Independent and joint effect of type 2 diabetes and gastric and hepatobiliary diseases on risk of pancreatic cancer risk: 10-year follow-up of population-based cohort
Cheng-Chieh Lin,1,2,3 Jen-Huai Chiang,†4,5,6 Chia-Ing Li, 2,3 Teng-Fu Hsieh, 7,8,9 Chiu-Shong Liu, 1,2,3
Wen-Yuan Lin,1,2 Yih-Dar Lee,10,11 Tsai-Chung Li 4,12*
1. Department of Family Medicine, China Medical University Hospital, Taichung, Taiwan 2. School of Medicine, College of Medicine, China Medical University, Taichung, Taiwan 3. Department of Medical Research, China Medical University Hospital, Taichung, Taiwan
4. Graduate Institute of Biostatistics, College of Management, China Medical University, Taichung, Taiwan
5. Management Office for Health Data, China Medical University Hospital, Taichung, Taiwan
6. Research Center for Chinese Medicine & Acupuncture, China Medical University, Taichung, Taiwan
7. Division of Urology, Department of Surgery, Buddhist Tzu Chi General Hospital, Taichung Branch, Taichung, Taiwan
8. School of Medicine, Buddhist Tzu Chi University, Hualien, Taiwan
9. Graduate Institute of Clinical Medical Science, College of Medicine, China Medical University, Taichung, Taiwan
10. Department of Psychiatry, Medical College, National Cheng-Kung University, Tainan, Taiwan 11. Bristol-Myers Squibb (Taiwan) Ltd, Global Development & Medical Affairs, Taipei, Taiwan 12. Department of Healthcare Administration, College of Medical and Health Science, Asia
University, Taichung, Taiwan * Correspondence to: Tsai-Chung Li
China Medical University, 91 Hsueh-Shih Road, Taichung, 40421, Taiwan, Tel: 886-4-2205-3366 ext. 6605, Fax: 886-4-2207-8539, e-mail: [email protected]
†Equal contribution as the first author
Running title: Pancreatic cancer risks with T2DM
Abstract
Background:Type 2 diabetes mellitus, gastric and hapatobiliary comorbidities, and cancer share common risk factors: e.g., tobacco, obesity, physical inactivity, high calorie intake, metabolic disorders. Prior studies find type 2 diabetes and gastric and hapatobiliary comorbidities heightening risk of pancreatic cancer. Yet joint association of type 2 diabetes mellitus and gastric and
hapatobiliary comorbidities on pancreatic cancer risk has not been assessed.
Methods: This study rates independent/joint effects of type 2 diabetes as well as gastric and
hapatobiliary comorbidity on pancreatic cancer risk for a retrospective population-based cohort of 166,850 type 2 diabetics identified in 1997-1998 and followed for 10-11 years, comparing their cancer incidence with that of 166,850 non-diabetics matched for age, gender, and locale. Time-dependent Cox’s proportional hazards model evaluted joint association of type 2 diabetes and chronic conditions on pancreatic cancer risk.
Results: A total of 1,178 subjects were newly diagnosed with pancreatic cancer during follow-up,
with incidence rates of 0.49 per 1,000 person-years in type 2 diabetics cohort and 0.26 per 1,000 person-years in the non-diabetics cohort. We observed greater magnitude of HRs of pancreatic cancer for patients with type 2 diabetes along with acute alcoholic hepatitis, acute pancreatitis, cholecystitis, and gastric ulcer compared with patients without type 2 diabetes or counterpart
comorbidity (hazard ratio [HR]: 1.36, 95% confidence interval [CI]: 1.19-1.56; 1.74, 1.23-2.45; 9.18, 7.44-11.33; and 2.31, 1.98-2.70, respectively). Main effects of type 2 diabetes were all statistically with narrow 95% CI and remained similar across risk stratification with various comorbidities: range 1.59-1.80.
Conclusions: Our study demonstrates that pre-existing type 2 diabetes, acute alcoholic hepatitis,
acute pancreatitis, cholecystitis, and gastric ulcer independently or jointly predicts subsequent pancreatic cancer risk. Clinicians must recognize burden of these gastric and hepatobiliary comorbidities and keep clinically vigilant for their diagnosis.
Keywords: type 2 diabetes; pancreatic cancer; gastric diseases; hepatobiliary diseases; gastric
Introduction
Cancer has ranked number-one cause of death in Taiwan since 1982, and average age of those diagnosed with it shows trend a downward. Taiwan’s Department of Health national statistics report cited pancreatic cancer in 2012 ranking ninth highest overall for cancer death among the Taiwanese population: 6.4 per 100,000 (Ministry of Health and Welfare, 2012).
Type 2 diabetes mellitus, gastric and hepatobiliary comorbidity, and cancers share common risk factors, including tobacco, alcohol, obesity, physical inactivity, a high calorie (particularly saturated fat) intake, and metabolic disorders (Cornier MA et al, 2008; Giovannucci E et al, 2007; Xue F et al, 2007). The possible biological mechanism that type 2 diabetes and gastric and hepatobiliary comorbidity contributed to elevated risk of developing pancreatic cancer may be via inflammatory (Lee DF et al, 2008). Prior bench studies show that dysregulation of tuberous sclerosis 1 (TSC1)/TSC2/mTOR signaling pathway by IκB kinaseβ (IKKβ) is a common molecular switch for both cancer pathogenesis and diet- and obesity-induced insulin resistance (Lee DF et al, 2008). Obesity-derived chronic inflammation with insulin resistance is also associated with gastric and hepatobiliary comorbidity (Farrow B et al, 2002).
Previous population studies using rate standardization indicate pancreatic cancer strongly correlating with type 2 diabetes (Atchison EA et al, 2011; Ben Q et al, 2011a; Ben Q et al, 2011b; Hemminki K et al, 2010; Lin CC et al, 2014). Several studies further rated association of pancreatic cancer with type 2 diabetes (Chen HF et al, 2011; Chodick G et al, 2010; Ogunleye AA et al, 2009; Stevens RJ et al, 2009; Jee SH et al, 2005; Coughlin SS et al, 2004) to elucidate such association after adjusting for traditional risk factors in across ethnicities (Chodick G et al, 2010; Ogunleye AA et al, 2009; Stevens RJ et al, 2009; Lam EK et al, 2010; Larsson SC et al, 2005),but this line of study conducted in a Chinese population was limited (Chen HF et al, 2011). Since 2000, several case-control and cohort studies explored the association between type 2 diabetes and pancreatic cancer (Frye JN et al, 2000; Silverman DT, 2001; Bonelli L et al, 2003; Rulyak SJ et al, 2003; Inoue M et al, 2003; Batty GD et al, 2004; Jee SH et al, 2005; Lund Nilsen TI et al, 2000; Gapstur SM et al, 2000; Stolzenberg-Solomon RZ et al, 2002; Lin Y et al, 2002; Coughlin SS et al, 2004). One
case-control study reported that type 2 diabetes was associated with 2.8-fold increased risk of pancreatic cancer (Bonelli L et al, 2003) whereas two case-control studies did not observe a significant association (Frye JN et al, 2000; Silverman DT, 2001). Similarly, findings of most prior cohort studies supported this association with a relative risk ranging from 1.48 to 3.99 (Rulyak SJ et al, 2003; Inoue M et al, 2003; Batty GD et al, 2004; Jee SH et al, 2005; Gapstur SM et al, 2000; Stolzenberg-Solomon RZ et al, 2002; Lin Y et al, 2002; Coughlin SS et al, 2004). Only two cohort studies did not support the hypothesis that patients with type 2 diabetes are more likely to develop pancreatic cancer (Lund Nilsen TI et al, 2000). However, none of these studies considered gastric and hepatobiliary comorbidity.
Some researchers exploring links between type 2 diabetes and pancreatic cancer, took gastric and hepatobiliary comorbidity such as acute pancreatitis, chronic pancreatitis, alcoholic liver disease, pancreatic pseudocyst, cholelithiasis (Bansal P et al, 1995), gallbladder disease (Bracci PM et al, 2009), hepatitis B, hepatitis C, cholecystitis, cholangitits, cholelithiasis, gastric ulcer and duodenal ulcer (Chen HF et al, 2011) into account; none considered joint effect with type 2 diabetes on pancreatic cancer. This population-based study examined independent and joint association of type 2 diabetes and gastric or hapatobiliary comorbidities on pancreatic cancer risk in Taiwan.
Methods
A single-payer national health insurance (NHI) program was implemented in March 1995. As of 2007, 22.60 million of Taiwan’s 22.96 million populations enrolled. Nation-run Bureau of National Health Insurance (BNHI) contracted with 97% of hospitals as well as 92% of clinics nationwide (Ministry of Health and Welfare, 2012).
Our population-based cohort study used type 2 diabetes patients (aged ≥ 20 years) identified in 1997-1998 and followed up through December 31, 2010 or until the first manifestation of pancreatic cancer. Population with type 2 diabetes should have at least three ambulatory claims or at least one inpatient claim with diagnosis of ICD-9-CM code 250 or A-code A181 in 1997-1998. To exclude those individuals with type 1 diabetes, we have done two steps. First, we identify all individuals with type 1 diabetes from Registry for Catastrophic Illness database. Second, we excluded those
individuals with type 1 diabetes identified in the first step from our study cohort with diabetes. We excluded subjects with type 1 diabetes (N=3,750) and any cancer type at baseline (N = 135,060) from 633,680 patients with type 2 diabetes, aged < 20 years (N = 17,679), and/or with incomplete information on gender as well as residential area (N =4,212). This left 472,979 patients with type 2 diabetes. Subjects from the general population were selected from Longitudinal Health Insurance Database 2005 (LHID2005) created by National Health Research Institutes (NHRI) by randomly sampling 1,000,000 beneficiaries from Registry for Beneficiaries data files for Year 2005. Our sample proved representative of the overall population (Tseng CH et al, 2012). Database contained all longitudinal reimbursement information of this random sample from 1996 to the end of 2010. There were a total of 874,053 subjects in 1997-1998 in the file of LHID2005; excluding those with type 1 diabetes (N=363) from Registry for Catastrophic Illness database, cancer (N=28,550), diabetes (N=121,227), and/or age under 20 years (N=304,293) in 1997-1998, as well as those with incomplete information on sex and residential area (N=11), left 419,609 eligible non-diabetics. The same eligibility criteria applied to each group, yet distribution of age, gender, and residential areas was unbalanced between groups. To bolster comparability between cases of type 2 diabetes and persons without diabetes, we randomly selected equal numbers of type 2 diabetics and non-diabetics from each stratum of combination of age (5-year groups), sex and residential areas (25 counties or cities). This left 166,850 patients with type 2 diabetes and individuals without any diabetes in 1997 to 1998 (Figure 1). Baseline or index date for type 2 diabetes group was date of first outpatient visit or inpatient admission. For non-diabetics, index date was randomly assigned from January 1, 1997 to December 31, 1998 according to index date distribution of type 2 diabetes group.
All datasets can be interlinked via individual personal identification number (PIN), which was scrambled cryptographically by NHIRD to protect enrollee’s privacy. Ambulatory care claims contain the individual’s gender and birthday, date of visit, and codes for International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM) codes, or A-codes for three primary diagnoses. Inpatient claims contain ICD-9-CM codes for principal diagnosis up to four secondary diagnoses. The primary outcome was a new diagnosis of pancreatic cancer (ICD-9-CM code 157;
A-code A096), including all malignant pancreatic tumors such as adenocarcinoma and pancreatic endocrine tumors after index date during the follow up. Gastric and hepatobiliary comorbidity comprised acute or chronic pancreatitis, acute hepatitis, alcoholic fatty liver or cirrhosis, acute alcoholic hepatitis, cholelithiasis, morbid obesity, alcohol dependence syndrome, pseudocyst of pancreas, jaundice, hepatitis B, hepatitis C, cholecystitis, cholangitis, gastric ulcer and duodenal ulcer. Each individual patient’s status of gastric and hepatobiliary comorbidities at each year was identified for time-dependent data analysis. Sociodemographic factors include age, gender, insurance premium, and urbanization degree of residential area. Age was divided into 17 groups with five-year intervals from 20 to >90 years. Gender was categorized as male and female, insurance according to median of amounts of premiums, in which median value for these two groups was both NT$19,200 from 1997 to 1998. We used an urbanization indicator developed by Liu et al (Liu CY et al, 2006), who categorized 365 Taiwan towns as per degrees of urbanization: high- and medium-density urban areas, newly developed area, general area, aging-society area, rural area, and non-developed area (Liu CY et al, 2006).
We compared baseline characteristic between subjects with and without type 2 diabetes using standardized mean differences. All standardized mean differences were less than 0.1 SD, indicating a negligible difference in means or proportions between two groups. Time-dependent Cox’s proportional hazards model evaluted hazards ratio of type 2 diabetes on pancreatic cancer. Time-dependent covariates included acute or chronic pancreatitis, acute hepatitis, alcoholic fatty liver or cirrhosis, acute alcoholic hepatitis, cholelithiasis, morbid obesity, alcohol dependence syndrome, pseudocyst of pancreas, jaundice, hepatitis B, hepatitis C, cholecystitis, cholangitis, gastric ulcer and duodenal ulcer. Outcome variable was timed to occurrence of newly diagnosed pancreatic cancer during study period. A subject were censored if he or she died, developed non-pancreatic cancer or else did not develop pancreatic cancer before end of study. For selected independent variables that result in a “best” model, we followed four steps (Hosmer DW et al, 2000). First, selection process began with a careful univariable analysis of each variable. Second, on completion of univariate analysis, we selected variable whose univariable test has a p-value<0.25 (Bendel RB et al, 1997;
Mickey RM et al, 1989) as a candidate for our multivariable model. Third, enter candidate variables into the multivariable model. With some co-morbidity variables highly collinear, we estimated their regression coefficients and compared these for significance. Only one such highly correlated variable remained in a multivariate Cox model. Lastly, after refining a main effects model, we checked assumption of Cox’s proportional hazard model for all variables in our multivariate model, further examining interactions between independent variables.
Results
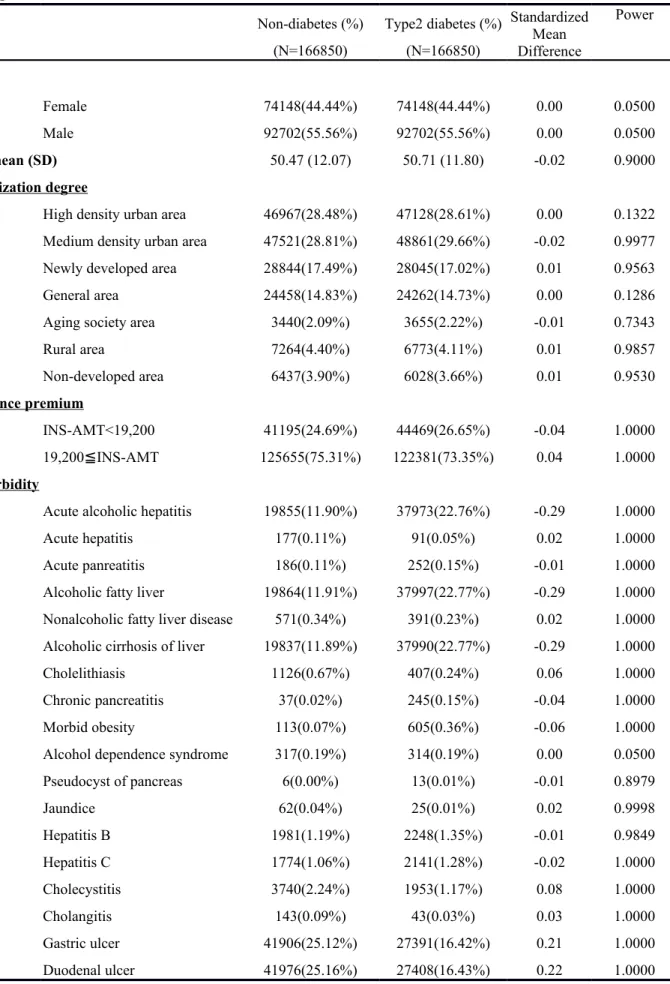
Table 1 shows baseline characteristics according to status of type 2 diabetes. Subjects with and without type 2 diabetes had similar distributions of gender, age, and residential area. Percentages of female and male were 44.44% and 55.56%. Compared to non-diabetics, type 2 diabetics had higher proportion of aging society area, insurance premium less than NT$19,200, gastric and hepatobiliary co-morbidities for acute alcoholic hepatitis, acute hepatitis, acute pancreatitis, alcoholic fatty liver and/or cirrhosis, nonalcoholic fatty liver, cholelithiasis, chronic pancreatitis, morbid obesity, alcohol dependence, pseudocyst of pancreas, jaundice, hepatitis B, hepatitis C and cholangitis.
A total of 1,178 subjects were newly diagnosed with pancreatic cancer during follow-up, with incidence rates of 0.49 per 1,000 years in type 2 diabetics cohort and 0.26 per 1,000 person-years in the non-diabetics cohort. Table 2 displays uni- and multivariate time-dependent Cox's proportional hazard models in a cohort of type 2 diabetics versus general population during 1999-2010. Our model building strategy determined a final multivariable model shown in Table 2. Significant adjusted hazard ratios of pancreatic cancer in Cox proportional hazard models were type 2 diabetes (hazard ratio: 1.50, 95% CI: 1.32-1.71), age (per 5 years) (1.18, 1.75-1.21), men (1.31, 1.16-1.47), acute alcoholic hepatitis (1.36, 1.19-1.56), acute pancreatitis (1.74, 1.23-2.45), cholelithiasis (0.46, 0.33-0.62), chronic pancreatitis (2.55, 1.69-3.87), cholangitis (9.18, 7.44-11.33), gastric ulcer (2.31, 1.98-2.70), and duodenal ulcer (0.51, 0.43-0.60).
In sensitivity analysis by calculating follow-up starting one or three years after baseline to rule out the possibility of reverse causaility, type 2 diabetes also showed strong linkage with pancreatic cancer during follow-up starting one year after baseline (hazard ratio: 1.57, 95% CI: 1.38-1.78,
P<0.0001), as well as follow-up beginning three years later (HR: 1.43, 95% CI: 1.25-1.63). Figure 2
shows adjusted HR of pancreatic cancer for joint effects of type 2 diabetes and acute alcoholic hepatitis, acute pancreatitis, nonalcoholic fatty liver disease, cholelithiasis, cholecystitis, cholangitis, gastric ulcer, and duodenal ulcer. We observed greater magnitude of HRs of pancreatic cancer for type 2 diabetics with acute alcoholic hepatitis, acute pancreatitis, cholecystitis, cholangitis and gastric ulcer versus patients with neither type 2 diabetes nor counterpart comorbidity (2.15, 1.81-2.56; 6.55, 2.52-17.04; 3.34, 2.16-5.16; 7.30, 1.01-52.78 and 4.41, 2.38-8.20, respectively). Independent effects of type 2 diabetes were all statistically significant, with narrow 95% CI, and remained similar across risk stratification with comorbidity (range 1.59-1.80). Factors exerting significant independent effect were acute alcoholic hepatitis (1.35, 1.18-1.55), cholecystitis (2.02, 1.47-2.77), and gastric ulcer (2.85, 1.56-5.18). Due to limited number of study subjects with chronic pancreatic or alcohol dependence syndrome, joint association of type 2 diabetes with these was not evaluated. In addition, we detected significant interaction of type 2 diabetes with cholelithiasis, gastric ulcer, and duodenal ulcer (p=0.027, 0.007, and 0.001, respectively).
Discussion
This study evaluated association between type 2 diabetes and pancreatic cancer among a large prospective cohort to find positive association between type 2 diabetes and pancreatic cancer during 10-11 year follow-up. Our study’s findings show that patients with type 2 diabetes are associated with increased risk of pancreatic cancer; sensitivity analyses remained similar after adjustment for sociodemography and time-dependent co-morbidity, to rule out reverse causality. We observed significant joint associations between type 2 diabetes and acute alcoholic hepatitis, acute pancreatitis, cholecystitis, and gastric ulcer on pancreatic cancer risk.
Most previous studies correlating diabetes with pancreatic cancer indicate type 2 diabetes as a risk factor (Chen HF et al, 2011; Chodick G et al, 2010; Ogunleye AA et al, 2009; Stevens RJ et al, 2009; Jee SH et al, 2005; Coughlin SS et al, 2004; Lam EK et al, 2011; Larsson SC et al, 2005; Inoue M et al, 2006; Khan M et al, 2006), although one conducted in Japan observed no such association (Khan M et al, 2006). Temporal association between diabetes and pancreatic cancer has been
questioned; some studies had too short a follow-up (Chen HF et al, 2011; Lam EK et al, 2011). It is likely that pancreatic cancer could lead to diabetes by abnormal glucose metabolism (so-called “reverse-causality” or effect-cause). The American Society of Clinical Oncology (ASCO) Annual Meeting in 2010 reported temporal association between type 2 diabetes and pancreatic cancer as unclear (Matsubayashi H et al, 2011). It may be that a small portion of pancreatic cancer belonging to neuroendocrine tumor secretes diverse hormones that cause florid stomach ulcers or uncontrolled high blood pressure and diabetes (Ghaneh P et al, 2007). To rule out reverse causation or effect-cause association, we evaluated this association at the outset of follow-up; one and three years after baseline, hazard ratio remained significant. This finding enhances causative association.
Type 2 diabetes has been confirmed as a risk factor for development of pancreatic cancer (Chen HF et al, 2011; Chodick G et al, 2010; Ogunleye AA et al, 2009; Stevens RJ et al, 2009; Lam EK et al, 2011; Larsson SC et al, 2005; Inoue M et al, 2006), but this association has so far been described for its independent effect. Some previous studies accounted for acute pancreatitis, chronic pancreatitis, alcoholic liver disease, pancreatic pseudocyst and cholelithiasis (Bansal P et al, 1995); one of them considered gallbladder disease (Bracci PM et al, 2009), whereas another adjusted for hepatitis B, hepatitis C, cholecystitis, cholangitits, cholelithiasis, gastric ulcer and duodenal ulcer (Chen HF et al, 2011), however, none of them consider their joint effect with type 2 diabetes on pancreatic cancer. It is unclear whether type 2 diabetes and other gastric and hepatobiliary comorbidities play significant joint roles. Our research showed history of acute alcoholic hepatitis, acute pancreatitis, cholecystitis, and gastric jointly associated with type 2 diabetes for higher risk. Data further suggest acute alcoholic hepatitis, cholecystitis, and gastric ulcer as risk factors.
Prior studies report antidiabetic medication altering association between diabetes and pancreatic cancer (Yang YX, 2009). Metformin and thiazolidinediones (TZDs) protect against tumorigenesis; sulfonylurea raised risk (Yang YX, 2009; Giovannucci E et al, 2010; Lee MS et al, 2011). One study demonstrated great reduction in pancreatic cancer risk for metformin users (Lee MS et al, 2011), sulfonylureas elevating risk (Bodmer M et al, 2012). We tallied about 10% each for sulfonylurea monotherapy and metformin monotherapy (data not shown). Impact of antidiabetic medication on
linkage between type 2 diabetes and pancreatic cancer can thus be ignored. Among the merits of our study: it is based on a large and representative population-based sample, hence adequate to detect independent and joint effect of type 2 diabetes and such comorbidity. Also, high coverage rate of NHI program throughout our study could minimize number of cohort subjects lost to follow-up. Availability of NHIRD dataset during follow-up can facilitate time-dependent status of comorbidities. Still, there were limitations. First, we could not obtain data of behavioral factors: e.g., tobacco, alcohol, obesity, BMI, physical activity. We did not consider them, yet it is unlikely that the effect of type 2 diabetes and gastric or hapatobiliary comorbidities would arise solely to effect of behavioral factors, which was weakly associated with pancreatic cancer. Second, it lacks histological features or pathological stages of pancreatic cancer and thus could not evaluate histological patterns, molecular markers or clinical stages. Third, it is possible that the effect of type 2 diabetes is due to reverse causality. To rule out this possibility, we performed a sensitivity analysis by calculating follow-up starting one or three years after baseline and the hazard ratios remained significant. However, it is difficult to rule out the possibility of reverse causality due to the weak to moderate association between type 2 diabetes and pancreatic cancer.
Our study highlights pre-existing type 2 diabetes, acute alcoholic hepatitis, acute pancreatitis, chronic pancreatitis, alcohol dependence, cholecystitis, and/or gastric ulcer portending pancreatic cancer. Significant joint effects of acute alcoholic hepatitis, acute pancreatitis, cholecystitis, and gastric ulcer along with type 2 diabetes on pancreatic cancer risk were likewise noted. Clinicians must recognize burden of these gastric and hepatobiliary comorbidities and keep clinically vigilant for diagnosis.
Acknowledgements
This study is supported in part by Taiwan Ministry of Health and Welfare Clinical Trial and Research Center of Excellence (MOHW103-TDU-B-212-113002) and Health and welfare surcharge of tobacco products, China Medical University Hospital Cancer Research Center of Excellence (MOHW103-TD-B-111-03, Taiwan).
References
Atchison EA, Gridley G, Carreon JD, Leitzmann MF, McGlynn KA (2011) Risk of cancer in a large cohort of U.S. veterans with diabetes. Int J Cancer. 128(3): 635-643.
Bansal P, Sonnenberg A (1995) Pancreatitis is a risk factor for pancreatic cancer. Gastroenterology
109(1):247-251.
Batty GD, Shipley MJ, Marmot M, Smith GD (2004) Diabetes status and post-load plasma glucose concentration in relation to site-specific cancer mortality: findings from the original Whitehall study. Cancer Causes Control 15: 873-881.
Ben Q, Cai Q, Li Z, Yuan Y, Ning X, Deng S, Wang K (2011a) The relationship between new-onset diabetes mellitus and pancreatic cancer risk: a case-control study. Eur J Cancer. 47(2):248-254. Ben Q, Xu M, Ning X, Liu J, Hong S, Huang W, Zhang H, Li Z (2011b) Diabetes mellitus and risk
of pancreatic cancer: A meta-analysis of cohort studies. Eur J Cancer. 47(13):1928-1937. Bendel RB, Afifi AA (1977) Comparison of stopping rules in forward regression. Journal of the
American Statistical Association 72:46-53.
Bodmer M, Becker C, Meier C, Jick SS, Meier CR (2012) Use of antidiabetic agents and the risk of pancreatic cancer: a case-control analysis. Am J Gastroenterol. 107(4):620-626.
Bonelli L, Aste H, Bovo P, Cavallini G, Felder M, Gusmaroli R, Morandini E, Ravelli P, Briglia R, Lombardo L, De Micheli A, Pugliese V (2003) Exocrine pancreatic cancer, cigarette smoking, and diabetes mellitus: a case–control study in northern Italy. Pancreas 27:143-149.
Bracci PM, Wang F, Hassan MM, Gupta S, Li D, Holly EA (2009) Pancreatitis and pancreatic cancer in two large pooled case-control studies. Cancer Causes Control 20(9):1723-1731.
Chen HF, Chen P, Li CY (2011) Risk of Malignant Neoplasm of the Pancreas in Relation to Diabetes: A population-based study in Taiwan. Diabetes Care 34(5):1177-1179.
Chodick G, Heymann AD, Rosenmann L, Green MS, Flash S, Porath A, Kokia E, Shalev V (2010) Diabetes and risk of incident cancer: a large population-based cohort study in Israel. Cancer
Causes Control 21(6):879-887.
Cornier MA, Dabelea D, Hernandez TL, Lindstrom RC, Steig AJ, Stob NR, Van Pelt RE, Wang H, Eckel RH (2008) The metabolic syndrome. Endocr Rev. 29(7):777-822.
Coughlin SS, Calle EE, Teras LR, Petrelli J, Thun MJ (2004) Diabetes mellitus as a predictor of cancer mortality in a large cohort of US adults. Am J Epidemiol 159(12):1160-1167.
Farrow B, Evers BM (2002) Inflammation and the development of pancreatic cancer. Surg Oncol
10(4):153-169.
Frye JN, Inder WJ, Dobbs BR, Frizelle FA (2000) Pancreatic cancer and diabetes: is there a relationship? A case-controlled study. Aust NZ J Surg 70:722-724.
Gapstur SM, Gann PH, Lowe W, Liu K, Colangelo L, Dyer A (2000) Abnormal glucose metabolism and pancreatic cancer mortality. JAMA 283:2552-2558.
Ghaneh P, Costello E, Neoptolemos JP (2007) Biology and management of pancreatic cancer. Gut.
Giovannucci E, Harlan DM, Archer MC, Bergenstal RM, Gapstur SM, Habel LA, Pollak M, Regensteiner JG, Yee D (2010) Diabetes and cancer: a consensus report. CA Cancer J Clin
60(4):207-221.
Giovannucci E, Michaud D (2007) The role of obesity and related metabolic disturbances in cancers of the colon, prostate, and pancreas. Gastroenterology. 132(6):2208-2225.
Hemminki K, Li X, Sundquist J, Sundquist K (2010) Risk of cancer following hospitalization for type 2 diabetes. Oncologist. 15(6):548-555.
Hosmer DW, Lemeshow S (2000) Applied Logistic Regression. Second Edition: Wiley-Interscience Publication, 2nd edition.
Inoue M, Iwasaki M, Otani T, Sasazuki S, Noda M, Tsugane S (2006) Diabetes mellitus and the risk of cancer: results from a large-scale population-based cohort study in Japan. Arch Intern Med.
166(17):1871-1877.
Inoue M, Tajima K, Takezaki T, Hamajima N, Hirose K, Ito H, Tominaga S (2003) Epidemiology of pancreatic cancer in Japan: a nested case–control study from the Hospital-based Epidemiologic Research Program at Aichi Cancer Center (HERPACC). Inter J Epidemiol 32:257-262.
Jee SH, Ohrr H, Sull JW, Yun JE, Ji M, Samet JM (2005) Fasting serum glucose level and cancer risk in Korean men and women. JAMA 293(2):194-202.
Khan M, Mori M, Fujino Y, Shibata A, Sakauchi F, Washio M, Tamakoshi A; Japan Collaborative Cohort Study Group (2006) Site-specific cancer risk due to diabetes mellitus history: evidence from the Japan Collaborative Cohort (JACC) Study. Asian Pac J Cancer Prev. 7(2):253-259. Lam EK, Batty GD, Huxley RR, Martiniuk AL, Barzi F, Lam TH, Lawes CM, Giles GG, Welborn T,
Ueshima H, Tamakoshi A, Woo J, Kim HC, Fang X, Czernichow S, Woodward M; Asia Pacific Cohort Studies Collaboration (2011) Associations of diabetes mellitus with site-specific cancer mortality in the Asia-Pacific region. Ann Oncol 22(3):730-738.
Larsson SC, Permert J, Håkansson N, Näslund I, Bergkvist L, Wolk A (2005) Overall obesity, abdominal adiposity, diabetes and cigarette smoking in relation to the risk of pancreatic cancer in two Swedish population-based cohorts. Br J Cancer 93(11):1310-1315.
Lee DF, Kuo HP, Chen CT, Wei Y, Chou CK, Hung JY, Yen CJ, Hung MC (2008) IKKbeta suppression of TSC1 function links the mTOR pathway with insulin resistance. Int J Mol Med.
22(5):633-638.
Lee MS, Hsu CC, Wahlqvist ML, Tsai HN, Chang YH, Huang YC (2011) Type 2 diabetes increases and metformin reduces total, colorectal, liver and pancreatic cancer incidences in Taiwanese: a representative population prospective cohort study of 800,000 individuals. BMC Cancer 11:20. Lin CC, Chiang JH, Li CI, Liu CS, Lin WY, Hsieh TF, Li TC (2014) Cancer risks among patients
with type 2 diabetes: a 10-year follow-up study of a nationwide population-based cohort in Taiwan. BMC Cancer 14:381.
Lin Y, Tamakoshi A, Kawamura T, Inaba Y, Kikuchi S, Motohashi Y, Kurosawa M, Ohno Y (2002) Risk of pancreatic cancer in relation to alcohol drinking, coffee consumption and medical history: findings from the Japan collaborative cohort study for evaluation of cancer risk. Inter J Cancer 99:742-746.
Liu CY, Hung YT, Chuang YL, Chen YJ, Weng WS, Liu JS, Liang KY (2006) Incorporating Development Stratification of Taiwan Townships into Sampling Design of Large Scale Health Interview Survey. Journal of Health Management 4:1-22.
Lund Nilsen TI, Johnsen R, Vatten LJ (2000) Socio-economic and lifestyle factors associated with the risk of prostate cancer. Br J Cancer 82:1358-1363.
Matsubayashi H, Maeda A, Kanemoto H, Uesaka K, Yamazaki K, Hironaka S, Miyagi Y, Ikehara H, Ono H, Klein A, Goggins M (2011) Risk Factors of Familial Pancreatic Cancer in Japan: Current Smoking and Recent Onset of Diabetes. Pancreas. 40(6):974-978.
Mickey RM, Greenland S (1989) The impact of confounder selection criteria on effect estimation.
Am J Epidemiol 129(1): 125-137.
Ministry of Health and Welfare (2012) Statistical Annual Report of Medical Care: National Health Insurance, 2012: http://www.mohw.gov.tw/EN/Ministry/Statistic.aspx?f_list_no=474
Ogunleye AA, Ogston SA, Morris AD, Evans JM (2009) A cohort study of the risk of cancer associated with type 2 diabetes. Br J Cancer 101(7):1199-1201.
Rulyak SJ, Lowenfels AB, Maisonneuve P, Brentnall TA (2003) Risk factors for the development of pancreatic cancer in familial pancreatic cancer kindreds. Gastroenterology 124:1292-1299. Silverman DT (2001) Risk factors for pancreatic cancer: a case–control study based on direct
interviews. Teratogen Carcinogen Mutagen 21:7-25.
Stevens RJ, Roddam AW, Spencer EA, Pirie KL, Reeves GK, Green J, Beral V; Million Women Study Collaborators (2009) Factors associated with incident and fatal pancreatic cancer in a cohort of middle-aged women. Int J Cancer 124(10):2400-2405.
Stolzenberg-Solomon RZ, Pietinen P, Taylor PR, Virtamo J, Albanes D (2002) Prospective study of diet and pancreatic cancer in male smokers. Am J Epidemiol 155:783-792.
Tseng CH, Chen CJ, Landolph JR Jr (2012) Diabetes and cancer: epidemiological, clinical, and experimental perspectives. Exp Diabetes Res. 2012:101802.
Xue F, Michels KB (2007) Diabetes, metabolic syndrome, and breast cancer: a review of the current evidence. Am J Clin Nutr. 86(3):s823-835.
Yang YX (2009) Do diabetes drugs modify the risk of pancreatic cancer? Gastroenterology
Figure Legends:
Figure 1: Flowchart of recruitment procedures
Figure 2. Joint relationship of gastric and hapatobiliary comorbidity and diabetes status on risk of pancreatic cancer. *: p<0.05; **: p<0.01; ***: p<0.001. DM: diabetes mellitus; ALH: alcoholic hepatitis; AP: acute hepatitis; NAFLD: nonalcoholic fatty liver disease.
Table 1 Baseline characteristics of study cohorts by socio-demographic status and comorbidity in Taiwan Non-diabetes (%) (N=166850) Type2 diabetes (%) (N=166850) Standardized Mean Difference Power Sex Female 74148(44.44%) 74148(44.44%) 0.00 0.0500 Male 92702(55.56%) 92702(55.56%) 0.00 0.0500 Age, mean (SD) 50.47 (12.07) 50.71 (11.80) -0.02 0.9000 Urbanization degree
High density urban area 46967(28.48%) 47128(28.61%) 0.00 0.1322
Medium density urban area 47521(28.81%) 48861(29.66%) -0.02 0.9977
Newly developed area 28844(17.49%) 28045(17.02%) 0.01 0.9563
General area 24458(14.83%) 24262(14.73%) 0.00 0.1286
Aging society area 3440(2.09%) 3655(2.22%) -0.01 0.7343
Rural area 7264(4.40%) 6773(4.11%) 0.01 0.9857 Non-developed area 6437(3.90%) 6028(3.66%) 0.01 0.9530 Insurance premium INS-AMT<19,200 41195(24.69%) 44469(26.65%) -0.04 1.0000 19,200≦INS-AMT 125655(75.31%) 122381(73.35%) 0.04 1.0000 Comorbidity
Acute alcoholic hepatitis 19855(11.90%) 37973(22.76%) -0.29 1.0000
Acute hepatitis 177(0.11%) 91(0.05%) 0.02 1.0000
Acute panreatitis 186(0.11%) 252(0.15%) -0.01 1.0000
Alcoholic fatty liver 19864(11.91%) 37997(22.77%) -0.29 1.0000
Nonalcoholic fatty liver disease 571(0.34%) 391(0.23%) 0.02 1.0000
Alcoholic cirrhosis of liver 19837(11.89%) 37990(22.77%) -0.29 1.0000
Cholelithiasis 1126(0.67%) 407(0.24%) 0.06 1.0000
Chronic pancreatitis 37(0.02%) 245(0.15%) -0.04 1.0000
Morbid obesity 113(0.07%) 605(0.36%) -0.06 1.0000
Alcohol dependence syndrome 317(0.19%) 314(0.19%) 0.00 0.0500
Pseudocyst of pancreas 6(0.00%) 13(0.01%) -0.01 0.8979 Jaundice 62(0.04%) 25(0.01%) 0.02 0.9998 Hepatitis B 1981(1.19%) 2248(1.35%) -0.01 0.9849 Hepatitis C 1774(1.06%) 2141(1.28%) -0.02 1.0000 Cholecystitis 3740(2.24%) 1953(1.17%) 0.08 1.0000 Cholangitis 143(0.09%) 43(0.03%) 0.03 1.0000 Gastric ulcer 41906(25.12%) 27391(16.42%) 0.21 1.0000 Duodenal ulcer 41976(25.16%) 27408(16.43%) 0.22 1.0000
Table 2 Risk factors of pancreatic cancer from uni- and multivariate time-dependent Cox’s proportional hazard models in cohort of patients with and without type 2 diabetes during 1999-2010 (n=1,156 for pancreatic cancer). Variable Crude HR (95% CI) P value Adjusted HRb (95% CI) P value Type 2 diabetes 1.61(1.43-1.83) <.0001 1.50 (1.32-1.71) <.0001
Age (per 5 years) 1.19(1.17-1.22) <.0001 1.18 (1.75-1.21) <.0001
Sex (men vs. women) 1.29(1.14-1.45) <.0001 1.31 (1.16-1.47) <.0001
Acute alcoholic hepatitis 1.49(1.31-1.69) <.0001 1.36 (1.19-1.56) <.0001
Acute hepatitis 3.38(2.37-4.83) <.0001
Acute pancreatitis 3.10(2.29-4.19) <.0001 1.74 (1.23-2.45) 0.0018
Alcoholic fatty liver 1.46(1.28-1.66) <.0001
Nonalcoholic fatty liver disease 1.31(1.02-1.67) 0.0332 1.02(0.79-1.32) 0.8674
Alcoholic cirrhosis of liver 1.38(1.22-1.58) <.0001
Cholelithiasis 1.07(0.81-1.41) 0.6533 0.46 (0.33-0.62) <.0001
Chronic pancreatitis 4.64(3.23-6.66) <.0001 2.55 (1.69-3.87) <.0001
Alcohol dependence syndrome 1.16(0.64-2.09) 0.631 0.81 (0.44-1.50) 0.4988
Pseudocyst of pancreas 5.03(1.89-13.40) 0.0012 Hepatitis B 0.71(0.52-0.98) 0.0392 Hepatitis C 0.80(0.56-1.15) 0.2218 Cholecystitis 1.84(1.40-2.40) <.0001 1.21(0.90-1.62) 0.204 Cholangitis 11.81(9.77-14.26) <.0001 9.18(7.44-11.33) <.0001 Gastric ulcer 1.74(1.55-1.95) <.0001 2.31(1.98-2.70) <.0001 Duodenal ulcer 1.07(0.94-1.21) 0.3187 0.51(0.43-0.60) <.0001
Hazard ratios adjusted for residential area, insurance premium and urbanization indicator. Abbreviations: CI, confidence interval.
a Crude hazard ratios without multivariate adjustment.
477,191 subjects eligible 633,680 type2 diabetics (1997-1998) 156,489 Excluded 3,750 Type I diabetes 135,060 Any cancer 17,679 Age<20 4,212Lack information on gender and residential area
472,979 diabetics selected
Figure 1: Flowchart of follow-up cohort selection
419,620 non-diabetics eligible 21,680,686 subjects among total
insured population
454,433 Excluded 363 Type I diabetes
28,550 Any cancer
121,227 Having any diabetes 304,293 Age<20
11 Lack information on
gender and residential area
419,609 non-diabetics selected 874,053 people insured in 1997-1998
in LHID2005 file
166,850 subjects in each cohort
Randomly selected equal number by age, sex and residential area
Figure 2. Joint relationship of gastric and hapatobiliary comorbidity and diabetes status on risk of pancreatic cancer. *: p<0.05; **: p<0.01; ***: p<0.001. DM: diabetes mellitus; ALH: alcoholic hepatitis; AP: acute pancreatitis; NAFLD: nonalcoholic fatty liver disease. Significant interaction of type 2 diabetes with cholelithiasis, gastric ulcer, and duodenal ulcer was detected (p=0.027, 0.007, and 0.001, respectively).