評值南部某醫院的出院準備服務
顧雅利 郭世明 郭心怡
摘要
自從 1993 年台灣老人已經超過世界衛生組織所定 7%老人國的標準,因此長 期照護於台灣非常重要,而出院準備又為長期照護之一部份,可確認出需要持續 照護之高危險群。高品質的出院準備計畫能夠於出院前訓練患者及家屬自我照顧 的技巧,以減少患者的再入院率,和降低醫療成本。本研究即評值南部某醫院出 院準備計畫,二手資料分析以回溯方式檢視 2002 年 1 月至 2003 年 6 月間 346 位 個案的出院準備計畫,以瞭解其健康狀況和目前情況,及 37 位個案的自我照顧 能力和家庭支持功能。成果評值依照南部某大學醫院的評估工具,包括患者的健 康狀況、目前情況、自我照顧能力、和家庭支持功能。研究結果顯示個案的健康 狀況於一年間呈現顯著進步,且此進步不受性別和照顧者人數的影響。此外,內 容分析患者目前的情況,結果如下:57.4%穩定續追蹤,15.1%失去連絡,11.3 %死亡,8.7%再度入院,7.5%轉至私人醫院、公共衛生單位、護理之家、或居家 照護。再者,37 位個案的進食、如廁、沐浴、移動、用藥、疾病瞭解、焦慮、 和溝通的自我照顧能力與家庭支持功能於一年間呈現顯著的進步,且此進步不受 性別和照顧者人數的影響,僅患者的大、小便控制和穿衣自我照護能力無顯著地 進步。 關鍵字:出院準備、成效評值 1 2 3 2010 3 2 2010 12 10 2010 12 30壹、Introduction
Growing life expectancy
worldwide has increased the importance of long-term care. Since 1993, the population of elders in Taiwan has increased by over 7% and fit the WHO criteria for an aging country. According to the statistics of the Department of Health Executive Yuan (2003), the elderly population over 65 years old in Taiwan has reached 2,087,734,
comprising 9.2% of the total population. In 2050, the population of the elderly in Taiwan as a percentage of the total population is anticipated to be 29.8%. Increasing health problems accompany the rise in the proportion of elderly in the population. According to the Department of Statistics, Ministry of Interior (2003), 55.7% of elders experienced chronic illness, and the health status of half of the elderly was rated poor, while 49.7% of these could not practice ADL. Long-term care can supply elderly continuing and complete services. Long-term care services not only can provide for those who have chronic illness, but can also shorten hospitalization time and therefore control the medical cost (Wu, et al, 2001).
Discharge planning is the essential element of long-term care. Discharge planning attempts to forecast potential health problems and care needs for
patients before discharge and design a health care plan as well as offer appropriate transferred facilities early (Pan, 2000). Lin and Chang (2004) identified the importance of discharge planning for 103 elders one year after hip fracture surgery because of
inefficient ADL and IADL. The benefit of discharge panning lies in increased the satisfaction of nursing service and reduced hospitalization and provision of good continuing care, thus lowering re-hospitalization and medical costs (Chiu, 1999; Hou, Hollenberg, Charlson, 2001; Liao, Shao, Lee, Hsu, 2000), as well as Saltvedt, Opdahl, Fayers, Kaasa, and Sletvold (2002) reported after following up with three monthly surveys that mortality in the group which
practiced discharge planning was lower than the one that did not.
貳、Purpose of Study
The purpose of this study was to evaluate the discharge planning. Secondary data analysis was applied to examine 346 cases in discharge
planning retrospectively from January, 2002 to June, 2003 in a Southern University Hospital to understand their health status and current situation, as well as the self-care abilities and family support function of 37 cases. The
outcomes-evaluated criteria included the patient’s health status, current situation,
self-care ability, and family support function. Health status was defined as the numbers of Tracheotomy, N-G tube, Foley tube, PCN tube as well as wounds and decubitous ulcers patients have had in their bodies. Current situation was defined as the patients’ status as stable or follow up, re-hospitalized, transferred to other units, dead, or missing.
Self-care abilities were defined as the capabilities of feeding, toileting, bladder and bowel control, bathing, dressing, moving, medication, illness awareness, anxiety, and communication. Family support function was defined as the abilities of family members to take care of patients by their feeding, toileting, bladder and bowel control, bathing, clothing, moving, medication, illness awareness, anxiety, and communication.
參、Literature Review
As numbers of aging and
chronically ill patients burgeoned, the Department of Health Executive Yuan (1994) began discharge planning to lower hospitalization time and medical costs (Wu, 2001). Discharge planning aims to integrate medical, social, and financial resources to attain high quality care based on patients’ situations and welfare status (Kuo, Hsu, Chen, Lee, Chang, 2000). The six groups of working content in discharge planning included cases screening, designing and
conducting the care plan, monitoring and evaluating the quality of care, multidisciplinary service and
coordination, utilizing and managing of resources, and quality of referred agency (Yang, Shiao, Chen, 2004). Evaluation of discharge planning is measured by using criteria as patients and family satisfaction, days of hospitalization, totals of
re-hospitalization, and resources for discharge planning as criteria (Kuo, et al, 2000; Liao, et al, 2000). Taipei Veterans General Hospital commenced training case managers for discharge planning in 2001. Case managers consulted 2,792 patients for discharge planning and confirmed that average of
hospitalization days dropped from 10.38 in 2000 to 10.15 in 2001, although beds-transferred rate rose from 2.47 in 2000 to 2.55 in 2001 (Yang and Yin, 2002). Pan (2000) surveyed 27,724 patients for discharge planning in Mackay Memorial Hospital from 1996 to 1999 and disclosed that the average numbers of transfer cases from 1996 to 1999 had risen from 11.2 persons to 41.6 persons for per month. Wu (2001) also discovered the average
hospitalization days for 554 cases of discharge planning in a regional hospital had reduced from 6.75 days in 1995 to 6.16 days in 1998, while the numbers renting for assistance tools have
multiplied five times from 1995 to 1998. Wu et al. (2000) assessed discharge planning for COPD patients with self- designed questionnaire by comparing 25 experimental and 31 control groups after hospital admission, discharge date, and 15-20 days following discharge. Results indicated that days of hospitalization, rates of following up, re-hospitalization, and satisfaction did not produce
significant difference between the two groups. However, knowledge of medication and illness caring in the experimental group practicing discharge planning was superior to the control group. Additionally, discharge planning in Kaohsiung Chang Gung Memorial Hospital from 1997 to 1998 showed that its transferred rate has increased from 67.8% to 85.3%, average days of
hospitalization diminished from 10.78 to 8.97, the rate of satisfaction for patients and family from 66.5% to 71.7%, and re-hospitalization decreased from 5.1% to 4.2% (Kuo et al, 2000). Furthermore, Liao and others (2000) analyzed the satisfaction of 24 patients in one Medical Center one, three, and six months following discharge and
indicated that their ADL and IADL have become seriously declined and
satisfaction has gradually reduced as the period after discharge lengthened; however, patients were remained satisfied about continuing care from the
hospital.
Counsell, Holder, Liebenauer, and Palmer et al (2000) randomly selected 1531 community patients of discharge planning from 1994 to 1997 for experimental and control groups. The previous group had more independent nursing interventions, physical
counseling, and fewer constraints than the later one. After one year the
previous group has less decline of ADL. However, hospitalization days,
re-hospitalization, and cost effectiveness have shown no significant differences between the two groups. Similarly, Shao and Yeh (2006) compared 22 elderly patients in neurological ward A and B who have taken routine outpatient service plus caregiver-oriented discharge planning with the other 22 elders in ward C and D as a control group. Results indicated that 22 stroke elders reported caregiver-oriented discharge planning could improve their health outcomes and the readiness of caregivers for care after one month discharge planning program.
Griffiths (2000) randomly selected 58 Canada Acute Strokes from
dischargee planning with physical, occupational, verbal therapies, and nutritional counseling and compared with 56 patients in the control group. Judging by three months follow-up the experimental group produced better
results than the control group in acute unit hospital time, improved physical health, and readjustment to the community. However, mental health, injury, and disability revealed no significant difference between the two groups. Brooks, Ashton, and Hainsworth (2003) reviewed 57 patients’ records of discharge planning, which disclosed only 7% re-hospitalization, 33% requiring no further interventions, although 47% needed transferred into another organization, and hygiene care was the most-requested patient need.
肆、Methodology
The outcomes-evaluation study design was to compare 346 cases’ records retrospectively from January in 2002 to June in 2003 in a Discharge Planning Program of Southern Fooyin University Hospital. The majority of discharge cases were from medical units with chronic illness referred by the staff nurses and evaluated by a discharge manager, who often managed 20 to 30 cases monthly. The outcomes-evaluated criteria included the patient’s health status, current situation, self-care ability, and family support function. Health status was measured as the amounts of equipments used such as Tracheotomy, N-G tube, Foley tube, PCN tube as well as the numbers of wound and
decubitous ulcers patients have had in
their bodies. Current situation was categorized as the patients’ current status as stable or follow up,
re-hospitalized, transferred to other units, dead, or missing. Self-care abilities and family support function were measured as the capabilities of the patients themselves and family members of feeding, toileting, bladder and bowel control, bathing, dressing, moving, medication, illness awareness, anxiety, and communication by 1-5 Likert scale with 1 as completely dependent, 2 as 75% dependent, 3 as 50% dependent, 4 as 25% dependent, and 5 as completely independent.
The secondary data were collected by two nursing students who have been trained by the chief investigator to have the consistent way of coding data. Both of the nursing students would review the documents of 346 cases together to key in the data of the patient’s health status, self-care ability, and family support function, while the content analysis was conducted by the principal investigator. The data were analyzed by the ANOVA statistics of SPSS Window 10.0,
including health status of 346 cases, as well as the self-care abilities and family support function of 37 cases, in
discharge planning from January, 2002 to June, 2003 of a Southern University Hospital. Additionally, the monthly records of 346 cases in June, 2003 were
used as the content analysis for understanding their current situation.
伍、Results
一 一 一
一、、、、Health Status
The health status of 346 cases confirmed that the amounts of
equipments and the numbers of wounds
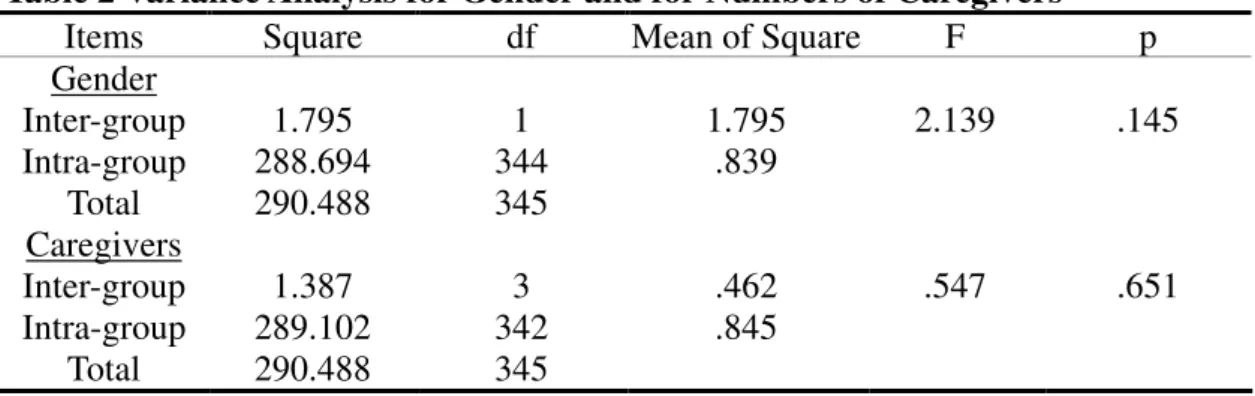
and decubitous ulcers the patients in their bodies had declined from January, 2002 to June, 2003 (t=10.253, p<.05) (Table 1). The improvement was apparently unaffected by gender (F=2.139, p>.05), and numbers of caregivers (F=.547, p>.05)(Table 2).
Table 1 Health Status among 346 cases
Health Status N Mean SD t p January in 2002 June in 2003 346 346 .74 .23 .94 .63 10.253 .000 p<.05
Table 2 Variance Analysis for Gender and for Numbers of Caregivers
Items Square df Mean of Square F p Gender Inter-group Intra-group Total 1.795 288.694 290.488 1 344 345 1.795 .839 2.139 .145 Caregivers Inter-group Intra-group Total 1.387 289.102 290.488 3 342 345 .462 .845 .547 .651 p<.05 二 二 二 二、、、、Current Situation
The current situation were
conducted in the records of 346 patients in June 2003 as content analysis by the categories of stable or follow up,
re-hospitalized, transferred to other units, dead, or missing. Content analysis
classified the 346 cases as follows: 57.4% stable or follow up, 15.1% missing, 11.3 % dead, 8.7%
re-hospitalized, and 7.5% transferred to other units such as local clinics, public health stations, nursing homes, or home care.
三 三三
三、、、、Self-Care Abilities
Results demonstrated that patients markedly elevated their illness
awareness as well as improving abilities of feeding, toileting, bathing, moving, medication, and communication from January, 2002 to June, 2003. However, bladder and bowel control and self-care ability in dressing display no significant improvement (Table 3). The results were also unaffected by gender (F=.287, p>.05), and numbers of caregivers (F=.923, p>.05)(Table 4).
Table 3 Self-Care Abilities among 37 cases
Self-Care Abilities N Mean SD t P Feeding
Toileting Urine and Stool Control
Bathing Clothing Moving Medication Ill-Awareness Anxiety Communication 37 37 37 37 37 37 37 37 37 37 -.57 -.68 -.30 -.38 -.32 -.54 -.41 -.92 -1.16 -.81 1.24 .85 1.29 .98 1.08 .80 1.04 .76 1.19 1.22 -2.791 -4.826 -1.404 -2.344 -1.824 -4.097 -2.372 -7.361 -5.938 -4.039 .008 .000 .169 .025 .076 .000 .023 .000 .000 .000 Total 37 -6.32 6.63 -5.803 .000 p<.05
Table 4 Variance Analysis for Gender and for Numbers of Caregivers
Items Square df Mean of Square F p Gender Inter-group Intra-group Total 12.870 1569.238 1582.108 1 35 36 12.870 44.835 .287 .596 Caregivers Inter-group Intra-group Total 81.512 1500.596 1582.108 2 34 36 40.756 44.135 .923 .407 p<.05 四 四 四
四、、、、Family Support Function
Results indicated that all family support function was identified as significantly improved from January,
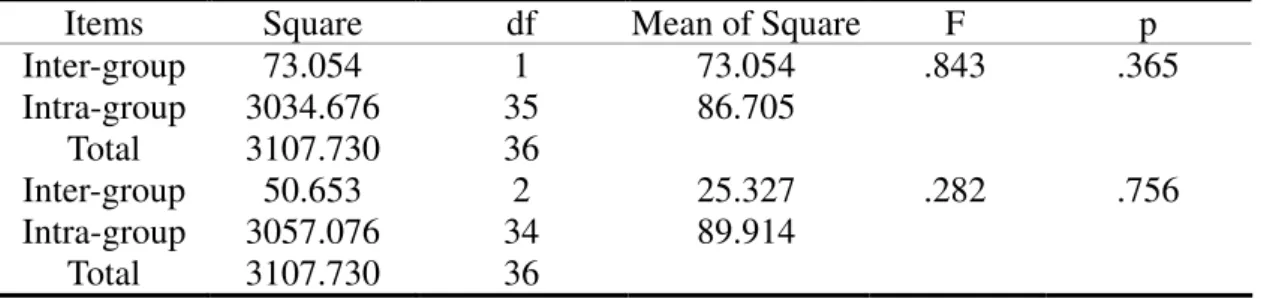
2002 to June, 2003 (Table 5). Again, these results were unaffected by gender (F=.843, p>.05), and numbers of caregivers (F=.282, p>.05) (Table 6).
Table 5 Family Support Function among 37 cases
Family Support Function N Mean SD t P Feeding
Toileting
Urine and Stool Control Bathing Clothing Moving Medication Ill-Awareness Anxiety Communication 37 37 37 37 37 37 37 37 37 37 -.43 -.39 -.35 -.32 -.32 -.46 -.35 -.95 -.76 -.49 1.04 1.02 .98 .91 .88 .99 .92 .91 1.12 1.07 -2.525 -2.283 -2.185 -2.157 -2.233 -2.827 -2.324 -6.315 -4.126 -2.765 .016 .029 .035 .038 .032 .008 .026 .000 .000 .009 Total 37 -4.70 9.29 -3.079 .004 p<.05
Table 6::::Variance Analysis for Gender and for Numbers of Caregivers
Items Square df Mean of Square F p Inter-group Intra-group Total 73.054 3034.676 3107.730 1 35 36 73.054 86.705 .843 .365 Inter-group Intra-group Total 50.653 3057.076 3107.730 2 34 36 25.327 89.914 .282 .756 P<.05
陸、Discussion and Conclusion
The literature review about
evaluation of discharge planning placed major emphasis on the days of
hospitalization, re-hospitalization, and the satisfaction of patients. The secondary focus was on transfer
numbers, rates of used assistance tools, ADL, knowledge of illness and caring, and rates of regular follow up. The rate of re-hospitalization in this study is 8.7%, which is greater than Brooks, Ashton, and Hainsworth (2003) reported 7%,while Kuo(2000) identified 4.2%;
However, the present study reported only 7.5% cases transferred into other units for continuing care, which was distinctly lower than the 47% Brooks, Ashton, and Hainsworth (2003) mentioned.
Additionally, health status, self-care abilities, and family support function have advanced noticeably regardless of their gender and numbers of caregivers. In other words, despite patient gender and how many caregivers they have, their health status, self-care
abilities, and family support function all would have improved significantly through discharge planning. These outcomes have provided the important evidences for the quality of care from discharge planning, and resembles Counsell, Holder, Liebenauer, Palmer et al findings (2000) that a group involved discharge planning indicated less ADL deterioration than the control group one year later. However, this result differs from Liao’s (2000) that 24 cases’ ADL and IADL had become seriously declined since discharge. Besides, this study reminds health care professionals to enhance the bladder and bowel control and self-care ability in dressing of the patients. The results are different from Brooks, Ashton, and Hainsworth (2003) emphasizing hygiene as the generally requested need.
Overall, studies on discharge planning in Taiwan tends to emphasize outcome criteria such as shortened hospitalization time, re-hospitalization, and medical costs, instead of patient- centered focus on developing the nursing care plan. The authors
recommend that future studies focus on developing the independent abilities such as ADL for hygiene, dressing, and bladder and bowel control of the patients. Besides, the amount of equipments used, size of wounds, infection rates, physical health, health status could be taken into account as evaluation criteria for discharge
planning. Additionally, instead of using the evaluated sheet in the hospital without the process of validation, the author suggested that Yeh, Huang, Cheng, and Cheng (1998) developed the evaluation form of discharge planning program, as well as Yang and Huang (2007) revised the patient needs rank assessment scale for discharge planning, could be applied into the future
evaluation of discharge planning. Finally, long-term care in discharge planning can be evaluated by mixed-methods that is expected to evaluate the quality of care for the elderly comprehensively and completely.
柒、Limitations
There are some limitations in this study. First, secondary data analysis would have the problem of
misinterpretation and coding data when comparing the data from the primary patients because the case manger of discharge planning may record the
wrong data. Secondly, sample size for data analysis of health status and current situation was different from the self-care abilities and family support function that could impact the power of data
explanation. The reason of only 37 cases in the data of self-care abilities and family support function was that they and their family members are able and willing to do self-care activities. Additionally, there is no control group compared with the discharge planning group which has reduced the validity of evaluation. Finally, the lack of
evaluation of the satisfaction from the patients and family members, as well as validation the evaluating methods, the process of data collecting and coding have impacted the validity of the study results; however, this study can provide an initial guide for the evidence-based evaluation of discharge planning.
捌、Acknowledgement
The author thanks the previous manager of Discharge Planning,
Chao-Chun Wang, of Fooyin University Hospital in Taiwan for providing the valuable data. Hsuan-Wen Hsu and others who are two-years BSN program students are appreciated for their assistance of data collection. Special thanks are given to the 346 cases in Discharge Planning where the study subjects were recruited, under the
auspices of the Fooyin University Hospital in Taiwan.
玖、References
Brooks, N., Ashton, A., & Hainsworth, B. (2003). Pilot evaluation of an intermediate care scheme. Nursing Standard,17(23), 33-35.
Chiu, S. H. (1999). Exploring the effectiveness of discharge planning service for neurosurgery patients in medical center. Chung Gang Nursing,10(4), 1-8.
Counsell, S. R., Holder, C. M.,
Liebenauer, L. L., Palmer, R. M., Fortinsky, R. H., Kresevic, D. M., Quinn, L. M., Allen, K. R.,
Covinsky, K. E., & Landefeld, C. S. (2000). Effects of a
multicomponent intervention on functional outcomes and process of care in hospitalized older patients: a randomized controlled trial of acute care for elders (ACE) in a community hospital. Journal of the American Geriatrics Society,48(12), 1572-1581.
Department of Health Executive Yuan (2004,August).Population in Taiwan.Taiwan
Health Internet.Available at: http:// www.doh.gov.tw/statistic/data/livin g statisics /91/02.XLS.
Department of Statistics, Ministry of Interior (2004,August).Analysis
of elder condition in Taiwan.
Available at: http:// www.moi.gov. tw/W3/stat/home.asp.
Griffiths, P. (2000). Prompt hospital discharge with home care improved physical health and community reintegration and reduced initial length of hospital stay after acute stroke. Evidence-Based
Nursing,3(4), 126-127.
Hou, J. W., Hollenberg, J., & Charlson, M. E. (2001). Can physicians’ admission evaluation of patients’ status help to identify patients requiring social work interventions? Social Work in Health Care,33(2), 17-19.
Kuo, M. L., Hsu, L. N., Chen, C. O., Lee, Y. C., & Chang, G. G. (2000).Kaohsiung Chang Gung Memorial Hospital-construction and evaluation of discharge planning services.Chung Gang Nursing,11(2), 43-54.
Liao, M. N., Shao, L. H., Lee, S. G., & Hsu, Y. Y. (2000).The quality care and satisfaction of discharge
planning and home care in one medical center.Chung Gang Nursing,11(3), 1-12.
Lin, P. C., & Chang, S. U. (2004). Functional recovery among elderly people one year after hip fracture surgery. Journal of Nursing
Research, 12(1), 72-82.
Pan, Y. L. (2000).Construction and development of discharge planning- Mackay
Memorial Hospital as an example.
Journal of Nursing, 47(4), 76-86. Saltvedt, I., Opdahl, E., Fayers, P.,
Kaasa, S., & Sletvold, O. (2002). Reduced mortality in treating acutely sick, frail older patients in a geriatric evaluation and
management unit. A prospective randomized trial. Journal of the American Geriatrics Society, 50(5), 792-798.
Shao, J. H., & Yeh, H. F. (2006). Evaluation of carer readiness and care outcome following a caregiver needs directed discharge program for elderly stroke patients. The Journal of Long-Term Care, 10(3), 238-256.
Wu, C. C., Lin, L. C., Su, S. A., Weng, L. H., Zou, P. Y., Wu, Y. Y., & Kuo, Y. G. (2001).Evaluation of
discharge planning-the middle hospital as an example.Nursing Administration, 34(2), 45-52. Wu, Y. C., Hsu, H. M., Sun, S. J., Chang,
F. C., & Hsu, M. T. (2000). Evaluation of discharge planning for COPD syndromes.Public Health, 27(2), 139-147.
Yang, C. T., & Yin, S. C. (2002).
Applying case management model into discharge planning in one medical center.Veterans Nursing, 19(2), 125-131.
Yang, H. C., Shiao, J. SC, & Chen, Y. H. (2004). Job contents and work conditions of the discharge
planners in Taiwan. Taiwan Journal of Family Medicines, 14(4),
193-204.
Yang, L. H., & Huang, T. T. (2007). A project to revise the patient needs rank assessment scale for discharge planning. Journal of Nursing, 54(2), 55-61.
Yeh, L. L., Huang, Y. W., Cheng, Y. L., & Cheng, S. G. (1998). The evaluation form of discharge planning program. Journal of Nursing, 45(6), 71-80.
Evaluation of Discharge Planning in a Southern Hospital
Ya-Lie Ku
1Shih-Ming Kuo
2Hsin-Yi Kuo
3Abstract
The population of elders in Taiwan has increased by over 7% since 1993 and fit the WHO criteria for an aging country. Long-term care thus is very important in Taiwan, and discharge planning is the part of long-term care for identifying high-risk cases that require continuing care. High quality discharge planning can train patients and their family members in self-care skills early before discharging the hospital; thus reduced hospitalization return rate and health care costs. The purpose of this study was to evaluate the discharge planning. Secondary data analysis was applied to examine 346 cases in discharge planning retrospectively from January, 2002 to June, 2003 to understand their health status and current situation, as well as the self-care abilities and family support function of 37 cases. The outcome data were evaluated by the assessment tool of a Southern University Hospital, including the patient’s health status, current situation, self-care ability, and family support function. The study results identified that the outcomes evaluation of the patient’s health status improved significantly during one year, but sex and the number of caregivers do not affect the improvement. Additionally, content analysis of the patients’ current status broke down as follows: 57.4% stable or follow up, 15.1% missing, 11.3 % dead, 8.7% re-hospitalized, and 7.5% transferred to other units such as local clinics, public health stations, nursing homes, or home care. Furthermore, self-care abilities and family support function such as feeding, toileting, bathing, moving, medicating, illness awareness, anxiety, and communication of 37 cases improved significantly within one year, but sex and the number of caregivers do not affect the improvement. Only the patient’s bladder and bowel control and self-care ability in dressing did not improve.
Keywords: discharge planning、outcomes evaluation
1
Assistant Professor, Elder/Community Field, Department of Nursing,, Fooyin University 2
Lecturer, Center of General Education, Fooyin University 3
Lecturer, Medical/Surgical Field, Department of Nursing, Fooyin University Received:Mar.2,2010 Revised:Dec.10,2010 Accepted:Dec.30,2010