ISSN 1992-2248 ©2012 Academic Journals
Full Length Research Paper
An intelligence system approach using artificial neural
networks to evaluate the quality of treatment planning
for nasopharyngeal carcinoma
Tsair-Fwu Lee
1*
#, Pei-Ju Chao
1,2#, Chang-Yu Wang
3,4, Wei-Luen Huang
1, Chiu-Ching Tuan
5,
Mong-Fong Horng
1, Jia-Ming Wu
6, Shyh-An Yeh
6, Fu-Min Fang
2and Stephen Wan Leung
41
Medical Physics and Informatics Laboratory, Department of Electronics Engineering, National Kaohsiung University of
Applied Sciences, Kaohsiung, Taiwan.
2
Department of Radiation Oncology, Kaohsiung Chang Gung Memorial Hospital and Chang Gung University College of
Medicine, Kaohsiung, Taiwan.
3
Department of Electrical Engineering, National Kaohsiung University of Applied Sciences, Kaohsiung, Taiwan.
4
Department of Radiation Oncology, Yuan’s General Hospital, Kaohsiung City, Taiwan.
5Department of Electronics Engineering, National Taipei University of Technology, Taipei Taiwan.
6
Department of Radiation Oncology, E-Da Hospital /I-Shou University, Kaohsiung, Taiwan.
Accepted 30 May, 2012
The quality of the nasopharyngeal carcinoma (NPC) treatment plans evaluation using three types of
artificial neural networks (ANNs) are instructed by three different training algorithms. Three ANNs
including Elman (ANN
-E), feed-forward (ANN
-FF), and pattern recognition (ANN
-PR) were trained by using
three different models, that is, leave-one-out (Train
-loo), random selection (Train
-random), and user defined
(Train
-user) method. One hundred sets of NPC treatment plans were collected as the input data of the
neural networks. The conformal index (CI) and homogeneity index (HI) were used as the characteristic
values and also to train the neurons. Four grades (A, B, C, and D) were classified in degrading order.
The over-training issue is considered between the train data and the number of neurons. The receiver
operating characteristic (ROC) curves were obtained to evaluate the performed accuracies. The optimal
numbers of neurons for ANN
-E, ANN
-FF, and ANN
-PR, in the loo method are 6, 24, and 9; in the
random-selection method, they are 26, 22, and 4; and in the user-defined method they are 12, 8, and 11 neurons,
respectively. The optimal size of train data is 92% of total inputs in the cases of ANN
-Eand ANN
-FFand
76% in the case of ANN
-PR. The networks with higher accuracy are ANN
-PR-loo(93.65 ± 3.60%), ANN
-FF-loo(88.05 ± 5.84%), and ANN
-E-loo(87.55 ± 5.86%), respectively. The networks with shorter training time are
ANN
-PR-random(0.55 ± 0.11 s), ANN
-PR-user(0.59 ± 0.08 s), and ANN
-PR-user(1.07 ± 0.16 s), respectively. The
ROC curves show that the ANN
-PR-looapproach has the highest sensitivity, which is 99%. ANN
-PR-looreduces the amount of trail-and-error during the iterative process of generating inverse treatment plans.
It is concluded that the ANN
-PR-loois an excellent model among the three for classifying the quality of
treatment plans for NPC.
Key words: Artificial neural networks (ANNs), dose-volume histogram (DVH), intelligence system,
nasopharyngeal carcinoma (NPC).
INTRODUCTION
Clinically, intensity modulated radiation therapy (IMRT) is
the most common technique to deliver radiation doses to
nasopharyngeal carcinoma (NPC) patients, because
IMRT is capable of delivering a high dose to the irregular
tumors, and prevents organs at risk (OARs) and normal
tissues from being exposed to radiation. However, it is
usually difficult to complete a suitable IMRT plan at one
time because both the patient’s condition and some
complex formulas need to be considered simultaneously.
The IMRT technique greatly benefits NPC patients,
offering much higher treatment quality. The IMRT
technique combines several different radiation fields to
produce steep dose-volume histogram (DVH) and
isodose curves for the planned target. These steep
curves mean that the dose gradient at the border
between cancerous and normal tissue varies rapidly.
Usually the acceptable dose distribution can be produced
by using seven to nine fields (Lee et al., 2008; Oldham et
al., 2008).
A treatment plan that results in a higher planning target
volume (PTV) coverage and reduce the complications in
normal tissues is preferred, and this may be done after
several attempts using trial and error. The inverse
calculation is one kind of algorithm that is embedded in
treatment planning systems (TPS). It is generally used in
the optimization procedure for IMRT. The inverse
calculation adopts iterative operation and an optimal
algorithm to produce varied intensity of treatment beams.
This allows IMRT to find a dose that compromises
between the PTV and critical organs (Webb, 2004; Leung
et al., 2007). The interactive interface is also supported in
modern planning systems. The dose-volume based
weighting and the priority of the critical organs can be set.
Therefore, planners can define some limits for PTV and
OARs, which is called constraint-based optimization.
In order to find the solution during the optimization
procedure, three steps are performed: (1) determine the
constraints and priority setting making up an objective
function by the planner, (2) work out the objective
function, and (3) evaluate the quality of the treatment
plan with the prescribed dose and criteria. These three
steps are executed sequentially or iteratively until an
optimal solution is reached (Stieler et al., 2009).
However, the quality of a final plan depends on the
planners’ experiences, which may be learned from
others’ experience or published journals (Deasy et al.,
2007; Wilkens et al., 2007). It is very time-consuming for
a planner to fine-tune for individual optimal solutions.
Technically the final result obtained is usually not an
optimal solution, but a sub-optimal one. Generally, if we
want to find an optimal solution, we have to consider not
only a minimum objective function, but also the individual
clinical conditions and many parameters not included in
the objective function. If an expert knowledge-based
system is applied to learn and to accumulate those
experiences, then the time taken to create an optimal
treatment plan will be reduced. This knowledge-based
system is especially effective for complex treatment
plans, such as NPC plans.
Artificial neural networks (ANNs) are widely used in the
modern sciences (Wu et al., 2009; Bahi et al., 2006;
*Corresponding author. E-mail: tflee@kuas.edu.tw or lwan@ms36.hinet.net.
#Both author contribution equally. Part of this study was presented at the International Conference on Agricultural, Food and Biological Engineering (ICAFBE 2012)
Lee et al. 2077
Vasseur et al., 2008). There are some major researches
on ANN models that were used to predict the side effects
after radiation therapy. For instant, the leave-one-out
(loo), random-selection, and user-defined methods were
applied to train the feed-forward ANN model introduced
by Su et al. (2005) which is used to predict the probability
of pneumonitis after treatment. The sensitivity obtained
by the three different methods are 0.95, 0.57, and 0.71
and their respective accuracies are 0.94, 0.88, and 0.90.
The ANN is also used to calculate the probability of
developing radiation pneumonitis, as proposed by Chen
et al.
(2007). Based on Chen’s model, the receiver
operating characteristic (ROC) curves show that the
sensitivity is 0.67, the specificity is 0.69, p = 0.020.
Obviously, involvement of the aforementioned non-dose
characteristics
makes
ANNs
more
generalized.
Moreover, Mathieu et al. (2005a) adopts an ANN to
optimize the dose distribution. It is applied in treatment
plans to make sure the time taken for calculation is
acceptable and the error is less than 2%. Isaksson et al.
(2005) also uses the feed-forward network to predict the
motion of a tumor in the lung during radiation therapy.
Results show that this method is better than the
conventional one and the self-adaptive filter. Many kinds
of treatment techniques introduced by Bortfeld and Webb
(2009) are used to reduce the treatment time effectively.
Our preliminary result (Chao et al., 2010) shows that a
back-propagation model using dose parameters and
dose indices can produce high accuracy in evaluating
NPC plans. Some applications of ANNs were used in the
past to implement 3DCRT plans effectively and
efficiently, and a few of them were applied in the expert
system of IMRT.
Whether a treatment plan is acceptable or
unaccept-able, it usually depends on the planner’s experience. It is
time-consuming to evaluate the calculated results and
fine-tune the weightings by trial and error. In this study,
three types of ANNs are instructed by three different
training algorithms to effectively evaluate the quality of
the NPC treatment plans. A better match for ANN and the
training algorithm will be chosen and established. We aim
to help to make an intelligence judgment that reduces the
amount of interaction between planner and TPS during
the iterative process of generating inverse treatment
plans. It can decide whether a plan is acceptable and
ranking the quality of treatment plans automatically,
therefore, providing an improvement suggestion when the
plan was not acceptable.
MATERIALS AND METHODS
Three different neural network models, namely, the Elman (ANN-E), feed-forward (ANN-FF), and pattern recognition (ANN-PR) models, are adopted. Each model is worked with three selection methods, named the leave-one-out (loo), random-selection, and user-defined methods, to train the neurons. The overall system flowchart is as shown in Figure 1. The data of DVHs are imported into the untrained ANNs and the training method is selected. We want to
Treatment
planing
Manual
evaluation
ANN
Evaluation
system
Check
criteria
Ready for
delivery
Plan improvement
suggestions
Yes
No
Figure 1. System flowchart for plan quality evaluation and
improvement suggestions; ANN: artificial neural networks.
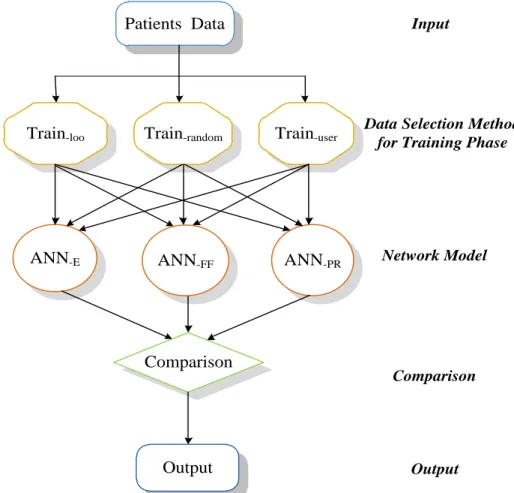
find an ANN model that matches a specific training method to produce the highest accuracy by consideration a mong the conditions of the training time, the number of neurons, the size of training data population, and ROC curves (Chen et al., 2007; Mathieu et al., 2005b). Then, the model can be taken as the best one to evaluate the treatment plans. The basic neural networks structure of the selection procedure is as shown in Figure 2. In the following, parameters and neural networks used are described.
Input parameters
According to the International Commission on Radiation Units and Measurements (ICRU) Report 62, the planning organ-at-risk volumes (PRVs) were defined as a safety margin around the OARs, particularly for a high-dose gradient area. In this study, the PRV of the spinal cord was determined by adding a 3D margin of at least 5 mm to the delineated spinal cord. The PRVs of the brain stem and chiasm were defined through addition of a 3D margin of at least 1 mm around the delineated structures. According to the suggestions of Radiation Therapy Oncology Group (RTOG) 0225 (Lee et al., 2003), one hundred NPC samples (NP = N100) are collected as the inputs, where NP denotes the dimension of sample space and the suffix p denotes the number of samples in that group. This study was approved by the institutional review boards of the hospitals involved (IRB 99-1420B). Eventually, all the samples will be separated into four ranking classes, named A, B, C, and D. Each class is described as follows:
A: the treatment plan is accepted by physicians.
B: the prescription dose calculated on parallel organs exceeds the criteria.
C: the prescription dose calculated on serial organs exceeds the
criteria.
D: the coverage of PTV does not meet the criteria.
The energy selected is of a 6 MV photon beam and a seven-field IMRT plan is created (Chao et al., 2010). This leads to the reduction of treatment time and enhance the biological effect. Each NPC plan has its own dosimetric indices and parameters (Lee et al., 2010, Lee et al., 2011, Fang et al., 2010; Widesott et al., 2008; Leung et al., 2007), which are discussed subsequently.
Dosimetric parameters Planning target volume
Three parameters are commonly used to evaluate the coverage of the PTV. V93 means 93% of the total dose is received by 97% of PTV. The parameter V100 means 100% of the prescription dose covers more than 95% of PTV. Similarly, V110 means that 110% of the dose covers less than or equal to 20% of the PTV.
Constraints for the organs at risk
1) Spinal cord (SC): The maximum dose ≤ 45 Gy or 1 cc of PRV ≤ 50 Gy;
2) Brain stem (BS): The maximum dose ≤ 54 Gy or 1% of PRV ≤ 60 Gy;
3) Chiasm: The maximum dose ≤ 54 Gy or maximum dose of PRV ≤ 60 Gy;
Lee et al. 2079
Data Selection Method
for Training Phase
Network Model
Input
Output
Patients Data
ANN
-EANN-FF
ANN
-PRComparison
Output
Comparison
Train-loo
Train-random
Train-user
Figure 2. Basic neural networks structure. ANN: artificial neural networks; ANN-E: the Elman network; ANN-FF: the feed-forward network; ANN-PR: a pattern recognition network; Train-loo: ANN with leave-one-out method for training data selection; Train-random: ANN with random selection method for training data selection; Train-user: ANN with user-defined method for training data selection.
5) Lens: The maximum dose must be ≤ 10 Gy and as low as possible;
6) Eyes: the maximum dose must be ≤ 45 Gy;
7) Mandible: The maximum dose must be ≤ 70 Gy or 1 cc of PRV and cannot exceed 75 Gy;
8) Oral cavity excluding PTV: the mean dose must be ≤ 40 Gy; 9) Healthy tissue: the mean dose must be ≤ 30 Gy or no more than 1% or 1 cc of the tissue outside the PTV will receive ≥ 110% of the dose prescribed to the PTV.
Dosimetric indices Conformal index (CI)
This is used to estimate the coverage of PTV (Feuvret et al., 2006).
2 PV TV PTV
TV
V
V
CI
where
V
TV is the treatment volume of prescribed isodose lines,PTV
V
is the volume of PTV, andTV
PV is the volume ofV
PTVwithin
V
TV. The best conformal case is the value of CI equal to 1.Homogeneity index (HI)
This index describes how the homogeneity varies within the PTV.
% 95 % 5
D
D
HI
where
D
5% andD
95%are the minimum doses delivered to 5 and 95% of the PTV. A higher HI indicates poorer homogeneity.Therefore, there are 14 indices included in D = [V93, V100, V110, SC, BS, rt Parotid, lt Parotid, Lens, rt Eye, lt Eye, Oral, Mandible, CI, HI] which are presented in this paper as the input vector (rt: right side, lt: left side).
Training parameters
Three distinct training methods are considered separately as follows:
1) Leave-one-out (Train-loo): This method selects one set of the patient’s data at a time to be the validation vector, and the other sets (Np – 1) are used to train the network until Np iterations have been done. It is suitable for use when the amount of data is small and high accuracy is needed.
2) Random selection (Train-random): Here, four kinds of arrangement are made. The first kind selects 60% of the patient’s data (N60) to be the training data and the remaining 40% are used as the test vector. In the second arrangement, 67% of data are chosen to be the training data and the remainder is the test vector; in the third arrangement, the training data and test vector comprise 75 and 25% of the data, respectively, and in the fourth, 80 and 20%, respectively.
3) User-defined (Train-user): This method is similar to Train-random, but differs in that the data are selected manually. We prefer to select typical data to train the network, because it is easier to describe the border of data when the population of data is small.
The cross-validation method is adopted to prevent ANNs from over-training. If an ANN model is over-trained, non-generalized problems may occur as a result; for example, the training time may be too long or the accuracy may fall below an acceptable level, and so on.
Artificial neural networks
ANN is a brain-like network that possesses self-learning and memory abilities. The signal routes of a network are similar to the axons that carry the electrical signal out to other layers (Gulliford et al., 2004). Three types of ANNs are instructed by three different training algorithms to evaluate the quality of the plans. MATLAB (v 7.9, The MathWorks, Natick, Massachusetts) is adopted to construct the network and to evaluate the treatment plans.
Feed-forward network
Many kinds of structures can be produced by combining learning modes and nodes. A basic one is the feed-forward network (ANN -FF), it has three main layers (Isaksson et al., 2005; Deasy et al., 2007; Bortfeld and Webb, 2009; Luo et al., 2005; Zhang et al., 2010):
1) Input layer: This layer actually consists of input components. Generally, it has two types: one whose input components are weighted in neurons with a bias value, and another which just connects the input components to neurons directly without operations. Here, the first type is adopted.
2) Hidden layer: The intermediate layer between input and output layers. This layer receives input signals and processes them with a defined transfer function. The number of layers could be zero or multiple. Here, there is one hidden layer. It should be noted that the number of neurons will decide the speed of convergence.
3) Output layer: A layer whose output is the output of the network. An error between the output and the actual value could feed backward to the weighting matrix. This feedback procedure is done until the output converges.
Elman network
The Elman network structure (ANN-E) (Cheng et al., 2002) is a simple recursive network (SRN). In an Elman network, some outputs of the hidden layer feed information back to the input layer. Those components are called context units and their weightings are fixed. This mechanism produces a signal which returns to where it came from, and thus the Elman network acts like a dynamic memory that can remember some previous information temporarily.
The weighting is adjusted by an error back-propagation algorithm. The linear transfer function is adopted in the input layer and the output layer, but a hyperbolic tangent function is used in the hidden layer. A factor δ called self-feedback gain denotes the state of the previous inputs contained in a context component (Liu et al., 2006; Qi et al., 2008; Su et al., 2007; Yuan-Chu et al., 2008). When δ approaches 1, this means that a context unit possesses more previous states. Otherwise, the network returns to the standard Elman network as δ is equal to zero. The value δ is chosen to be zero in our study.
Pattern recognition network
A pattern recognition network (ANN-PR) (Duin et al., 2007) can be trained to classify inputs according to target classes. The target data for pattern recognition networks should consist of vectors of all zero values except for a 1 in element i, where i is the class they are to represent. The input patterns are sensed and transformed into measurements by an ANN-PR. The features will be extracted from those measurements during the preprocessing procedure and features extraction. Therefore, the ANN-PR can recognize the patterns with respect to the features (Klopf and Gose, 1969; Lee and Bezdek, 1988; Maruno et al., 1993; Ulug, 1996; Weaver, 1975). In this study, the transfer function of the input layer is linear. Besides, there is only one stage in the hidden layer, whose transfer function is a hyperbolic tangent. The arrangement of the output layer is the same as that of the hidden layer here.
Three networks, named Elman, feed-forward, and pattern recognition, are adopted in this study. During training, the data are selected by the loo, random selected, and user defined methods separately. The over-training problem is also discussed in the following along with the inputted data and the number of neurons, and the accuracies of the three algorithms are evaluated by using ROC curves.
Statistical analysis
Statistical tests of differences between the models were performed using a two-tail matched-pair exact Student t-test. Differences were considered statistically significant for p-values ≤ 0.05. All data presented in the text, tables and figures refer to the mean and standard deviation. The Statistical Package for Social Sciences (SPSS)-16.0 software was used for data processing (SPSS, Inc., Chicago, IL, USA).
RESULTS
Neurons and training data
The cross-validation method is used to prevent the
over-training situation from occurring for evaluating the
number of neurons and the amount of training data; the
results on two issues are as follow:
1) Training data: The accuracies of the system and
training time of networks versus the size of training data
is shown in Table 1, the simulated results for ANN
-Eand
ANN
-FFshow that the optimal size of training data is 84%
of total inputs. In the case of ANN
-PR, the optimal size of
training data is 76% of total inputs.
2) Number of neurons: Relations between the number of
neurons and neural networks are as shown in Figure 3.
2088 Sci. Res. Essays
Treatment Planning Based on Prioritizing Prescription Goals. Phys . Med. Biol., 52(6): 1675-92.
Wu HY, Hsu CY, Lee TF, Fang FM (2009). Improved SVM and ANN in incipient fault diagnosis of power transformers using clonal selection algorithms. Int. J. Innov. Comput. Inf. Control, 5(7): 1959-1974. Yuan-Chu C, Wei-Min Q, Jie Z (2008). A new Elman Neural Network
and its Dynamic Properties. Cybern. Intell. Syst. 2008 IEEE Conf., pp. 971-975.
Zhang LD, Jia L, Zhu WX (2010). Overview of Traffic Flow Hybrid ANN Forecasting Algorithm Study. Comput. Appl. Syst. Model. (ICCASM), 2010 Int. Conf., 1: 615-619.