Willingness to pay for drug abuse treatment: Results from a
contingent valuation study in Taiwan
Chao-Hsiun Tang
a,∗, Jin-Tan Liu
b, Ching-Wen Chang
c, Wen-Ying Chang
d aSchool of Health Care Administration, Taipei Medical University, 250 Wu-Xing Street, Taipei 110, TaiwanbDepartment of Economics, National Taiwan University, Taipei, Taiwan
cGraduate Institute of Injury Prevention and Control, Taipei Medical University, Taipei, Taiwan dGraduate Institute of Nursing, Taipei Medical University, Taipei, Taiwan
Abstract
Objective: In this study, we attempted to describe and justify the use of a contingent valuation (CV) method to elicit the
willingness to pay (WTP) for a drug abuse treatment program by the general public in Taiwan.
Method: In total, 1817 CV survey questionnaires were conducted through telephone interviews from randomly dialed numbers.
Subjects were members of the general public aged between 20 and 65 years, with full-time jobs, and residing in the three major Taiwanese cities of Taipei, Taichung, and Kaohsiung. Respondents’ WTP for drug treatment programs was elicited for two different financing mechanisms: payment through ‘compulsory’ payroll tax/health insurance premiums, and through ‘voluntary’ donations. The WTP was modeled as a function of scenarios and policies of the treatment program, respondents’ socio-demographic information, and their responses to knowledge and attitudes questions.
Results: The general public in Taiwan was estimated to be willing to pay between NT$81.00 and NT$95.00 per month for a
drug abuse treatment program, while the benefits of drug abuse treatment were estimated to range between NT$12.8 billion and NT$15.0 billion in 2004 (US$1 = NT$31.9 in 2004), which was equal to around 0.15% of Taiwan’s GDP for that year. The general public in Taiwan was more willing to pay for drug abuse treatment via increases in NHI premiums than via donations. Preferences for the drug abuse treatment program were also found to be sensitive to the target treated population as well as the sequence in which the WTP questions were asked.
Conclusions: Results of this study provide policymakers with important evidence on the monetary value of a substance abuse
treatment program, allocation of healthcare resources, and a possible financing mechanism of the treatment program, which may be justified by knowledge of the WTP of the general public. This study has also advanced the knowledge of the methodological issues with regard to CV questionnaire design, and it provides a base case for further studies on drug abuse in Taiwan. © 2006 Elsevier Ireland Ltd. All rights reserved.
Keywords: Willingness to pay; Contingent valuation methods; Substance abuse; Economic evaluation; Health care financing; National Health Insurance; Taiwan
∗Corresponding author. Tel.: +886 2 23785339; fax: +886 2 23789788.
E-mail address:[email protected](C.-H. Tang).
0168-8510/$ – see front matter © 2006 Elsevier Ireland Ltd. All rights reserved. doi:10.1016/j.healthpol.2006.09.007
1. Introduction
The widespread use of drugs is often perceived as an ‘epidemic’ affecting both developed and developing countries alike. According to estimates by the United Nations Drug Control Program (UNDCP), there were approximately 185 million drug users worldwide (or 3% of the world’s population) in 1994, and the number is steadily rising[1].
Furthermore, over the past two decades or so, coun-tries all over the world have seen this devastating addiction inflict tremendous harm on younger elements of society, with drug-related suicides, accidents, and absenteeism rising at alarming rates among teenagers and adolescents. A conservative estimate of the num-ber of drug abusers in Taiwan in 2000 indicated that in excess of 400,000 of the island’s population of 21 mil-lion were affected, with 60% of these being juveniles under the age of 18[2].
Individuals who receive drug-abuse treatment invariably reduce their frequency of drug use, which in turn, reduces the incidence of drug-related risk behav-iors, thereby lowering the risk of contracting infectious diseases such as AIDS, hepatitis B, and hepatitis C through the use of contaminated needles. Treatment of drug abuse also improves overall health, social functioning, and work productivity, and effectively lowers the probability of relapse. When drug users undergo successful treatment, the quality of life within the community as a whole is also improved through a reduction in crime and greatly enhanced personal security.
According to the experiences of many developed countries, as a direct result of the enactment of drug-related legislation, which began in the 1960s, the use of drugs and subsequent drug dependence have become acknowledged as a chronic form of mental illness, with medical intervention now being deemed necessary to alleviate the burden of the disease. One earlier study in particular showed that reliance solely on law enforce-ment as a means of combating drug abuse is neither a sufficient nor a strategic measure[3], and in Taiwan, prior to the amendment of the Anti-Drug and Preven-tion Act, which was promulgated in May 1998, drug use had been regarded as a criminal behavior, resulting in major penal consequences for drug users, but with no subsequent educational, treatment, or rehabilitation intervention being provided.
Earlier in 1995, when the National Health Insurance (NHI) program was about to be implemented, drug abuse was still regarded as criminal behavior; there-fore, treatment for drug abuse was excluded from the package of benefits at the time of the introduction of the NHI program, and has still not been included. Con-sequently, despite the fact that drug abuse treatment is inexpensive, most addicts do not receive the necessary treatment, and it is therefore necessary for them to seek help from their families instead, who must then bear the brunt of their current untreated condition and the asso-ciated disabilities. However, over recent years, it has become clear that more philanthropic donors are now coming forward to provide support for drug abuse pro-grams, and indeed, public health professionals and pol-icymakers alike are now taking a much greater interest in issues arising from drug abuse. Despite this, how-ever, reform is still very slow, and drug abuse remains at the bottom of most policymakers’ agenda.
Most prior studies examined the economic costs of substance abuse to society by summing up the costs associated with medical care, reduced productivity, and law enforcement[4–7]. In addition to these costs, how-ever, drug abuse also causes pain and suffering both to the patients themselves, and to their families, as well as considerable anxiety for society as a whole, given the threat to security associated with drug-related crime. Nevertheless, relatively little information has been col-lected with regard to the intangible costs of drug abuse borne by patients, families, victims, and the general public.
When attempting to assign specific values to the benefits of an intervention, one of the more-encompassing approaches used is ‘willingness to pay’ (WTP). The ‘contingent valuation’ (CV) method, in the form of the assessment of a person’s WTP, seeks to elicit the value that people attach to various forms of healthcare intervention by asking them how much they would be prepared to pay to obtain the benefits of the intervention. The CV methods have been extensively applied in the evaluation of various healthcare inter-ventions[8–15], as well as the evaluation of the WTP for health insurance and the optimal size of the health care budget[16–18]. The method has also been used to evaluate the WTP for altruistic reasons among the general public, with those indicating their WTP being aware that some public goods may become available to those in need of it[11,19–21]. There are, however,
some concerns regarding the reliability and validity of CV assessments as measures of societal values[22–24]. Methodological issues have been discussed in many studies, including issues of sensitivity to questionnaire formats[8,14,25,26], scope effects, and the effects of question order[27–29]. Those studies highlighted the importance of careful study design and the adoption of appropriate methods of analysis when attempting to apply CV methods to public policy.
In the present study, we set out to describe the use of a CV survey to characterize the preferences of members of the general public who are not themselves involved in drug abuse. In our study, we tried to determine how much the general public was willing to pay for treat-ment that would be available either to themselves and their families (a self-interest motive) or to others (an altruistic motive). Our aim was to better understand the potential value of drug abuse treatment programs for the general public, and to examine the differen-tial effects of financing through ‘compulsory’ payroll tax/health insurance premiums or ‘voluntary’ dona-tions (payment vehicle effect). We also attempted to test whether such preferences revealed by a CV survey are sensitive to scenarios and policies of the program, such as the number of patients treated (scope effect), the treated target population (target population effect), the background information provided (information effect), or the sequence in which the questions are asked (ques-tion order effect).
2. Methods
2.1. Study setting and sampling
The survey was conducted by a professional survey company (Taiwan Marketing Research, Taipei, Tai-wan), in September and October 2004 using telephone interviews conducted through random-digit dialing as a means of sampling members of the general public aged between 20 and 65 years, with full-time jobs, and residing in the three major Taiwanese cities of Taipei, Taichung and Kaohsiung. Of the 5358 phone numbers successfully called, 2216 family members of eligible respondents refused to allow them to participate; 1325 calls successfully contacted eligible respondents but they refused to participate, and 1817 interviews were successfully completed. The response rate was 58%.
Given the populations of the three cities, the sample dis-tributions were quite even, with 40% residing in Taipei City, 31% in Taichung City, and 29% in Kaohsiung City.
2.2. Measurement of the WTP
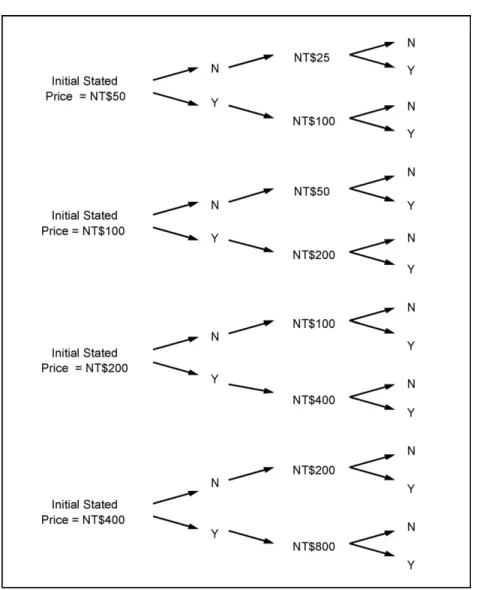
The WTP for substance abuse treatment was elicited using the CV method, including double-bounded binary-choice questions. Each respondent was randomly assigned one of the four starting values of NT$50, NT$100, NT$200, and NT$400 (US$1 = NT$31.9 in 2004). The starting values were guided by the expected costs of reimbursement for sub-stance abuse treatment within the NHI program, along with the results of a pilot CV survey.
If a respondent’s answer to the first bid offered was ‘yes’, the interviewer then doubled the bid and asked the same WTP question again. If the initial answer was ‘no’, the interviewer then reduced the bidding price by half and continued by asking the same question again (Fig. 1); this procedure resulted in WTP values being provided at intervals between the ‘yes’ and ‘no’ responses in the double-bounded questions.
Those cases where the respondent’s subsequent answer was ‘yes’ to the double-bounded question resulted in the WTP value being provided as the interval between the final ‘yes’ response and infinity; similarly, those cases where the respondent’s subsequent answer was ‘no’ to the double-bounded question resulted in the WTP value being provided as the interval between 0 and the final ‘no’ response.
Respondents were asked two valuation questions: whether the respondent would be willing to pay by means of a ‘compulsory’ payment method (i.e., through increased monthly insurance premiums), or whether the respondent would be willing to pay by means of a ‘voluntary’ mechanism (through monthly donations). The 1817 respondents provided 3634 responses which we then analyzed.
In addition, two sets of policy versions were designed to test the sensitivity of the elicited WTP to the scope and target of the benefits. The number of treated patients was described as either 5000 or 1000 patients, with the target patients being either young drug users (under the age of 20) or all users (regardless of age).
Moreover, two scenarios were also designed to test the information and sequence effects. The respondents
Fig. 1. Bidding process of the contingent valuation method.
were randomly assigned to answer either the first ques-tion (on whether they would be willing to pay for substance abuse treatment through NHI insurance pre-miums) followed by the second question (on their WTP through donations), or vice versa (answering the sec-ond question on WTP through donations, followed by the first question on WTP through insurance premi-ums). The respondents were also randomly assigned to answering the questions after having been provided with the background information regarding substance abuse, or answering the questions without any prior
background information having been provided. Alto-gether, there were 16 combinations of scenarios and policies, each of which was administered randomly to a different population subsample.
2.3. Statistical analyses
Since the outcome measures (the WTP values) were interval-censored and the distribution was skewed to the right, the log-normal model in the survival analysis was estimated using the maximum-likelihood method.
In this log-linear specification, the expected WTP given fixed covariates is dependent on the scale parameter, whereas changes in the scale parameter merely com-press (if the scale term is <1) or stretch (if the scale term is >1) the probability density function of the WTP.
The logarithm of the WTP was assumed to be nor-mally distributed with a mean comprising a linear func-tion of the payment method, scope and magnitude of the benefits, the sequence of the questions, whether background information was provided, and individual characteristics. The (predicted) median WTP was cal-culated at the sample mean to represent the value placed on drug abuse treatment among the sample population. All analyses were carried out using PROC LIFEREG in the SAS/Stats software program package, Version 8.02 (SAS Institute, Cary, NC).
3. Results
3.1. Sample characteristics
The summary statistics and definitions of the vari-ables are given inTable 1, where it is shown that the sample was broadly representative of the non-elderly working-aged population residing in urban areas of Taiwan. More than half of the respondents had good knowledge of substance abuse; and indeed, fewer than 1% of all respondents had poor knowledge of the sub-ject. Around 90% of all respondents either ‘agreed’ or ‘strongly agreed’ that the drug abuse problem in Tai-wan is serious, while more than 90% either ‘agreed’ or ‘strongly agreed’ that drug abuse was the main rea-son for the deterioration in public safety, and that they would personally advise their family, friends, or work colleagues to seek treatment if they had any form of a substance abuse problem. About 80% of all respon-dents either ‘agreed’ or ‘strongly agreed’ that substance abuse was a chronic disease which can possibly be cured through proper treatment.
About 70% of the respondents were married; the balance, in terms of gender, was 48% male and 52% female; the mean age was 39.28 years; more than 60% of all respondents were educated to college level or higher; the average monthly household income was NT$36,316 (US$1 = NT$31.9 in 2004); and about 60% of the respondents expressed some form of religious belief. About 17% of respondents had children in the
0–6-year age group, 22% of respondents had children in the 7–12-year age group, 23% of respondents had children in the 13–19-year age group, and 26% of respondents had children in the≥20-year age group. Over half of all respondents (54.93%) considered them-selves to be healthy.
3.2. Willingness to pay
The details of the initial bids and the respective num-bers (and percentages) of respondents indicating that they would be willing to pay for substance abuse treat-ment in the initial question are provided in Table 2. Generally speaking, those respondents with a higher bidding start point for the WTP amount indicated that they were likely to pay less, irrespective of the payment method proposed; however, the respondents were more price sensitive with regard to paying through insurance premiums than through donations.
For the lowest price (NT$50), the proportions of respondents willing to pay were 57.08% for payment through insurance premiums and 55.97% for payment through donations, which were similar for both pay-ment methods. With a rise in the stated price, although there was a corresponding and significant fall in the pro-portion of respondents willing to pay through insurance premiums, there was little change in the proportion of respondents willing to pay through donations. Further-more, while there was a 21.05% difference between the proportion of respondents willing to pay through insurance premiums at the highest (NT$400) and low-est (NT$50) bidding prices, the difference was only 7.18% between the two stated prices with regard to payment through donations. It appears that the starting bids in this study were not able to capture the extremes at either end, especially in the case of willingness to pay through donations.
3.3. Factors predicting the WTP
Table 3presents the results of the multivariate anal-ysis on the prediction of WTP values, with three regres-sion models having been estimated. Model 1 (the sim-plest model) includes only the dummy variables char-acterizing the effects of the payment method, as well as the sensitivity of the WTP elicited from the respon-dents, with regard to the scope and target of the ben-efits, order effect, and information effect; in addition,
Table 1
Definitions of variables and descriptive statistics
Variable Definition Mean S.D.
Insurance premium Dummy = 1 if payment is made through compulsory health insurance premiums; 0 if payment is made through voluntary donations
0.50 0.50
No. of drug users treated Dummy = 1 if 5000 patients are treated each year; 0 if 1000 patents are treated each year
0.51 0.50
Targeting youth Dummy = 1 if targeting young users under 20 years old; 0 if targeting all drug users regardless of age
0.50 0.50
Question order Dummy = 1 if the questions on payment through insurance premiums was asked first; 0 if the question on payment through donations was asked first
0.53 0.50
Information provided Dummy = 1 if background of the treatment plan was addressed; 0 otherwise 0.53 0.50 High knowledge Dummy = 1 if score on knowledge of substance abuse was 4 or 5; 0 if score
was 0 or 1
0.51 0.50
Medium knowledge Dummy = 1 if score on knowledge of substance abuse was 2 or 3; 0 if score was 0 or 1
0.45 0.50
Community security Dummy = 1 if respondent agrees or strongly agrees that drug abuse is the main reason for worsening community security; 0 if they don’t know, disagree, or strongly disagree
0.95 0.22
Seriousness of drug abuse Dummy = 1 if respondent agrees or strongly agrees that drug abuse in Taiwan is serious; 0 if they do not know, disagree, or strongly disagree
0.89 0.32
Treatment of drug abuse Dummy = 1 if respondent agrees or strongly agrees that drug abuse is a type of chronic disease and may be cured through proper treatment; 0 if they do not know, disagree, or strongly disagree
0.79 0.41
Medical assistance Dummy = 1 if respondent agrees or strongly agrees that if their family or colleagues had a drug abuse problem, they would advise and assist them to obtain proper treatment; 0 if they do not know, disagree, or strongly disagree
0.92 0.28
Health status Dummy = 1 if respondent’s perceived health status is good or excellent; 0 if they don’t know, or it is so-so, not good, or very bad
0.23 0.42
Age Respondent’s age (in years: between 20 and 65 years) 39.28 10.25
Male Dummy = 1 if respondent is male; 0 otherwise 0.48 0.50
Elementary Dummy = 1 if respondent’s highest education is primary school; 0 if it is senior high school
0.04 0.19
Junior high Dummy = 1 if respondent’s highest education is junior high school; 0.06 0.25 0 if it is senior high school.
College Dummy = 1 if respondent’s highest education is college or vocational school; 0 if it is senior high school.
0.26 0.44
University Dummy = 1 if respondent’s highest education is university; 0 if it is senior high school
0.29 0.45
Postgraduate Dummy = 1 if respondent’s highest education is postgraduate or higher; 0 if it is senior high school.
0.07 0.25
Married Dummy = 1 if respondent is married; 0 otherwise 0.69 0.46
Children 0–6 years old Dummy = 1 if respondent has children aged 0–6 years; 0 otherwise 0.17 0.38 Children 7–12 years old Dummy = 1 if respondent has children aged 7–12 years; 0.22 0.41
0 otherwise
Children 13–19 years old Dummy = 1 if respondent has children aged 13–19 years; 0 otherwise 0.23 0.42 Children≥20 years Dummy = 1 if respondent has children aged≥20 years; 0 otherwise 0.26 0.44 Religion Dummy = 1 if respondent has religious beliefs; 0 otherwise 0.59 0.49
Log (income) Log of monthly wage income (in NT$) 10.50 0.56
Taipei Dummy = 1 if the respondent lives in Taipei City; 0 if the respondent lives in Taichung
0.40 0.49
Kaohsiung Dummy = 1 if the respondent lives in Kaohsiung City; 0 if the respondent lives in Taichung City
0.29 0.45
Table 2
Willingness to pay by the general public on the first bid Willingness to pay Starting point
NT$50 NT$100 NT$200 NT$400 Total
No. % No. % No. % No. %
Payment through insurance premiums
Not willing to pay 194 42.92 235 52.46 283 61.66 293 63.97 1005
Willing to pay 258 57.08 213 47.54 176 38.34 165 36.03 812
Payment through donations
Not willing to pay 199 44.03 212 45.30 243 54.73 232 51.21 886
Willing to pay 253 55.97 256 54.70 201 45.27 221 48.79 931
Note: Total sample number = 3634.
model 2 includes the knowledge and attitudes of indi-viduals towards drug abuse and drug abuse treatment; and additionally, model 3 includes socioeconomic variables.
Aggregating across models, the estimated values of the coefficients on both scenarios and policy instru-ments were quite similar, since all of the coefficients on insurance premiums were positive and significantly differed from 0 at the 1% level, and all of the coeffi-cients on 5000 drug users treated and targeting youth were positive; however, only the coefficients for tar-geting youth significantly differed from 0 at the 5% significance level.
Question order effects were found to exist in this study, since the WTP was significantly higher at the 1% significance level if the question on payment through insurance premiums was asked first. The WTP was also higher if background information on substance abuse was provided at the beginning of the interview; how-ever, the coefficient on information provided did not achieve significance.
The estimated coefficients of the knowledge and attitude variables appeared to be both reasonable and consistent across the specifications of models 2 and 3. Those respondents with high and medium knowl-edge levels about substance abuse were willing to pay higher amounts than those with lower knowledge. The willingness to pay a higher price for substance abuse treatment was greatest among those who either ‘agreed’ or ‘strongly agreed’ (i) that substance abuse was the main reason for the deterioration in community safety; (ii) that substance abuse was very serious in Taiwan; (iii) that substance abuse was a chronic disease which can be cured by proper treatment; and (iv) that they
would advise their family, friends, or work colleagues to seek medical assistance if they had problems with substance abuse.
The evidence for the socio-demographic charac-teristics also appears reasonable and consistent with our expectations. The effect of household income was positive and highly significant. The estimated income elasticity was 0.16. Respondents with children aged 13–19 years were willing to pay more than those whose children were not in this age group. The WTP was significantly higher for respondents who held religious beliefs. Furthermore, the willingness to pay was higher for respondents residing in Kaohsiung than for those residing in either Taipei or Taichung. Coefficients of educational level were not consistently significant in explaining the WTP, and the direction was not in line with our expectations either; those respondents whose highest education level was elementary school had the highest willingness to pay, while those respondents whose highest education level was college had the lowest willingness to pay. Collinearity of educational level with income and age might have been the cause of instability in the coefficients of educational level.
The results inTable 3also show that the scale esti-mates ranged from 1.71 to 1.80, which indicates that the probability density function of the WTP was heav-ily skewed to the right.
4. Discussion
Unlike most diseases, drug abuse not only has direct effects on patients and their families, but it also places
Table 3
Regression analysis (survival analysis) of the WTP of the general publica,b
Variable Regression modelc
(1) (2) (3)
Coefficient t-Ratio Coefficient t-Ratio Coefficient t-Ratio
Intercept 4.12 50.18*** 1.88 7.37*** −0.34 0.46
Insurance premiums 0.36 5.40*** 0.36 5.58*** 0.36 5.63***
5000 drug users treated 0.03 0.47 0.05 0.73 0.04 0.66
Targeting youth 0.16 2.33** 0.16 2.40** 0.16 2.44** Information provided 0.03 0.51 0.02 0.30 0.01 0.10 Question order 0.20 3.00*** 0.18 2.79*** 0.17 2.66*** High knowledge – – 0.40 2.13** 0.44 2.39** Medium knowledge – – 0.37 1.99** 0.48 2.54** Community security – – 0.27 1.84* 0.22 1.50
Seriousness of drug abuse – – 0.22 2.05** 0.17 1.61
Treatment of drug abuse – – 0.40 4.80*** 0.43 5.09***
Medical assistance – – 0.58 4.58*** 0.61 4.84*** Health status – – – – −0.10 1.28 Age – – – – 0.0023 0.41 Male – – – – 0.11 1.40 Elementary – – – – 0.27 1.82* Junior high – – – – −0.02 0.20 College – – – – −0.18 1.95* University – – – – −0.07 0.44 Postgraduate – – – – −0.01 0.10 Married – – – – −0.10 1.28
Children 0–6 years old – – – – −0.04 0.42
Children 7–12 years old – – – – 0.05 0.53
Children 13–19 years old – – – – 0.15 1.72*
Children≥20 years – – – – 0.13 1.20 Religion – – – – 0.18 2.57** Log (income) – – – – 0.16 2.36** Taipei – – – – 0.04 0.52 Kaohsiung – – – – 0.24 2.79*** Scale 1.80 1.73 1.71 Log likelihood −4548.21 −4429.50 −4399.12 WTP, median (NT$) 81 90 93
aTotal sample number = 3634.
b *Indicates that the estimated coefficient significantly differs from 0 at the 10% level;**indicates a significant difference from 0 at the 5%
level;***indicates a significant difference from 0 at the 1% level.
cModel 1 includes only the dummy variables characterizing the effect of the payment method, as well as the sensitivity of the WTP elicited
from the respondents on the scope and magnitude of the benefits, order effect, and information effect; in addition, model 2 includes the knowledge and attitudes of individuals towards drug abuse and drug abuse treatment; and additionally, model 3 includes socio-economic variables.
an enormous burden on society as a whole, largely because of the associated incidences of crime related to drugs. Patients consume more healthcare resources and have a higher potential for contagious diseases, such as AIDS, hepatitis B, and hepatitis C if they share injec-tion syringes. It has been estimated that the benefits of drug abuse treatment are equal to the cost savings asso-ciated with reduced crime and healthcare utilization
[30], which indicates that there are significant tangible and intangible benefits to be gained from drug abuse treatment through the direct effects on the reduced con-sumption of healthcare resources and indirect effects on reduced crime. Nevertheless, the NHI system in Taiwan does not provide coverage for drug abuse treatment, despite the fact that apart from the monetary burden that drug addiction creates, patients, their families, and
victims of drug-related crime invariably suffer some forms of physical and psychological pain.
Using the CV method, this paper has attempted to evaluate the willingness of the general public in Taiwan to pay for substance abuse treatment. From the results of the WTP regression analysis (Table 3), we estimated that the general public in Taiwan is willing to pay between NT$81.00 and NT$95.00 per month for the drug abuse treatment program. How-ever, it is worth noting that the WTP estimates in our study underestimated the WTP if it is for treat-ment for themselves or someone in their families. In a sense, it is the ‘willingness to fund’ rather than ‘willingness to pay’ that we estimated in this study. Multiplying the estimated WTP by the number of per-sons insured (13,163,135) in the NHI program in 2004 in Taiwan[31], the benefits for drug abuse treatment was estimated to range between NT$12.8 billion and NT$15.0 billion in 2004 (US$1 = NT$31.9 in 2004), which was equal to around 0.15% of Taiwan’s GDP for that year.
Similar to public policy arguments, we assumed that respondents were willing to pay for treatment either by way of voluntary donations or through an increase in payroll taxes/health insurance premiums in order to reduce the level of drug-related crime and improve the security of the community as a whole; therefore, each respondent was interviewed with regard to their WTP through insurance premiums or through dona-tions. This approach has the merit of capturing the externality of drug abuse treatment, which is often omitted by economic evaluation studies.
Previous studies demonstrated that WTP values placed on a commodity are sensitive to the payment vehicle employed in the WTP questions[32–34]. Gafni [35]argued that in a publicly financed healthcare sys-tem, the WTP for a therapy should be best assessed from an insurance perspective with the tax-paying general public as the relevant respondents. In addi-tion, paying via insurance premiums has an important advantage over alternative ‘voluntary’ mechanisms like donations, that of avoiding ‘free-riding’ behavior[36]. However, due to the non-transparent methods of financ-ing and budgetfinanc-ing within governments, people may be less willing to pay directly to the government, and may therefore be more willing to donate money directly to a specific non-governmental organization. Zarkin et al. [11]chose donation as the payment mechanism in their
study on the WTP for substance abuse treatment by arguing that respondents’ mistrust of the government to effectively spend the funds may have resulted in a large number of protest zero bids.
In this study, we simultaneously asked the gen-eral public about their WTP for drug abuse treatment through insurance premiums and donations. Our study found that the WTP was significantly higher by means of insurance premiums than by donations. A possible reason for this discrepancy is that since drug abuse is generally perceived as being related to criminal behav-ior and a hazard to community security, people in Taiwan may believe that it is the government’s respon-sibility to provide treatment for drug abuse patients so as to improve the general public safety by reducing drug-related criminal activities.
This study also examined the sequence effects with regard to the order of presentation of the questions on payment. Half of the respondents were first asked the question on whether they were willing to pay higher insurance premiums; they were then asked if they were willing to make payment through donations. The other half were asked the same two questions, but in reverse order. The results revealed that when respondents were first questioned about their WTP through increased insurance premiums, they were willing to pay a sig-nificantly higher amount for drug abuse treatment. We postulate that this is also due to respondents’ prefer-ence for financing substance abuse treatment programs via insurance premiums.
This study also analyzed the effects of scope and dif-ferences in age of the target group. Each respondent was asked to consider cases in which either 5000 or 1000 patients could be treated, since the hypothesis was that people would be willing to pay a higher amount if their contribution meant that more target patients were able to be treated; however, the results indicated that there was no significant difference in the willingness to pay for treating 5000 or 1000 patients. Given the question-naire design, we postulate that respondents in our study might not be aware of the scope effect, since they were only asked the question under a specific scenario—their willingness to pay for treating either 5000 or 1000 patients. As a result, the WTP the respondents revealed in this study simply showed their preference for drug abuse patients to be treated, regardless of the number of the patients to be treated. Nevertheless, our results do indicate that when the proposed age of the target
patients was below 20 years, respondents were more willing to pay for their treatment. It is surmised that the general public may believe that greater effective-ness can be achieved if drug users are treated as early as possible.
This study also attempted to analyze the infor-mation effect. Half of the respondents being inter-viewed were given no background information on drug abuse treatment, while the other half were pro-vided information on recent increases in overall drug abuse, as well as information on the effectiveness of treatment; however, the results of the responses from these two groups revealed no significant difference. One likely reason for this is that the general pubic may already have some awareness of drug abuse and drug-related crime as a result of the ubiquitous nature of information through the various media or through information available on the Internet. Since the sam-ple of respondents was drawn from the three major cities in Taiwan, there was a greater likelihood of these people being well informed about drug abuse in general.
Our study suffers from some limitations which should be considered. As a result of the research restric-tions and limited financial support, this study only used telephone interviews among a random sample of respondents over 20 years of age, with full-time jobs, and in one of the three major cities in Taiwan; how-ever, according to the CV methods guidelines provided by the US National Oceanic Atmospheric Administra-tion[37], face-to-face interviews are the preferred form of questioning. With better financial support, we hope that future studies may be able to extend this work to recruit a random sample representative of the Tai-wanese general population to conduct such face-to-face interviews.
Despite the aforementioned limitations, this study does provide policymakers with the latest survey infor-mation on the WTP by the general public for drug abuse treatment. The results demonstrate a consciousness among the general public with regard to the problem of drug abuse, as well as the intangible benefits of treat-ment, which include a reduction in the fear of criminal activity and an increase in well-being attributable to the knowledge that drug addicts are being treated.
These results also provide policymakers with impor-tant evidence on the monetary value of treatment, the allocation of healthcare resources, and a possible
financing mechanism of drug abuse treatment pro-grams, which may be justified by the knowledge of the WTP of the general public. We believe that this study has advanced our knowledge of the methodolog-ical issues with regard to WTP questionnaire design, and that it provides a base case for further studies on drug abuse in Taiwan.
Acknowledgments
The financial support (DOH93-NNB-1015) pro-vided by the National Bureau of Controlled Drugs at the Department of Health, Taiwan, for which we are extremely grateful, is duly acknowledged. We are also grateful to Prof. James K. Hammitt at Harvard School of Public Health, for his valuable comments on the design of the questionnaires for this study. Our special thanks also go to Prof. Jeff Richardson in the Faculty of Business and Economics at Monash University, Aus-tralia, for his comments on an earlier version of this paper, as well as to Professor Shu-Hui Chang at the Graduate Institute of Epidemiology, College of Public Health, National Taiwan University, for her comments on the statistical analysis used in this study.
Appendix A
Background information and questions on willing-ness to pay for drug abuse treatment.
The issue of drug abuse has become an increasingly serious problem in recent years. The main purpose of this study is to survey the opinions and attitudes of the general public towards the problem of drug abuse, and their willingness to pay for treating substance abusers. I am now going to ask you how much you would be willing to pay for treatment for those who suffer from problems associated with drug abuse Background informationa
It is estimated that more than 400,000 people have drug abuse problems in Taiwan, which means at least two in every 100 people are suffering from such problems. In addition, at least 6 of 10 drug addicts are under 18 years of age. Drug abuse not only causes physical and mental illnesses, but also brings into play other social problems such as unemployment, isolation from friends and family, and negative effects on a person’s self respect. Drug addicts may end up obtaining drugs through violent and illegal ways, such as stealing and robbing, thereby causing considerable problems for society
Appendix A (Continued )
Question 1b
If the program can treat (5000 or 1000)cpatients, would you be willing to pay (NT$50, NT$100, NT$150, or NT$200)d per month through insurance premiums for treating (all substance abuse patients or young patients under 20 years of age)e?
Question 2b
If the program can treat (5000 or 1000)cpatients, would
you be willing to pay (NT$50, NT$100, NT$150, or NT$200)dper month through donations for treating (all
substance abuse patients or young patients under 20 years of age)e?
aInformation effect: Half of the respondents were provided
back-ground information before being asked the WTP questions; the other half of the respondents were not provided the background informa-tion before being asked the WTP quesinforma-tions.
b Question order effect: Half of the respondents were asked
ques-tion 1 first, and then quesques-tion 2; the other half of respondents were asked question 2 first, and then question 1.
cScope effect. d Starting points. eTarget population effect.
References
[1] United Nations on Drugs and Crime. World Drug Report. New York: United Nations Office on Drugs and Crime (UN Publica-tion no. NCJ-E.04.XI.16); 2004.
[2] Ministry of Justice. Annual Anti-Drug Abuse Report. Taipei, Taiwan: Ministry of Justice; 2000.
[3] Nasir S. Combating drug abuse, law enforcement is necessary but not sufficient. The Jakarta Post; 2005.
[4] Xie X, Rehrn J, Single E, Robson L, Paul J. The economic costs of illicit drug use in Ontario, 1992. Health Economics 1998;7:81–5.
[5] Office of National Drug Control Policy. The Economic Costs of Drug Abuse in the United States, 1992–1998. Washington, DC: Office of National Drug Control Policy, Executive Office of the President (Publication no. NCJ-190636); 2001. [6] Mark TL, Woody GE, Juday T, Kleber HD. The economic costs
of heroin addiction in the United States. Drug Alcohol Depen-dence 2001;61:195–206.
[7] Garcia-Altes A, Olle JM, Antonanzas F, Colom J. The social cost of illegal drug consumption in Spain. Addiction 2000;97:1145–53.
[8] Johannesson M, Johansson PO, Kristrom B, Gerdtham UG. Willingness to pay for antihypertensive therapy—further report. Journal of Health Economics 1993;12:95–108.
[9] Lee SJ, Neumann PJ, Churchill WH, Cannon ME, Weinstein MC, Johannesson M. Patients’ willingness to pay for autologous blood donation. Health Policy 1997;40:1–12.
[10] Chiu L, Tang KY, Shyu WC, Chang TP. The willingness of families caring for victims of stroke to pay for in-home
respite care—results of a pilot study in Taiwan. Health Policy 1999;46:239–54.
[11] Zarkin GA, Cates SC, Bala MV. Estimating the willingness to pay for drug abuse treatment: a pilot study. Journal of Substance Abuse Treatment 2000;18:149–59.
[12] Wagner TH, Hu TW, Due˜nas GV, Kaplan CP, Nguyen BH, Pasick RJ. Does willingness to pay very by race/ethnicity? An analysis using mammography among low-income women. Health Policy 2001;58:275–88.
[13] Lenert LA. Use of willingness to pay to study values for pharmacotherapies for migraine headache. Medical Care 2003;41:299–308.
[14] Whynes DK, Frew E, Wolstenholme JL. A comparison of two methods for eliciting contingent valuations of colorectal cancer screening. Journal of Health Economics 2003;22:555–74. [15] Greenberg D, Bakhai A, Neumann PJ, Cohen DJ. Willingness
to pay for avoiding coronary restenosis and repeat revascular-ization: results from a contingent valuation study. Health Policy 2004;70:207–16.
[16] Eckerlund I, Johannesson M, Johansson PO, Tambour M, Zethraeus N. Value for money? A contingent valuation study of the optimal size of the Swedish health care budget. Health Policy 1995;34:135–43.
[17] Asenso-Okyere WK, Osei-Akoto I, Anum A, Appiah EN. Will-ingness to pay for health insurance in a developing economy. A pilot study of the informal sector of Ghana using contingent valuation. Health Policy 1997;42:223–37.
[18] Dong H, Kouyate B, Cairns J, Sauerborn R. Differential will-ingness of household heads to pay community-based health insurance premia for themselves and other household members. Health Policy and Planning 2004;19:120–6.
[19] Tohmo T. Economic value of a local museum: factors of will-ingness to pay. Journal of Socio-Economics 2004;33:229–40. [20] Gyrd-Hansen D, Slothuus U. The citizen’s preferences for
financing public health care: a Danish survey. International Jour-nal of Health Care Finance and Economics 2002;2:25–36. [21] Olsen JA, Donaldson C. Helicopters, hearts and hips: using
will-ingness to pay to set priorities for public sector health care programmes. Social Science and Medicine 1998;46:1–12. [22] Diener A, O’Brien B, Gafni A. Health care contingent
valua-tion studies: a review and classificavalua-tion of the literature. Health Economics 1998;7:313–26.
[23] Klose T. The contingent valuation method in health care. Health Policy 1999;47:97–123.
[24] Foreit JR, Fleischman Foreit KG. The reliability and validity of willingness to pay surveys for reproductive health pricing deci-sions in developing countries. Health Policy 2003;63:37–47. [25] Johannesson M, Jonsson B, Borgquist L. Willingness to pay
for antihypertensive therapy—results of a Swedish pilot study. Journal of Health Economics 1991;10:461–73.
[26] Frew EJ, Wolstenholme JL, Whynes DK. Comparing wiliness-to-pay: bidding game format versus open-ended and payment scale formats. Health Policy 2004;68:289–98.
[27] Kartman B, Stalhammar NO, Johannesson M. Valuation of health changes with the contingent valuation method: a test of scope and question order effects. Health Economics 1996;5:531–41.
[28] Federick S, Fischhoff B. Scope insensitivity in elicited valua-tions. Risk Decision Policy 1998;3:109–23.
[29] Norinder A, Hjalte K, Persson U. Scope and scale insensitivities in a contingent valuation study of risk reductions. Health Policy 2001;57:141–53.
[30] Gerstein DR, Johnson RA, Harwood HJ, et al. Evaluating recov-ery services: the California drug and alcohol treatment assess-ment (CALDATA) general report. California: Departassess-ment of Alcohol and Drug Problems; 1994.
[31] Bureau of National Health Insurance. Statistics of the National Health Insurance in 2004. Taipei, Taiwan: Bureau of National Health Insurance, Department of Health, Executive Yuan; 2004.
[32] Randall A, Grunewald O, Johnson S, Ausness R, Pagoulatos A. Reclaiming coal surface mines in central Appalachia: a case study of the benefits and costs. Land Economics 1978;54:472–89.
[33] Daubert JT, Young RA. Recreational demands for maintain-ing instream flows: a contmaintain-ingent valuation approach. American Journal of Agricultural Economics 1981;63:666–76. [34] Greenley DA, Walsh AG, Young RA. Option value:
empiri-cal evidence from a case study of recreation and water quality. Quarterly Journal of Economics 1981;95:657–73.
[35] Gafni A. Using willingness-to-pay as a measure of benefits: what is the relevant question to ask in the context of public decision making? Medical Care 1991;29:1246–52.
[36] Day B, Mourato S. Willingness to pay for water quality main-tenance in Chinese rivers. GSERGE Working Paper WM98-02. Norwich, UK: The Centre for Social and Economic Research on the Global Environment, the University of East Anglia; 1998. [37] National Oceanic and Atmosphere Administration. Report of
the NOAA panel on contingent valuation. Federal Register 1993; 58:4602–4614.
Chao-Hsiun Tang, PhD, is an Associate Professor at the School of Health Care Administration, Taipei Medical University, Taiwan. She holds a PhD in Health Economics from the School of Hygiene and Public Health, Johns Hopkins University. Her research interests include economic evaluation and health policy analyses.
Jin-Tan Liu, PhD, is a Professor at the Department of Economics, National Taiwan University, Taiwan, and research associate at the National Bureau of Economic Research, USA. He holds a PhD in Economics from Vanderbilt University. His research interests include environmental economics and health economics.
Ching-Wen Chang, MSc, works at the Institute of Injury Prevention and Control, Taipei Medical University, Taiwan. She holds an MSc in International Health Policy from the London School of Economics. Wen-Ying Chang, PhD, is an Associate Professor in the Graduate Institute of Nursing, Taipei Medical University, Taipei, Taiwan. Her research interests include outcome research and nursing administration.