ORIGINAL ARTICLE
Effects of Lateral Trunk Support on Scoliotic Spinal
Alignment in Persons With Spinal Cord Injury: A
Radiographic Study
Hui-Fen Mao, MS, OTR, Sheau-Ling Huang, MS, OTR, Tung-Wu Lu, DPhil, Yen-Sheng Lin, MS, Hon-Man Liu, MD, Yen-Ho Wang, MD, Ting-Ming Wang, MD
ABSTRACT. Mao H-F, Huang S-L, Lu T-W, Lin Y-S, Liu H-M, Wang Y-H, Wang T-M. Effects of lateral trunk support on scoliotic spinal alignment in persons with spinal cord injury: a radiographic study. Arch Phys Med Rehabil 2006;87:764-71. Objective: To develop a radiographic method for measuring the spinal alignment of a person in a seated position and with which to investigate the effects of lateral trunk supports (LTS) in special seating on the frontal and sagittal spinal alignment in persons with spinal cord injury (SCI).
Design: Before-after trial.
Setting: University-based research laboratory.
Participants: Ten men and 7 women who had SCI with scoliosis (age, 35.4⫾9.4y; injury level, C5-T11) voluntarily participated.
Intervention: An adjustable seating system with LTS. Main Outcome Measures: Radiographs of the spine in the anteroposterior (AP) and lateral directions were taken while sitting on an adjustable seating system without and with LTS. The Cobb angles and scoliotic indices based on the AP radio-graphic images and the angles of the thoracic and lumbar spine based on lateral were calculated. The relative change in angle (RCA) with LTS in terms of the percentage reduction of the Cobb angles was also obtained.
Results: The Cobb angles and scoliotic indices while sitting with LTS were significantly smaller than those without, the mean difference of Cobb angles⫾ standard error (SE) being 9.12°⫾1.64° (P⬍.001) and those for the scoliotic indices being
.09⫾.04 (P⫽.027). The mean RCA ⫾ SE was
26.16%⫾4.23%. The RCA correlated weakly with the original Cobb angles (r⫽⫺.347, P⫽.172). The LTS caused a signifi-cant reduction in the lumbar angles (P⬍.001), but no signifi-cant effects on the thoracic angles were found.
Conclusions: The radiographic findings demonstrate im-proved scoliotic spinal alignment in the frontal plane and reduced lumbar angles in the sagittal plane in persons with SCI when seated in a special seat and using LTS.
Key Words: Orthotic devices; Radiography; Rehabilitation; Scoliosis; Spinal cord injuries.
© 2006 by the American Congress of Rehabilitation Medi-cine and the American Academy of Physical MediMedi-cine and Rehabilitation
S
COLIOSIS, A CONDITION CHARACTERIZED by lat-eral curvature of the spine with rotation of the vertebrae and deformity in the sagittal plane,1-3 is often observed in persons with spinal cord injury (SCI) who have poor trunk control when using a wheelchair seating system.4-9These spinal de-formities can lead to back pain, pressure ulcers, and respiratory problems, affecting activities of daily living.7-11The degree of the spinal curvature may increase over time. Clinical observa-tions suggest that the greater the magnitude of the curvature, the greater the health and functional difficulties that are asso-ciated with it.12-14 The prevention of the progression of the spinal deformity remains a crucial issue in the management of persons with SCI.Both surgical and nonsurgical treatment methods have been suggested for the management of the progression of the spinal deformity.1Surgical correction of scoliotic deformity is usually suggested if the Cobb angle is greater than 40°.10Although the effects of surgical correction have been shown in patients with cerebral palsy (CP) and adolescent subjects with idiopathic scoliosis,15,16to date no studies have been conducted for the SCI population. The surgical intervention may provide good spinal curve correction, but the procedure may not be justified for routine cases when considering the risks of significant complications for these patients.15,17For Cobb angles less than 40°, nonsurgical methods, such as the use of spinal braces and special seating, can serve as a viable alternative.10These meth-ods have focused mainly on the orthotic management of the scoliosis.1,18,19 Spinal braces have been reported to control scoliosis curve progression effectively for adolescents with idiopathic scoliosis,1,18,19but the users often felt that the braces impacted negatively on their body image and felt uncomfort-able and encumbered, especially when performing daily activ-ities.20On the other hand, special wheelchair seating systems have been a more acceptable method in the management of spinal postural deformities, and may be helpful in the control of the progression of spinal deformities.8,21,22
Special seating has been widely used in clinical practice to improve the sitting posture of persons with SCI who have a low level of sitting ability and are unable to maintain their own sitting posture. There are many types of special seating with different components prescribed for different needs.8,21,22For SCI persons with scoliosis, lateral trunk support (LTS) is among the basic components in seating prescriptions.22 Gen-erally, LTS is applied at 3 positions on the trunk providing a so-called 3-point force system.23Proper use of LTS may enable a better alignment and stabilization of the upper body in the frontal plane and potentially help prevent further spinal defor-mity. However, no study has quantified the influence of LTS in From the School of Occupational Therapy (Mao, Huang), Institute of Biomedical
Engineering (Lu, Lin), Departments of Radiology (Liu) and Physical Medicine and Rehabilitation (Wang Y-H), National Taiwan University, Taipei, Taiwan; and De-partment of Orthopaedics, National Taiwan University Hospital, Taipei, Taiwan (Wang T-M).
Supported by the National Science Council of Taiwan (grant no. NSC 91-2314-B-002-393).
No commercial party having a direct financial interest in the results of the research supporting this article has or will confer a benefit upon the authors or upon any organization with which the authors are associated.
Correspondence to Tung-Wu Lu, DPhil, Institute of Biomedical Engineering, National Taiwan University, No. 1, Sec. 1, Jen-Ai Rd, Taipei 100, Taiwan, e-mail: twlu@ntu.edu.tw. Reprints are not available from the author.
0003-9993/06/8706-10727$32.00/0 doi:10.1016/j.apmr.2006.02.029
764
a special seating system on the spinal alignment in subjects with SCI.
Although LTS provides the trunk with supports in the frontal plane, and is presumably helpful for the reduction of the flexible scoliotic deformity of the spine, many persons with SCI in special seating with LTS subjectively described that they were able to sit more upright. Because the scoliotic deformity of the spine is 3-dimensional in nature,24,25 correc-tion of the spinal curve in 1 plane may result in curve changes in the other 2 planes. Changes of the body alignment and muscle control may also contribute to the phenomenon. Thus, data on the spinal shape changes both in the frontal and sagittal planes owing to LTS are helpful for a better understanding of the effects of LTS on the spinal curve.
The purposes of the present study were to develop a radio-graphic technique that can be used to measure the spinal alignment of a person in a seated position, and use it to investigate the effects of LTS on the frontal and sagittal spinal alignment in persons who had SCI with scoliosis.
METHODS
Ten men and 7 women participated voluntarily in the present study after we obtained informed consents. Table 1 lists the main demographic features of the enrolled subjects. Subjects met the following criteria: (1) SCI between C4 and T12, (2) onset over 1 year, (3) sitting on the wheelchair more than 4 hours a day, (4) diagnosed thoracic or lumbar scoliosis through anteroposterior (AP) radiographs, (5) flexible scoliosis, con-firmed by supine and side-lying bending radiographs. The SCI was neurologically complete, as defined by the American Spi-nal Injury Association.26 All subjects gave written informed consent, as approved by the Medical Ethics Committee at the National Taiwan University Hospital.
In a radiography room, the subject sat relaxed on an adjust-able seating systemawithout any extra support except for a seat belt and foot rests (fig 1). The seat plane was level with a 90° backrest. We adjusted the dimensions of the chair according to each subject’s anthropometry. The seat depth and foot rest height were adjusted according to the thigh and leg lengths. These steps allowed the customization of the adjusted seating system to the specific subject. The backrest of the chair was made of transparent acrylic boards to prevent the degradation of the quality of the radiographic images. During the experi-ment, we instructed subjects to put their hands on their thighs for support and to sit as much upright as possible. Radiographs of the thoracic and lumbosacral spine in the AP and lateral directions were taken with a computerized radiography sys-tem.bThe radiation dose was about 1mSv in 1 exposure. Apart from the radiographic measurements, the spinal alignment was also photographed from AP and lateral views using a digital camera. The shape of the spine was described by stickers attached to the spinous processes of the vertebrae via careful palpation. To examine the effects of LTS, 3-point lateral trunk
supports made of transparent acrylic boards were then applied to the subject by an experienced occupational therapist, based on the shape of the subject’s spinal curve from the radiographs. Radiographs in the AP and lateral directions were then taken in the same way as in the without-LTS condition described above. It took about 1 hour to complete the experiment.
To quantify the changes of the spinal curve with LTS in the frontal plane, we measured Cobb angles2,3and scoliotic indi-ces3from the radiographic images in both the and
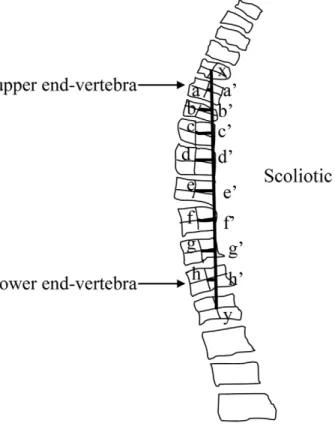
with-out-LTS conditions. The Cobb method has been commonly used to measure and describe the severity of scoliosis in clin-ical research and practice because it is easy and quick to calculate.1 However, because only the angle of curvature de-fined by the ends of the scoliotic curve is obtained, the change of the whole spine is not included in the Cobb method. The scoliotic index proposed by Greenspan overcomes the limita-tion by considering the devialimita-tion of each involved vertebra (fig 2).3It is calculated as follows.
Scoliotic Index⫽aa
⬘⫹ bb⬘⫹ cc⬘⫹ · · · ⫹ hh⬘
xy
where a to h represent each vertebra that was considered as an integral part of the curve; aa=, bb=, . . . , hh= are the lengths of the line segments drawn from the center of each vertebral body and perpendicular to the spinal line that connects the center of the vertebrae immediately above and below the upper and lower end vertebrae of the curve; and xy is the length of the spinal line (fig 2). A scoliotic index of zero denotes a straight spine. The bigger the scoliotic index the more severe the scoliosis.
Fig 1. The experimental setup. Each subject was seated on an adjustable seating system in place for radiographic imaging. Table 1: Demographic Data of the Subjects
Demographic Data Value
Subjects (n) 17
Mean age (range) (y) 35.4 (18.3–51.7) Men/women (n) 10/7 Mean body weight⫾ SE (kg) 58.0⫾2.7 Mean body height⫾ SE (cm) 161.9⫾2.8 Time from onset (range) (y) 17.6 (2.9–35.0)
Abbreviation: SE, standard error.
765 LATERAL TRUNK SUPPORT EFFECTS ON SCI SPINAL ALIGNMENT, Mao
In the sagittal plane, we measured the thoracic angle on the lateral radiograph between the upper endplate of the T6 verte-bra and the lower endplate of the T12 verteverte-bra using the Cobb method, while the lumbar angle was measured from the upper endplate of the L1 vertebra to the lower endplate of the L5 vertebra.16 These 2 variables, together with the Cobb angles
and scoliotic indices, were all measured by an orthopedic surgeon (TMW) using a house-developed software system in Matlab, version 6.5.cThe software loaded the image and then corrected the image distortion using the lead grid before as-sisting the user to draw lines for the calculation of the Cobb angles and scoliotic indices.
We analyzed the measured data using a paired t test with a significance level of .05 to compare the differences between the without- and with-LTS conditions. Relative change in angle (RCA) with LTS was defined as the percent change of the Cobb angle relative to the Cobb angle in the without-LTS condition. The correlation of the Cobb angles and scoliotic indices was examined with the Pearson product moment correlation. SPSSd was used for all the statistical analyses.
RESULTS
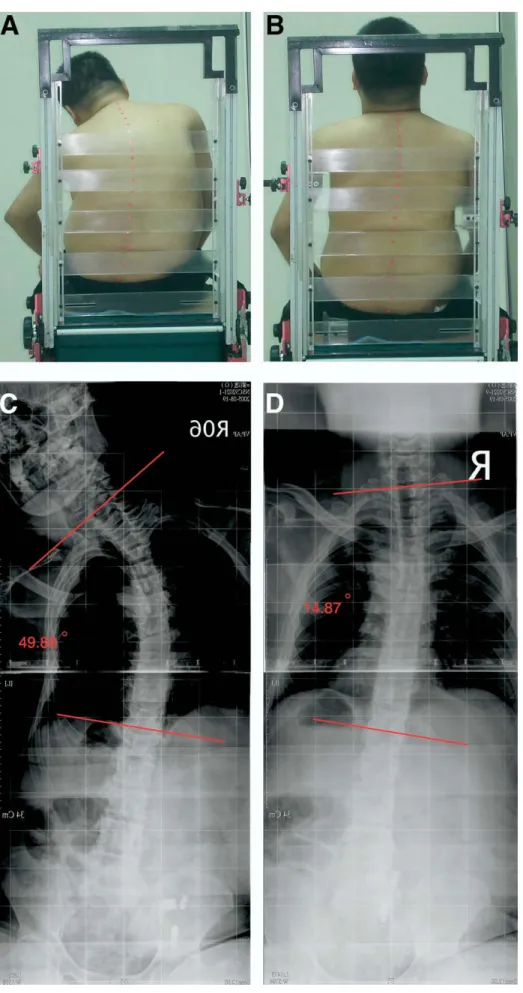
The main clinical features of all 17 subjects before and after applying LTS are listed in table 2. The AP radiographic images of a subject (C5, class A) with line segments drawn for the calcula-tion of the Cobb angles without and with LTS are given in figure 3. The means of the Cobb angles ⫾ standard error (SE) of the subjects in the frontal plane without and with LTS were 39.57°⫾5.24° and 30.45°⫾4.64°, respectively. Seating with LTS gave significantly smaller Cobb angles than without LTS (P⬍.001), the mean difference ⫾ SE being 9.12°⫾1.64°. An average RCA of 26.16%⫾4.23% was noted after applying LTS. The mean scoliotic indices of the subjects without and with LTS were .55⫾.09 and .46⫾.07, respectively. The improvement of the spinal curve with LTS was also indicated by a significant mean
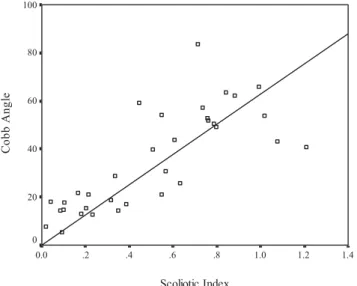
reduction of .09⫾.04 in the scoliotic indices (P⫽.027). The Cobb angles and scoliotic indices for all subjects correlated highly (r⫽.783, P⬍.001) (fig 4). There was a weak correlation between the severity of scoliosis (Cobb angles) and the corresponding RCA (r⫽⫺.347, P⫽.172).
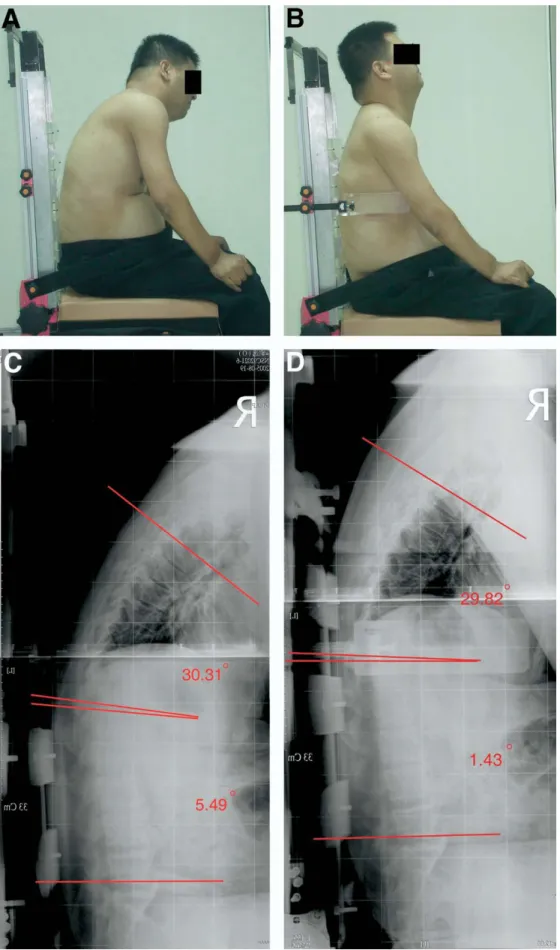
The mean of the lumbar angles without and with LTS were 29.50°⫾5.73° and 24.78°⫾5.56°, respectively. The lumbar angle was significantly decreased with LTS (P⬍.001), the mean reduction and mean RCA being 4.72°⫾0.93° and 24.24%⫾5.68%, respectively. However, there was no signifi-cant difference in the thoracic angles between the 2 seating configurations (without LTS: 37.95°⫾4.03°; with LTS: 34.54° ⫾4.47°; mean difference: 3.40°⫾3.99°; P⫽.41; mean RCA: 1.68%⫾12.4%), although a decreasing trend after using LTS was present. As often observed in clinical practice, a better posture alignment with LTS, including a more symmetric and erect trunk and head-neck posture in both the frontal and sagittal planes, could be seen from photographs of a subject (fig 5).
DISCUSSION
Special seating with LTS is among the methods found most acceptable by persons with SCI and clinicians for managing scoliosis after SCI.8,21However, as indicated in the introduction, no study has quantified the influence of LTS in a special seating system on the spinal alignment in persons with SCI. One reason for this is the difficulties in measuring or assessing the spine of persons with SCI, including the inability of photographic methods to measure skeletal alignment directly, 4,5,27and technical difficul-ties in taking spine radiographs of persons with SCI who have lost the ability to sit independently,16,28while they are sitting in special seating or a wheelchair. Holmes et al 22investigated the effects of lateral support pads on the correction rate for the scoliotic spinal curve in subjects with CP by using photography. Because only the Fig 2. Scoliotic index for mea-suring scoliosis severity.
766 LATERAL TRUNK SUPPORT EFFECTS ON SCI SPINAL ALIGNMENT, Mao
Table 2: Cobb Angles, Lateral Thoracic and Lumbar Angles, and Corresponding RCA Values of All Subjects Without and With LTS
Subject No.
Level of SCI
Cobb Angles Lateral Thoracic Angles Lateral Lumbar Angles
Without LTS (deg) With LTS (deg) RCA* (%) Without LTS (deg) With LTS (deg) RCA* (%) Without LTS (deg) With LTS (deg) RCA* (%) 1 T9 65.83 62.06 5.74 48.12 42.07 12.57 11.43 3.60 68.50 2 T3 21.59 12.87 40.38 19.91 35.26 ⫺77.10 3.40 2.49 26.69 3 T7 28.63 21.24 25.83 30.36 36.16 ⫺19.10 13.71 8.72 36.41 4 T5 52.95 30.75 41.93 50.86 52.82 ⫺3.85 53.05 51.49 2.93 5 T3 54.13 39.76 26.55 42.43 31.31 26.21 33.96 22.09 34.95 6 T9 18.12 7.59 58.13 48.88 70.69 ⫺44.62 72.30 66.82 7.58 7 C6 20.99 14.36 31.59 55.23 35.58 35.58 35.13 33.03 5.99 8 T10 14.37 5.48 61.90 21.10 17.58 16.68 26.42 16.32 38.21 9 T9 63.52 57.35 9.72 14.87 1.47 90.11 72.35 62.43 13.71 10 T11 83.77 59.14 29.40 30.09 39.91 ⫺32.64 34.92 26.36 24.51 11 C5 40.94 25.90 36.73 47.68 55.85 ⫺17.14 14.56 15.82 ⫺8.65 12 T5 17.88 14.85 16.96 34.99 31.80 9.12 11.65 6.32 45.78 13 T5 51.72 43.74 15.43 72.71 30.96 57.42 66.16 64.77 2.11 14 T7 50.42 49.20 2.41 5.46 11.13 ⫺103.85 19.26 15.80 17.99 15 C6 15.39 13.18 14.41 38.22 31.13 18.55 26.16 21.08 19.42 16 C5 53.90 43.03 20.16 37.40 6.68 82.14 3.91 0.99 74.80 17 C6 18.58 17.20 7.45 46.83 56.90 ⬃21.50 3.16 3.12 1.27 Mean⫾ SE 39.57⫾5.24 30.45⫾4.64 26.16⫾4.23 37.95⫾4.03 34.54⫾4.47 1.68⫾12.40 29.50⫾5.73 24.78⫾5.56 24.24⫾5.68 Mean difference⫾ SE 9.12⫾1.64† 3.40⫾3.99 4.72⫾.93†
*Relative change in angle (%)⫽ (without LTS angle ⫺ with LTS angle)/without LTS angle ⫻ 100%.
†
P⬍.05 (significant difference between angles without and with LTS).
767 LATERAL TRUNK SUPPORT EFFECTS ON SCI SPINAL ALIGNMENT, Mao Arch Phys Med Rehabil Vol 87, June
Fig 3. Posterior photographs of a sub-ject with a complete C5 lesion (A) without and (B) with LTS. (C) and (D) are the corresponding mirror-imaged AP radiographs on which lines are drawn for the calculation of the Cobb angles.
768 LATERAL TRUNK SUPPORT EFFECTS ON SCI SPINAL ALIGNMENT, Mao
spinous processes could be palpated and identified when using photography, they had to use the spinous process angle to repre-sent the severity of the scoliosis. This may lead to errors in the measurements because as the degree of rotation increases, the spinous process migrates toward the convexity of the curve. 3,29 Most radiographs of the spine were taken in standing or supine positions,3and few were taken in a sitting position. 30The exper-imental method developed in this study overcame these difficul-ties, thus enabling the first documentation of the effect of special seating with LTS on the changes of the frontal and sagittal scoli-otic spinal alignment in persons with SCI.
The LTS in the special seating significantly improved the spinal alignment of the SCI persons with SCI in the frontal plane with reduced Cobb angles and scoliotic indices. Because the subjects had flexible scoliotic spines, the spinal curvature at the apex would be expected to increase owing to gravitational action, especially when the line of action of the gravitational force is further away from the center of the base of the spinal curve. Persistent bending as a result of this eccentric loading may accelerate the progression of the scoliosis.14,25 LTS ac-cording to the 3-point force configuration aims to provide a moment that counterbalances the bending effect of the eccen-tric gravitational loading on the scoliotic spine, reducing the tension on the convex side and the compression on the concave side of the apex of the spinal curve. A similar biomechanic principle was also used in orthotic devices for the nonoperative treatment of idiopathic scoliosis.23It is noted that the RCA in the frontal plane was not associated with the severity of sco-liosis, because there existed only a weak correlation between the RCA and initial Cobb angle. This suggests that LTS in special seating is effective in improving spinal alignment in the frontal plane, regardless of the severity of the scoliosis. Apart from this immediate effect, the application of LTS to support the trunk and to counterbalance the gravitational bending mo-ment may have a long-term effect on the progression of sco-liosis. The radiographic technique would need to be applied longitudinally to a population of persons with SCI who had been treated with special seating interventions to explore the long-term effect of LTS on the progression of scoliosis.
LTS not only significantly improved the spinal alignment, but also reduced the lumbar angle in the sagittal plane, resulting in a
more erect seating posture. This phenomenon has not been de-scribed in the literature before. A possible explanation is that LTS provides a derotational effect on the spinal column while applying a bending moment on the spine in the frontal plane. 24 This is because a scoliotic spine is often coupled with rotational defor-mities in the other 2 planes, the amount of which depends on the constraints from both the bony and ligamentous structures. Axial rotational deformity can also cause the spine to appear deformed in the sagittal plane. A bending moment in the body’s frontal plane may also produce moment components in the spinal trans-verse and sagittal planes at the same time, which may help reduce the lumbar angle in the subject by improving the bony alignment and removing abnormal tension in the surrounding ligamentous structures.25This effect was also found for thoracic curves, but with less statistical significance, possibly because the restraint from the rib cage that was further restricted by the specialized back support limited the derotational effects. 31 Without LTS a subject’s trunk tended to deviate from the vertical because of the spinal deformity and loss of muscle control (see figs 3, 5). A compensatory movement of the head and neck to position the head close to an upright and center posture was noted. This is clearly shown by the photographic data. LTS helped maintain the upright and center position of the head by correcting and supporting the vertical alignment of the trunk, thus reducing the required effort for the head and neck muscles. It seems that LTS not only helped in improving the spinal alignment, but also enhanced the align-ment of the head and trunk with less muscular effort.
The radiographic method combined with the adjustable seat-ing system developed in the present study allows the AP and lateral radiographs of the thoracic and lumbosacral spine to be taken in a seated position. This technique can be very useful in monitoring changes of spinal alignment in patients who have to remain in a seated position in daily living, which cannot be achieved by traditional approaches such as photographs4,5,27or radiographs taken in standing or supine positions.3The method was used to demonstrate the immediate effects of LTS on the improvement of the spinal alignment in the frontal plane and reduction of the lumbar angles that could be obtained with a special seating system with LTS. However, because scoliosis is a complex deformity in 3 dimensions involving both bending and rotation of the vertebrae,25,32often together with rib de-formation,31 further development of the present method to obtain transverse plane data from the bi-planar radiographs such as using model-based 2- and 3-dimensional registration techniques33is needed. Apart from LTS, further research effort will be needed for the quantification of the long-term effects of other components of special seating, such as pelvic support, on the alignment of the spine.
CONCLUSIONS
A radiographic method combined with an adjustable seating system was developed which can be used to measure the frontal and sagittal spinal alignment of a person in a seated position. The method was used to quantify the immediate effects of special seating with LTS on the changes of the frontal and sagittal spinal alignment in persons with SCI. The results showed that LTS significantly improved the spinal alignment in the frontal plane, regardless of the severity of scoliosis. LTS also reduced the lumbar angle in the sagittal plane, result-ing in a more erect seatresult-ing posture. Because scoliosis is a complex deformity in 3 dimensions, further investigation using a 3-dimensional measurement technique is necessary to pro-vide additional data in the transverse plane. The quantification of the long-term effects of LTS as well as other components of special seating also requires further study.
Fig 4. Correlation of Cobb angles and scoliotic indices (Pearson
rⴝ.783, P<.001).
769 LATERAL TRUNK SUPPORT EFFECTS ON SCI SPINAL ALIGNMENT, Mao
Fig 5. Lateral photographs of a subject with a complete C5 le-sion (A) without and (B) with LTS. (C) and (D) are the corre-sponding radiographs.
770 LATERAL TRUNK SUPPORT EFFECTS ON SCI SPINAL ALIGNMENT, Mao
References
1. Keim HA. Scoliosis. Clin Symp 1978;30:1-30.
2. Magee DJ. Assessment of posture. In: Magee DJ, editor. Ortho-pedic physical assessment. 4th ed. Philadelphia: WB Saunders; 2002. p 873-903.
3. Greenspan A. Scoliosis and anomalies with general affect on the skeleton. In: Greenspan A, editor. Orthopedic imaging: a practical approach. 4th ed. Philadelphia: Lippincott Williams & Wilkins; 2004. p 927-63.
4. Alm M, Gutierrez E, Hultling C, Saraste H. Clinical evaluation of seating in persons with complete thoracic spinal cord injury. Spinal Cord 2003;41:563-71.
5. Bolin I, Bodin P, Kreuter M. Sitting position—posture and per-formance in C5-C6 tetraplegia. Spinal Cord 2000;38:425-34. 6. Hobson DA. Comparative effects of posture on pressure and shear
at the body-seat interface. J Rehabil Res Dev 1992;29:21-31. 7. Minkel JL. Seating and mobility considerations for people with
spinal cord injury. Phys Ther 2000;80:701-9.
8. Salerno S, Kirshblum S. Wheelchairs/adaptive mobility equip-ment and seating. In: Kirshblum S, Campagnolo DI, DeLisa JA, editors. Spinal cord medicine. Philadelphia: Lippincott Williams & Wilkins; 2002. p 578-99.
9. Samuelsson K, Larsson H, Thyberg M, Tropp H. Back pain and spinal deformity— common among wheelchair users with spinal cord injuries. Scand J Occup Ther 1996;3:28-32.
10. Hsu JD. The natural history of spine curvature progression in the nonambulatory Duchenne muscular dystrophy patient. Spine 1983;8:771-5.
11. Turner JA, Cardenas DD, Warms CA, McClellan CB. Chronic pain associated with spinal cord injuries: a community survey. Arch Phys Med Rehabil 2001;82:501-9.
12. Lancourt JE, Dickson JH, Carter RE. Paralytic spinal deformity following traumatic spinal-cord injury in children and adolescents. J Bone Joint Surg Am 1981;63:47-53.
13. Saito N, Ebara S, Ohotsuka K, Kumeta H, Takaoka K. Natural history of scoliosis in spastic cerebral palsy. Lancet 1998;351: 1687-92.
14. Wilkins KE, Gibson DA. The patterns of spinal deformity in Duchenne muscular dystrophy. J Bone Joint Surg Am 1976;58: 24-32.
15. Lonstein JE, Akbarnia A. Operative treatment of spinal deformi-ties in patients with cerebral palsy or mental retardation. An analysis of one hundred and seven cases. J Bone Joint Surg Am 1983;65:43-55.
16. Mac-Thiong JM, Labelle H, Poitras B, Rivard CH, Joncas J. The effect of intraoperative traction during posterior spinal instrumen-tation and fusion for adolescent idiopathic scoliosis. Spine 2004; 29:1549-54.
17. Kim HS, Park JO, Lee HM, et al. Radiographic and functional outcome after surgical management of severe scoliosis in skele-tally immature patients with muscular dystrophy. J Spinal Disord Tech 2004;17:505-10.
18. Goldberg CJ, Moore DP, Fogarty EE, Dowling FE. Adolescent idiopathic scoliosis: the effect of brace treatment on the incidence of surgery. Spine 2001;26:42-7.
19. Rowe DE, Bernstein SM, Riddick MF, Adler F, Emans JB, Gardner-Bonneau D. A meta-analysis of the efficacy of
non-operative treatments for idiopathic scoliosis. J Bone Joint Surg Am 1997;79:664-74.
20. Ugwonali OF, Lomas G, Choe JC, et al. Effect of bracing on the quality of life of adolescents with idiopathic scoliosis. Spine J 2004;4:254-60.
21. Cook AM, Hussey SM. Seating systems as extrinsic enablers for assistive technologies. In: Cook AM, Hussey SM, editors. Assis-tive technologies: principles and practice. 2nd ed. St. Louis: Mosby; 2002. p 165-211.
22. Holmes KJ, Michael SM, Thorpe SL, Solomonidis SE. Manage-ment of scoliosis with special seating for the non-ambulant spastic cerebral palsy population—a biomechanical study. Clin Biomech (Bristol, Avon) 2003;18:480-7.
23. Veldhuizen AG, Cheung J, Bulthuis GJ, Nijenbanning G. A new orthotic device in the non-operative treatment of idiopathic sco-liosis. Med Eng Phys 2002:24:209-18.
24. Carpineta L, Labelle H. Evidence of three-dimensional variability in scoliotic curves. Clin Orthop Relat Res 2003;Jul(412):139-48. 25. Suzuki S, Kasahara Y, Yamamoto S, Seto Y, Furukawa K, Nishino Y. Three-dimensional spinal deformity in scoliosis asso-ciated with cerebral palsy and with progressive muscular dystro-phy. Spine 1993;18:2290-4.
26. Maynard FM Jr, Bracken MB, Creasey G, et al. International Standards for Neurological and Functional Classification of Spinal Cord Injury. American Spinal Injury Association. Spinal Cord 1997;35:266-74.
27. Hastings JD, Fanucchi ER, Burns SP. Wheelchair configuration and postural alignment in persons with spinal cord injury. Arch Phys Med Rehabil 2003;84:528-34.
28. Steib JP, Dumas R, Mitton D, Skalli W. Surgical correction of scoliosis by in situ contouring: a detorsion analysis. Spine 2004; 29:193-9.
29. Herzenberg JE, Waanders NA, Closkey RF, Schultz AB, Hens-inger RN. Cobb angle versus spinous process angle in adolescent idiopathic scoliosis. The relationship of the anterior and posterior deformities. Spine 1990;15:874-9.
30. Hobson DA, Tooms RE. Seated lumbar/pelvic alignment. A com-parison between spinal cord-injured and noninjured groups. Spine 1992;17:293-8.
31. Aubin CE, Dansereau J, de Guise JA, Labelle H. Rib cage-spine coupling patterns involved in brace treatment of adolescent idio-pathic scoliosis. Spine 1997;22:629-35.
32. Stokes IA, Gardner-Morse M. Analysis of the interaction between vertebral lateral deviation and axial rotation in scoliosis. J Bio-mech 1991;24:753-9.
33. DeFrate LE, Sun H, Gill TJ, Rubash HE, Li G. In vivo tibiofemo-ral contact analysis using 3D MRI-based knee models. J Biomech 2004;37:1499-504.
Suppliers
a. Aerospace Industrial Development Corp, No. 111-15, Lane 68, Fu-Hsing N Rd, Taichung, Taiwan 407, ROC.
b. Agfa-Gevaert NV, Septestraat 27, B-2640 Mortsel, Belgium. c. The MathWorks Inc, 3 Apple Hill Dr, Natick, MA 01760-2098. d. Version 11.0.1; SPSS Inc, 233 S Wacker Dr, 11th Fl, Chicago, IL
60606.
771 LATERAL TRUNK SUPPORT EFFECTS ON SCI SPINAL ALIGNMENT, Mao