Original Report: Patient-Oriented, Translational Research
American Journal of Am J Nephrol 2012;36:27¡V33 Received: February 9, 2012
Accepted: April 17, 2012 Nephrology
DOI: 10.1159/000339004
Published online: June 13, 2012
A Comparison of Herpes Zoster Incidence across the Spectrum of Chronic Kidney Disease, Dialysis and Transplantation
Shih-Yi Lin a, b Jiung-Hsiun Liu a, b Cheng-Li Lin c I-Ju Tsaic Pei-Chun Chenc, d
Chi-Jung Chungd, e Yao-Lung Liu a, b I-Kuan Wanga, b Hsin-Hung Lin a, b
Chiu-Ching Huang a, b
aDivision of Nephrology and Kidney Institute, China Medical University Hospital, bChina Medical University,
College of Medicine, cDepartment of Public Health and Management Office for Health Data and d Department of
Health Risk Management and Graduate Institute of Clinical Medical Science, China Medical University and Hospital,
and eDepartment of Medical Research, China Medical University Hospital, Taichung, Taiwan, ROC
Key Words
Peritoneal dialysis End-stage renal disease Abstract
Background: The effect of different renal replacement therapies on the risk of developing herpes zoster in renal failure
patients is unknown. We aimed to investigate the incidence of herpes zoster attack among renal failure patients who were receiving different dialysis modalities, renal
transplantation
(RT), or not receiving any of the above mentioned therapies yet. Methods: A retrospective cohort study of the national health insurance register database was conducted.
This observational cohort study involved 79,581 study controls, 15,802 chronic kidney disease patients, 3,694 hemodialysis
(HD) patients, 317 peritoneal dialysis (PD) patients, and 159 RT patients. Results: The RT group had the worst risk of herpes zoster (hazard ratio, HR, 8.46; 95% CI 5.85¡V12.2), followed
by PD (HR 3.61; 95% CI 2.49¡V4.83) and HD (HR 1.35; 95% CI 1.18¡V1.55), compared with the comparison group (p !
0.0001). The RT group had also the highest risk of developing herpes zoster with complications among all groups (adjusted HR 15.3). The HRs of the PD group were higher than the HRs of the HD group in terms of herpes zoster or its complications (p ! 0.0001 and p = 0.0002, respectively). Conclusions:
This
study suggests that different treatment modalities are associated with different risks of herpes zoster attacks in renal
failure patients. PD patients had higher risks than the HD group in terms of herpes zoster or its complications.
Copyright c 2012 S. Karger AG, Basel Introduction
is not uncommon in clinical practice. Subsequent to primary varicella infection, VZV establishes latency in the
dorsal root ganglia [1]. The reactivation of latent VZV presents as localized shingles and related neurological disorders
usually confined within a dermatome. Old age is the
most well-known risk factor of herpes reactivation [2] . In addition to aging, lymphoproliferative malignancies, receiving immunosuppressants, diabetes and human immunodeficiency
virus disease also predispose patients to the
reactivation of VZV [3¡V6]. Although patients with chron
c 2012 S. Karger AG, Basel Chiu-Ching Huang, MD
0250¡V8095/12/0361¡V0027$38.00/0 China Medical University Hospital Fax +41 61 306 12 34 No. 2, Yu Der Road, Taichung, Taiwan (ROC) E-Mail [email protected] Accessible online at: Tel. +886 04 2205 2121, ext. 2902
ic kidney disease (CKD) or end-stage renal disease (ESRD) are being well recognized as immune-compromised
groups, few studies have actually investigated the relationship between clinical herpes and renal dysfunction [7, 8].
Sato et al. [7] found that ESRD contributed to the herpes attack. Wung et al. [8] showed that renal dysfunction is a
strong risk factor for herpes zoster in patients with Wegener¡¦s granulomatosis. These studies were limited by various
factors: a small number of subjects, a cross-sectional
design, short follow-up time or focusing only on a specific population [7, 8]. Though Kuo et al. [9] have shown that hemodialysis (HD) patients have a higher incidence of herpes than general populations, the epidemiology and complications of herpes zoster have not been investigated or
compared among ESRD patients receiving HD, peritoneal dialysis (PD), or renal transplantation (RT). In terms of
herpes zoster, more than 95% of adults have had VZV infections and would have reactivation later once their
VZV-specific immunity declines [10]. Our previous study implied that ESRD patients could not maintain adequate immunological memory after HBV vaccination, especially
those on PD modality [11]. In the present study, we hypothesized that renal status and dialysis modality might have
impacts on the risk of developing herpes zoster. We conducted a retrospective cohort analysis to assess the incidence
rates of herpes zoster attack and its associated complications among the general population, CKD and ESRD
patients receiving different dialysis modalities. Materials and Methods
Data Source
We used the Longitudinal Health Insurance Database 2000
(LHID2000) from the Taiwan National Health Insurance Institute (NHRI), which contained 1 million beneficiaries randomly
selected from insurers in 1996¡V2008. There were no significant differences in the distribution of sex and age between cohorts in
the LHID2000 and the Taiwan National Health Insurance Program (NHIP) [12, 13]. The NHIP was established in March 1995
by the Bureau of National Health Insurance, Department of Health, with coverage over 99% of Taiwanese residents in 2009 [14]. The LHID2000 contained all registration and medical care data, retrospectively collected to January 1, 1996, and
prospectively
recoded up to December 31, 2008. The coding diagnoses
used International Classification of Diseases Revision 9th Clinical
Modification (ICD-9-CM). Baseline Measurement
We identified all patients with a first diagnosis of CKD, defined as an ICD-9-CM code 585 listed on an inpatient or outpatient
claim, among subjects aged 618 years during 1997¡V2008. Among them, subjects with ESRD were identified by using Catastrophic
Illness Registration and were further classified into three groups, PD, HD and RT (ICD-9-CM code V42.0). Patients with CKD (ICD-9-CM code 585) formed the CKD group. In Taiwan,
patients with ESRD who require regular dialysis are qualified to apply for the catastrophic illness card, with which the copayments are waived. The index date was the date of an initial diagnosis of CKD and the date of the catastrophic illness registration for ESRD for the corresponding groups. The definition of receiving HD or PD was based on the original dialysis modality at the beginning
of ESRD diagnosis. We excluded the following patients:
(1) Patients with herpes zoster diagnosed before the index date, (2) patients who registered catastrophic illness but did not have medical records of dialysis, and (3) patients on dialysis without ESRD registration. If an RT recipient had a prior diagnosis of herpes
according to the treatment modality preceding the RT. A comparison group was randomly selected among patients
without diagnosis of CKD during 1997¡V2008, frequency matched on age, sex, and index year based on a 1:4 ratio. All subjects were
followed up for occurrence of herpes zoster until date of death, date
of loss to follow-up (withdrawal from insurance), or the last date of
follow-up, i.e. December 31, 2008. We also compared the incidence of herpes zoster with complications among the study groups. The presence of complications was defined by the ICD-9 codes
053.0053.8 or ICD-9 code 053 with prescription of pain relievers. The baseline comorbidities analyzed which may increase the
risk of developing herpes zoster include diabetes (ICD-9 code 250), hypertension (ICD-9 codes 401¡V405), lymphoma (ICD-9 codes 203¡V208), malignancy (ICD-9 codes 140¡V202), human immunodeficiency
virus (ICD-9 code 042), systemic lupus erythematosus (SLE; ICD-9 code 710), malnutrition (ICD-9 codes 261¡V
263, V121, V772, V7799), and psychosis (ICD-9 codes 295¡V305). Use of immunosuppressive medications was defined as being
prescribed
within 3 months before the attack of herpes zoster. Statistical Analysis
The differences in demographic characteristics, comorbidities, and prescription of immunosuppressive medications among
the CKD, PD, HD, RT, and the comparison groups were examined by using 2 test for categorical variables and one-way ANOVA for continuous variables. We used the Kaplan-Meier method to estimate the herpes zoster-free rates and the log-rank test to examine the statistical significance of the differences between the study groups. Cox proportion hazard model was used to estimate the
hazard ratios (HRs) and 95% CIs for the risk of developing herpes zoster. Baseline characteristics that were associated with renal
status and herpes zoster in the univariate analysis were included in the multivariate regression model for adjustment. We performed all statistical analysis using SAS 9.1 statistical software
(SAS Institute, Inc., Cary, N.C., USA). A p value of !0.05 was considered
significant. Results
Baseline Characteristics of Patients
During the 12-year period, we included 15,802 patients in the CKD group, 3,694 subjects in the HD group, 317 in the PD group, and 159 in the RT group. The comparison
Am J Nephrol 2012;36:27¡V33 Lin /Liu /Lin /Tsai /Chen /Chung /Liu /
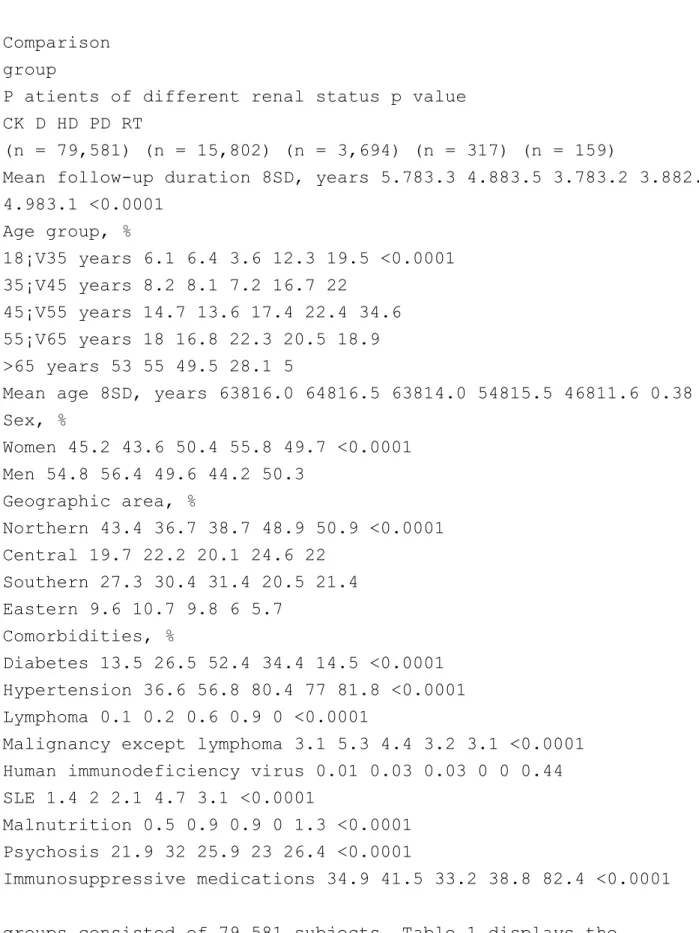
Table 1. Comparison of sociodemographic characteristics,
comorbidities, and medications used in different groups of renal status
Comparison group
P atients of different renal status p value CK D HD PD RT
(n = 79,581) (n = 15,802) (n = 3,694) (n = 317) (n = 159)
Mean follow-up duration 8SD, years 5.783.3 4.883.5 3.783.2 3.882.8 4.983.1 <0.0001 Age group, % 18¡V35 years 6.1 6.4 3.6 12.3 19.5 <0.0001 35¡V45 years 8.2 8.1 7.2 16.7 22 45¡V55 years 14.7 13.6 17.4 22.4 34.6 55¡V65 years 18 16.8 22.3 20.5 18.9 >65 years 53 55 49.5 28.1 5
Mean age 8SD, years 63816.0 64816.5 63814.0 54815.5 46811.6 0.38 Sex, % Women 45.2 43.6 50.4 55.8 49.7 <0.0001 Men 54.8 56.4 49.6 44.2 50.3 Geographic area, % Northern 43.4 36.7 38.7 48.9 50.9 <0.0001 Central 19.7 22.2 20.1 24.6 22 Southern 27.3 30.4 31.4 20.5 21.4 Eastern 9.6 10.7 9.8 6 5.7 Comorbidities, % Diabetes 13.5 26.5 52.4 34.4 14.5 <0.0001 Hypertension 36.6 56.8 80.4 77 81.8 <0.0001 Lymphoma 0.1 0.2 0.6 0.9 0 <0.0001
Malignancy except lymphoma 3.1 5.3 4.4 3.2 3.1 <0.0001 Human immunodeficiency virus 0.01 0.03 0.03 0 0 0.44 SLE 1.4 2 2.1 4.7 3.1 <0.0001
Malnutrition 0.5 0.9 0.9 0 1.3 <0.0001 Psychosis 21.9 32 25.9 23 26.4 <0.0001
Immunosuppressive medications 34.9 41.5 33.2 38.8 82.4 <0.0001 groups consisted of 79,581 subjects. Table 1 displays the
difference of sociodemographic characteristics and comorbidity history among these five groups. Compared to
the comparison group (mean age 63 years), the CKD and
HD group had a similar mean age (64 and 63 years, respectively), but patients in the PD group (54 years) and the
RT group (46 years) were much younger. Patients in the CKD, HD, PD or RT groups had a higher prevalence of all comorbidities and prescriptions with immunosuppressive medications than subjects in the comparison group.
Among the groups of different renal status, the HD group was much more likely to have diabetes with a prevalence rate of 52.4%, while the PD group tended to have SLE or lymphoma. The HD group (80.4%) and RT group (81.8%) had a higher prevalence of hypertension than other
groups. Almost all RT recipients (82.4%) have been prescribed with immunosuppressive medications.
The Risks of Developing Herpes Zoster in Patients with Different Renal Status
The mean duration of follow-up for the comparison group was 5.7 years, approximately 1 year longer than that for the CKD and RT groups and 2 years longer than that for the PD and HD groups (table 1). The herpes zoster-free probability estimated by using Kaplan-Meier
methods revealed significant differences among the five study groups over the follow-up period (fig. 1). The dis-ease-free rate was much lower in patients who underwent PD and RT than in those in the HD, CKD, and the comparison group, and the HD group had a lower disease-free
rate than the CKD and the comparison groups. The incidence density (per 100 person-years) of herpes zoster was
the highest for the PD group (3.82), similar to that for the RT recipients (3.70). The incidence for the HD group was 1.70 per 100 person-years, higher than that for the CKD group and comparison group (1.41 and 1.21 per 100
person-years, respectively). Multivariate regression analyses
Risk of Herpes Zoster among Renal Am J Nephrol 2012;36:27¡V33 Patients
Table 2. HRs for incidence of herpes zoster in different groups of renal status
Case PY Incidence1 H R and 95% CI unadjust ed adjusted
Comparison group 5,551 457,371 1.21 1 (reference) 1 (reference) CKD 1,072 75,971 1.41 1.17 (1.09¡V1.25)** 1.21 (1.13¡V1.29)* ESRD
HD 233 13,682 1.7 1.42 (1.25¡V1.62)** 1.35 (1.18¡V1.55)** PD 46 1,205 3.82 3.22 (2.41¡V4.30)** 3.61 (2.69¡V4.83)** RT 29 783 3.70 3.09 (2.14¡V4.45)** 8.46 (5.85¡V12.2)** Adjusted for age, diabetes, hypertension, lymphoma, SLE, malignancy, psychosis, and immunosuppressive
medications. PY = Person-years. 1 Per 100 person-years. * p < 0.001; ** p < 0.0001. 1.0 Comparison group 0.9 CKD 0.8 HD 0.7 RT 0.6 0.5 PD
0.4
log-rank p < 0.0001
Herpes zoster-free rate 0 2 4 6 810 12 14
Time (years)
Fig. 1. Kaplan-Meier curves of herpes zoster-free rate in patients in different groups of renal status.
showed that compared with the comparison group, the
risk for developing herpes zoster for the RT group was the highest (HR 8.46; 95% CI 5.85¡V12.2). The adjusted HR
was 3.61 in the PD group (95% CI 2.69¡V4.83), 1.35 in the HD group (95% CI 1.18¡V1.55), and 1.21 in the CKD group (95% CI 1.13¡V1.29) (table 2). Furthermore, the HR of her
pes zoster in the PD group was higher than that of the HD group (HR 2.46; 95% CI 1.78¡V3.41; p !
0.0001).
Relationship between Renal Status and Herpes Zoster-Related Complications
Within the 6,931 patients with herpes zoster, 2,590 developed the complication of herpes zoster (table 3). The
RT group had the highest risk of acquiring herpes-related complications (HR 15.3; 95% CI 8.80¡V26.7) compared
with the comparison group, after adjusting for age and comorbidities. The risk was at a similar strength for the PD group (HR 3.94; 95% CI 2.43¡V6.39) and much lower
for the CKD group (HR 1.27; 95% CI 1.14¡V1.42) and the HD group (HR 1.43; 95% CI 1.15¡V1.78). The HR of herpes-related complications in the PD group was higher
than that in the HD group (HR 2.41; 95% CI 1.41¡V4.12; p = 0.0003). As the PD group tended to have more SLE and receive more immunosuppressive medications, we
also analyzed HRs for incidence of herpes zoster in subjects among different groups of renal status without SLE.
The PD group (HR 3.48; 95% CI 2.57¡V4.73) and the RT
group (HR 8.45; 95% CI 5.81¡V12.3) still had a higher risk of herpes zoster (table 4).
Discussion
Our large population-based study revealed one unique finding: renal failure patients receiving RT, PD, or HD have different risks of herpes zoster. PT patients had a
higher incidence of herpes zoster and herpes-related complications than the HD group. This is the first and largest
cohort study to compare the risks of herpes zoster and its related complications in groups with different renal status. Am J Nephrol 2012;36:27¡V33 Lin /Liu /Lin /Tsai /Chen /Chung /Liu /
Table 3. HRs for incidence of herpes zoster with complications in different groups of renal status
Case PY Incidence1 H R and 95% CI unadju sted adjusted
Comparison group 2,053 443,047 0.46 1 (reference) 1 (reference) CKD 417 73,518 0.57 1.23 (1.10¡V1.36)* 1.27 (1.14¡V1.42)*
ESRD
HD 90 13,262 0.68 1.47 (1.19¡V1.82)* 1.43 (1.15¡V1.78)* PD 17 1,113 1.53 3.36 (2.08¡V5.41)** 3.94 (2.43¡V6.39)** RT 13 717 1.81 3.95 (2.29¡V6.81)** 15.3 (8.80¡V26.7)** Adjusted for age, diabetes, hypertension, lymphoma, SLE, malignancy, psychosis, and immunosuppressive
medication. PY = Person-years. 1 Per 100 person-years. * p < 0.001; ** p < 0.0001.
Table 4. HRs for incidence of herpes zoster in different groups of renal status without SLE
Case PY Incidence1 H R and 95% CI unadjusted adjusted
Comparison group 5,472 452,516 1.21 1 (reference) 1 (reference) CKD 1,047 74,616 1.40 1.16 (1.09¡V1.24)** 1.21 (1.13¡V1.29)* ESRD HD 224 13,374 1.67 1.41 (1.23¡V1.61)** 1.32 (1.15¡V1.52)** PD 42 1,146 3.66 3.1 (2.29¡V4.2)** 3.48 (2.57¡V4.73)** Renal transplant 28 757 3.70 3.1 (2.14¡V4.49)** 8.45 (5.81¡V12.3)**
Adjusted for age, diabetes, hypertension, lymphoma, malignancy, psychosis, and immunosuppressive medications.
PY = Person-years. 1 Per 100 person-years. * p < 0.001; ** p < 0.0001.
This study also showed that RT patients have the highest risk of clinical herpes. Post-organ transplantation
[15]. Steroids, antiproliferative agents (azathioprine and mycophenolate), calcineurin inhibitors (cyclosporine and tacrolimus), and target-of-rapamycin inhibitors (sirolimus and everolimus) would interfere with different aspects of immune reaction [15]. It has been suggested that enhanced immunosuppression with mycophenolate
mofetil might be a potential risk factor for herpes zoster in RT recipients [16, 17]. However, Pandya et al. [18] found no significant association existing between VZV infection and specific immune suppressants. The risk for viral
infection is a function of the intensity of exposure and virulence of the specific virus, the intensity of immune
suppression, underlying immune deficits, and factors affecting host susceptibility [19]. It remains inconclusive
whether specific immune suppressant use would lead to an increased risk of herpes zoster.
Our data showed that the risk of developing herpes zoster in the CKD group lay between the comparison and
the ESRD group. Recent studies have attempted to investigate the correlation between declining renal function
and immune defects. Several studies have discovered that selective loss of circulating dendritic cell, naive T-cell, and CD4+ central memory cell counts are related to the
loss of glomerular filtration rate [20, 21]. In a retrospective study of 175 patients, Sato et al. [7] demonstrated a
higher incidence of herpes zoster in CKD stages 4 and 5 than in early-stage CKD patients. Our data might imply that the decline in renal functional status is associated with declining protection against VZV. Further investigations into the direct relationship between the glomerular
filtration rate and the risk of herpes are therefore necessary.
The immunological impairment of uremic status is recognized [22]. This immune incompetence involves
phago-Risk of Herpes Zoster among Renal Am J Nephrol 2012;36:27¡V33 Patients
cytosis, antigen presentation, antibody production, cytokine regulation, and most importantly, T-cell homeostasis
[23, 24]. Our finding that ESRD patients have a
higher incidence of herpes zoster attacks and of herpes
zoster complications than the general population is consistent with that of Sato et al. [7]. Smetana et al. [25] had
noted that VZV was frequently reactivated in HD or PD
patients. Kuo et al. [9] also showed that HD patients have a higher incidence of herpes than the general population. The incidence of herpes zoster in the HD patients
examined by Kuo et al. [9] was 73.34 per 1,000 person-years, which is higher than the incidence in our HD group, which was 17 per 1,000 person-years. The reason might result from the different study designs. Kuo et al. [9] initially excluded all HD patients who would receive RT or PD later, but we followed up these HD patients
until the date of developing herpes zoster, shifting to PD, or receiving RT. Thus, the value of calculated follow-up person-years in our study would be larger and the calculated incidence would be lower but more accurate than
that of Kuo et al. Despite adjusting for several confounders contributing to herpes zoster, the risks of acquiring
herpes zoster were still significantly high in ESRD patients in these two studies. Therefore, we suppose that
the uremic status causes both impaired cellular and humoral immunity, and might account for increasing rates
of herpes.
It is interesting that our study reveals that the PD group has the higher risk of developing herpes or herpes complications than the HD group, which has never been reported before. Previous studies showed that the higher-risk groups for herpes or post-herpetic neuralgia are those aged 660 years with diabetes, leukemia/lymphoma, renal failure, SLE, and transplant recipients [7¡V9, 26,
27]. Age is recognized as an important risk factor for herpes zoster [2, 28]. While the PD groups are younger than
patients having a higher risk of herpes zoster than HD patients. One potential explanation might be associated
with the influence of the dialysis process of PD on immunity as a whole. Several studies have demonstrated
that PD patients might lose macrophages and immunoglobulin into the dialysate effluent, which could alter
their humoral immunity [29, 30]. The effect of HD on immunity status is under ongoing investigation [23, 31].
Since the decrease in VZV-specific T cells is associated with a risk of herpes [32, 33], we suggest that PD patients have more impaired VZV-specific cell-mediated immune
functioning than HD patients.
Herpes zoster and associated complications also represent higher medical costs [34, 35]. Recently, a live attenuated zoster vaccine has been documented to markedly
decrease the morbidity and mortality in immunocompetent elderly [36]. In the case of renal failure patients, varicella vaccine is only routinely recommended for
transplant candidates [37]. The varicella vaccine is reported to be safe and efficacious for ESRD children [38].
We propose a need for further research that the varicella vaccine might decrease relapses of herpes zoster as well as associated complications and medical costs in ESRD adults, especially those who are elderly and on PD.
Our study has several strengths. It is the first population-based study comparing the risks of herpes zoster in
populations with different renal status. Using a large population database with comprehensive electronic medical
records provided complete information on the incidence of herpes zoster and associated complications categorized according to age, gender, and dialysis modality.
However, the study has several limitations: the diagnosis of herpes zoster might be miscoded or dismissed; the patients might have used over-the-counter medications,
and most importantly, the patients could have received
These limitations would lead to an underestimation
of the incidence of herpes zoster and its complications. Finally, an additional limitation is that we did not have precise information on types of artificial kidneys, residual renal function, dialysis efficiency or the levels of albumin, all of which might affect the immune response to
herpes. However, since these factors have not been proved to have a strong impact on the immunity of the host, the
possible bias of these factors in our results might be prevented.
In conclusion, our study demonstrates that different
renal status is associated with different risks of herpes zoster attacks in Taiwan. RT patients had the highest risk of developing herpes zoster and its complications. PD patients had a higher risk of developing herpes zoster and
its complications than HD patients. Future studies are needed to investigate the possible mechanism accounting
for the different clinical manifestations of adaptive immunity among ESRD patients receiving RT, PD, and HD.
Disclosure Statement
The authors declare no conflicts of interest.
Am J Nephrol 2012;36:27¡V33 Lin /Liu /Lin /Tsai /Chen /Chung /Liu /
References
1 Wareham DW, Breuer J: Herpes zoster. BMJ 2007; 334: 1211¡V1215.
2 Schmader K: Herpes zoster in older adults. Clin Infect Dis 2001; 32: 1481¡V1486.
3 Thomas SL, Hall AJ: What does epidemiology tell us about risk factors for herpes zoster. Lancet Infect Dis 2004; 4: 26¡V33.
4 Thomas S, Wheeler J, Hall AJ: Case-control study of the effect of mechanical trauma on the risk of herpes zoster. BMJ 2004; 328: 439¡V 440.
5 Schmader KE, Dworkin RH: Natural history and treatment of herpes zoster. J Pain 2008; 9: 3¡V9.
6 Kato S, Chmielewski M, Honda H, Pecoits-Filho R, Matsuo S, Yuzawa Y, Tranaeus A, Stenvinkel P, Lindholm B: Aspects of immune dysfunction in end-stage renal disease. Clin J Am Soc Nephrol 2008; 3: 1526¡V 1533.
7 Sato T, Inoue T, Endo K, Watanabe Y, Kikuta T, Tsuda M, Arai J, Kobayashi K, Ikeda N, Ohno Y: End-stage renal disease (ESRD)
contributes to the increasing prevalence of herpes zoster. NDT Plus 2009; 2: 263¡V264. 8 Wung PK, Holbrook JT, Hoffman GS, Tibbs AK, Specks U, Min YI, Merkel PA, Spiera R,
Davis JC, St Clair EW: Herpes zoster in immunocompromised patients: incidence, timing,
1416¡V1418.
9 Kuo CC, Lee CT, Lee IM, Ho SC, Yang CY:
Risk of herpes zoster in patients treated with long-term hemodialysis: a matched cohort
study. Am J Kidney Dis 2012; 59: 428¡V33. 10
Miller G, Dummer J: Herpes simplex and
varicella zoster viruses: forgotten but not gone. Am J Transplant 2007; 7: 741¡V747. 11
Lin SY, Liu JH, Lin CC, Wang SM, Tsai CA, Chou CY, Kuo HL, Wang IK, Lin HH, Huang
CC: Comparison of hepatitis B surface antibody decay rates after vaccination between
hemodialysis and peritoneal dialysis patients. Vaccine 2011; 29: 3738¡V3741.
12
Cheng TM: Taiwan¡¦s national health insurance system: high value for the dollar; in
Okma KGH, Crivelli L (eds): Six Countries, Six Reform Models: The Healthcare Reform, Experience of Israel, the Netherlands, New Zealand, Singapore, Switzerland and Taiwan. Hackensack, NJ, World Scientific,
2009, pp 171¡V204. 13
Gau CS, Chang IS, Lin Wu FL, Yu HT, Huang YW, Chi CL, Chien SY, Lin KM, Liu MY,
Wang HP: Usage of the claim database of national health insurance programme for analysis
of cisapride-erythromycin co-medication in Taiwan. Pharmacoepidemiol Drug
14
Liu CY, Hung YT, Chuang YL, Chen YJ, Weng WS, Liu JS, Liang KY: Incorporating
development stratification of Taiwan townships into sampling design of large scale
health interview survey. J Health Manag 2006; 4: 1¡V22.
15
Taylor AL, Watson CJE, Bradley JA: Immunosuppressive agents in solid organ transplantation:
mechanisms of action and therapeutic efficacy. Crit Rev Oncol Hematol 2005; 56: 23¡V46.
16
Lauzurica R, Bayes B, Frias C, Fontsere N, Hernandez A, Matas C, Jimenez A, Matas C, Jimenez A, Bonet J, Romero R: Disseminated varicella infection in adult renal allograft recipients: role of mycophenolate mofetil. Transplant Proc 2003; 35: 1738¡V1759.
17
Rothwell WS, Gloor JM, Morgenstern BZ,
Milliner DS: Disseminated varicella infection in pediatric renal transplant recipients
treated with mycophenolate mofetil. Transplantation 1999; 68: 158¡V161.
18
Pandya A, Wasfy S, Hebert D, Allen UD.
Varicella-zoster infection in pediatric solid-organ transplant recipients: a hospital-based study in the prevaricella vaccine era. Pediatr Transplantation 2001: 5:153¡V159.
19
Kotton CN, Fishman JA: Viral infection in the renal transplant recipient. J Am Soc Nephrol 2005; 16: 1758¡V1774.
20 Hesselink DA, Betjes MG, Verkade MA, Athanassopoulos P, Baan CC, Weimar W:
The effects of chronic kidney disease and renal replacement therapy on circulating dendritic cells. Nephrol Dial Transplant 2005;
20: 1868¡V1873. 21
Litjens NHR, van Druningen CJ, Betjes
MGH: Progressive loss of renal function is associated with activation and depletion of naive T lymphocytes. Clin Immunol 2006; 118: 83¡V91.
22 Hauser AB, Stinghen AE, Kato S, Bucharles
S, Aita C, Yuzawa Y, Pecoits-Filho R: Characteristics and causes of immune dysfunction
related to uremia and dialysis. Perit Dial Int 2008; 28(suppl 3):S183¡VS187.
23 Eleftheriadis T, Antoniadi G, Liakopoulos V,
Kartsios C, Stefanidis I: Basic science and dialysis: disturbances of acquired immunity in
hemodialysis patients. Semin Dial 2007; 20: 440¡V451.
24 Girndt M, Sester M, Sester U, Kaul H, Kohler H: Molecular aspects of T- and B-cell function in uremia. Kidney Int 2011; 59:S206¡V
S211.
25 Smetana Z, Leventon-Kriss S, Broide A, Jedwab M, Smetana SS: Varicella-zoster virus
immune status in CAPD and chronic hemodialysis patients. Am J Nephrol 1991; 11: 229¡V
236.
26 Jih JS, Chen YJ, Lin MW, Chen YC, Chen TJ, Huang YL, Chen CC, Lee DD, Chang YT,
Wang WJ, Liu HN: Epidemiological features
and costs of herpes zoster in Taiwan: a national study 2000 to 2006. Acta Derm Venereol
2009; 89: 612¡V616.
27 Arness T, Pedersen R, Dierkhising R, Kremers W, Patel R: Varicella zoster virus associated disease in adult kidney transplant recipients: incidence and risk factor analysis.
Trans Infect Dis 2008; 10: 260¡V268.
28 Arivn A: Aging, immunity, and the varicella-zoster virus. N Eng J Med 2005; 352: 2266¡V 2267.
29 Boesken WH, Schuppe HC, Seidler A: Peritoneal membrane permeability for high and
low molecular weight proteins under CAPD. Perit Dial Bull 1984; 4(suppl):7 (abstract). 30 Bouts AH, Davin JC, Krediet RT, van der Weel MB, Schroder CH, Monnens L, Nauta
J, Out TA: Immunoglobulins in chronic renal failure of childhood: effects of dialysis modalities. Kidney Int 2000; 58: 629¡V637. 31 Pertosa G, Grandaliano G, Gesualdo L, Schena FP: Clinical relevance of cytokine production in hemodialysis. Kidney Int 2000; 58:S104¡VS111.
Levin MJ, Smith JG, Kaufhold RM, Barber D, Hayward AR, Chan CY, Chan IS, Li DJ,
Wang W, Keller PM, Shaw A, Silber JL,
Schlienger K, Chalikonda I, Vessey SJ, Caul-field MJ: Decline in varicella-zoster virus (VZV)-specific cell-mediated immunity
with increasing age and boosting with a high-dose VZV vaccine. J Infect Dis 2003; 188: 1336¡V1344.
33
Castle SC: Clinical relevance of age-related immune dysfunction. Clin Infect Dis 2000; 31: 578¡V585.
34 Vossen MT, Gent MR, Weel JF, de Jong MD, van Lier RA, Kuijpers TW: Development of virus-specific CD4+ T cells on reexposure to varicella-zoster virus. J Infect Dis 2004; 190: 72¡V82.
35
Yawn BP, Itzler RF, Wollan PC, Pellissier JM, Sy LS, Saddier P: Health care utilization and cost burden of herpes zoster in a community population. Mayo Clin Proc 2009; 84: 787¡V794. 36
Oxman MN, Levin MJ, Johnson GR, Schmader
KE, Straus SE, Gelb LD, Arbeit RD, Simberkoff MS, Gershon AA, Davis LE, Weinberg
A, Boardman KD, Williams HM, Zhang JH,
Peduzzi PN, Beisel CE, Morrison VA, Guatelli JC, Brooks PA, Kauffman CA, Pachucki CT, Neuzil KM, Betts RF, Wright PF, Griffin MR, Brunell P, Soto NE, Marques AR, Keay SK, Goodman RP, Cotton DJ, Gnann JW Jr, Lout-it J, Holodniy M, KeLout-itel WA, Crawford GE,
Yeh SS, Lobo Z, Toney JF, Greenberg RN, Keller PM, Harbecke R, Hayward AR, Irwin MR, Kyriakides TC, Chan CY, Chan IS, Wang
WW, Annunziato PW, Silber JL; Shingles Prevention Study Group: A vaccine to prevent
herpes zoster and postherpetic neuralgia in older adults. NEJM 2005; 352: 2271¡V2284. 37
Dinits-Pensy M, Forrest GN, Cross AS, Hise MK: The use of vaccines in adult patients with renal disease. Am J Kidney Dis 2005; 46: 997¡V1011.
38 Furth SL, Hogg RJ, Tarver J, Moulton LH,
Chan C, Fivush BA; Southwest Pediatric Nephrology Study Group: Varicella vaccination
in children with chronic renal failure. A report of the Southwest Pediatric Nephrology
Study Group. Pediatr Nephrol 2003; 18: 33¡V 38.
Risk of Herpes Zoster among Renal Am J Nephrol 2012;36:27¡V33 Patients