AUTHOR QUERY SHEET
Author(s): Chih-Chia Liang, I-Kuan Wang, Huey-Liang Kuo, Hung-Chieh Yeh, Hsin-Hung Lin,
Yao-Lung Liu, Wei-Min Hsu, Chiu-Ching Huang, and Chiz-Tzung Chang
Article Title: Long-Term Use of Fenofibrate Is Associated with Increased Prevalence of Gallstone
Disease among Patients Undergoing Maintenance Hemodialysis
Article No.: LRNF 577545
Dear Author,
Please check these proofs carefully. It is the responsibility of the corresponding author to check against the
original manuscript and approve or amend these proofs. A second proof is not normally provided. Informa Healthcare cannot be held responsible for uncorrected errors, even if introduced during the composition process. The journal reserves the right to charge for excessive author alterations, or for changes requested after the proofing stage has concluded.
The following queries have arisen during the editing of your manuscript and are marked in the margins of the proofs. Unless advised otherwise, submit all corrections using the CATS online correction form. Once you have added all your corrections, please ensure you press the “Submit All Corrections” button.
Ref. no: Query Remarks
AQ1
Please verify all author names, their affiliations and
correspondence details.
AQ2
Please provide the department for the affiliation “College of
Medicine, China Medical University, Taichung, Taiwan” if
available.
AQ3
Please provide the full form of MHD.
AQ4
Please check the edit of the sentence “Among HD
patients...”.
AQ5
A declaration of interest statement reporting no conflicts of
interest has been inserted. Please confirm the statement is
accurate.
Renal Failure, 00(00): 1–5, (2011) Copyright © Informa Healthcare USA, Inc. ISSN 0886-022X print/1525-6049 online DOI: 10.3109/0886022X.2011.577545
LRNF
CLINICAL STUDY
Long-Term Use of Fenofibrate Is Associated with Increased Prevalence
of Gallstone Disease among Patients Undergoing Maintenance
Hemodialysis
Long-Term Fenofibrate Use in Hemodialysis Patients
Chih-Chia Liang
1,2, I-Kuan Wang
1,2, Huey-Liang Kuo
1,2, Hung-Chieh Yeh
1,2, Hsin-Hung Lin
1,2,
Yao-Lung Liu
1,2, Wei-Min Hsu
3, Chiu-Ching Huang
1,2and Chiz-Tzung Chang
1-41Department of Internal Medicine, Kidney Institute and Division of Nephrology, China Medical University Hospital, Taichung, Taiwan; 2College of Medicine, China Medical University, Taichung, Taiwan; 3Zen-Ho Dialysis Center, Taichung, Taiwan; 4Chuan-An Dialysis Center, Taoyuan, Taiwan
Abstract
Background: In spite of insufficient evidence to guide the use of lipid-lowering drugs (LLDs) among the dialysis
popu-lation, these drugs are frequently used to treat dyslipidemia. Several studies have found that long-term use of LLDs is associated with an increased risk of gallstone disease (GSD) in the general population. However, the lithogenic risk of LLDs in patients undergoing hemodialysis (HD) has not been studied. Aim: It is to assess the influence of long-term use of LLDs on the prevalence of GSD among patients undergoing HD. Methods: This cross-sectional study included 108 eligible patients receiving maintenance HD: 35 receiving lovastatin; 34 fenofibrate; and 39 no LLD. GSD was defined as the presence of gallstones or the performance of cholecystectomy while taking LLD. Abdominal ultra-sonography, demographic parameters, and laboratory data were obtained for all enrolled subjects. ANOVA with Bon-ferroni’s test and chi-square test were used to compare differences among the three groups. Results: The three groups had similar clinical characteristics with regard to age, gender, duration of HD, body mass index, and total cho-lesterol values. However, a significantly higher prevalence of GSD and higher triglyceride levels were found in patients receiving fenofibrate, compared with those in other groups (p < 0.05). Among dialysis patients on fenofibrate, increased age, female gender, larger daily dose, and longer duration of treatment were associated with increased risks for GSD. Conclusions: Our study shows that long-term use of fenofibrate is related to increased risk of GSD among HD patients. Further large-scale studies are needed to confirm our findings.
Keywords: Dyslipidemia, end-stage renal disease, fenofibrate, gallstone disease, hemodialysis
INTRODUCTION
The prevalence of gallstone disease (GSD) varies greatly among people of different ethnic origins. There are many known risk factors for the formation of gall-stones, including female gender, increasing age, obe-sity, pregnancy, and lipid-lowering drugs (LLDs).1–3 Among many reports, only a few articles have focused on the dialysis population. Some studies indicated that the incidence of GSD in hemodialysis (HD) patients was similar to that in controls;4–6 however, others found a higher prevalence in the dialysis population.7,8 Biliary cholesterol hypersecretion and slower intestinal transition are proposed explanations for the higher
prevalence of GSD among HD patients compared with the general population.9 In addition, the gallbladder is innervated by the autonomic nervous system, which malfunctions in uremia; this might further contribute to gallstone formation.6,10
On the other hand, end-stage renal disease (ESRD) patients tend to have abnormalities in lipid metabolism and alterations in lipid profiles, such as increased levels of triglycerides and lipoprotein a.11,12 Dyslipidemia, a well-known contributor to cardiovascular disease (CVD) in the general population, has also been pro-posed to explain the high mortality from CVD among ESRD patients.11,12 Although several large-scale stud-ies did not demonstrate clear clinical benefits of LLDs
Address correspondence to Chiz-Tzung Chang, Department of Internal Medicine, Division of Nephrology and Kidney Institute, China Medical University Hospital, No. 2, Yu-der Road, North District, Taichung 404, Taiwan. Tel.: Tel.: +886 4 22052121; Fax: +886 4 22076863; E-mail: [email protected]
Received 13 January 2011; Revised 20 March 2011; Accepted 28 March 2011
AQ1 AQ2 10 15 20 25 30 35 40 45 50 5
2 C.-C. Liang et al.
Renal Failure
in reducing morbidity and mortality due to CVD in the dialysis population, many nephrologists prescribe these drugs to treat dyslipidemia according to the treatment guidelines for the general population.13 These drugs, especially fibrates, may change biliary lipid and bile acid compositions, that is, increase the concentration of bil-iary cholesterol and phospholipids but reduce that of bile acids.14–16 Through this mechanism, these drugs have been found to predispose patients to formation of gall-stones.14 However, the lithogenic risk of long-term LLD administration to ESRD patients has not been studied.
We conducted a cross-sectional study to assess the influence of long-term LLD administration on the prevalence of GSD in patients undergoing maintenance HD. As a secondary objective, we also implemented subgroup analysis to identify risk factors for GSD among HD patients receiving fibrates.
MATERIALS AND METHODS
Patient Population and Study Design
This study initially included 305 dialysis patients receiving maintenance HD at Zen-Ho Dialysis Center (Taichung County, Taiwan) and Chuan-An Dialysis Center (Taoyuan County, Taiwan). Of these patients, 167 had received lovastatin (20 μg tablets) or fenofi-brate (200 μg micronized capsules) after initiation of HD. Patients were considered eligible for inclusion if they received LLDs for a total period of more than 1 year and agreed to participate in this study. For a sin-gle subject, several periods of LLD use were summed up. We excluded patients if they had undergone perito-neal dialysis or transplantation, received other types of LLDs (except lovastatin and fenofibrate), used oral conceptive agents, or had a history of GSD prior to receiving LLDs. Finally, there were 35 eligible patients in the lovastatin group and 34 in the fenofibrate group. From the 138 MHD patients without LLD use, we chose 39 age- and sex-matched patients to serve as the control group, in accordance with the exclusion criteria mentioned above. Finally, 108 subjects were enrolled in this study for further analysis.
Collection of Clinical Data
We collected complete blood counts, serum biochemical data, and parameters of dialysis adequacy at the time of the study (December 2009). To assess the impact of LLDs on the prevalence of GSD, ultrasonography was performed by a single operator for all enrolled subjects. It should be noted that ultrasound has become the initial diagnostic study of choice in patients with suspected gallstones because of its high sensitivity and specificity.17 Besides, GSD was defined as the presence of gallstones at the time of the study or cholecystectomy performed during the period of therapy with LLDs. Subjects were asked to fast for at least 8 h before sonography studies. Gallstones were diagnosed by the presence of a moveable
hyperechoic substance with an acoustic shadow.18 Cholecystectomy was confirmed by surgical history or the absence of the gallbladder on ultrasonography. This clinical study followed the principles of the Declaration of Helsinki and was compatible with the policies of the local ethics committee. Informed written consent was obtained from all participants.
Statistical Analysis
All statistical analyses were carried out using Statistical Packages for Social Sciences (SPSS) 13.0 for Windows (SPSS, Inc., Chicago, IL, USA). Unless otherwise stated, continuous variables are expressed as mean ± standard deviation and categorical variables as num-bers or percentages. For continuous variables, compar-isons among the three groups were analyzed using ANOVA with Bonferroni’s test for post hoc analysis. For categorical variables, a cross-table with chi-square test or Fisher’s exact test was used, as appropriate. To identify risk factors of GSD among MHD patients receiving fenofibrate, we performed Student’s t-test or Mann–Whitney U-test to compare continuous variables and Fisher’s exact test to compare categorical variables. The criterion for significance was the 95% confidence interval to reject the null hypothesis.
RESULTS
Study Population Characteristics
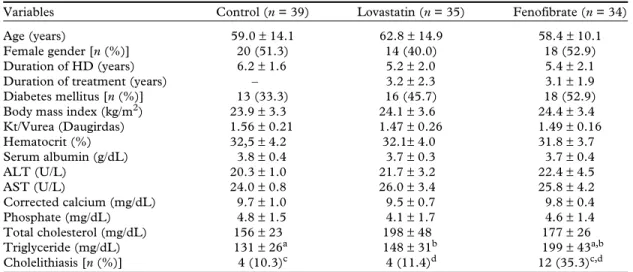
A total of 108 patients were enrolled in this study and all received maintenance HD with a high-flux dialyzer during the study period. There were 39 subjects in the control group, 35 in the lovastatin group, and 34 in the fenofibrate group. As shown in Table 1, the three groups were similar with respect to baseline character-istics, except for serum triglyceride value and the fre-quency of GSD. Patients receiving fenofibrate had a higher serum triglyceride level than that of patients in the control or lovastatin group (199 ± 43 vs. 131 ± 26 mg/dL, p < 0.01; 199 ± 43 vs.148 ± 31 mg/dL, p < 0.05, respectively). However, there were no statistical differ-ences in serum cholesterol values between the three groups. During the follow-up period, 4 of 39 patients in the control group, 4 of 35 in the lovastatin group, and 12 of 34 in the fenofibrate group developed GSD. Patients receiving fenofibrate had a significantly higher prevalence of GSD compared with that in the lovasta-tin or control group (p < 0.05).
Clinical Manifestations of GSD
GSD showed various manifestations in fenofibrate users. Four subjects presented with sudden colic pain, four with acute cholecystitis, and two with acute pan-creatitis; two subjects had no symptoms. Fever occurred in all patients who presented with acute cholecystitis and acute pancreatitis. Nine fenofibrate users underwent cholecystectomy but only one in the AQ3 70 75 80 85 90 95 100 105 110 115 120 125 130 135 140 145 150 155 160 165 170
lovastatin group and one in the control group under-went this procedure. The fenofibrate group had the highest cholecystectomy rate among the three groups (9/34 vs. 1/35 vs. 1/39, p = 0.001, not shown in tables). Furthermore, we implemented subgroup analysis to explore risk factors for GSD among HD patients using fenofibrate (Table 2). We found that increased age, female gender, higher daily dose of fenofibrate, and longer duration of treatment were associated with increased risks for GSD. However, the subgroup analy-sis did not find any association between GSD and body mass index or diabetes status.
DISCUSSION
This cross-sectional study evaluated the impact of long-term administration of LLDs on the prevalence of
GSD among ESRD patients undergoing chronic HD in Taiwan. We found that long-term use of fenofibrate, instead of lovastatin, was related to higher prevalence of GSD in MHD patients. Furthermore, our results showed that higher daily dose of fenofibrate, increased age, female gender, and longer duration of treatment were associated with a higher risk of developing GSD. To our knowledge, this is the first study to report a higher prevalence of GSD in MHD patients with long-term fenofibrate use.
GSD is a common disease not only in Western countries but also in Taiwan.19 Similarly, the prevalence and incidence of ESRD are also very high in Taiwan.20 However, until now few studies have investigated the relationship between these two common diseases. Con-flicting results were reported regarding GSD rates among HD patients. The complex factors related to
Table 1. Baseline characteristics of the control, lovastatin, and fenofibrate groups.
Variables Control (n = 39) Lovastatin (n = 35) Fenofibrate (n = 34)
Age (years) 59.0 ± 14.1 62.8 ± 14.9 58.4 ± 10.1
Female gender [n (%)] 20 (51.3) 14 (40.0) 18 (52.9)
Duration of HD (years) 6.2 ± 1.6 5.2 ± 2.0 5.4 ± 2.1
Duration of treatment (years) – 3.2 ± 2.3 3.1 ± 1.9
Diabetes mellitus [n (%)] 13 (33.3) 16 (45.7) 18 (52.9)
Body mass index (kg/m2) 23.9 ± 3.3 24.1 ± 3.6 24.4 ± 3.4
Kt/Vurea (Daugirdas) 1.56 ± 0.21 1.47 ± 0.26 1.49 ± 0.16 Hematocrit (%) 32,5 ± 4.2 32.1± 4.0 31.8 ± 3.7 Serum albumin (g/dL) 3.8 ± 0.4 3.7 ± 0.3 3.7 ± 0.4 ALT (U/L) 20.3 ± 1.0 21.7 ± 3.2 22.4 ± 4.5 AST (U/L) 24.0 ± 0.8 26.0 ± 3.4 25.8 ± 4.2 Corrected calcium (mg/dL) 9.7 ± 1.0 9.5 ± 0.7 9.8 ± 0.4 Phosphate (mg/dL) 4.8 ± 1.5 4.1 ± 1.7 4.6 ± 1.4 Total cholesterol (mg/dL) 156 ± 23 198 ± 48 177 ± 26 Triglyceride (mg/dL) 131 ± 26a 148 ± 31b 199 ± 43a,b Cholelithiasis [n (%)] 4 (10.3)c 4 (11.4)d 12 (35.3)c,d
Notes: n, number of patients; HD, hemodialysis; Kt/Vurea, adequacy of dialysis dose; ALT, alanine transami-nase; AST, aspartate transaminase.
aControl versus fenofibrate (p < 0.01). bLovastatin versus fenofibrate (p < 0.05). cControl versus fenofibrate (p < 0.05). dLovastatin versus fenofibrate (p < 0.05).
Table 2. Comparison of clinical characteristics between fenofibrate users with and without gallstone formation.
Variables Subjects without
gallstones (n = 22) Subjects with gallstones (n = 12) p-Value Age (years) 56.2 ± 2.3 63.6 ± 2.8 0.020 Female gender [n (%)] 8 (36.4) 10 (83.3) 0.013 Diabetes mellitus [n (%)] 12 (54.5) 6 (50.0) NS
Body mass index (kg/m2) 23.5 ± 3.6 24.6 ± 3.3 NS
Duration of HD (years) 5.6 ± 2.3 5.1 ± 2.0 NS
Duration of treatment (years) 2.5 ± 1.8 3.9 ± 2.4 0.048
Number of L/M/H dosea 10/6/6 0/3/9 0.006
Total cholesterol (mg/dL) 175 ± 25 180 ± 12 NS
Triglyceride (mg/dL) 191 ± 47 212 ± 35 NS
Notes: n, number of patients; NS, not significant.
aL: subjects received low dose of fenofibrate (50 mg/day); M: medium dose of fenofibrate (100 mg/day);
H: high dose of fenofibrate (200 mg/day).
175 180 185 190 195 200 205
4 C.-C. Liang et al.
Renal Failure
kidney disease and dialysis are likely to complicate find-ings on prevalence and risk of GSD in ESRD patients. Since administration of multiple drugs is very common in the dialysis population, the influence of these drugs should be elucidated.
Fibric acid derivatives are indicated for the treat-ment of dyslipidemia by reducing levels of triglycerides and increasing levels of high-density lipoprotein choles-terol.13 Treatment with fibrates increases relative con-centrations of biliary cholesterol and phospholipids but decreases that of bile acid.14–16 These changes lead to elevated cholesterol saturation index and increased incidence of cholesterol gallstones in patients receiving long-term fibrate administration.14–16 In addition, gall-stone formation has been linked to the reduction of hepatic cholesterol 7a-hydroxylase activity by fibrates.21 Although fibrates have been found to be a potential risk factor for GSD in the general population, their effects have not been investigated in the dialysis population. Our study shows that these adverse effects also exist in the dialysis population.
Lovastatin is an HMG-CoA reductase inhibitor used for the treatment of hypercholesterolemia by blocking the synthesis of cholesterol or cholesterol crystal nucle-ation.13 In an animal study, lovastatin could alter bile composition and dissolve gallstones.22 In contrast to this animal study showing statins to be a protective fac-tor, our results did not demonstrate any difference in GSD rates between the lovastatin and control groups. Similarly, an epidemiological study reported by Caroli-Bosc et al.14 did not find HMG-CoA reductase inhibi-tors to be associated with protection from GSD. Because of renal failure and advanced age, most of our patients received low-dose lovastatin (10 mg/day) to treat hypercholesterolemia. We considered that such a low dose may be insufficient to dissolve gallstones.
On the other hand, our results showed higher serum triglyceride levels existed in the fenofibrate group. Previous studies also demonstrated that hyper-triglyceridemia might be a risk factor for the develop-ment of GSD.23,24 It has been found that hypertriglyceridemia and GSD are often linked, par-ticularly in patients with overweight and insulin resis-tance.25 Furthermore, patients with obesity and insulin resistance have an increased risk for hypertrig-lyceridemia and gallstone formation.26 Hypertriglyc-eridemia is most often a disorder with multiple factors, such as diet, age, lifestyle, drug therapy, and metabolic syndrome.24 This condition is similar for gallstone formation as well. In addition, hypertriglyc-eridemia patients with poor response to diet control usually receive fibrates which are also related to an increased prevalence of GSD. Whether hypertriglycer-idemia per se is a risk factor for GSD or it is just asso-ciated with this disease remains uncertain. To settle this dispute, further studies are warranted to elucidate the complex relationship among hypertriglyceridemia, gallstone formation, and fibrate uses.
Our present findings revealed that the prevalence of GSD in the fenofibrate group was strikingly high, compared with that in other reports.4–8 We propose the following possible explanations. First, most of our dialysis patients had multiple risk factors for GSD, such as diabetes, old age, and the use of fenofibrates, which may greatly increase this risk. Second, HD removed little of the fenofibrates so that a large amount of fenofibrate was retained in the body of HD patients despite reduction in dose.27 This may be why HD patients receiving higher doses of fenofibrate had GSD more frequently than those receiving lower doses. However, many physicians still prescribe this drug to treat dyslipidemia in HD patients because of its cheaper cost. Although we did not observe the occurrence of rhabdomyolysis or hepatitis in the study population, the use of fibrates indeed caused an increase in the prevalence of GSD. Therefore, we suggest that fenofibrate be avoided in patients under-going HD.
However, some limitations still exist in the present study. First, the main limitation was the small sample size, which prevented us from performing multivariate analysis. Second, several risk factors for GSD, such as smoking, drinking alcohol, and dietary habits, were not included in the analysis. However, previous stud-ies had similar limitations. Third, because gallstone formation needs a long time to develop, previous studies adopted cross-sectional designs to demon-strate the relationship between fibrates and gallstones. Our study also used a cross-sectional design, that is, prevalence study, to explore the prevalence of GSD among maintenance HD patients; therefore, we could not know if gallstone formation developed before the administration of fenofibrate. Finally, our study could not confirm a causal relationship between fibrates and gallstone formation in the dialysis population. To clarify whether the use of fibrates was a surrogate for other known risk factors or a cause of GSD, more studies are needed to elucidate this relationship among HD patients.
In conclusion, our study demonstrated that HD patients receiving fibrates had a higher prevalence of GSD. Among HD patients on fibrates, those on a higher daily dose, that is, the elderly, women, and patients with a longer duration of treatment, were more likely to develop GSD. Our findings highlight the fact that the use of fenofibrates should be avoided in patients undergoing long-term HD.
ACKNOWLEDGMENTS
We appreciate the efforts of all dialysis staff at Zen-Ho Dialysis Center (Taichung County) and Chuan-An Dialysis Center (Taoyuan County) for the collection of clinical data. Parts of this study were presented at the Annual Meeting of the Taiwan Society of Nephrology (11–12 December 2010, Taipei, Taiwan).
AQ4 210 215 220 225 230 235 240 245 250 255 260 265 270 275 280 285 290 295 300 305 310 315
Declaration of Interest: The authors report no
con-flicts of interest. The authors alone are responsible for the content and writing of the paper.
REFERENCES
[1] Martínez de Pancorbo C, Carballo F, Horcajo P, et al. Preva-lence and associated factors for gallstone disease: Results of a population survey in Spain. J Clin Epidemiol. 1997;50:1347– 1355.
[2] Bates T, Harrison M, Lowe D, Lawson C, Padley N. Longitu-dinal study of gallstone prevalence at necropsy. Gut. 1992;33:103–107.
[3] Jensen KH, Jorgensen T. Incidence of gallstones in a Danish population. Gastroenterology. 1991;100:790–794.
[4] Hojs R. Cholecystolithiasis in patients with end-stage renal disease treated with hemodialysis: A study of prevalence. Am J Nephrol. 1995;15:15–17.
[5] Dumlu S, Bali M, Yilmaz M, et al. Prevalence of gallstone dis-ease in hemodialysis patients. Nephron. 1998;78:347–348. [6] Altiparmak MR, Pamuk ON, Pamuk GE, et al. Prevalence of
gallstones in chronic renal failure patients undergoing hemodi-alysis: Experience of a center in Turkey. Am J Gastroenterol. 2003;98:813–820.
[7] Li Vecchi M, Soresi M, Cusimano R, et al. Prevalence of bil-iary lithiasis in a Sicilian population of chronic renal failure patients. Nephrol Dial Transplant. 2003;18:2321–2324. [8] Badalamenti S, DeFazio C, Castelnovo C, et al. High
preva-lence of silent gallstone disease in dialysis patients. Nephron. 1994;66:225–227.
[9] Marecková O, Skála I, Marecek Z, et al. Bile composition in patients with chronic renal insufficiency. Nephrol Dial Trans-plant. 1990;5:423–425.
[10] Bektas A, Belet U, Kelkitli E, Bakir T, Acikgoz A, Akpolat T. Ultrasonic gallbladder function in chronic kidney disease: Does predialysis, hemodialysis, or CAPD affect it? Ren Fail. 2005;27:677–681.
[11] Toto RD, Vega GL, Grundy SM. Mechanisms and treatment of dyslipidemia of renal diseases. Curr Opin Nephrol Hypertens. 1993;2:784–790.
[12] Ponda MP, Barash I. Lipid metabolism in dialysis patients – The story gets more complicated. Semin Dial. 2008;21: 390–394.
[13] Nogueira J, Weir M. The unique character of cardiovascular disease in chronic kidney disease and its implications for
treatment with lipid-lowering drugs. Clin J Am Soc Nephrol. 2007;2:766–785.
[14] Caroli-Bosc FX, Le Gall P, Pugliese P, et al. Role of fibrates and HMG-CoA reductase inhibitors in gallstone formation: Epidemiological study in an unselected population. Dig Dis Sci. 2001;46:540–544.
[15] Bateson MC, Maclean D, Ross PE, Bouchier IAD. Clofibrate therapy and gallstone induction. Dig Dis Sci. 1978;7:623–628. [16] Palmer RH. Effect of fenofibrate on bile lipid composition.
Arteriosclerosis. 1985;5:631–638.
[17] Cooperberg PL, Burhenne HJ. Real-time ultrasonography. Diagnostic technique of choice in calculous gallbladder dis-ease. N Engl J Med. 1980;302:1277–1279.
[18] Hahm JS, Park JY, Park KG, Ahn YH, Lee MH, Park KN. Gallbladder motility in diabetes mellitus using real time ultra-sonography. Am J Gastroenterol. 1996;91:2391–2394. [19] Chen CY, Lu CL, Huang YS, et al. Age is one of the risk
fac-tors in developing gallstone disease in Taiwan. Age Ageing. 1998;27:437–441.
[20] U.S. Renal Data System. USRDS. Annual data report: Atlas of chronic kidney disease and end-stage renal disease in the United States. Bethesda, MD: National Institutes of Health, National Institute of Diabetes and Digestive and Kidney Diseases; 2008.
[21] Roglans N, Vazquez-Carrera M, Alegret M, et al. Fibrates modify the expression of key factors involved in bile-acid syn-thesis and biliary-lipid secretion in gallstone patients. Eur J Clin Pharmacol. 2004;59:855–861.
[22] Abedin MZ, Narins SC, Park EH, Smith PR, Kirkwood KS. Lovastatin alters biliary lipid composition and dissolves gall-stones: A long-term study in prairie dogs. Dig Dis Sci. 2002;47:2192–2210.
[23] Andreotti G, Chen J, Gao YT, et al. Serum lipid levels and the risk of biliary tract cancers and biliary stones: A population-based study in China. Int J Cancer. 2008;122:2322–2329. [24] Breuer HW. Hypertriglyceridemia: A review of clinical
rele-vance and treatment options: Focus on cerivastatin. Curr Med Res Opin. 2001;17:60–73.
[25] Pagliarulo M, Fornari F, Fraquelli M, et al. Gallstone disease and related risk factors in a large cohort of diabetic patients. Dig Liver Dis. 2004;36:130–134.
[26] Smelt AH. Triglycerides and gallstone formation. Clin Chim Acta. 2010;411:1625–1631.
[27] Desager JP, Costermans J, Verberckmoes R, Harvengt C. Effect of hemodialysis on plasma kinetics of fenofibrate in chronic renal failure. Nephron. 1982;31:51–54.
AQ5 320 325 330 335 340 345 350 355 360 365 370 375 380 385 390 395 400 405