Contents lists available at ScienceDirect
Journal of the Formosan Medical Association
Journal homepage: http://www.jfma-online.com
Journal of the Formosan Medical Association
ISSN 0929 6646
Formosan Medical Association Taipei, Taiwan
Volume 109 Number 12 December 2010
Recent advances in clinical application of gut hormones Urinary NGF levels in OAB and lower urinary tract disorders Pollen allergy in Taiwanese patients Parvovirus infection among hospital staff
Case Report
Hepatitis Associated With Prothionamide for
Treatment of Multidrug-resistant Tuberculosis
Han-Lin Hsu,1 Kuan-Jen Bai,1Yi-Chun Chiang,2,3Shian-Jiun Lin,1Ming-Chih Yu1*
Timely and intensive monitoring for, and management of, adverse effects caused by anti-tuberculosis drugs are essential components of control programs for multidrug-resistant tuberculosis (MDR-TB). This retrospective case series was conducted in northern Taiwan from January 2007 to December 2008 at Taipei Medical University–Wan Fang Hospital, a 750-bed tertiary-care center and MDR-TB referral center. Hepatitis associated with prothionamide was defined as the recurrence of hepatitis after a second prothionamide treatment re-challenge. In total, 47 patients with MDR-TB enrolled in the Directly Observed Therapy, Short Course–Plus Program were identified during the study period, and 44 (93.6%) were treated with prothionamide. Seven of these 44 patients (15.9%) developed hepatitis after being treated with prothion-amide concurrent with other anti-tuberculosis agents. Hepatitis associated with prothionprothion-amide occurred in three of these seven patients (6.8%). In these three patients, hepatitis developed following treatment with prothionamide for 28 days, 39 days or 45 days. Hepatitis developed rapidly after re-challenge with prothionamide at 4 days, 4 days and 3 days, respectively. Liver function returned to the normal range after cessation of prothionamide treatment for 19 days, 27 days or 28 days. Close monitoring of liver function was necessary in MDR-TB patients who received prothionamide treatment.
Key Words: hepatitis, multidrug-resistant tuberculosis, prothionamide
Multidrug-resistant tuberculosis (MDR-TB) is defined as resistance to, at a minimum, the anti-tuberculosis drugs isoniazid and rifampicin. Multidrug resistance severely compromises anti-tuberculosis management, and MDR-TB is a growing problem throughout the world. The laboratory-based Taiwan Surveillance of Drug
Resistance in TB program was established in 2003. Surveillance has revealed that 5.3% (2004) and 4.0% (2005) of TB isolates were MDR-TB.1 The World Health Organization has recommended a duration of at least 18 months for culture con-version when treating for MDR-TB.2 Concerns have been raised over the possibility of excessive
©2010 Elsevier & Formosan Medical Association
. . . .
1Division of Pulmonary Medicine, Department of Internal Medicine, 2Department of Pharmacy, Taipei Medical University–
Wan Fang Hospital, and 3School of Pharmacy, Taipei Medical University, Taipei, Taiwan.
Received: January 8, 2010 Revised: April 1, 2010 Accepted: April 8, 2010
*Correspondence to: Dr Ming-Chih Yu, Division of Pulmonary Medicine, Department of
Internal Medicine, Taipei Medical University-Wan Fang Hospital, 111, Section 3, Hsin-Long Road, Section 3, Taipei, Taiwan.
adverse affects during long-term use of multidrug regimens. Second-line anti-tuberculosis agents used in treatment of MDR-TB have many known side effects,3–10for example, hepatitis is associated with prothionamide or ethionamide. This condi-tion occurs more frequently when prothionamide treatment is combined with another second-line anti-tuberculosis medication, para-aminosalicylic acid.3,4,6,9,11,12Furthermore, treatment with pro-thionamide was the most likely cause of fatali-ties in a previous study.6 The clinical course of prothionamide-associated hepatitis has only been described in a few cases in the literature.11,12Here, we report three cases of hepatitis associated with prothionamide treatment for MDR-TB.
Case Report
This retrospective case series was conducted in Taiwan from January 2007 to December 2008, at the Taipei Medical University–Wan Fang Hospital, a 750-bed tertiary-care center and MDR-TB referral center. For the purposes of this study, hepatitis was defined as an elevated aminotransferase level > five times the upper limit of normal [aspartate aminotransferase (AST) < 41 U/L; alanine amino-transferase (ALT)< 40 U/L], with or without symp-toms, or > three times upper limit of normal in the presence of symptoms, or elevated total biliru-bin > 2 mg/dL (normal range, 0.3–1.2 mg/dL).13 Hepatitis associated with prothionamide was de-fined as hepatitis that re-occurred after prothion-amide re-challenge.
A total of 47 patients with MDR-TB enrolled into the Directly Observed Therapy, Short Course (DOTS)–Plus program were monitored during the study period. The mean age of the patients was 50.5± 16.3 years. Forty-four of these patients (93.6%) received prothionamide. Seven of these 44 patients (15.9%) developed hepatitis during concurrent treatment with prothionamide and other anti-tuberculosis agents (para-aminosalicylic acid, isoniazid, or pyrazinamide). Among these seven patients, three (3/44, 6.8%) met our defini-tion of hepatitis associated with prothionamide.
Case 1
A 37-year-old man with MDR-TB, who weighed 77.0 kg received the following anti-tuberculosis multidrug regimen: rifater (rifampicin 120 mg/ isoniazid 80 mg/pyrazinamide 250 mg, 5 tablets daily), ethambutol (800 mg daily), streptomycin (1.0 g daily), levofloxacin (750 mg once daily), cycloserine (250 mg 3 times daily) and prothion-amide (250 mg 3 times daily). Baseline AST, ALT, total bilirubin, blood cell counts and serum crea-tinine levels were within normal limits. Blood specimens tested on day 28 of treatment revealed AST 215 U/L, ALT 366 U/L and total bilirubin 0.47 mg/dL. The patient complained of a mildly poor appetite during the office visit, and denied a history of alcohol abuse and exposure to any other hepatotoxic drug or toxin. Tests for hepatitis B surface antigen (HBsAg), anti-hepatitis A virus IgM, and anti-hepatitis C virus (HCV) were nega-tive. On the same day, all anti-tuberculosis agents were discontinued. Eighteen days later, the original doses of ethambutol, streptomycin, levofloxacin and cycloserine were resumed. The AST and ALT levels gradually decreased thereafter. Eight days later, the patient was treated with prothionamide (250 mg 3 times daily). Unfortunately, AST and ALT increased again from 34 U/L to 286 U/L and from 39 U/L to 185 U/L, respectively, after 4 days. Prothionamide was discontinued on the fourth day of this second administration course. Nineteen days after discontinuation of the second proth-ionamide treatment, AST and ALT returned to normal levels (Figure 1).
Case 2
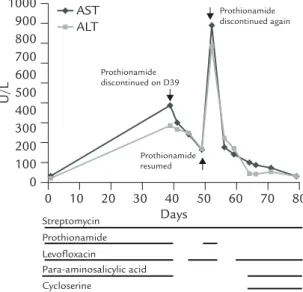
A 53-year-old man with MDR-TB, who weighed 61.2 kg received the following anti-tuberculosis multidrug regimen: levofloxacin (750 mg daily), streptomycin (1.0 g daily), para-aminosalicylic acid (2.5 g 4 times daily) and prothionamide (250 mg 3 times daily). Baseline AST, ALT, total bilirubin, blood cell counts and serum creatinine levels were within normal limits. Blood spe-cimens tested on day 39 of treatment revealed AST 433 U/L, ALT 319 U/L and total bilirubin 1.32 mg/dL. Five days prior to the office visit, the
patient described decreased appetite, general fa-tigue, and multiple joint pain. The patient de-nied a history of alcohol abuse and exposure to any other hepatotoxic drug or toxin. Tests for HBsAg and anti-hepatitis A virus IgM were nega-tive, but anti-HCV was positive. The patient had a history of hepatitis related to first-line tuberculosis agents. On the same day, all anti-tuberculosis agents were discontinued with the exception of streptomycin. Five days later, levo-floxacin (750 mg daily) was resumed. Four days later, prothionamide 250 mg three times daily was resumed. Four days later, AST and ALT levels had increased from 174 U/L to 885 U/L and from 186 U/L to 764 U/L, respectively. Prothionamide and levofloxacin were stopped immediately. Lev-ofloxacin (750 mg daily), para-aminosalicylic acid (2.5 g 4 times daily), and cycloserine (250 mg twice daily) were added sequentially to the ther-apeutic regimen, and close monitoring revealed that liver function improved gradually. Twenty-seven days after cessation of prothionamide treat-ment, AST and ALT levels returned to normal (Figure 2).
Case 3
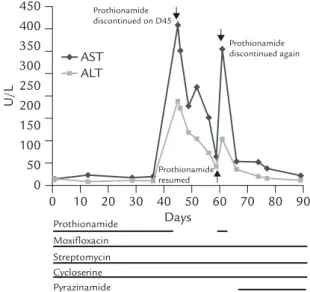
A 52-year-old man with MDR-TB, who weighed 59.2 kg received the following anti-tuberculosis multidrug regimen: moxifloxacin (400 mg daily), streptomycin (0.9 g daily), cycloserine (250 mg twice daily) and prothionamide (250 mg twice daily). Baseline AST, ALT, total bilirubin, blood cell counts and serum creatinine levels were nor-mal. Blood specimens tested on day 45 of treat-ment revealed AST 409 U/L and ALT 215 U/L. The patient made no complaints during the office visit. The patient denied a history of alcohol abuse and exposure to any other hepatotoxic drug or toxin, but he did have diabetes mellitus. Tests for HBsAg and anti-HCV were negative. On the same day, all anti-tuberculosis agents were continued with the exception of prothionamide. AST and ALT levels gradually decreased thereafter. Fifteen days later, prothionamide (250 mg twice daily) was resumed. Three days later, AST and ALT levels had increased from 73 U/L to 346 U/L and 47 U/L to 118 U/L, respectively. Prothionamide treatment was discontinued and AST and ALT lev-els returned to normal after 28 days (Figure 3). 100 90 80 70 Days 60 50 40 30 20 10 0 0 100 200 300 400 U/L 500 Prothionamidediscontinued on D28 Prothionamide discontinued again Prothionamide resumed 600 700 Rifater Ethambutol Streptomycin Levofloxacin Cycloserine Prothionamide ALT AST
Figure 1. Hepatitis developed in a 37-year-old man with
multidrug-resistant tuberculosis after 28 days of treatment with a combination of prothionamide, rifater, ethambutol, streptomycin, levofloxacin and cycloserine. Prothionamide treatment was terminated immediately. Hepatitis recurred at 4 days into a second prothionamide treatment regimen. Liver function normalized 19 days after discontinuation of prothionamide. 80 70 Days 60 50 40 30 20 10 0 0 100 200 300 400 U/L 500 Prothionamide discontinued on D39 Prothionamide discontinued again Prothionamide resumed 600 1000 700 800 900 Streptomycin Prothionamide Levofloxacin Para-aminosalicylic acid Cycloserine ALT AST
Figure 2. Hepatitis developed in a 53-year-old man with
multidrug-resistant tuberculosis after 39 days of treatment with a combination of prothionamide, streptomycin, lev-ofloxacin and para-aminosalicylic acid. Prothionamide treat-ment was terminated immediately. Hepatitis recurred at 4 days into a second prothionamide treatment regimen. Liver function normalized 27 days after discontinuation of prothionamide.
Prothionamide was discontinued permanently due to hepatitis in all three cases described.
Discussion
One of the major concerns about second-line anti-tuberculosis agents to treat MDR-TB is their potential adverse effects. Hepatitis is one of the severe adverse effects associated with MDR-TB treatment. The reported rates of hepatitis associ-ated with second-line drug treatment in patients with MDR-TB have varied considerably, and range from 1.7% to 16.8% with a median time of 3.0–8.2 months into treatment.3–7Hepatitis has been reported to be more commonly associated with ethionamide, prothionamide and para-aminosalicylic acid treatment.3,6Prothionamide has been reported as the most likely factor re-sponsible for fatal events.6However, no previous study has described in detail the clinical course of hepatitis associated with prothionamide treat-ment in patients with MDR-TB.
In our retrospective case series, seven patients developed hepatitis (15.9%) during treatment
with prothionamide and other anti-tuberculosis medications; however, prothionamide associated with hepatitis was verified here in only three (6.8%) patients. The failure of some of our pa-tients to meet our definition of prothionamide-associated hepatitis could have been because they did not received prothionamide re-challenge at a later date. Although prothionamide-associated hepatitis was confirmed in 6.8% of our patients, the possibility of prothionamide-associated hepa-titis could not be totally excluded in those patients who failed to conform to our strict definition. Prothionamide-associated hepatotoxicity has pre-viously been reported to occur in 9.0–22.7% of patients with TB and < 2% of those with MDR-TB.6,11,12 However, these earlier studies were published before the advent of the DOTS-Plus program, and the patients were typically lacking re-challenge with prothionamide, and did not conform to a strict definition for hepatitis. The fact that hepatitis was strictly defined in our patient population and that face-to-face clinical assessments were supervised under the DOTS-Plus program make our study distinct. It would be a reasonable assumption that development of hepatitis is not infrequent in MDR-TB patients who receive prothionamide treatment.
Prothionamide-associated hepatitis can occur in patients with or without chronic hepatitis B or C, and also with or without a history of hepatitis related to first-line anti-tuberculosis agents. The day of treatment when hepatitis occurred was ear-lier than in previous studies,3–7,12and it was on days 28, 39 and 45 in the three cases described here. The dose of prothionamide used for these three patients ranged from 500 mg to 750 mg daily, and the dose used in the treatment regimen did not exceed the weight-base dosing (500 mg/ day for 33–50 kg, and 750 mg/day for 51–70 kg), as recommended by the World Health Organization in 2008.2 Our cases developed prothionamide-associated hepatitis regardless of a history of hepatitis B or C. In addition, this condition oc-curred earlier during the treatment regimen than previously reported, even when patients received adequate dosing. 90 80 70 Days 60 50 40 30 20 10 0 0 50 100 150 200 U/L 250 Prothionamide discontinued on D45 Prothionamide discontinued again 300 450 350 400 Prothionamide Moxifloxacin Streptomycin Cycloserine Pyrazinamide Prothionamide resumed ALT AST
Figure 3. Hepatitis developed in a 52-year-old man with
multidrug-resistant tuberculosis after 45 days of treatment with a combination of prothionamide, moxifloxacin, strep-tomycin and cycloserine. Prothionamide was terminated immediately. Hepatitis recurred at 3 days into a second prothionamide treatment regimen. Liver function normalized 28 days after discontinuation of prothionamide.
In these three cases, hepatitis occurred shortly after re-challenge with prothionamide (4 days, 4 days and 3 days, respectively); however, a long time period was required for liver function to be normalized (19 days, 27 days and 28 days, respec-tively). These findings should serve to remind physicians to be careful when deciding on a sec-ond round of prothionamide treatment, particu-larly in patients with a suspicious history of hepatitis related to prothionamide.
In conclusion, hepatotoxic effects of prothion-amide might develop in MDR-TB patients with or without chronic hepatic liver disease, at varying times during treatment and with varying doses. Judicious follow-up of the clinical condition and close monitoring of liver function is warranted in MTB-TB patients who are receiving prothion-amide treatment.
Acknowledgments
This study was supported by the MDR-TB pro-gram of the Centers for Disease Control, Department of Health, Taiwan.
References
1. Yu MC, Wu MH, Jou R. Extensively drug-resistant tuber-culosis, Taiwan. Emerg Infect Dis 2008;14:849–50. 2. World Health Organization. Guidelines for the programmatic
management of drug-resistant tuberculosis. Emergency
update. WHO/HTM/TB/2008.402. Geneva, Switzerland: WHO, 2008.
3. Shin SS, Pasechnikov AD, Gelmanova IY, et al. Adverse reactions among patients being treated for MDR-TB in Tomsk, Russia. Int J Tuberc Lung Dis 2007;11:1314–20. 4. Torun T, Gungor G, Ozmen I, et al. Side effects associated
with the treatment of multidrug-resistant tuberculosis.
Int J Tuberc Lung Dis 2005;9:1373–7.
5. Furin JJ, Mitnick CD, Shin SS, et al. Occurrence of serious adverse effects in patients receiving community-based ther-apy for multidrug-resistant tuberculosis. Int J Tuberc Lung
Dis 2001;5:648–55.
6. Chiang CY, Enarson DA, Yu MC, et al. Outcome of pul-monary multidrug-resistant tuberculosis: a 6-yr follow-up study. Eur Respir J 2006;28:980–5.
7. Nathanson E, Gupta R, Huamani P, et al. Adverse events
in the treatment of multidrug-resistant tuberculosis: results from the DOTS-Plus initiative. Int J Tuberc Lung Dis 2004; 8:1382–4.
8. Suarez PG, Floyd K, Portocarrero J, et al. Feasibility and cost-effectiveness of standardised second-line drug treat-ment for chronic tuberculosis patients: a national cohort study in Peru. Lancet 2002;359:1980–9.
9. Goble M, Iseman MD, Madsen LA, et al. Treatment of 171 patients with pulmonary tuberculosis resistant to isoniazid and rifampin. N Engl J Med 1993;328:527–32.
10. Yew WW, Chan CK, Chau CH, et al. Outcomes of patients with multidrug-resistant pulmonary tuberculosis treated with ofloxacin/levofloxacin-containing regimens. Chest 2000; 117:744–51.
11. Anonymous. A comparison of the toxicity of prothionamide and ethionamide: a report from the research committee of the British Tuberculosis Association. Tubercle 1968;49: 125–35.
12. Somner AR, Brace AA. Changes in serum transaminase due to prothionamide. Tubercle 1967;48:137–43.
13. Saukkonen JJ, Cohn DL, Jasmer RM, et al. An official ATS statement: hepatotoxicity of antituberculosis therapy.