Date 2014/November/5
Type of manuscript: original article
Manuscript title :Increased risk of Parkinson’s disease in cataract
patients: A population-based cohort study
Running head : cataracts and Parkinson’s disease Authors' full names:
Shih-Wei Lai1,2, Cheng-Li Lin3,4, Kuan-Fu Liao5,6, Kao- Chi Chang-Ou6
1School of Medicine, China Medical University and 2Department of Family
Medicine, China Medical University Hospital, Taichung, Taiwan
3Department of Public Health, China Medical University and 4Management
Office for Health Data, China Medical University Hospital, Taichung, Taiwan
5Graduate Institute of Integrated Medicine, China Medical University and 6Department of Internal Medicine, Taichung Tzu Chi General Hospital,
Taichung, Taiwan
Corresponding author: Kuan-Fu Liao, Department of Internal Medicine, Taichung Tzu Chi General Hospital, No.66, Sec. 1, Fongsing Road, Tanzi District, Taichung City, 427, Taiwan
Phone: 886-4-2205-2121 Fax: 886-4-2203-3986
E-mail: [email protected]
ABSTRACT
Background. The purpose of this study was to investigate whether there is an
association between cataracts and Parkinson’s disease in Taiwan. Methods. A retrospective cohort study was conducted to analyze the database of the Taiwan National Health Insurance Program from 1999 to 2002. This study consisted of 26031 individuals aged 40 to 84 years with newly diagnosed cataracts as the cataract group and 25937 randomly selected individuals without cataracts as the
non-cataract group. Both groups were matched for sex, age and index year of diagnosing cataracts. The incidence of Parkinson’s disease by the end of 2011 and the association of Parkinson’s disease with cataracts and other comorbidities were measured. Results. The overall incidence of Parkinson’s disease was 1.48-fold higher in the cataract group than the non-cataract group (3.18 vs. 2.15 per 1000 person-years, crude HR 1.48, 95% CI 1.32, 1.66). After adjusting for confounding factors, the adjusted HR of Parkinson’s disease was 1.26 (95% CI 1.12, 1.42) for the
cataract group, when compared with the non-cataract group. Dementia (HR 2.72, 95% CI 1.92, 3.84), depression (HR 2.09, 95% CI 1.63, 2.66), hypertension (HR 1.42, 95% CI 1.26, 1.61), cerebrovascular disease (HR 1.32, 95% CI 1.07, 1.63) and
age (every one year, HR 1.08, 95% CI 1.07, 1.09) were other factors significantly related to Parkinson’s disease. Conclusions. Overall, this study discloses a 26%
increased hazard of Parkinson’s disease in cataract patients. Further studies are required to investigate whether cataracts are one of non-motor manifestations of
Parkinson’s disease.
INTRODUCTION
Parkinson’s disease is the second most common neurodegenerative disease associated with motor dysfunction, after Alzheimer's disease. Traditionally, the typical motor-related manifestations of Parkinson’s disease are bradykinesia, rigidity
and resting tremor, which result from progressive loss of dopaminergic neurons in the substantia nigra. In addition to motor dysfunction, recently, there is growing evidence demonstrating that numerous non-motor manifestations may exist in
patients with Parkinson’s disease and even may develop before the onset of motor-related manifestations. These non-motor manifestations mainly include anxiety, depression, sleep disorder, as well as gastrointestinal, cognitive and autonomic
dysfunction, but cataracts have not been reported.
Cataracts are one of the leading causes of vision loss worldwide and are also a major public health problem. It is estimated that cataracts account for 39% of the world’s 37 million blind individuals. Although the real etiology of cataracts remains
inconclusive, to date, many factors have been identified to be associated with the risk of cataracts. Moreover, the sparsely available epidemiological studies using a nationwide database have not provided the information of an association between cataracts and Parkinson’s disease. If cataracts are one of non-motor manifestations of Parkinson’s disease, physicians can inform cataract patients about the possibility
of developing Parkinson’s disease. Therefore, we conducted a retrospective cohort study to study the risk of Parkinson’s disease in cataract patients.
MATERIALS AND METHODS Data sources
A retrospective cohort study was conducted to analyze the database of the Taiwan National Health Insurance Program. In a brief, The Taiwan National Health
Insurance Program began in March 1995 and covered at least 99% of 23 million residents in Taiwan. It provides outpatient, hospitalization and emergency services.
The details of this insurance program can be found in previous studies. This study was approved by the Institutional Review Board of China Medical University and
Hospital, Taiwan (CMU-REC-101-012).
Participants
This study consisted of individuals aged 40 to 84 years with newly diagnosed cataracts in 1999-2002 (according to the International Classification of Diseases (ICD) 9th Revision, ICD-9 codes 366) as the cataract group. For each cataract
individual included in this study, one individual without cataracts was randomly selected from the same database as the non-cataract group. Both groups were matched for sex, age (within 5 years) and index year of diagnosing cataracts. We defined the index date as the date of diagnosing cataracts. Both groups were followed up until individuals received a diagnosis of Parkinson’s disease (ICD-9 codes 332.0), withdrawal from the insurance program, loss of follow-up, death or
December 31, 2011.
Comorbidities assessment
To enhance unbiased results, individuals who had a diagnosis of Parkinson’s disease, secondary Parkinsonism or congenital cataracts before the date of
diagnosing cataracts were excluded from the study. Baseline comorbidities were included as follows: cerebrovascular disease, chronic kidney disease, dementia, depression, diabetes mellitus, head injury, hyperlipidemia and hypertension. In order
to increase the diagnosis accuracy and to avoid individuals who were misdiagnosed or were mistakenly coded by similar manifestations with unconfirmed diagnosis,
only those with at least 3 episodes of the same diagnosis for cataracts, Parkinson’s disease and other comorbidities in the ambulatory care could be included in this study. Individuals with only 1-2 episodes of diagnosis of cataracts, Parkinson’s disease or other comorbidities were excluded from this study. All disorders were diagnosed with ICD-9 codes. The validity of disease diagnosis, such as Parkinson’s
diabetes mellitus, head injury, hyperlipidemia and hypertension, was documented in previous studies.
Statistical analysis
We compared the differences in sex, age, and comorbidities between the cataract group and the non-cataract group by the Chi-square test. The incidence of
Parkinson’s disease was calculated as the number of Parkinson’s disease patients identified during follow-up period, divided by the total follow-up person-years for each group. Initially, all variables were included in a univariable Cox proportional hazards regression model. Next, the significant variables were further included in a
multivariable Cox proportional hazards regression model to calculate the hazard ratio (HR) and 95% confidence interval (CI) of Parkinson’s disease. To address the
concern of constant proportionality, we have examined the proportional hazard assumption using a test of scaled Schoenfeld residuals. The test suggests the
proportionality assumption is not violated (P = 0.13). The statistical significance level was set at probability value of < 0.05 (SAS software version 9.1, SAS Institute
Inc., Cary, North Carolina, USA).
RESULTS
Baseline characteristics of the study population
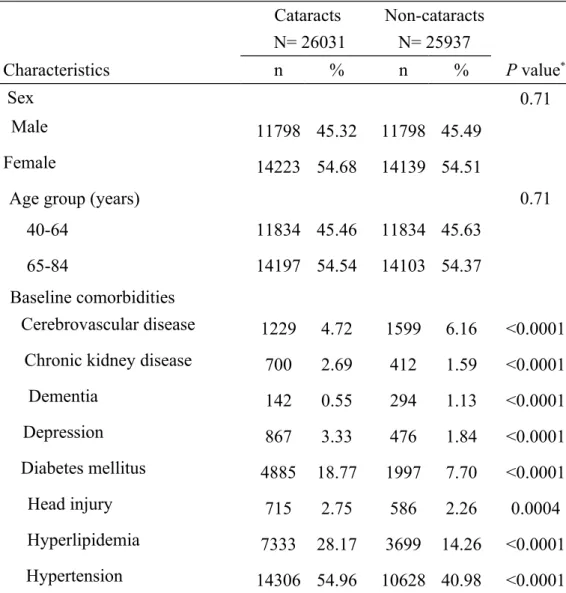
In total, the study included 26031 Individuals in the cataract group and 25937 Individuals in the non-cataract group, with similar distributions in sex and age. Some characteristics of the study population are shown in Table 1. There were
higher proportions of chronic kidney disease, depression, diabetes mellitus, head injury, hyperlipidemia and hypertension in the cataract group than those in the non-cataract group (P = 0.0004 for head injury and P < 0.0001 for others), but
cerebrovascular disease and dementia were more prevalent in the non-cataract group (P < 0.0001). The mean ages (standard deviation) were 65.64 (8.65) years in the cataract group and 65.22 (9.08) years in the non-cataract group.
Incidence of Parkinson’s disease in both groups
At the end of the cohort study, there were 792 Parkinson’s disease patients and 249182 person-years in the cataract group. There were 476 Parkinson’s disease patients and 221579 person-years in the non-cataract group. The overall incidence of
Parkinson’s disease was 3.18 per 1000 person-years in the cataract group and 2.15 per 1000 person-years in the non-cataract group (crude HR 1.48, 95% CI 1.32, 1.66). Figure 1 shows that the cumulative incidence of Parkinson’s disease was higher in the cataract group than that in the non-cataract group for 1.39% by the end
of follow-up (3.87% vs. 2.48%; P < 0.001).
Parkinson’s disease associated with cataracts and other comorbidities
After adjusting for confounding factors, the multivariable Cox proportional hazards regression model showed that the adjusted HR of Parkinson’s disease was 1.26
(95% CI 1.12, 1.42) for the cataract group, when compared with the non-cataract group. Dementia (HR 2.72, 95% CI 1.92, 3.84), depression (HR 2.09, 95% CI 1.63, 2.66), hypertension (HR 1.42, 95% CI 1.26, 1.61), cerebrovascular disease (HR
1.32, 95% CI 1.07, 1.63) and age (every one year, HR 1.08, 95% CI 1.07, 1.09) were other factors significantly related to Parkinson’s disease (Table 2).
DISCUSSION
In this retrospective cohort study, we found that cataract patients were at a 1.26-fold increased hazard of developing Parkinson’s disease. Despite there is a lag period
between the onset of Parkinson’s disease and confirmed diagnosis, we cannot make sure whether cataracts were diagnosed before or after the onset of Parkinson’s
disease. In further analysis, we found that the risk of Parkinson’s disease remained higher even 9 years after cataract diagnosis (adjusted HR1.52, 95% CI 1.10, 2.09,
data not shown in Table). This means that cataracts are potentially associated with the risk of Parkinson’s disease. Although the mechanisms behind the association between cataracts and Parkinson’s disease cannot be determined in this
observational study, the available literature reveals that cataracts and Parkinson’s disease could be linked by mitochondrial dysfunction theory. Mitochondria are highly important intracellular organelles with numerous key cellular functions,
particularly involved in the regulation of energy metabolism, calcium homeostasis, stress response and even apoptosis. Theoretically, mitochondrial genetic mutations cause alteration of mitochondrial activities, including depletion of energy
production, inhibition of the electron transport chain, reactive oxygen species, as well as subsequent oxidative stress, which can result in oxidation of cellular components, loss of cellular function, cellular damage and even apoptosis of lens
and neurons. Therefore, mitochondrial dysfunction, at least partially, could contribute to the pathogenesis of cataracts and Parkinson’s disease.
In further analysis, we found that there was no statistical significance in the incidence of Parkinson’s disease between individuals with and without cataract
extraction among the cataract group (3.41 vs. 2.91 per 1000 person-years, adjusted HR 1.01, 95% CI 0.88, 1.16, data not shown in Table). This finding highlights that cataract extraction does not alter the nature course of Parkinson’s disease. Whether or not undergoing cataract extraction, individuals with cataracts are substantially at an increased hazard of Parkinson’s disease, as compared with the non-cataract
individuals (adjusted HR 1.26, Table 2).
Some limitations should be considered in this present study. First, due to a natural limitation of this study database, we cannot distinguish whether cataracts developed before the onset of motor manifestations of Parkinson’s disease or not. That is, the clinical manifestations of Parkinson’s disease may actually precede cataracts. Second, the cataract group has more comorbidities at baseline than the non-cataract
group did. So individuals with cataracts might be more likely to seek medical help and thereby they were more likely to be diagnosed with Parkinson’s disease. Third,
since cataract patients aged 20-39 did not develop Parkinson’s disease during the follow-up period, only those aged 40-84 were included in this study. Moreover, this is the first epidemiological cohort study using a nationwide database with marked
statistical power to investigate the association between cataracts and Parkinson’s disease.
We conclude that this study discloses a 26% increased hazard of Parkinson’s disease in cataract patients. Further studies are required to investigate whether cataracts are one of non-motor manifestations of Parkinson’s disease.
Funding
This study is supported in part by Taiwan Ministry of Health and Welfare Clinical
Trial and Research Center of Excellence (MOHW103-TDU-B-212-113002). The funding agency did not influence the study design, data collection and analysis,
decision to publish, or preparation of the manuscript.
Specific author contributions
Shih-Wei Lai: (1) substantial contributions to the conception of this article; (2) planned and conducted the study; (3) participated in data interpretation; (4) initiated
the draft of the article and critically revised the article.
Cheng-Li Lin and Kao- Chi Chang-Ou: (1) conducted data analysis; (2) critically revised the article.
Kuan-Fu Liao: (1) planned and conducted the study; (2) participated in data interpretation; (3) critically revised the article.
Conflict of Interest Statement
REFERENCES
[1] Alves G, Forsaa E, Pedersen K, Dreetz Gjerstad M, Larsen J. Epidemiology of Parkinson’s disease. J Neurol. 2008;255:18-32.
[2] Wirdefeldt K, Adami H-O, Cole P, Trichopoulos D, Mandel J. Epidemiology and etiology of Parkinson’s disease: a review of the evidence. European journal of epidemiology. 2011;26:1-58.
[3] Lohle M, Storch A, Reichmann H. Beyond tremor and rigidity: non-motor features of Parkinson's disease. J Neural Transm. 2009;116:1483-92.
[4] Lima MM, Martins EF, Delattre AM, Proenca MB, Mori MA, Carabelli B, et al. Motor and non-motor features of Parkinson's disease - a review of clinical and
experimental studies. CNS Neurol Disord Drug Targets. 2012;11:439-49.
[5] Meissner WG. When does Parkinson's disease begin? From prodromal disease to motor signs. Rev Neurol (Paris). 2012;168:809-14.
[6] Maass A, Reichmann H. Sleep and non-motor symptoms in Parkinson's disease. J Neural Transm. 2013;120:565-9.
[7] Weikel KA, Garber C, Baburins A, Taylor A. Nutritional modulation of cataract. Nutr Rev. 2014;72:30-47.
[8] Hodge WG, Whitcher JP, Satariano W. Risk factors for age-related cataracts. Epidemiol Rev. 1995;17:336-46.
[9] West S. Epidemiology of cataract: accomplishments over 25 years and future directions. Ophthalmic Epidemiol. 2007;14:173-8.
[10] Liao KF, Lai SW, Li CI, Chen WC. Diabetes mellitus correlates with increased risk of pancreatic cancer: a population-based cohort study in Taiwan. J Gastroenterol
Hepatol. 2012;27:709-13.
[11] Lai SW, Liao KF, Liao CC, Muo CH, Liu CS, Sung FC. Polypharmacy correlates with increased risk for hip fracture in the elderly: a population-based study. Medicine (Baltimore). 2010;89:295-9.
[12] Hung SC, Liao KF, Lai SW, Li CI, Chen WC. Risk factors associated with symptomatic cholelithiasis in Taiwan: a population-based study. BMC
Gastroenterol. 2011;11:111.
[13] Lai SW, Liao KF, Chen PC, Tsai PY, Hsieh DP, Chen CC. Antidiabetes drugs correlate with decreased risk of lung cancer: a population-based observation in
Taiwan. Clin Lung Cancer. 2012;13:143-8.
[14] Lai SW, Chen PC, Liao KF, Muo CH, Lin CC, Sung FC. Risk of hepatocellular carcinoma in diabetic patients and risk reduction associated with anti-diabetic therapy: a population-based cohort study. Am J Gastroenterol. 2012;107:46-52.
[15] Lai SW, Liao KF, Lin CL, Sung FC. Irritable bowel syndrome correlates with increased risk of Parkinson's disease in Taiwan. Eur J Epidemiol. 2014;29:57-62. [16] Lai SW, Liao KF, Lin CL, Lin CC, Sung FC. Hearing loss may be a non-motor feature of Parkinson's disease in older people in Taiwan. Eur J Neurol. 2014;21:752-7.
[17] Brennan LA, Kantorow M. Mitochondrial function and redox control in the aging eye: role of MsrA and other repair systems in cataract and macular
degenerations. Exp Eye Res. 2009;88:195-203.
[18] Jarrett SG, Lewin AS, Boulton ME. The importance of mitochondria in age-related and inherited eye disorders. Ophthalmic Res. 2010;44:179-90.
[19] Winklhofer KF, Haass C. Mitochondrial dysfunction in Parkinson's disease. Biochim Biophys Acta. 2010;1802:29-44.
[20] Mounsey RB, Teismann P. Mitochondrial dysfunction in Parkinson's disease: pathogenesis and neuroprotection. Parkinsons Dis. 2010;2011:617472.
[21] Subramaniam SR, Chesselet MF. Mitochondrial dysfunction and oxidative stress in Parkinson's disease. Prog Neurobiol. 2013;106-107:17-32.
Table 1. Basic characteristics between cataract group and non-cataract group Cataracts N= 26031 Non-cataracts N= 25937 Characteristics n % n % P value* Sex 0.71 Male 11798 45.32 11798 45.49 Female 14223 54.68 14139 54.51
Age group (years) 0.71
40-64 11834 45.46 11834 45.63
65-84 14197 54.54 14103 54.37
Baseline comorbidities
Cerebrovascular disease 1229 4.72 1599 6.16 <0.0001 Chronic kidney disease 700 2.69 412 1.59 <0.0001
Dementia 142 0.55 294 1.13 <0.0001 Depression 867 3.33 476 1.84 <0.0001 Diabetes mellitus 4885 18.77 1997 7.70 <0.0001 Head injury 715 2.75 586 2.26 0.0004 Hyperlipidemia 7333 28.17 3699 14.26 <0.0001 Hypertension 14306 54.96 10628 40.98 <0.0001
Data are presented as the number of subjects in each group, with percentages given in parentheses.
Table 2. Multivariable Cox model measured hazard ratio and 95% confidence interval of Parkinson's disease associated with cataracts and other comorbidities
Crude Adjusted†
Variable HR (95%CI) HR (95%CI)
Sex (male vs. female) 1.29 (1.16, 1.44) 0.90 (0.80, 1.00)
Age (per one year) 1.09 (1.08, 1.09) 1.08 (1.07, 1.09)
Baseline comorbidities (yes vs. no)
Cataracts 1.48 (1.32, 1.66) 1.26 (1.12, 1.42)
Cerebrovascular disease 2.15 (1.75, 2.63) 1.32 (1.07, 1.63) Chronic kidney disease 1.21 (0.81, 1.81) 0.85 (0.56, 1.27)
Dementia 5.56 (3.97, 7.78) 2.72 (1.92, 3.84) Depression 2.34 (1.84, 2.98) 2.09 (1.63, 2.66) Diabetes mellitus 1.37 (1.18, 1.59) 1.14 (0.97, 1.33) Head injury 1.44 (1.05, 1.96) 1.18 (0.86, 1.61) Hyperlipidemia 1.26 (1.11, 1.43) 1.10 (0.96, 1.26) Hypertension 2.06 (1.83, 2.30) 1.42 (1.26, 1.61)
†Initially, all variables were included in a univariable Cox proportional hazards
regression model. Only significant variables were further included in a multivariable Cox proportional hazards regression model.
Additionally adjusting for sex, age, cataracts and other comorbidities including
cerebrovascular disease, chronic kidney disease, dementia, depression, diabetes mellitus, head injury, hyperlipidemia and hypertension
Figure 1. Cumulative incidence of Parkinson's disease was higher in individuals with