RESEARCH
Development of an ultra-high sensitive
immunoassay with plasma biomarker
for differentiating Parkinson disease dementia
from Parkinson disease using antibody
functionalized magnetic nanoparticles
Shieh‑Yueh Yang
1,2*, Ming‑Jang Chiu
3,4,5,6, Chin‑Hsien Lin
3, Herng‑Er Horng
2, Che‑Chuan Yang
1, Jen‑Jie Chieh
2,
Hsin‑Hsien Chen
1and Bing‑Hsien Liu
1Abstract
Background: It is difficult to discriminate healthy subjects and patients with Parkinson disease (PD) or Parkinson disease dementia (PDD) by assaying plasma α‑synuclein because the concentrations of circulating α‑synuclein in the blood are almost the same as the low‑detection limit using current immunoassays, such as enzyme‑linked immuno‑ sorbent assay. In this work, an ultra‑sensitive immunoassay utilizing immunomagnetic reduction (IMR) is developed. The reagent for IMR consists of magnetic nanoparticles functionalized with antibodies against α‑synuclein and dispersed in pH‑7.2 phosphate‑buffered saline. A high‑Tc superconducting‑quantum‑interference‑device (SQUID) alternative‑current magnetosusceptometer is used to measure the IMR signal of the reagent due to the association between magnetic nanoparticles and α‑synuclein molecules.
Results: According to the experimental α‑synuclein concentration dependent IMR signal, the low‑detection limit is 0.3 fg/ml and the dynamic range is 310 pg/ml. The preliminary results show the plasma α‑synuclein for PD patients distributes from 6 to 30 fg/ml. For PDD patients, the concentration of plasma α‑synuclein varies from 0.1 to 100 pg/ml. Whereas the concentration of plasma α‑synuclein for healthy subjects is significantly lower than that of PD patients.
Conclusions: The ultra‑sensitive IMR by utilizing antibody‑functionalized magnetic nanoparticles and high‑Tc SQUID magnetometer is promising as a method to assay plasma α‑synuclein, which is a potential biomarker for discriminat‑ ing patients with PD or PDD.
Keywords: α‑synuclein, Parkinson disease, Immunomagnetic reduction
© 2016 The Author(s). This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/ publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
Background
Parkinson disease (PD) is the second most common neu-rodegenerative disease after Alzheimer’s disease. More than 1 % of people older than 65 years old are suffering from PD [1]. About 10 million people worldwide are liv-ing with PD. The direct and indirect healthcare cost for
one PD patient is estimated to be US 100,000 per year [2]. Many countries, especially the US, Canada, Europe and Australia, are worrying about unsustainable increases in the costs of healthcare. Lots of resources and effort have been put into developing the diagnosis, treatments and vaccine for PD.
The clinical criteria for diagnosing PD are the observa-tions of movement disorders such as bradykinesia, cogwheel rigidity, resting tremor and postural instability. Although these clinical features are popularly used, there are several
Open Access
*Correspondence: syyang@magqu.com
1 MagQu Co., Ltd., Xindian District, New Taipei City 231, Taiwan
fatal issues for diagnosing PD. For example, other movement disorders (e.g. multiple system atrophy, corticobasal degen-eration, or progressive supranuclear palsy) might overlap with the clinical symptoms of PD and decrease the accuracy of diagnosing PD [3]. In addition, it has been reported the clinical symptoms are present after degeneration of over 50 % of dopaminergic neurons in the basal ganglia, particu-larly in the substantia nigra [4]. The early-stage diagnosis of PD is very difficult, using observations of clinical movement disorders. Analysis of the genetic sequence seems a better method for early-stage diagnosis of PD [5–7]. Nevertheless, only 10 % of PD patients are hereditary. Ninety percent of PD patients are sporadic.
Development of cognitive impairment and demen-tia, referred as Parkinson disease dementia (PDD), is common in PD [8]. The prediction of development of dementia in PD is challenging and of significant impact in the field. Researchers are now trying to achieve bio-molecular diagnosis for differentiating PD from PDD. α-synuclein is the most recognized biomarker for PD or PDD [9, 10]. As α-synuclein molecules are phosphoryl-ated, phosphor-α-synuclein molecules easily aggregate with one another to form Lewy body in the dopaminergic neurons [11, 12]. Dopaminergic neurons with Lewy bod-ies become degenerative and lose the ability to express dopamine. Neural cells in the motor cortex of the brain are damaged due to the lack of dopamine and movement disorders are stimulated.
Numerous discoveries show the concentration of α-synuclein in the cerebrospinal fluid (CSF) is reduced because of the formation of Lewy bodies for PD or PDD patients as compared to healthy subjects [13–16]. However, the reported results for the variations in the concentration of α-synuclein in blood are not consist-ent [17–20]. The main reason for the inconsistent assay results for plasma α-synuclein is the poor low-detection limit of assays. According to these reports [13–20], the enzyme-linked immunosorbent assay (ELISA) is cur-rently used for assaying α-synuclein in either CSF or plasma. α-synuclein is expressed and is abundant in the brain and spinal cord, but occurs in very low amounts in the peripheral blood system. ELISA is not able to pre-cisely detect the proteins at ultra-low concentrations, such as α-synuclein in plasma. Thus, CSF instead of plasma is better for the assay of α-synuclein in the bio-molecular diagnosis of PD or PDD using ELISA.
CSF is usually collected via lumbar puncher, which is high-risk and uncomfortable. The early-stage diagnosis by assaying α-synuclein in CSF is not widely accepted by the general population. Alternatively, blood is much easier to obtain in clinics. To do this, a high-sensitivity detection technology is required to achieve the assay of ultra-low α-synuclein in plasma.
Authors have developed an immunoassay technology, so-called immunomagnetic reduction (IMR), for quanti-tatively detecting bio-molecules at ultra-low concentra-tions, e.g. 1–10 pg/ml or lower [21, 22]. The main reason contributed to the ultra-high sensitivity of IMR is the uti-lization of antibody-functionalized magnetic nanoparti-cles. These magnetic nanoparticles are well dispersed in reagent and can catch target bio-molecules everywhere in a tested sample. Besides, due to the nano-scaled sizes of particles, the total binding area is extremely large. Hence, antibodies immobilized on the surfaces of mag-netic nanoparticles are highly efficiently able to associ-ate with target bio-molecules and result in an ultra-high sensitive immunoassay using IMR. It has been demon-strated IMR can be applied to assay ultra-low concen-tration β-amyloids and tau protein in human plasma [23–25]. A clear discrimination between healthy sub-jects and patients with mild cognition impairment due to Alzheimer’s disease was evidenced by assaying plasma β-amyloids and tau protein [26]. These results motivated us to investigate the feasibility of assaying ultra-low con-centration α-synuclein in human plasma to achieve a bio-molecular diagnosis of PD or PDD, or to differentiate PD from PDD according to the plasma α-synuclein concen-tration. In this work, the reagent for assaying α-synuclein by utilizing IMR is prepared. The characterizations of the reagent and assaying α-synuclein are explored. For com-parison, the assay characteristics for α-synuclein using ELISA are examined. Finally, the preliminary results for discriminating PD patients, PDD patients and healthy subjects by assaying plasma α-synuclein are reported. Although the cross sectional study done in this work can-not address the prediction of the development of PDD in PD, the results might point to the potential use of this method of measuring plasma α-synuclein in differentiat-ing PD from PDD.
Results and discussion
The mean value of the hydrodynamic diameters for the antibody-functionalized magnetic Fe3O4 nanoparticles was found to be 55.5 nm and the standard deviation of particle hydrodynamic diameters was 12.7 nm. By using scanning electronic microscope, the mean value of the diameters for the antibody-functionalized magnetic Fe3O4 nanoparticles was obtained as ~40 nm. The reagent is superparamagnetic with the saturated magnetization of 0.3 emu/g. According to a previously published paper [27], the numbers of antibody-functionalized nanopar-ticles in 1-ml reagent with 0.3 emu/g are around 1013. The total surface area of antibody-functionalized mag-netic nanoparticles in 1-ml reagent is around 1000 cm2. In experiment, 80-μl reagent is used. The total surface area of antibody-functionalized magnetic nanoparticles
in 80-μl reagent for each assay is around 80 cm2. As compared with a 96-well ELISA plate, the binding area between antibody and target bio-molecules for each well is 0.45 cm2. Thus, the binding area with IMR is almost 180 times larger than that of ELISA.
The bio-activity of the immobilized antibodies on mag-netic nanoparticles is investigated by measuring the IMR signals due to the association between α-synuclein and antibodies on magnetic nanoparticles. The time depend-ent ac magnetic susceptibility χac of reagent after mixing the reagent and the tested solution is recorded, as shown in Fig. 1 Two tested samples are prepared: one is pure PBS solution, the other is 3.1-fg/ml α-synuclein solution. The dashed line in Fig. 1 denotes the time dependent ac magnetic susceptibility χac of the mixture of reagent and PBS solution. Clearly, temporal χac with the dashed line almost remains unchanged. However, as to the solid line corresponding to the mixture of reagent and 3.1-fg/ml α-synuclein solution, the temporal χac descends in 45 min and then reaches a lower level. A significant reduction in the ac magnetic susceptibility χac of the reagent due to the association between α-synuclein and the antibodies on the magnetic nanoparticles is observed.
To quantify the reduction in the ac magnetic suscepti-bility χac of the reagent, the initial/final χac before/after the association between α-synuclein and antibodies on mag-netic nanoparticles is calculated according to the temporal χac shown in Fig. 1. As addressed in previously published papers [22, 28], the confidence intervals for the determi-nation of reduction in ac magnetic susceptibility χac of the reagent are that within the first and the last 40–50 min of the time dependent ac magnetic susceptibility χac shown in Fig. 1. In this study, the data of ac magnetic susceptibil-ity χac of the reagent within the first and the last 45 min are used for determining the reduction in χac.
In Fig. 1, the p value for the ac magnetic susceptibility χac between the intervals of the first and the last 45 min is found to be 0.046 for PBS solution. A slight reduction in the ac magnetic susceptibility χac of reagent mixed with PBS is observed. As to 3.1-fg/ml α-synuclein solution, the p-value for the ac magnetic susceptibility χac between the intervals of the first and the last 45 min is found to be 0.007. A clear reduction in the time dependent ac mag-netic susceptibility χac of reagent after being mixed with α-synuclein solution is evidenced.
The initial χac is referred to as χac,o, which is the aver-age value of χac’s within the first 45 min. The final χac is referred to as χac,φ, which is the average value of χac’s within the last 45 min. The reduction in the ac mag-netic susceptibility χac of the reagent, e.g. IMR signal, is obtained via
(1) IMR (%) =
χac,o− χac,ϕ /χac,o×100 %
Via Eq. (1), the IMR signals for the dashed line and the solid line in Fig. 1 are calculated to be 1.56 and 2.13 %, respectively. The results shown in Fig. 1 reveal a back-ground level for the IMR assay. Such a backback-ground level is mainly attributed to the electronic noises of the assay system. According to the duplicate measurements, the IMR signals for the PBS solution are 1.56 and 1.65 %. Thus, the background level of the IMR signal is 1.61 % with a standard deviation of 0.06 %.
The IMR signal as a function of the concentration of α-synuclein, i.e. IMR (%) − φα-syn curve, is plot-ted in Fig. 2. As the concentration of α-synuclein φα-syn increases from 3 × 10−4 pg/ml (=0.3 fg/ml), the IMR sig-nal increases. The φα-syn dependent IMR (%) was found to follow the logistic function expressed as
where A, B, φo and γ are fitting parameters. By fitting the data point in Fig. 2 to Eq. (2), the fitting parameters are obtained as A = 1.94, B = 3.95, φo = 49.7 and γ = 0.26. The fitting curve is plotted with the solid line in Fig. 2. The corresponding coefficient of determination R2 is 0.998. The fact R2 is very close to 1 implies φ
α-syn depend-ent IMR (%) is truly governed by the logistic function.
The parameter A in Eq. (2) is the value of IMR (%) as φ α-syn extrapolates to zero. Usually, value A is a little higher than the background level. For example, A is 1.94 % and the background level here is 1.61 %. The difference (2) IMR(%) = A − B 1+ ϕα−syn ϕo γ + B 0.0 1.0 2.0 3.0 4.0 5.0
Time (hr.)
720.0 760.0 800.0 840.0 880.0 χac(a.u.)
χac,o χac,φPBS
φα-syn= 3.1 fg/ml
p = 0.007 p = 0.046Fig. 1 Bio‑activity test for the antibody immobilized on magnetic
between A and the background level is predominantly due to the noises caused by the dynamic equilibrium in the association between the protein molecules and the antibody-functional magnetic nanoparticles. However, A is not used as the low-detection limit. Convention-ally, the low-detection limit is defined as the concentra-tion showing an IMR signal higher than A by three times as the standard deviation of IMR signals for a low-con-centration test, i.e. 3-σ criterion. In this experiment, the standard deviation of low-concentration tests is 0.028 %. Thus, the low-detection limit is the concentration having an IMR signal of 2.02 %. Via Eq. (2), the low-detection limit for assaying α-synuclein is found to be 0.3 fg/ml.
The α-synuclein concentration dependent optical absorbance density at 450 nm, O.D. 450 nm, using ELISA is plotted by cross symbols in Fig. 2. The experimental data are fitted to the logistic function
The fitting parameters are found to be 0.189, 5.070, 13566.08 and 1.44 for A′, B′, φ
o
′ and γ′ in Eq. (3). The logistic function of Eq. (3) is plotted by the dashed line in Fig. 2. The coefficient of determination R2 between the cross symbols and the dashed line is 0.999. By utiliz-ing the 3-σ criterion, the low-detection limit of assayutiliz-ing α-synuclein using ELISA is 79.04 pg/ml. It is obvious IMR is more sensitive than ELISA by a factor of 250,000 for assaying α-synuclein. As mentioned, the detecting sensi-tivity of IMR is higher than ELISA by a factor of 200 by taking the reacting surface into account. Additional fac-tor of 1250 might be due to the ultra-low-noise magnetic
(3) O.D. 450 nm = A ′ + B′ 1+ ϕ α−syn ϕ′o γ′ +B′
sensor, i.e. high-Tc superconducting quantum interfer-ence device (SQUID) magnetometer. High-Tc SQUID magnetometer shows a noise level of 50 fT/Hz1/2, which is lower than the magnetic signal generated by a single magnetic nanoparticle by three orders of magnitude. This implies that the reduction in ac magnetic signal resulted from a single magnetic nanoparticle due to the associat-ing with target bio-molecule can be sensed by high-Tc SQUID magnetometer. Hence, the ultra-low-noise high-Tc SQUID magnetometer is extremely sensitive to the reduction in ac magnetic signal of reagent and shows ultra-high sensitivity in assaying bio-molecules.
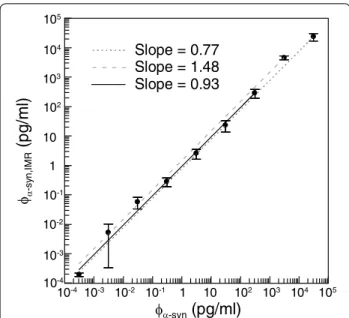
In addition to the low-detection limit, the dynamic range of assaying α-synuclein using IMR is an impor-tant characteristics. To examine the dynamic range, the experimental IMR signals in Fig. 2 are converted to con-centrations of α-synuclein via Eq. (2). The converted con-centrations of α-synuclein are denoted by φα-syn,IMR. The correlation between φα-syn,IMR and φα-syn is examined, as shown in Fig. 3. In Fig. 3, the linearity between φα-syn,IMR and φα-syn can be obtained. According to the regulation issued by US Food and Drug Administration (FDA), the slope of the linearity in Fig. 3 must be between 0.90 and 1.10. In Fig. 3, if the φα-syn,IMR’s for the α-synuclein concentration φα-syn’s from 0.31 fg/ml to 31 ng/ml are used, the slope of the φα-syn,IMR-φα-syn curve is 0.77 and the coefficient of determination R2 is 0.991, as plotted by the dotted line in Fig. 3. The slope of the dotted line in Fig. 3 does not meet the requirement of the US FDA. The concentration range of α-synuclein for investigating the assay dynamic range should be narrowed. Hence, the highest φα-syn,IMR in Fig. 3, i.e. with φα-syn being 31 ng/ml, is ignored. The linear curve between φα-syn,IMR and φα-syn within the range from 0.31 to 3.1 ng/ml is plotted by the dashed line in Fig. 3. The slope of the dashed line is 1.48 and the coefficient of determination R2 is 0.999. The slope of the dashed line is much higher than the requirement of the US FDA. It seems the second highest φα-syn,IMR in Fig. 3 should also be ignored. The linear curve between φα-syn,IMR and φα-syn within the range from 0.31 fg/ml to 310 pg/ml is plotted by the solid line in Fig. 3. The slope of the solid line is 0.93 and the coefficient of determina-tion R2 is 0.999. Notably, the slope of the solid line meets the requirement of the US FDA. Thus, the dynamic range of α-synuclein concentration for IMR assay is from 0.3 fg/ ml to 310 pg/ml.
The data shown in Fig. 2 prove the IMR assay is extremely sensitive and might possibly detect α-synuclein in human plasma. Plasma samples contributed by nine healthy persons, nine PD patients and fourteen PDD patients were collected for prior study on the discrimi-nation between healthy subjects, PD patients and PDD patients by using IMR. The demographic information of 2.00 2.50 3.00 3.50 4.00 IM R (%) 0.10 1.00 10.00 O. D. 450 nm 10-4 10-3 10-2 10-1 1 10 102 103 104 105 φα-syn (pg/ml) IMR ELISA
Fig. 2 α‑synuclein concentration dependent IMR signal (solid line)
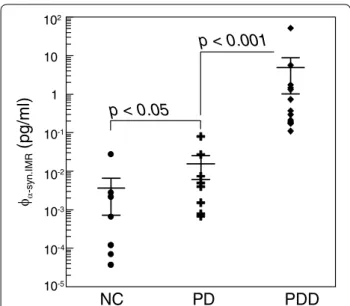
the collected 33 subjects is listed in Table 1. The detected concentrations φα-syn,IMR of α-synuclein in human plasma are shown in Fig. 4. The plasma φα-syn,IMR’s for PDD patients range from 0.1 to 100 pg/ml, while the plasma φα-syn,IMR’s for healthy subjects are much lower than 0.1 pg/ml. The plasma φα-syn,IMR’s for PD patients distrib-ute between those of healthy subjects and PDD patients. The p value in terms of plasma φα-syn,IMR between healthy subjects and PD patients was found to be 0.005, which reveals the fact that PD patients show higher concentra-tions for plasma α-synuclein as compared to healthy sub-jects. In Fig. 4, a clear discrimination in plasma φα-syn,IMR between PD patients and PDD patients was observed (p < 0.001). According to the results in Fig. 4, the con-centration plasma α-synuclein keeps raising as a healthy subject suffering from PD and progressing to PDD. It is worthy noting that the age is matched between healthy subjects and PD patients (p > 0.05), as well as between PD patients and PDD patients (p > 0.05).
Previous studies have shown that α-synuclein would be released from neurons by exocytosis into body fluids, including CSF and plasma, which contributes to cell-to-cell transmission of α-synuclein pathology in the brain [29]. Numerous studies have focused on checking lev-els of either total or oligomeric α-synuclein in plasma samples from patients with PD compared with healthy controls but the results are conflicting [30]. Since phos-phorylated and fibrillar α-synuclein are the main patho-logical forms of the protein, one recent study observed that plasma level of phospho-α-synuclein was higher in
early-stage PD samples without dementia than controls [31]. These observations suggest the feasibility and poten-tiality of plasma level of α-synuclein (either total, oligo-meric or phosphorylated form) could partly reflect the α-synuclein pathology in the brains of PD patients. Fur-thermore, cortical Lewy body/neuritic pathology is more extensive in PDD than in PD without dementia, which implies the α-synuclein burden in plasma is more severe in PDD than in PD. Our results supported this hypoth-esis that plasma level of α-synuclein is significantly higher in PDD than in PD with normal cognition, which level is slightly higher than healthy controls. As amyloid β plaques and tau neurofibrillary tangles, the hallmark pathologies of Alzheimer’s dementia, are also observed and correlate with cognitive status in patients with PDD [29], future studies incorporating assessing phospho-α-synuclein, amyloid β protein, total and phospho-tau in plasma levels of PDD are needed to better understanding the pathophysiology of PDD.
In plasma samples, heterophilic antibody is a major confounder and interferes the assaying results by sand-wich ELISA method [32]. Heterophilic antibody (HA) is defined as one of the common interference materials for immunoassay according to the guidance of Clinical and Laboratory Standards Institute (CLSI-EP-A2: Interfer-ence Testing of Clinical Chemistry) [33]. IMR method showed low-interference and high-specificity effects in comparison with ELISA through previous researches [34–36]. The selection mechanism is based on centrifu-gation force contributed from oscillating magnetic nan-oparticles in reagent. The details have been discussed in previous research [37]. In fact, not only HA but also naturally existed biomolecules of frequently used drug in plasma are prevented from associating with magnetic nanoparticles via the selection mechanism [36]. This features IMR a high-specificity methodology for clinical analysis of plasma biomarkers of Parkison’s disease.
Clinically, patients first are diagnosed with PD and in later stages of the disease may develop dementia and thus get the diagnosis of PDD; Hence, biomarkers that can predict or diagnose early stages of progression to PDD
φα-s yn ,IMR
(p
g/
ml
)
10-4 10-3 10-2 10-1 1 10 102 103 104 105 φα-syn(pg/ml)
Slope = 0.77 Slope = 1.48 Slope = 0.93 105 104 103 102 10 1 10-1 10-2 10-3 10-4Fig. 3 Converted α‑synuclein concentration φα‑syn,IMR versus spiked α‑synuclein concentration φα‑syn in PBS solution for the analysis of dynamic range for assaying α‑synuclein
Table 1 Demographic characteristics of the subjects
PD Parkinson disease; PDD Parkinson disease dementia; MMSE mini-mental state
examination; SD standard deviation
Group Healthy
subjects PD with normal cognition PDD patients
Numbers 9 9 14
Female/Male 4/5 4/5 7/7
Age (years) 38–73 38–85 60–81
MMSE (mean ± SD) 29.0 ± 1.1 28.7 ± 1.2 18.7 ± 6.3 Disease duration (years) – 9.3 ± 6.7 10.1 ± 5.3
in PD subject would indeed be of clinical significance. According to the results in Fig. 4, the plasma α-synuclein in PDD patients show clearly higher level than that in PD patients (p < 0.001). This implies that plasma α-synuclein is promisingly used as a clinical parameter monitoring the progression to PDD in PD patients.
Conclusions
By immobilizing antibodies against α-synuclein onto magnetic nanoparticles, the reagent for assaying α-synuclein is developed. Through utilizing immu-nomagnetic reduction (IMR) with aid of high-Tc SQUID magnetometer, the dynamic range of assay-ing α-synuclein is from 0.3 fg/ml to 310 pg/ml. The ultra-sensitivity SQUID-based IMR is applied to assay human plasma α-synuclein. The preliminary results show a clear difference in the concentrations of plasma α-synuclein between healthy subjects, PD patients and PDD patients. This method seems promising to apply IMR to diagnosis of PD and PDD by assaying plasma α-synuclein.
Method
The reagent for assaying α-synuclein consists of mag-netic Fe3O4 nanoparticles (MF-DEX-0060, MagQu) functionalized monoclonal antibodies (sc-12767, Santa Crusz Biotech.) against α-synuclein. The detailed pro-cesses for immobilizing antibodies onto magnetic Fe3O4 nanoparticles are discussed in References [38, 39]. The antibody-functionalized magnetic Fe3O4 nanoparti-cles are dispersed in pH-7.2 phosphate-buffered saline (PBS) solution. The distribution of particle diameters is
analyzed by dynamic laser scattering (Nanotrac-150, Microtrac). The magnetic concentration of reagent is measured using a vibrating sample magnetometer (HysterMag, MagQu). The bio-activity of the antibod-ies on the magnetic nanoparticles is examined by an IMR analyzer (XacPro-S, MagQu). The IMR analyzer is an ac magnetosusceptometer equipped with a high-Tc superconducting-quantum-interference-device (SQUID) magnetometer as a magnetic sensor. The details of the ac magnetosusceptometer are described in References [23, 40]. To establish the relationship between the IMR signal and the concentration of α-synuclein, α-synuclein (ab51189, Abcam) spiked in PBS solutions is prepared. For each measurement of the IMR signal, 80-μl reagent is mixed with 40-μl α-synuclein solution, followed by detec-tion of the IMR signal using an IMR analyzer (XacPro-S, MagQu). Duplicate measurements are performed for IMR signals with each concentration of α-synuclein solu-tion. In addition to the measurements of the IMR signals, a commercial ELISA kit (KHB0061, Novex) is applied to find the α-synuclein concentration dependent optical absorbance unit.
Volunteers participating in this study were given a med-ical checklist of major systemic diseases, operations and hospitalizations. Volunteers reporting uncontrolled med-ical conditions including heart failure, recent myocardial infarction (in the past 6 months), malignancy (in the past 2 years), or poorly controlled diabetes (HbA1C > 8.5) were excluded. Volunteers also received physical exami-nations. Eight healthy subjects and six patients with PD were enrolled in this study. The study was approved by the ethics committee and institute review board of the university hospital.
Participants were asked to provide a 10-ml non-fast-ing venous blood sample (K3 EDTA, lavender-top tube). Each sample was assigned a registry number following the sampling sequence; hence, colleagues in the labora-tory were blind to the clinical status and the demographic data of the subjects. The blood samples were centrifuged (2500g for 15 min) within 1 h of collection and the plasma was aliquoted into cryotubes and stored at −80 °C for less than three months until being thawed for measure-ment via IMR. 80-μl of reagent was mixed with 40-μl of plasma for the measurement of α-synuclein concentra-tion via IMR. Duplicate measurements were performed for each plasma sample.
Nine human plasma samples from healthy subjects aged from 38 to 73 years, 9 human plasma samples from PD patients (38–85 years old) and 14 human plasma samples from patients with PDD (60–81 years old) were used for the α-synuclein assay using IMR. PD and PDD patients were identified using clinical symptoms. It is worthy noting that PD patients are cognitively normal.
φα-sy n. IM R
(
pg/m
l)
102 10 1 10-1 10-2 10-3 10-4 10-5NC PD PDD
p < 0.001
p < 0.05
Fig. 4 Detected plasma α‑synuclein concentrations using IMR for
All of the enrolled patients provided informed con-sent before undergoing the procedure and this study was approved by National Taiwan University Hospital Research Ethics Committee.
Authors’ contributions
SY participated the characterization of bio‑magnetic nanoparticles. CC carried out the IMR measurements. HR prepared the bio‑magnetic particles. JJ par‑ ticipated the characterization of bio‑magnetic nanoparticles. HH analyzed the experimental data. MJ and CH carried out the assessment of human plasma. All authors read and approved the final manuscript.
Author details
1 MagQu Co., Ltd., Xindian District, New Taipei City 231, Taiwan. 2 Institute
of Electro‑optical Science and Technology, National Taiwan Normal University, Taipei 116, Taiwan. 3 Department of Neurology, National Taiwan University
Hospital, College of Medicine, National Taiwan University, Taipei 100, Taiwan.
4 Graduate Institute of Brain and Mind Sciences, College of Medicine, National
Taiwan University, Taipei 100, Taiwan. 5 Department of Psychology, National
Taiwan University, Taipei 100, Taiwan. 6 Graduate Institute of Biomedical Engi‑
neering and Bioinformatics, National Taiwan University, Taipei 116, Taiwan. Acknowledgements
This work is supported by Ministry of Economic Affairs of Taiwan under grant numbers 101‑EC‑17‑A‑17‑I1‑0074 and by New Taipei City government under the grant number 103049 (SBIR) and by the Ministry of Science and Technol‑ ogy, Taiwan under grant number 104‑2745‑B‑003 ‑002.
Competing interests
The authors declare no competing financial interest. Received: 22 December 2015 Accepted: 24 May 2016
References
1. Pringsheim T, Jette N, Frolkis A, Steeves TDL. The prevalence of Parkin‑ son’s disease: a systematic review and meta‑analysis. Move Disorders. 2014;29:1583–90.
2. http://www.pdf.org/en/parkinson_statistics.
3. Kim D, Paik JH, Shin DW, Kim HS, Park CS, Kang JH. What is the clinical significance of cerebrospinal fluid biomarkers in Parkinson’s disease? Is the significance diagnostic or prognostic? Exp Neurobiol. 2014;4:352–64. 4. Tolosa E, Wenning G, Poewe W. The diagnosis of Parkinson’s disease.
Lancet Neurol. 2006;5:75–86.
5. Polymeropoulos MH, Lavedan C, Leroy E, Ide SE, Dehejia A, Dutra A, Pike B, Root H, Rubenstein J, Boyer R, Stenroos ES, Chandrasekharappa S, Athanassiadou A, Papapetropoulos T, Johnson WG, Lazzarini AM, Duvoisin RC, Di IG, Golbe LI, Nussbaum RL. Mutation in the alpha‑synuclein gene identified in families with Parkinson’s disease. Science. 1997;276:2045–7. 6. Ahn TB, Kim SY, Kim JY, Park SS, Lee DS, Min HJ, Kim YK, Kim SE, Kim JM,
Kim HJ, Cho J, Jeon BS. Alpha‑synuclein gene duplication is present in sporadic Parkinson disease. Neurology. 2008;70:43–9.
7. Krüger R, Kuhn W, Müller T, Woitalla D, Graeber M, Kösel S, Przuntek H, Epplen JT, Schols L, Riess O. Ala30Pro mutation in the gene encoding alpha‑synuclein in Parkinson’s disease. Nat Genet. 1998;18:106–8. 8. Aarsland D, Andersen K, Larsen JP, Lolk A, Kragh‑Sørensen P. Prevalence
and characteristics of dementia in Parkinson disease: an 8‑year prospec‑ tive study. Arch Neurol. 2003;60:387–92.
9. Dickson DW. Alpha‑synuclein and the Lewy body disorders. Curr Opin Neurol. 2001;14:423–32.
10. El‑Agnaf OMA, Salem SA, Paleologou KE, Cooper LJ, Fullwood NJ, Gibson MJ, Curran MD, Court JA, Mann DMA, Ikeda SI, Cookson MR, Hardy J, All‑ sop D: α‑synuclein implicated in Parkinson’s disease is present in extracel‑ lular biological fluids, including human plasma. FASEB J 2003;13:1945–7. 11. Spillantini MG, Schmidt ML, Lee VM, Trojanowski JQ, Jakes R, Goedert M.
Alpha‑synuclein in Lewy bodies. Nature. 1997;388:839–40.
12. Giasson BI, Uryu K, Trojanowski JQ, Lee VM. Mutant and wild type human α‑synucleins assemble into elongated filaments with distinct morpholo‑ gies in vitro. J Biol Chem. 1999;274:7619–22.
13. Hong Z, Shi M, Chung KA, Quinn JF, Peskind ER, Galasko D, Jankovic J, Zabetian CP, Leverenz JB, Baird G, Montine TJ, Hancock AM, Hwang H, Pan C, Bradner J, Kang UJ, Jensen PH, Zhang J. DJ‑1 and alpha‑synuclein in human cerebrospinal fluid as biomarkers of Parkinson’s disease. Brain. 2010;133:713–26.
14. Mollenhauer B, Locascio JJ, Schulz‑Schaeffer W, Sixel‑Döring F, Trenk‑ walder C, Schlossmacher MG. α‑synuclein and tau concentrations in cerebrospinal fluid of patients presenting with parkinsonism: a cohort study. Lancet Neurol. 2011;10:230–40.
15. LeWitt P, Schultz L, Auinger P, Lu M. CSF xanthine, homovanillic acid, and their ratio as biomarkers of Parkinson’s disease. Brain Res. 2011;1408:88–97.
16. van Dijk KD, Bidinosti M, Weiss A, Raijmakers P, Berendse HW, van de Berg WD. Reduced α‑synuclein levels in cerebrospinal fluid in Parkinson’s dis‑ ease are unrelated to clinical and imaging measures of disease severity. Eur J Neurol. 2014;21:388–94.
17. Lee PH, Lee G, Park HJ, Bang OY, Joo IS, Huh K. The plasma alpha‑ synuclein levels in patients with Parkinson’s disease and multiple system atrophy. J Neural Transm. 2006;113:1435–9.
18. Li QX, Mok SS, Laughton KM, McLean CA, Cappai R, Masters CL, Culvenor JG, Horne MK. Plasma alpha‑synuclein is decreased in subjects with Parkinson’s disease. Exp Neurol. 2007;204:583–8.
19. Shi M, Zabetian CP, Hancock AM, Ginghina C, Hong Z, Yearout D, Chung KA, Quinn JF, Peskind ER, Galasko D, Jankovic J, Leverenz JB, Zhang J. Significance and confounders of peripheral DJ‑1 and alpha‑synuclein in Parkinson’s disease. Neurosci Lett. 2010;480:78–82.
20. Fjorback AW, Varming K, Jensen PH. Determination of alpha‑synuclein concentration in human plasma using ELISA. Scand J Clin Lab Invest. 2007;67:431–5.
21. Chiu MJ, Horng HE, Chieh JJ, Liao SH, Chen CH, Shih BY, Yang CC, Lee CL, Chen TF, Yang SY, Hong CY, Yang HC. Multi‑channel SQUID‑based ultra‑high‑sensitivity in vitro detections for bio‑markers of Alzheimer’s disease via immunomagnetic reduction. IEEE Trans Appl Supercond. 2011;21:477–80.
22. Yang CC, Yang SY, Chieh JJ, Horng HE, Hong CY, Yang HC, Chen KH, Shih BY, Chen TF, Chiu MJ. Biofunctionalized magnetic nanoparticles for spe‑ cifically detecting biomarkers of Alzheimer’s disease in vitro. ACS Chem Neurosci. 2011;2:500–5.
23. Yang SY, Chieh JJ, Yang CC, Liao SH, Chen HH, Horng HE, Yang HC, Hong CY, Chiu MJ, Chen TF, Huang KW, Wu CC. Clinic applications in assaying ultra‑low‑concentration bio‑markers using HTS SQUID‑based AC magne‑ tosusceptometer. IEEE Trans Appl Supercond. 2013;23:1600604–7. 24. Chiu MJ, Chen YF, Chen TF, Yang SY, Yang FPG, Tseng TW, Chieh JJ, Chen
JCR, Tzen KY, Hua MS, Horng HE. Plasma tau as a window to the brain‑ negative associations with brain volume and memory function in mild cognitive impairment and early alzheimer’s disease. Human Barin Map‑ ping. 2013;35:3132–42.
25. Tzen KY, Yang SY, Chen TF, Cheng TW, Horng HE, Wen HP, Huang YY, Shiue CY, Chiu MJ. Plasma Aβ but not tau is related to brain PiB retention in early Alzheimer’s disease. ACS Neuro Chem. 2014;5:830–6.
26. Chiu MJ, Yang SY, Horng HE, Yang CC, Chen TF, Chieh JJ, Chen HH, Chen TC, Ho CS, Chang SF, Liu HC, Hong CY, Yang HC. Combined plasma biomarkers for diagnosing mild cognition impairment and Alzheimer’s disease. ACS Chem Neurosci. 2013;4:1530–6.
27. Yang SY, Chieh JJ, Huang KW, Yang CC, Chen TC, Ho CS, Chang SF, Chen HH, Horng HE, Hong CY, Yang HC: Molecule‑assisted nanoparticle clustering effect in immunomagnetic reduction assay. J Appl Phys 2013, 144903‑1‑5.
28. Chieh JJ, Yang SY, Horng HE, Yu CY, Lee CL, Wu HL, Hong CY, Yang HC: Immunomagneticreduction assay using high‑Tc superconducting‑quan‑ tum‑interference‑device‑based magnetosusceptometry. J Appl Phys 2010, 107:074903‑1‑5.
29. Irwin DJ, Lee VMY, Trojanowski JQ. Parkinson’s disease dementia: con‑ vergence of α‑synuclein, tau and amyloid‑β pathologies. Nature Rev Neurosci. 2013;14:626–36.
30. Lin CH, Wu RM. Biomarkers of cognitive decline in Parkinson’s disease. Parkinsonism Relat Disord. 2015;21:431–43.
• We accept pre-submission inquiries
• Our selector tool helps you to find the most relevant journal • We provide round the clock customer support
• Convenient online submission • Thorough peer review
• Inclusion in PubMed and all major indexing services • Maximum visibility for your research
Submit your manuscript at www.biomedcentral.com/submit
Submit your next manuscript to BioMed Central
and we will help you at every step:
31. Foulds PG, Mitchell JD, Parker A, Turner R, Green G, Diggle P, Hasegawa M, Taylor M, Mann D, Allsop D. Phosphorylated α‑synuclein can be detected in blood plasma and is potentially a useful biomarker for Parkinson’s disease. FASEB. 2011;25:4127–37.
32. Ishii R, Tokuda T, Tatebe H, Ohmichi T, Kasai T, Nakagawa M, Mizuno T, El‑Agnaf OMA. Decrease in plasma levels of α‑synuclein is evident in patient with Parkinson’s Disease after elimination of heterophilic antibody interference. Plos One. 2015;10:e0123162.
33. CLSI document EP7‑A2 (ISBN 1‑56238‑584‑4).
34. Huang KW, Yang SY, Hong YW, Chieh JJ, Yang CC, Horng HE, Wu CC, Hong CY, Yang HC. Feasibility studies for assaying alpha‑fetoprotein using anti‑ body‑ activated magnetic nanoparticles. Int J Nanomed. 2012;7:1991–6. 35. Yang CC, Huang KW, Yang SY, Chen HH, Chen TC, Ho CS, Chang SF, Chieh
JJ, Horng HE, Hong CY, Yang HC. Development for high‑accuracy in vitro assay of vascular endothelial growth factor using nanomagnetically labeled immunoassay. J NanoMater. 2013;2013:69527682‑1–7. 36. Yang CC, Yang SY, Ho CS, Chang JF, Liu BH, Huang KW. Development of
antibody functionalized magnetic nanoparticles for the immunoassay of carcinoembryonic antigen: a feasibility study for clinical use. J. Nanobio‑ tech. 2014;12:44–52.
37. Yang SY, Wang WC, Lan CB, Chen CH, Chieh JJ, Horng HE, Hong CY, Yang HC, Tsai CP, Yang CY, Cheng IC, Chung WC. Magnetically enhanced high‑ specificity virus detection using bio‑activated magnetic nanoparticles with antibodies as labeling markers. J Virol Methods. 2010;164:14–8. 38. Horng HE, Yang SY, Huang YW, Jiang WQ, Hong CY, Yang HC. Nanomag‑
netic particles for SQUID‑based magnetically labeled immunoassay. IEEE Trans Appl Supercond. 2005;15:668–71.
39. Yang SY, Jian ZF, Horng HE, Hong CY, Yang HC, Wu CC, Lee YH. Dual immobilization and magnetic manipulation of magnetic nanoparticles. J Magn Magn Mater. 2008;320:2688–91.
40. Chieh JJ, Yang SY, Jian ZF, Wang WC, Horng HE, Yang HC, Hong CY: Hyper‑ high‑sensitivity wash‑free magnetoreduction assay on biomolecules using high‑Tc superconducting quantum interference devices. J Appl Phys 2008, 103:014703‑1‑6.