Taiwan. Matern Child Health J 2001; 5:35-42.
15. Chen CS, Liu TC, Chen LM. National Health Insurance and the antenatal care use: a case in Taiwan. Health Policy 2003;
64:99-112.
16. Liu TC, Chen CS, Chen LM. The impact of National Health Insurance on neonatal care use and childhood vaccination in Taiwan. Health Policy Plan 2002; 17:384-92.
17. Ho PS, Wang TN, Hsieh TK, Ko YC. Differences in phy-sician utilization between Aboriginal and non-Aboriginal children. Fam Pract 2000; 17:414-21.
18. Ministry of the Interior, Taiwan. The Children Welfare Act. Taipei, Taiwan. Ministry of the Interior, 1993.
19. Hsieh WS, Wu HC, Jeng SF, et al. Nationwide singleton birth weight percentiles by gestational age in Taiwan, 1998-2002. Acta Paediatr Taiwan 2006; 47:25-33.
20. Nguyen RHN, Wilcox AJ. Terms in reproductive and peri-natal epidemiology: 2. Periperi-natal terms. J Epidemiol Com-munity Health 2005; 59:1019-21.
21. Li YT, Yin CS, Chan CC. Psychosocial risk factors of teen-age pregnancy in eastern Taiwan. Zhonghua Yi Xue Za Zhi (Taipei) 1999; 62:425-30.