T
RENDS
IN
THE
M
ORTALITY
OF
C
HRONIC
O
BSTRUCTIVE
P
ULMONARY
D
ISEASE
IN
T
AIWAN
, 1981-2002
Lu-Cheng Kuo,1 Pan-Chyr Yang,1 and Sow-Hsong Kuo2
Departments of 1Internal Medicine and 2Laboratory Medicine, National Taiwan University Hospital and National Taiwan
University College of Medicine, Taipei, Taiwan.
Received: 21 May 2004 Revised: 4 August 2004 Accepted: 7 September 2004
Reprint requests and correspondence to: Dr. Sow-Hsong Kuo, Department of Laboratory Medicine, National Taiwan University Hospital. No 7, Chung-Shan South Rd, Taipei, Taiwan.
Background and Purpose: The reported prevalence, morbidity and mortality of chronic obstructive pulmonary disease (COPD) varies in different countries due to actual differences and to differences in classification criteria. This study analyzed the trends in COPD mortality and its rank among leading causes of death in Taiwan.
Methods: Using national mortality and population data, we identified COPD as a cause of death according to codes 490 (bronchitis, not specified as acute or chronic), 491 (chronic bronchitis), 492 (emphysema) as has been officially calculated previously in Taiwan, and by adding code 496 (chronic airway obstruction, not elsewhere classified) of the ninth revision of the International Classification of Diseases (ICD-9). We calculated crude, age-adjusted and age-specific mortality rates and analyzed the rank of COPD as a cause of death for the period from 1981 to 2002. Results: Crude COPD mortality was unchanged from 1981 to 1993 at 8.26 to 8.47 deaths per 100,000 population, and steadily increased thereafter to 17.88 per 100,000 in 2002. After age standardization, mortality decreased from 8.26 to 4.91 per 100,000 population from 1981 to 1993 and then increased to a peak of 7.36 per 100,000 in 1999. This increase was due to greater increase in mortality in men. COPD mortality decreased steadily throughout the study period in those younger than 65 years while in older groups, it decreased during 1981-1991 and then increased. ICD-9 code A323 (including codes 490-493) has been previously used in official mortality data for asthma, chronic bronchitis and emphysema in Taiwan without inclusion of a specific code for chronic airway obstruction. According to our analysis, this method underestimated two-thirds of real overall mortality due to COPD and asthma. By including COPD and asthma, the obstructive airway disease category increased from 11th to sixth as a cause of death in 2002. Conclusions: In Taiwan, mortality rates for COPD decreased from 1981 to 1993 and increased thereafter, which is largely attributable to increased rates in men. COPD is increasingly important and a leading cause of death in Taiwan.
Key words: Chronic obstructive pulmonary disease; Mortality; Taiwan J Formos Med Assoc 2005;104:89-93
Chronic obstructive pulmonary disease (COPD) is a disease characterized by chronic airflow limitation that is fully or partly irreversible.1,2 Previous definitions
of COPD emphasized the terms “emphysema” and “chronic bronchitis”, which are no longer used in the new definition of COPD published by the Global Initiative for Chronic Obstructive Lung Disease in 2003.2 The clinical presentations and
treatments for bronchial asthma, chronic bronchitis and emphysema are often similar and can overlap.3
Therefore, these diseases are occasionally difficult to distinguish.
The prevalence, morbidity and mortality of COPD in men and women varies in different countries.4–7 Differences in International Classification
of Diseases (ICD) codes used in various analyses
might partly account for this variation8 and the
reported data concerning COPD should be inter-preted cautiously because of these differences. For instance, in Taiwan, previous official reports of the leading causes of death used ICD code A323 for “asthma, chronic bronchitis and emphysema” to represent asthma as well as allied COPD, while code 496 for “chronic airway obstruction” is commonly used in clinical practice and official COPD statistics from other countries. Data on the trend in COPD mortality has not been reported in Taiwan. This suggests that COPD has long been misclassified in cause of mortality analyses from Taiwan. The purpose of this study was to analyze the trend in COPD mortality and to describe its real rank among the leading causes of death in Taiwan.
M
ethods
Data from the annual mortality and mid-year population data from the National Health Statistics of Taiwan9 were
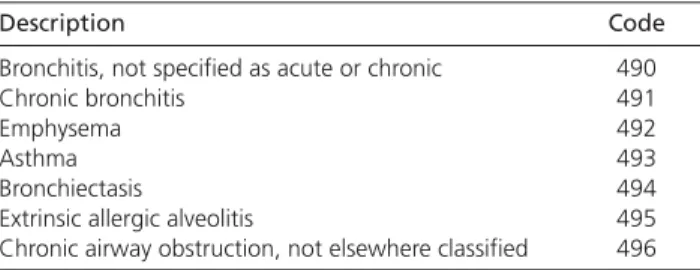
collected and analyzed using the ninth revision of the ICD (ICD-9), which has been in official use in Taiwan since 1981. According to the definition of COPD, we selected codes to match the diagnostic terms as follows: code 490 for “bronchitis, not specified as acute or chronic,” code 491 for “chronic bronchitis,” code 492 for “emphysema” and code 496 for “chronic airway obstruction, not elsewhere classified” (Table). No codes were changed during the study period.
Crude mortality rates were calculated by using the mid-year population data as denominators. COPD death rates were low among people younger than 35 years. Therefore, patients aged 34 years or younger were omitted from the subgroup analysis. The data were split into 5 age groups: 35-44, 45-54, 55-64, 65-74 and 75 years and older. Age-specific mortality rates were calculated by dividing the number of deaths by the mid-year population in the corresponding age group. Age-adjusted mortality rates were calculated using the direct standardization method based on the population of Taiwan in 1981, which was the first year of this study. All mortality rates were expressed as the number of deaths per 100,000 population per year. The mortality of asthma and allied chronic airway obstruction was calculated by including chronic airway obstruction (code 496) and with code A323 (codes 490-493) alone. The difference in the rank of leading causes of deaths obtained with these 2 different coding systems was compared.
R
esults
The crude mortality of COPD was stable from 1981 to 1993, at a rate of 8.26 to 8.47 per 100,000 population,
Table. Ninth revision of the International Classification
of Diseases codes of chronic obstructive pulmonary diseases and allied conditions.
Description Code
Bronchitis, not specified as acute or chronic 490
Chronic bronchitis 491
Emphysema 492
Asthma 493
Bronchiectasis 494
Extrinsic allergic alveolitis 495
Chronic airway obstruction, not elsewhere classified 496
1 10 100 1981 1986 1991 1996 2001 Year Mortality per 100,000 Total Male Female 1 10 100 1981 1986 1991 1996 2001 Year
Crude mortality Age-adjusted mortality
Mortality per 100,000
Total Male Female
A) B)
and it steadily increased thereafter to 17.88 per 100,000 population in 2002 (Fig. 1). A greater increase was observed in men, with a change from 12.17 to 26.20 per 100,000 population in 1993 to 2002. The male-to-female ratio was 1.5 in 1981 and 2.8 in 2002. After age standardization, the mortality rate decreased from 8.26 per 100,000 population in 1981 to 4.91 per 100,000 in 1993. It then increased to a peak of 7.36 per 100,000 in 1999 (Fig. 1). In men, it increased from 7.24 in 1993 to 11.14 in 1999. In women, mortality increased only minimally after 1993.
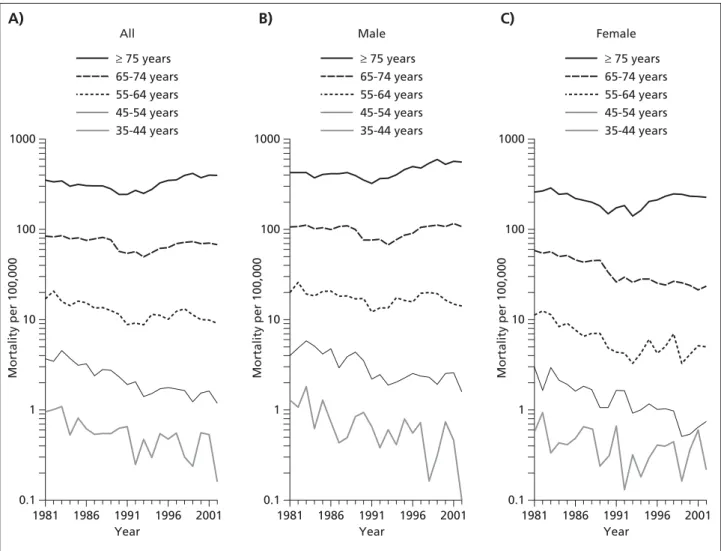
In the analysis by age groups, COPD mortality decreased steadily throughout the study period: from 0.95 to 0.16 per 100,000 in those aged 35-44 years, from 3.63 to 1.17 per 100,000 in those aged 45-54 years, and from 16.89 to 9.09 per 100,000 in those aged 55-64 years. For those aged 65-74 years, mortality remained stationary in men but decreased from 58.28 to 24.05 per 100,000 in women. In the age group of people older than 75 years, the mortality rate decreased from 1981 to 1990 (from 351 to 244
per 100,000) and then increased in following years (to 396 per 100,000 in 2002) [Fig. 2].
In Taiwan, code A323 (which includes ICD-9 codes 490-493) has been officially used to indicate asthma and “allied obstructive airway diseases” in ranking the leading causes of death. With this coding system, death rates due to asthma and “allied obstructive airway diseases” substantially decreased in the recent 2 decades: crude mortality decreased from 15.84 to 7.04 per 100,000 population, and age-adjusted mortality decreased to 3.10 per 100,000. The proportion of deaths included in code A323 relative to all-cause deaths also decreased, from 3.30% to 1.25% in the study period (Fig. 3). However, chronic airway obstruction (ICD-9 code 496), which was commonly used in practice in the recent decade, was omitted in the official data. Crude mortality attributed to code 496 was 0.59 per 100,000 in 1981 and increased rapidly to 3.31 and 15.49 per 100,000 in 1991 and 2002, respectively (Fig. 4). Code 496 accounted for more than two-thirds of all deaths due
Fig. 2. Age-specific mortality of chronic obstructive pulmonary disease in Taiwan, based on the population of Taiwan
in 1981. A) B) C) 0.1 1 10 100 1000 1981 1986 1991 1996 2001 Year All Mortality per 100,000 ≥ 75 years 65-74 years 55-64 years 45-54 years 35-44 years 0.1 1 10 100 1000 1981 1986 1991 1996 2001 Year Male Mortality per 100,000 ≥ 75 years 65-74 years 55-64 years 45-54 years 35-44 years 0.1 1 10 100 1000 1981 1986 1991 1996 2001 Year Female Mortality per 100,000 ≥ 75 years 65-74 years 55-64 years 45-54 years 35-44 years
to obstructive airway diseases. Therefore, the true mortality of obstructive airway diseases was obviously underestimated. After code 496 was included, the actual death number due to asthma and allied obstructive airway diseases increased from 1582 to 5062 per 100,000 in 2002. The proportion of these deaths relative to all-cause deaths increased from 3.42% to 3.99% in the 22-year period (Fig. 3). The asthma and allied obstructive airway diseases would have been the sixth, instead of the 11th, leading cause of death in Taiwan in 2002.
D
iscussion
Trends in COPD mortality in Taiwan showed a decreasing then increasing pattern that has not been reported in other countries.5–7,10–14 Data from
many countries show that COPD mortality rates are gradually increasing, mostly because of increasing mortality in older age groups. In younger groups, COPD mortality demonstrates a downward trend.
The crude mortality rate due to COPD and allied conditions increased in the United States from 1971 to 2000.15 The increase was greater in women than
in men. Death rates among men have remained steady since 1985, and in 2000, the number of women who died from COPD was, for the first time, higher than the number of men who died from COPD. This change is a reflection of the increase in smoking by women beginning the 1940s.15 We did not observe
this trend in our data. In Taiwan, the male-to-female ratio for death rates increased, possibly because most
0 1 2 3 4 5 1981 1986 1991 1996 2001 Year Percent
Asthma and allied obstructive airway disease (ICD-9 codes 490-493, 496) Asthma, chronic bronchitis, emphysema (ICD-9 code A323)
Fig. 3. Proportion of chronic obstructive pulmonary
dis-ease death to all-cause death between 2 different coding methods in Taiwan, 1981-2002. ICD-9 = Ninth revision of the International Classification of Diseases.
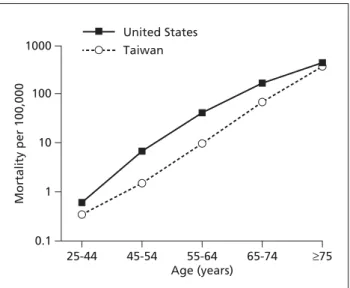
Fig. 5. Comparison of chronic obstructive pulmonary disease
mortality (ninth revision of the International Classification of Diseases codes 490, 491, 492, and 496) between Taiwan and the United States in 2000.
Fig. 4. Mortality trends in specific International Classification
of Diseases (ICD) codes in Taiwan, 1981-2002. 490 = bronchitis; 491 = chronic bronchitis; 492 = emphysema; 493 = asthma; 496 = chronic airway obstruction; All = asthma and allied obstructive airway diseases (ninth revision of the ICD codes 490-493, 496).
smokers in Taiwan are male. If the female smoking population increases in Taiwan as in the United States, their COPD mortality rate will likely increase as well. The rapid increase in overall COPD mortality in Taiwan was due to greater increase in mortality among men and older individuals. Fig. 5 shows mortality rates due to COPD (not including asthma) in specific age groups in Taiwan were similar to those from the United States in 2000.15 Except for people
younger than 45 years and those older than 75 years,
0.1 1 10 100 1000 25-44 45-54 55-64 Age (years) 65-74 ≥75 Mortality per 100,000 United States Taiwan 0 5 10 15 20 25 1981 1986 1991 1996 2001 Year Mortality per 100,000 490 491 492 493 496 All
COPD mortality in the United States was about 3-4 times that in Taiwan.
More physicians have been using the term “COPD” instead of “chronic bronchitis” or “pulmonary emphy-sema” in daily practice. We confirmed this trend, observ-ing increased use of ICD code 496 and a correspondobserv-ing proportional decrease in the use of codes 491 and 492 during the study period (Fig. 4).
Studies of mortality rely on death registration and certification. The major limitation in such studies is that the accuracy of death certification cannot be guaranteed. In a previous study in Northern Ireland, the estimated sensitivity and specificity of the registered cause of death in predicting the "true" cause of death were 69% and 70% for COPD.16 Inaccuracy
may be due to confusion in the diagnosis between chronic asthma and COPD, especially in older age groups. In another study of asthma mortality in Northern Ireland by Wright et al, the number of false-positive registrations was found to be balanced by the number of false negatives.17 This suggested that the
final registered totals might be reliable.
Exclusive use of code A323 underestimated by about two-thirds all deaths due to asthma and allied obstructive airway diseases. When the coding system used for the National Vital Statistics in Taiwan is changed to the 10th revision of the ICD in the near future, mortality due to chronic lower respiratory diseases (codes J40-J45) is expected to triple compared with previous official reports using code A323. Furthermore, COPD is likely to increase from the 11th leading cause of death to the sixth.
In conclusion, COPD mortality in Taiwan slightly decreased from 1981 to 1993 and increased there-after. COPD is a disease of increasing importance among the leading causes of death in Taiwan. The misconception of its decreasing trend is due to under-estimations of this disease due to misclassification by the current official coding system.
R
eferences
1. Standards for the diagnosis and care of patients with chronic obstructive pulmonary disease. American Thoracic Society. Am J Respir Crit Care Med 1995;152(5 Pt 2):S77-121.
2. Global Strategy for the Diagnosis, Management, and Preven-tion of Chronic Obstructive Pulmonary Disease: NHLBI/WHO Workshop Report. Global Initiative for Chronic Obstructive Lung Disease, National Institutes of Health, National Heart, Lung and Blood Institute, 2003.
3. Rennard SI: COPD: overview of definitions, epidemiology, and factors influencing its development. Chest 1998;113(Suppl): S235-41.
4. Anderson RN: Deaths: Leading causes for 2000. National Vital Statistics Report 2003;50:1-88.
5. Lacasse Y, Brooks D, Goldstein RS: Trends in the epidemiology of COPD in Canada, 1980 to 1995. COPD and Rehabilitation Committee of the Canadian Thoracic Society. Chest 1999;116: 306-13.
6. Pride NB, Soriano JB: Chronic obstructive pulmonary disease in the United Kingdom: trends in mortality, morbidity, and smoking. Curr Opin Pulm Med 2002;8:95-101.
7. Thom TJ: International comparisons in COPD mortality. Am Rev Respir Dis 1989;140(3 Pt 2):S27-34.
8. Hurd SS: International efforts directed at attacking the problem of COPD. Chest 2000;117(Suppl 2):S336-8.
9. Health and Vital Statistics Republic of China. Department of Health, the Executive Yuan, Republic of China, 1981-2002. 10. Feinleib M, Rosenberg HM, Collins JG, et al: Trends in COPD
morbidity and mortality in the United States. Am Rev Respir Dis 1989;140(3 Pt 2):S9-18.
11. Lesauskaite V: Age-related trends in mortality from COPD in Lithuania, 1989 to 1998. Chest 2003;124:90-3.
12. Manfreda J, Mao Y, Litven W: Morbidity and mortality from chronic obstructive pulmonary disease. Am Rev Respir Dis 1989; 140(3 Pt 2):S19-26.
13. Mannino DM, Brown C, Giovino GA: Obstructive lung disease deaths in the United States from 1979 through 1993. An analysis using multiple-cause mortality data. Am J Respir Crit Care Med 1997;156:814-8.
14. Rogot E, Hrubec Z: Trends in mortality from chronic obstructive pulmonary disease among U.S. veterans: 1954 to 1979. Am Rev Respir Dis 1989;140(3 Pt 2):S69-75.
15. Mannino DM, Homa DM, Akinbami LJ, et al: Chronic obstructive pulmonary disease surveillance--United States, 1971-2000. Respir Care 2002;47:1184-99.
16. Smyth ET, Wright SC, Evans AE, et al: Death from airways obstruction: accuracy of certification in Northern Ireland. Thorax 1996;51:293-7.
17. Wright SC, Evans AE, Sinnamon DG, et al: Asthma mortality and death certification in Northern Ireland. Thorax 1994;49:141-3.