行政院國家科學委員會專題研究計畫 成果報告
使用體外震波或超音波治療肌腱炎的療效機轉研究
計畫類別: 個別型計畫
計畫編號: NSC93-2314-B-002-130-
執行期間: 93 年 08 月 01 日至 94 年 07 月 31 日
執行單位: 國立臺灣大學醫學院復健科
計畫主持人: 陳文翔
共同主持人: 李百祺
計畫參與人員: 陳文翔, 馬秉模, 葉秩光
報告類型: 精簡報告
處理方式: 本計畫可公開查詢
中 華 民 國 94 年 9 月 9 日
The Generation of Inertial Cavitation in Constrained Media, in-vitro and ex-vivo
Investigations
P.M. Ma, C.K. Yeh. W.S. Chen* and M.S. Chen
National Taiwan University
Abstract
Shockwaves have been used routinely for the treatment of urolisthesis for decades. Strong evidences suggest that cavitation bubble activity plays an important role on the stone breakage. Recently, shockwaves were also shown to be effective in the treatment of certain soft tissue disorders such as tendinosis. However, whether or not cavitation occurs in tight tissue and contributes to tendon healing as well as pain relief remain unknown. In order to understand the possible physical mechanism of the shockwave therapy, we focused on searching the evidences of cavitation in tissue during the shockwave treatment, and also the determining factors of bubble generation. It was hypothesized that the shock-wave induced cavitation was constrained by the space for bubble expansion, and thus occurred more easily in vessels of larger diameters than capillaries, intercellular space and inside cells. To prove our hypothesis, a series of studies was performed to detect the presence of inertial cavitation in soft tissue blocks of various densities ex-vivo and elastic tissue phantoms embedded with vessels of different size in-vitro. We found that shock-wave induced bubble generation highly depended on the ‘porosity’ (equivalent to the perfusion status) of the ex-vivo tissue blocks. The bubble generation in muscle was substantially less than that in liver, and was undetectable in tendon. For vessel phantoms, cavitation occurred easily in vessels with diameters greater than or equal to 0.7 mm when tap water was pumped through. However, no trace of bubble signal was found in smaller vessels under the same acoustic conditions. Size threshold existed. After adding low concentrations of contrast agent (Definity®) in the flow-through fluid, cavitation threshold dropped substantially. For a vessel of 0.32 mm in diameter, bubble and signal enhancement could be easily obtained even after a single shot of shockwave. Furthermore, the presence of cavitation-induced bubbles significantly enhanced the signal-to-noise ratio of vessels in the B-mode image, comparing with the use of contrast agent alone. Concentration as low as 0.005% (v/v) could elevate the B-mode’s averaged gray level in the target area up to 76 levels, much higher than the enhancement contributed by contrast agent alone (about 2 to 3 levels in this concentration). *Corresponding author: wenshiang@ha.mc.ntu.edu.tw
Introduction
High amplitude acoustic pulses such as extracorporeal shock-wave lithotripsy (ESWL) can generate cavitation in test fluid and animal tissue. Evidences showed that cavitation occurred in human tissue during clinical ESWL. Bubbles are found in liver to appear as bright echogenic “flashes,” which intermittently give rise to sonographic shadowing at or near the shockwave focus [1]. However, it is much harder for cavitation to occur in tissue than in test fluid. It is reasonable to assume that a certain space is necessary for bubbles to expand and collapse during ultrasound insonification [2]. Free fluid has no constrain for free bubble to expand. However, tight tissue such as tendon or bone has lesser space than loose tissue such as liver or muscle. To determine the space limitation for inducing inertial cavitation, a series of experiments involving shockwave treatment and cavitation detection of (1) ex-vivo tissue of various densities (or “porosity”) and (2) transparent phantoms containing tunnels of various diameters were carried out. Ultrasound contrast agent (Definity®) was also used in
certain situations to provide cavitation nuclei in phantom experiments.
The occurrence of inertial cavitation can be monitored by two different approaches: passive cavitation detection (PCD) technique employed a hydrophone to passively receive acoustic emission generated during the collapsing stage of the inertial cavitation [3]. It provides information of the occurrence of inertial collapses, but it can not be used to determine the position where cavitation takes place. In contrast to PCD, transducers of active cavitation detection (ACD) transmit acoustic pulses and receive scattered signals from bubbles [4]. B-mode ultrasound imaging is one kind of ACD which though has low time resolution, but can be used to localize the exact position where inertial cavitation occurred. In this study, we used B-mode ultrasound to detect and quantify the existence of cavitation in phantoms and ex-vivo tissue.
Experiment Setup:
All experiments in this study were carried out in an acrylic water tank (24 cm
×
21 cm×
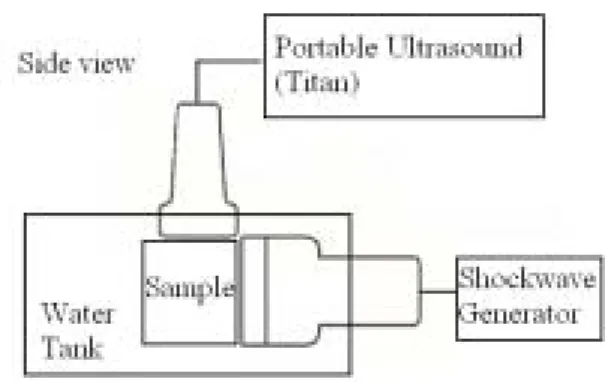
12 cm) filled with tap water. The experimental system consisted of two transducers: shockwave transducer (Piezoson 100 with a FB7 G2 probe, Richard Wolf, Knittkingen, Germany) was fixed on the side of water tank, and the B-mode scanner (Titan with a L38 probe, Sonosite, Bothell, USA) was placed on the top of the water tank. Two transducers were positioned orthogonally as shown in Fig. 1. The shockwave device was used as generation inertial cavitation, and the B-mode image was used as inertial cavitation detector. The focal size of the FB7 G2 probe for Piezoson 100 shockwave device is 1.7 mm in diameter and 6.7 mm in length, while the focal length is 20 mm from the edge plane of the probe (data from manufacturer). Shockwave was set at its highest output level (LV20, the corresponding peak negative pressure is 19.0 MPa) and the highest pulse repetition frequency (PRF 4Hz) for maximum bubble production. The B-mode L38 probe is a 38 mm linear array which has frequency range of 5-10MHz.Materials:
This study includes ex-vivo experiments
and in-vitro experiments. Several types of tissues with different “hardness” including cow eyes, cow liver, rabbit liver, pig muscle, cow Achilles tendon were tests. The transparent gel phantom used in this study was based on the poly vinyl alcohol (PVA) used for photoacoustic mammography [5]. When the phantom was forming, different diameter fishing wire was put inside to make tunnels.
In this study, ultrasound contrast agent (Definity®) was used to provide cavitation nuclei. After activating the contents of the vial in a Vialmix®, each ml of the milky white suspension
contains a maximum of 1.2
×
1010 perflutren lipid microspheres with 1.1-3.3μm in mean diameter.Experiment Procedures:
Ex-vivo experiments: The object of ex-vivo experiments was trying to search the
evidence of cavitation in tissue, and to compare the cavitation effect in tissue blocks of different “porosity”. Different tissues including eyes, liver, muscle, tendon, was arranged in “sample” zone (Fig. 1). The shockwave generator produced 100 shocks while B-mode images were taken simultaneously.
In-vitro experiments: In order to find the
main factors which constrained the cavitation took place in vivo. The tissue phantoms were embedded with tube of various diameters (1.0, 0.7, 0.5mm) before setting to make tunnels. Four different fluids including degas water (O2
concentration: 3.28±0.07mg/L), tap water (O2
concentration:5.97±0.92mg/L), 0.005% (v/v) and 0.0005% contrast agent were pumped through the tunnels each time. The shockwave generated 20 shocks while B-mode images were taken to observedif the inertial cavitation took place. For each diameter, the experiment was repeated 100 times to calculate the probability bubble generations.
Results
Ex-vivo experiments
Figure 2a shows the B-mode image of a cow eye before the shockwave treatment. The cornea and lens are at the figure’s left side. The same direction the shockwaves came. After 100 shocks, bubble signal was only found in the fluid-containing anterior and posterior chambers of the eyes (Fig. 2b, white arrow). No bubble was detected elsewhere.
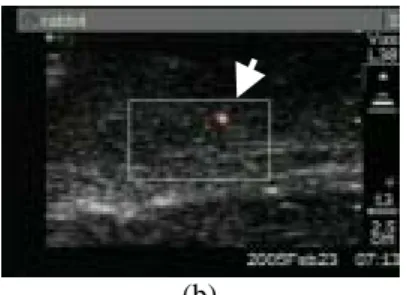
Figure 3a shows the cavitation signal inside the ex-vivo cow liver detected by the power Doppler mode (white arrow). Cavitation generated bubbles were found in big blood vessels, so as the ex-vivo rabbit liver (Fig. 3b, white arrow).
Because pig muscle had less blood vessels or spaces than the cow liver, cavitation was harder to occur. However, some signal could still be detected. Figure 4 are the B-mode images of the ex-vivo pig muscle before and after the shockwave treatment. The shockwave-generated bubbles are indicated by a white arrow.
Figure 5a is the picture of a section of cow tendon consisted of two parts, a central core and an outer ring separated by a thin space. No cavitation signal was detected in the tendon itself during a shockwave treatment. However,
Fig. 1: Experimental setup. The shockwave
transducer and the diagnostic ultrasound transducer are arranged in an orthogonal position.
prominent bubble signal was found in the intervening space (arrows in Fig. 5b & c).
In-vitro experiment
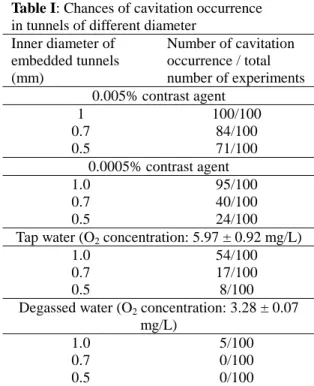
In order to understand why inertial cavitation was hard to be induced by shockwaves in tight tissue, in-vitro experiments were carried out to determine the probability of cavitation occurrence in tunnels of various diameters flowing with tap water or water mixed with diluted contrast microbubbles. The result is listed in table I. In these 12 cases, inertial cavitation was getting harder to occur for tunnels of smaller diameter or fluid containing less concentrated ultrasound contrast agent.
(a)
(b)
Fig. 3. Increased Doppler signal was seen in (a)
ex-vivo cow liver and (b) ex-vivo rabbit liver
during shockwaves treatment.
(a) (b)
Fig. 4. Small hyperechoic spot was seen in
the B-mode ultrasound image (a) during shockwaves treatment compared to the image taken before (a).
Fig. 5. (a) Transverse section of a cow’s
Achilles tendon which consists of a central core and an outer ring of tendinous tissue with a fluid-containing intervening space. (b) Before shockwave treatment, no bubble was seen. (c) During the shockwave treatment, bubbles were only seen in the intervening fluid-containing space.
(a)
(b)
Fig. 2. Sagittal section of a cow’s eye. (a)
Before shockwaves treatment, no bubble signal was found. (b) During the shockwave treatment, numerous bubbles were generated in the anterior and posterior chambers of the eyes. Shockwaves came from the left side of the pictures.
Table I: Chances of cavitation occurrence
in tunnels of different diameter Inner diameter of embedded tunnels (mm) Number of cavitation occurrence / total number of experiments 0.005% contrast agent 1 100/100 0.7 84/100 0.5 71/100 0.0005% contrast agent 1.0 95/100 0.7 40/100 0.5 24/100
Tap water (O2 concentration: 5.97 ± 0.92 mg/L)
1.0 54/100
0.7 17/100
0.5 8/100
Degassed water (O2 concentration: 3.28 ± 0.07
mg/L)
1.0 5/100
0.7 0/100
0.5 0/100
Discussions and Conclusions
In this investigation, we hypothesized that bubbles need enough space to expansion.
Ex-vivo experiments used three kinds of tissue
blocks to prove our hypothesis. In human beings, the portal vein in liver, the blood vessel in muscle, and the capillaries are in average 230, 22.5, and 15 µm in diameter, respectively. The result of ex-vivo experiments showed that cavitation could take place in ex-vivo tissue, and bubbles’ quantity depended on the extent of porosity and the size of existing cavities. In order to determine why space or porosity changed the amount and the possibility of bubble generation in ex-vivo tissue block, in-vitro experiment in PVA phantom was performed.
At first, we suggested that the limitation of bubble generation in tissue was due to the space constraint during bubble expansion. That is, bubble could not expand to its maximal diameter during shockwave treatment as it did in free fluid. In theory, bubbles can expansion till a size of 0.39 mm in radius by the shockwave pressure we used (calculated by Gilmore equation) [6]. Most of the tunnels we created in phantoms were smaller than 0.78 mm in diameter. Accordingly, bubble expansion may be limited, but inertial cavitation would still occur.
In ex-vivo experiments, the area of
hyperechoic change, that is, area of bubble generation, was getting smaller and lesser in tighter tissue. In vessel containing different size of vessels, inertial cavitation was less likely to occur in vessels of smaller diameters. However, after supplying the tunnels with microbubbles,
inertial cavitation could still be induced, e.g., 0.5 mm in Table 1. On the contrary, probability of cavitation’s occurrence in degassed water dropped dramatically. Therefore, the constraint in the occurrence of cavitation was probably not because bubble could not expand freely, but because the quantity of cavitation nuclei in the focal region decreased. That is, the number of cavitation nuclei in the shockwave focal zone determined the occurrence of inertial cavitation. In normal in-vivo conditions, the small vessels or capillaries contained few nuclei and thus the cavitation threshold was high. Contrast agent provided microbubbles to act as cavitation nuclei which substantially low the threshold. From our experimental results, we speculated that inertial cavitation was very hard to occur in vivo without the presence of UCA.
Refeences
[1] Forer, L. E., Davros, W. J., Goldberg, J., al Kawas, F., Garra, B. S., Hayes, W., and Zeman, R. K., "Hepatic cavitation. A marker of transient hepatocellular injury during biliary lithotripsy," Dig. Dis. Sci., vol. 37, no. 10, pp. 1510-1516, Oct. 1992. [2] Zhong, P., Zhou, Y., and Zhu, S.,
"Dynamics of bubble oscillation in constrained media and mechanisms of vessel rupture in SWL," Ultrasound Med.
Biol., vol. 27, no. 1, pp. 119-134, Jan.
2001.
[3] Chen, W. S., Brayman, A. A., Matula, T. J., and Crum, L. A., "Inertial cavitation dose and hemolysis produced in-vitro with or without Optison," Ultrasound Med. Biol., vol. 29, no. 5, pp. 725-737, May. 2003. [4] Chang, P. P., Chen, W. S., Mourad, P. D.,
Poliachik, S. L., and Crum, L. A., "Thresholds for inertial cavitation in albunex suspensions under pulsed ultrasound conditions," IEEE Trans.
Ultrason. Ferroelectr. Freq. Control, vol.
48, no. 1, pp. 161-170, Jan. 2001.
[5] Kharine, A., Manohar, S., Seeton, R., Kolkman, R. G., Bolt, R. A., Steenbergen, W., and de Mul, F. F., "Poly(vinyl alcohol) gels for use as tissue phantoms in photoacoustic mammography," Phys. Med.
Biol., vol. 48, no. 3, pp. 357-370, Feb.
2003.
[6] Church, C. C., "A theoretical study of cavitation generated by an extracorporeal shock wave lithotripter," J. Acoust. Soc.
Am., vol. 86, no. 1, pp. 215-227, Jul.