The Prevalence of Four Common Pathomechanical Foot Deformities in Primary School Students in Taichung County
9
0
0
全文
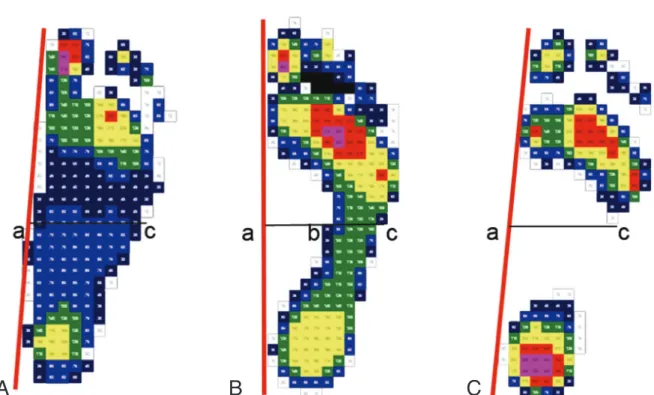
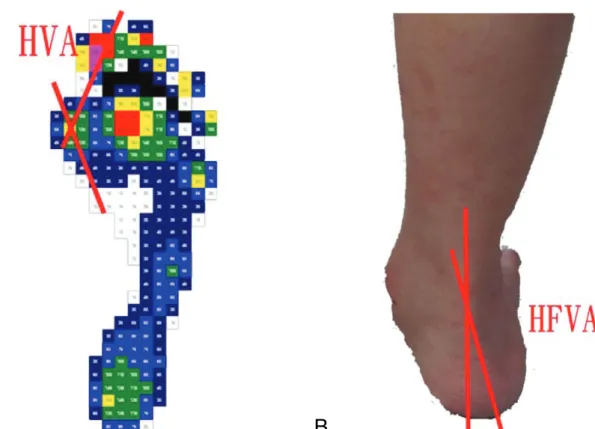
(2) 2. foot deformities encountered in pediatric orthopedic and rehabilitation practice. It is important to make an early diagnosis of these deformities so that treatment can begin as soon as possible. Flexible flatfoot [1-6] is defined as the postural appearance of the foot, with a depressed medial longitudinal arch and a pronated subtalar joint under weight bearing conditions. Flexible flatfoot rarely causes disability, and asymptomatic children are brought to clinics by concerned parents because of the common layman perception that flatfoot will be associated with pain in adulthood. High-arch foot [7,8] is the opposite of flatfoot. It is much less common than flatfoot and more likely to be associated with an abnormal orthopedic or neurological condition. Unlike flexible flatfoot, high-arch foot tends to be painful because more stress is placed on the section of the foot between the ankle and the toes, making it difficult to wear shoes. Hindfoot valgus [9] refers to increased lateral angulation of the heel relative to the longitudinal axis of the tibia. Hallux valgus [10] is defined as increased lateral angulation of the proximal phalanx of the great toe with respect to the first metatarsal. There is often an associated medial soft tissue prominence (bunion) overlying the first metatarsalphalangeal joint. A patient may present with a nonacute onset of deep or sharp pain in the first metatarsalphalangeal joint during ambulation, with exacerbation during particular activities. Patients may also describe aching pain in the metatarsal head secondary to shoe irritation, which is relieved when the shoe is removed. Although the four above-mentioned foot deformities are common and account for a significant number of office visits to foot and ankle specialists, relatively few studies have been conducted, especially in Chinese, and much of the information consists of empirical data based on patient observations. The prevalence profiles of flexible flatfoot, high-arch foot, hindfoot valgus and hallux valgus have not been studied in growing children. Therefore, the authors conducted this study to assess the overall prevalence of these four common. Common Foot Deformities in Primary Schoolchildren. pathomechanical foot deformities in a population of schoolchildren in Taichung County and to assess the prevalence profile in boys and girls of different ages. MATERIALS AND METHODS Subjects. We surveyed the static and dynamic footprints of 18,006 students (8883 boys and 9123 girls) from 14 primary schools in Taichung County, Taiwan, during the period February to July, 2006. The students ranged in age from 6 to 12 years. The age range in each grade was as follows: 6 to 7 years in the first grade; 7 to 8 years in the second grade; 8 to 9 years in the third grade; 9 to 10 years in the fourth grade; 10 to 11 years in the fifth grade; and 11 to 12 years in the sixth grade. None of them had a history of specific medical or orthopedic problems. Methods. Foot pressure data were collected by the Novel EMED platform system (AT-2). The EMED-AT system is a pedography measurement platform with calibrated capacitive sensors that can measure and record foot pressure in static and dynamic mode. Data from three trials were collected bilaterally with subjects placing all of their bodyweight on the platform. From each of the footprints we measured the arch index and the hallux valgus angle. The footprints were classified as normal, high-arched or flat (Fig. 1). If the width of the instep at its widest part was less than 1cm, the foot was considered flatfoot. If the width of the footprint at its narrowest part was less than 1cm, the arch was considered high. All other footprints were considered normal [11]. Hallux valgus is normally defined on X-ray images as a metatarsal-phalangeal angle of greater than 15 degrees; however, the authors tried to define the hallux valgus angle (Fig. 2A) using footprint analysis to protect the children from unnecessary X-ray exposure. The hallux valgus angle was defined as the angle formed by the intersection of the lines along the long axis of the proximal phalanx and the first metatarsus. The normal angle should be less than 15 degrees..
(3) Li-Wei Chou, et al.. A. 3. B. C. Fig. 1. Method of grading footprints. A: If the width of the instep (ab) at its widest part was less than 1 cm, the foot was considered flatfoot. B: All other footprints were considered normal foot. C: If the width of the footprint at its narrowest part (bc) was less than 1 cm, it was considered high-arch foot.. Children were asked to stand and march in place 4 or 5 times on the pressure platform with their backs toward the examiner [12]. In the weight-bearing standing position, the distal aspect of the bisection of the Achilles tendon extending down the hindfoot laterally deviates to form a valgus angle with the upper portion of the Achilles tendon (Fig. 2B). A goniometer is placed on the hindfoot valgus angle, which is formed by the upper Achilles tendon and the distal extension of the rearfoot. It is considered abnormal if the angle is greater than 7 degrees [13]. The protocol of this study was approved by the Institutional Review Board of the China Medical University Hospital, Taichung, Taiwan. Statistical analysis. Correspondence analysis [14,15] is an exploratory, multivariate descriptive analytical technique. As opposed to traditional hypothesis testing designed to verify a priori hypotheses about relations between variables, exploratory data analysis is used to identify systematic relations between variables when there are no (or rather incomplete) priori expectations as to the. nature of those relations. Correspondence analysis markedly simplifies complex data and provides a detailed description of practically all information in the data, yielding a simple, yet exhaustive analysis. The significance of association tested by the chi-square test provides no information as to the significant individual associations between two or more categorical variables. In contrast, correspondence analysis not only shows that a relationship exists, but also shows how the variables are related. Another important feature is the graphical display of row and column points in biplots, which can help in detecting structural relationships among the variable categories and objects. The data obtained from the survey are shown in Table 1. A joint-space representation of grade, sex and the foot deformities was developed by correspondence analysis. Table 2 is a threeway classification of the 3 variables, foot deformities, grade, and sex, from which a matrix (4 foot deformities 6 grades 2 sexes) with a total of 48 cells was created. The data were transformed into a two-way matrix by combining.
(4) 4. A. Common Foot Deformities in Primary Schoolchildren. B. Fig. 2. A: Hallux valgus angle (HVA) is formed by the intersection of the lines along the long axis of the proximal phalanx and the first metatarsus. An angle larger than 15 degrees indicates Hallux valgus. B: The distal aspect of the bisection of the Achilles tendon extending down the hindfoot deviates laterally to form a hindfoot valgus angle (HFVA). It is considered hinedfoot valgus if the HFVA is greater than 7 degrees.. Table 1. Prevalence of the four common foot deformities in 18,006 primary school students (8883 boys and 9123 girls), in Taichung county, Taiwan, 2006 Boys Girls Total Type of foot deformities n (%) n (%) n (%) Flexible flatfoot 1593 (8.85) 2499 (13.88) 906 (5.03) High-arch foot 84 (0.47) 237 ( 1.32) 153 (0.85) Hallux valgus 46 (0.26) 252 ( 1.40) 206 (1.14) Hindfoot valgus 346 (1.92) 599 ( 3.33) 253 (1.41). two variables (grade and sex) into one interactive variable. The 4 12 matrix comprising the type of foot deformity and sex combined with grade was entered into a simple correspondence program. The four foot deformities along with the groups (grade sex) were scaled. Categories with similar distributions will be represented as points that are close in space, and categories that have very dissimilar distributions will be positioned apart. The geometrical display (graphical display) shown in Fig. 3 thus serves to facilitate description of the authors’ results. The prevalence profile of the foot deformities was. scaled, giving X and Y coordinates for each point for the three variables. RESULTS. The correspondence analysis resulted in a total of three dimensions, of which the first two explain as much as 98% of the total variance. The authors chose the two-dimensional solution. The first dimension is dominant, accounting for 90% of the variance. Masses comprise the relative frequency of the marginal row and column frequency in percentage form (row and column masses) of the.
(5) Li-Wei Chou, et al.. 5. Table 2. Major foot deformities in 3587 primary schoolchildren of different grades Boys Total Girls Mass* Foot deformities 1st 2nd 3rd 4th 5th 6th 1st 2nd 3rd 4th 5th 6th FF 393 340 257 215 222 166 196 181 146 158 132 93 2499 0.697 HAF 4 23 17 30 15 29 18 25 22 23 2 29 237 0.006 HV 6 2 3 8 7 25 14 34 10 67 7 69 252 0.070 HFV 70 75 34 50 51 41 48 51 52 43 50 34 599 0.167 Total 473 440 330 295 306 225 250 269 241 268 265 225 3587 1 Mass* 0.132 0.123 0.092 0.082 0.085 0.063 0.070 0.075 0.067 0.080 0.074 0.063 1 FF = flexible flatfoot; HAF = high-arch foot; HV = hallux valgus; HFV = hindfoot valgus.*Masses are composed relative frequency of marginal row and column frequency in percentage form (row and column mass) of the total cases.. Fig. 3. The graph shows the relative positions of two sets of points, providing a picture of which foot deformities and which age groups are related. Dimension 1 is an age-specific deformity dimension. The points representing all the boy groups (B1 to B6), and the G1 girl group form a cluster near the centroid and closed to flatfoot and hindfoot valgus. This indicates that flatfoot and hindfoot valgus are closely associated foot deformities and related to all boy and younger girl groups, and hallux valgus is related to the older girl group. Dimension 2 is dominated by the points high-arch foot and hallux valgus. The low mass values and the large distance from the centroid indicate that there are fewer cases. The prevalence of high-arch, and hallux valgus is higher in the older girl groups. (B = boy; G = girl; FF = flexible flatfoot; HAF = high-arch foot; HV = hallux valgus; HFV = hindfoot valgus. 1 to 6 indicated grade). total number of cases (3587) as shown in Table 2. The masses are a measure of the importance of the point profile in the analysis. The high mass value of flexible flatfoot shows that most of the participants have flexible flatfoot. The higher mass values in boys in all grades and in the youngest girls indicate that these grades are associated with most cases of flexible flatfoot. The lower mass values of hindfoot valgus indicate that, although there is an association between hindfoot valgus and the above grade-sex groups, the prevalence of hallux valgus is not as high as that of flexible flatfoot. Furthermore, it can be. seen that flexible flatfoot and hindfoot valgus are the most prevalent deformities, while hallux valgus is the least prevalent. Figure 3 is a graphic presentation of the results for the two dimensions and shows the relative positions of two sets of points, providing a picture of which foot deformities and which grades are related. The proximity of flexible flatfoot and hindfoot valgus indicates a close association between the two foot abnormalities. In addition, the configuration shows that the points representing all the boy groups (1st to 6th grade) and first-grade girls form a cluster near the origin (centroid). The figure also shows that this gradesex group is positioned close to flexible flatfoot and hindfoot valgus, indicating that they are closely associated foot deformities. It is reasonable to interpret dimension 1 as an age-specific deformity dimension. As shown in Fig. 3, the grade groups, especially for girls, are ranked by increasing grade along the first dimension. Furthermore, hallux valgus and flexible flatfoot contribute as much as 92% to the variance of the first dimension. In the case of the column profile (age and sex), the greatest contribution to the first dimension (87%) is made by the younger boys and older girls. Examination of the configuration reveals that flexible flatfoot and hindfoot valgus are related to the group of younger boys, and hallux valgus is related to the group of older girls. These results indicate an interaction between the three variables; that is, the relationship between type of foot deformity and age differs between boys and girls. Dimension 2 is dominated by the points of high-arch foot and hallux valgus. They explain 86.
(6) 6. Common Foot Deformities in Primary Schoolchildren. percent of the variance of dimension 2. As far as the other set of points is concerned, it is seen that older girls dominate this dimension (70% of the variance). If the contributions of points to dimensions are compared with the configuration, it is seen that the prevalence of high-arch foot and hallux valgus is high among older girls. However, the low mass values and the large distance from the centroid indicate that there are fewer children with high-arch foot and hallux valgus. This analysis further shows that the relationship between type of foot deformity (high-arch foot and hallux valgus) and age differs between boys and girls. The proximity of the points between the column (high-arch foot and hallux valgus) and the row (grade sex) indicates that the association between these two foot deformities and the points (grade sex) is not as strong as the association between the other deformities (flexible flatfoot and hindfoot valgus) and the points (grade sex). DISCUSSION. The most accurate method of measuring the medial longitudinal arch of the foot is debated by many physicians. Various techniques are used to assess the medial arch height, although radiographic measurements and footprint analysis are the most common methods [16-18]. In this study, we used footprint analysis to screen foot deformities because it is a simple, readily available, low-cost, and noninvasive technique. It also does not have the potential hazardous effects of X-rays. Abnormalities of the foot often arise from abnormal structural support. An imbalance in the forces, including weakness of the muscular, ligamentous, or bony arch supporting structures will lead to collapse of the arch [6]. Bresnahan [5] states that intrauterine forces and fetal foot position initially create the abnormal bony relationships between anatomically normal bones characteristic of flatfoot disorders. The active muscular force balance between opposing muscle groups is distorted, causing abnormal bony relationships and disturbed muscular mechanical advantage, which exerts its influence immediately at the point of heel contact in the gait cycle. Therefore, the foot and posterior talocalcaneal. joint are dorsiflexed relative to the supporting surface, leading to predominance of motion execution in the transverse body plane. Kernozek and Ricard [19] investigated the relationship between foot placement angle, arch type, and rearfoot motion during running. They found that foot placement angle was the best single predictor of total rearfoot motion. Less abduction was associated with more total rearfoot motion. Arch type exhibited a quadratic relationship with total rearfoot motion. In this general survey of the prevalence profile of foot deformities in primary school students, we chose footprint analysis as the major evaluation tool. Although we were unable to show that flexible flatfoot is a result or a cause of hallux valgus, our results indicate that flexible flatfoot and hindfoot valgus are interrelated musculoskeletal deformities. The arch of the foot changes significantly throughout life. Staheli and colleagues found that the medial longitudinal arch has an undulating pattern according to age and arch index [20]. Volpon [21] stated that the feet grow most rapidly up to 3 years of age. From birth up to 2 years of age, there is a higher incidence of flatfoot. Rapid progression of plantar arch development was observed between 2 and 6 years of age. Rose stated that the critical age for development of the foot arch is 6 years, and consequently, if the prevalence of flat feet is evaluated before this age, the finding will overestimate the problem [3]. The overall prevalence of flexible flatfoot in the population studied by Bordin et al [22] was found to be 16.4%; however, the sex-specific prevalence was 18.1% among boys and 14.6 among girls. Lin et al [23] performed a crosssectional study to elucidate the correlating factors and clinical significance of flexible flatfoot in preschool children in Taiwan. In their study of 377 preschool children (201 boys, 176 girls), ranging in age from 2 to 6 years, 57% of children at 2 and 3 years of age were noted to have moderate or severe flexible flatfoot; however, the prevalence decreased with age, dropping to 40% at ages 3 and 4, to 28% at ages 4 and 5, and to 21% at ages 5 and 6. However, no studies have investigated the prevalence in older children. Furthermore, the relationship between age and.
(7) Li-Wei Chou, et al.. other foot deformities (high-arch foot, hindfoot valgus and hallux valgus) have not been studied in Chinese. In previous studies, investigators have demonstrated a relationship between flexible flatfoot and age in boys and girls. Cheng et al [24] found that foot length and width increase linearly from the age of 3 years until 12 years in girls and 15 years in boys. Volpon [21] found that from age 3 onward, the feet maintained an almost constant growth rate in both sexes until the age of 12 years, when girls’ feet stopped growing and boys’ feet exhibited further growth. Our results are consistent with these studies and further demonstrate that flexible flatfoot and hindfoot valgus are relatively more frequent among all boys and the youngest girls. The authors also found that hallux valgus is related to older age among girls. Flexible flatfoot and hindfoot valgus are the most prevalent foot deformities in primary school students in Taiwan. Many of the children in this study presented with hindfoot valgus but the relative prevalence of that foot deformity was not as high as that of flexible flatfoot. Hallux valgus was found to be the most deviating profile. The relationship between type of foot deformity (high-arch foot and hallux valgus) and age differed between boys and girls. Girls in grades 5 and 6 experienced relatively more high-arch foot and hallux valgus than boys in grades 1 to 6. The clinical diagnosis of flatfoot is based on a valgus position of the heel and a poor formation of the foot arch. Pfeiffer et al [25] demonstrate that the development of the medial arch of the foot in preschool-aged children is influenced by three factors: age, gender and weight. Rao et al [11] found that flexible flatfoot was much more frequent in hypermobile children, whereas body mass index did not differ significantly between shod and unshod children. El et al [26] confirmed that flexible flatfoot and the hypermobility are developmental profiles. In this study, technical problems precluded the collecting of body mass index data from all of the 18 006 children; therefore, we could not evaluate the relationship between the prevalence of flatfoot and weight or body mass index.. 7. Management of all musculoskeletal foot problems is based on understanding the causes and the natural course of the condition and on the effectiveness of various treatment modalities. Treatment begins with conservative care, including parental reassurance, observation, and possibly arch supports. For resistant cases in which nonsurgical management has failed, operative correction is suggested. Buerk et al [27] believe that there is no role for surgery in asymptomatic flexible flatfoot. Although parents are often concerned about pediatric foot problems, such as flexible flatfoot, high-arch foot, hallux valgus and hindfoot valgus, the child is usually found to be asymptomatic, and no treatment is indicated. The examining physician must rule out other conditions that do require treatment, such as congenital vertical talus, tarsal coalition, and skew-foot [2]. In most instances, the best treatment is simply taking enough time to convince the family that no treatment is necessary. Flexible flatfoot with tight heel cords may become symptomatic and can be addressed with a stretching program [28,29]. Surgical intervention for flexible flatfoot is reserved for patients who have persistent localized symptoms despite conservative care. Rigid or pathologic flatfoot has multiple etiologies and many patients will require treatment to alleviate symptoms or improve function. The four common pathomechanical foot deformities evaluated in this study rarely cause disability, but often are of major concern to the parents. Although many causes exist, a careful history and a stepwise approach to the physical examination will provide the examiner with sufficient information to make a correct diagnosis and provide appropriate treatment. In conclusion, we have shown for the first time the prevalence profile of the common pathomechanical foot deformities in primary school students in Taiwan. Our observations provide evidence that flexible flatfoot and hindfoot valgus are relatively more frequent in boys of all ages and in young girls. Furthermore, we found that high-arch foot and hallux valgus are more prevalent in older girls. Additional larger-scale studies are needed further investigate this important finding..
(8) 8. Common Foot Deformities in Primary Schoolchildren. ACKNOWLEDGMENTS. The authors would like to thank the China Medical University Hospital, Taichung, Taiwan for financial support (DMR-94-069), and to thank Chih-Sheng Chang, Chih-Yung Chiang and all schoolmasters and nurses in the 14 primary schools for their help in composing materials for this presentation. REFERENCES 1. Rose GK, Welton EA, Marshall T. The diagnosis of flat foot in the child. J Bone Joint Surg Br 1985;67:718. 2. Sullivan JA. Pediatric flatfoot: evaluation and management. J Am Acad Orthop Surg 1999;7:4453. 3. Rose GK. Flat feet in children. Br Med J 1990;301: 1330-1. 4. Kim HW, Weinstein SL. Flatfoot in children: Differential diagnosis and management. Curr Orthop 2000;14:441-7. 5. Bresnahan P. Flatfoot deformity pathogenesis. A trilogy. Clin Podiatr Med Surg 2000;17:505-12. 6. Van Boerum DH, Sangeorzan BJ. Biomechanics and pathophysiology of flat foot. Foot Ankle Clin 2003;8: 419-30. 7. Schwend RM, Drennan JC. Cavus foot deformity in children. J Am Acad Orthop Surg 2003;11:201-11. 8. Williams DS, Davis I, Scholz JP, et al. High-arched runners exhibit increased leg stiffness compared to low-arched runners. Foot Ankle Clin 2003;8:419-30. 9. Duckworth T. The hindfoot and its relation to rotational deformities of the forefoot. Clin Orthop Relat Res 1983;177:39-48. 10. Coughlin MJ, Roger A, Mann Award. Juvenile hallux valgus: etiology and treatment. Foot Ankle Int 1995; 16:682. 11. Rao UB, Joseph B. The influence of footwear on the prevalence of flat foot--a survey of 2300 Children. J Bone Joint Surg Br 1992;74-B:525-7. 12. Sobel E, Levitz S, Caselli M, et al. Natural history of the rearfoot angle: preliminary values in 150 children. Foot Ankle Int 1999;20:119-25. 13. Haight HJ, Dahm DL, Smith J, et al. Measuring standing hindfoot alignment: reliability of goniometric and visual measurements. Arch Phys Med Rehabil 2005;86:571-5. 14. Panagiotakos DB, Pitsavos C. Interpretation of Epidemiological Data Using Multiple Correspondence. Analysis and Log-linear Models. J Data Sci 2004;2: 75-86. 15. Beh EJ. A Bibliography of the Theory and Application of Correspondence Analysis. School of Quantitative Methods and Mathematical Sciences, University of Western Sydney, Australia. 2004. 16. Igbigbi PS, Msamati BC. The footprint ratio as a predictor of pes planus: a study of indigenous Malawians. J Foot Ankle Surg 2002;41:394-7. 17. Igbigbi PS, Msamati BC, Shariff MB. Arch index as a predictor of pes planus: a comparative study of indigenous Kenyans and Tanzanians. J Am Podiatr Med Assoc 2005;95:273-6. 18.Kanatli U, Yetkin H, Cila E. Footprint and radiographic analysis of the feet. J Pediatr Orthop 2001;21:225-8. 19. Kernozek TW, Ricard MD. Foot placement angle and arch type: effect on rearfoot motion. Arch Phys Med Rehabil 1990;71:988-91. 20. Staheli LT, Chew DE, Corbett M. The longitudinal arch. J Bone Joint Surg Am 1987;69:426-8. 21. Volpon JB. Footprint analysis during the growth period. J Pediatr Orthop 1994;14:83-5. 22. Bordin D, De Giorgi G, Mazzocco G, et al. Flat and cavus foot, indexes of obesity and overweight in a population of primary-school children. Minerva Pediatr 2001;53:7-13. 23. Lin CJ, Lai KA, Kuan TS, et al. Correlating factors and clinical significance of flexible flatfoot in preschool Children. J Pediatr Orthop 2001: 21:37882. 24. Cheng JC, Leung SS, Leung AK, et al. Change of foot size with weightbearing. A study of 2829 children 3 to 18 years of age. Clin Orthop Relat Res 1997;342:12331. 25. Pfeiffer M, Kotz R, Ledl T, et al. Prevalence of flat foot in preschool-aged children. Pediatrics 2006;118: 634-9. 26. El O, Akcali O, Kosay C, et al. Flexible flatfoot and related factors in primary school children a report of a screening study. Rheumatol Int 2006;26:1050-3. 27. Buerk A, Albert MC. Advances in pediatric foot and ankle treatment. Current Opinion in Orthopaedics 2001;12:437-42. 28. Cappello T, Song KM. Determining treatment of flatfeet in children. Curr Opin Pediatr 1998;10:77-81. 29. García-Rodríguez A, Martín-Jiménez F, Carnero-Varo M, et al. Flexible flat feet in children: a real problem? Pediatrics 1999;103:84-6..
(9) 9. 1,2. 1,2. 3. 1. 1,4. 1. 1. 3. 4. 5,6. 1. 2. 5. 6. /. 18,006. (8883. 9123. ). 13.88% 3.33%. 1.40%. 2009;14:1-9. 111. 105. 2008. 4. 2008. 10. 2 7. 2008. 8. 22. 1.32%.
(10)
數據

相關文件
An additional senior teacher post, to be offset by a post in the rank of CM or APSM as appropriate, is provided to each primary special school/special school with
堅毅 尊重他人 責任感 國民身份認同 承擔精神 誠信
* School Survey 2017.. 1) Separate examination papers for the compulsory part of the two strands, with common questions set in Papers 1A & 1B for the common topics in
5.1.1 This chapter presents the views of businesses collected from the business survey, 12 including on the number of staff currently recruited or relocated or planned to recruit
On top of the overall students’ attainment rates of a school in Chinese Language, English Language and Mathematics (starting from 2014, individual primary schools are no
In light of the unique context and different student needs in every school, and the common goal of fostering students’ learning abilities, the EDB has been encouraging schools
Forming the initial ideas as the base of the composition activity, as well as the fundamental
Based on a sample of 98 sixth-grade students from a primary school in Changhua County, this study applies the K-means cluster analysis to explore the index factors of the
