ORIGINAL PAPER
Impact of physical activity on heart rate variability
in children with type 1 diabetes
Su-Ru Chen&Yann-Jinn Lee&Hung-Wen Chiu&
Chii Jeng
Received: 29 December 2006 / Revised: 19 July 2007 / Published online: 28 September 2007 # Springer-Verlag 2007
Abstract
Objective Children with type 1 diabetes are usually associ-ated with cardiovascular autonomic neuropathy. The present study explored the influence of physical activity on their autonomic nervous function by measuring the heart rate variability (HRV).
Materials and methods A total of 93 type 1 diabetic children and 107 healthy control subjects were enrolled. The Physical Activity Questionnaire for Children (PAQ-C) was adopted to determine the physical activity level as low, moderate, or high activity. HRV was determined by frequency analysis and measured in both resting and active states.
Results Children with type 1 diabetes had significantly lower HRV than that of healthy control subjects in resting state but not in active state. The decreased HRV in diabetic children was observed only in subjects with low physical
activity. The HRV in diabetic children with moderate to high physical activity, however, was not different from that of their healthy controls.
Conclusions Diabetic children should be encouraged to engage in physical activity with more intensity, which can benefit their autonomic nervous function. Nevertheless, the potential risk of vigorous activity still needs our concern.
Keywords Cardiovascular autonomic neuropathy . Heart rate variability . Type 1 diabetes . Physical activity
Introduction
Diabetes is a metabolic disorder in which the body fails to produce enough insulin. Type 1 diabetes results from an autoimmune process, which leaves the patient dependent on insulin injections for survival. Type 2 diabetes, formerly known as adult-onset diabetes, tends to increase the need for insulin in the face of insulin resistance [3]. The incidence of type 1 diabetes is much lower than that of type 2 diabetes, but the earlier onset and higher degree of glycemic exposure in type 1 diabetes brings them a greater loss of quality life-years [31]. Children with type 1 diabetes are threatened by the acute complications of hypoglycemia and ketoacidosis, and the long-term complications of neuropathy, nephropathy, and retinopathy, which place them at a substantial risk for serious morbidities and earlier than expected mortality [23].
Autonomic neuropathy is a common complication of diabetes. Extensive involvement of the autonomic nervous system in diabetic patients produces a variety of physiolog-ical changes, which may include the electrphysiolog-ical and contractile activity of the myocardium [25]. In patients with type 1 diabetes, cardiovascular autonomic neuropathy (CAN) was detectable in 20 to 36% of individuals [24] and contributed
S.-R. Chen
Graduate Institute of Medical Sciences, College of Medicine, Taipei Medical University,
Taipei, Taiwan
S.-R. Chen
:
C. Jeng (*)College of Nursing, Taipei Medical University, No.250, Wuxing St., Xinyi District,
Taipei 110, Taiwan e-mail: [email protected] Y.-J. Lee
Department of Pediatrics, Mackay Memorial Hospital, Taipei, Taiwan
Y.-J. Lee
Department of Pediatrics, Taipei Medical University, Taipei, Taiwan
H.-W. Chiu
Graduate Institute of Medical Informatics, Taipei Medical University,
to a high mortality rate ranging from 27 to 56% [10,18]. Many diabetic patients demonstrate abnormal autonomic nervous function on specific testing before the onset of clinical signs. Once the diagnosis of CAN is established, a significant deterioration in the quality of life and increased morbidity and mortality will ensue [11,30,33].
Heart rate variability (HRV) has been widely applied to assess autonomic nervous function by measuring the frequency components of beat-to-beat variability in RR intervals of electrocardiography (ECG) [2]. With regard to HRV parameters, high frequency (HF; 0.15–0.5 Hz) mirrors parasympathetic nervous activities; low frequency (LF; 0.04–0.15 Hz) represents both sympathetic and parasym-pathetic nervous activities; LF/HF ratio reflects the auto-nomic nervous system balance or sympathetic nervous activity; and total power (TP; 0.04–0.5 Hz) denotes the overall state of autonomic nervous system [27]. Abnormal HRV can be detected in diabetic subjects even when the clinical signs of CAN are obscure [1,6,32]. HRV analysis has also been demonstrated to be more sensitive than traditional cardiovascular reflex test in clinical evaluation of autonomic nervous function [1,5,26].
Several previous studies have shown that HRV tend to be higher in active compared with inactive healthy subjects [15, 17, 20]. Physical exercise was also demonstrated to elevate the HRV in children who initially had low HRV [14,
17]. Regular physical activity may contribute to weight loss, decreased insulin resistance, and improved blood glucose control and was commonly advocated for both type 1 and type 2 diabetes [4, 22, 29]. However, little is known about the association between physical activity and the autonomic nervous function of diabetes. Thus we conducted this study to explore the influence of physical activity on HRV in children with type 1 diabetes.
Materials and methods
Subjects
Ninety-three children (48 females and 45 males) aged 8– 12 years with type 1 diabetes were prospectively studied. The diagnosis of diabetes was made at a pediatric dia-betic clinic in a tertiary medical center in Taiwan ac-cording to the revised American Diabetes Association guidelines [28]. At the time of the study, all patients were receiving regular insulin treatment. Control group was composed of 107 gender- and age-matched healthy children from a junior school. None of the children in either group had any clinical or historical evidence of cardiovascular or neurological diseases. Those who con-sumed medicine that affected cardiovascular function or autonomic nervous activities were excluded from this
study. Subjects were asked to have their HRV recorded according to the protocol described below. The local ethics committee of the hospital approved this study, and written informed consent was obtained from all subjects and their parents before participation.
Physical activity
All participants were asked to fill out a self-administered Physical Activity Questionnaire for Children (PAQ-C), which was designed for school-aged children [8]. The PAQ-C consists of nine items referring to the physical activity during the past 7 days. Each of which has five response options of frequency scaled from 1 (none) to 5 (>7 times/week). The physical activity level was determined according to the mean scale of the nine items as low (≤2), moderate (>2 and≤3), and high activity (>3).
The PAQ-C was in English originally. To ensure accuracy in the translation of the tool, the PAQ-C was translated into Chinese using a translation and back-translation procedure and was verified by a panel of experts to ensure the semantics of the Taiwanese version of the questionnaire. In this study, the internal consistency reliability was 0.78, and the test–retest reliability was 0.81 (p<0.01).
HRV analysis
Standard 3-channel ECG electrodes were attached to the anterior chest wall of subjects and connected to the monitor system (Acknowledge III, MP150WSW, BIOPAC System, Santa Barbara, CA). All QRS complexes on ECG were first edited automatically and then manually by careful inspec-tion of the RR intervals. Signals were digitalized at 500 Hz and transformed into a spectrum by Fast Fourier Transfor-mation. Separate frequency components of HRV were obtained including LF, HF, LF/HF, and TP. These HRV parameters were then logarithmically transformed (Ln) to control for the skewed distributions.
Experimental procedure
Personal data including age, gender, body mass index (BMI), and waist/hip ratio (WHR) were obtained at entrance. HbA1c and disease duration for diabetic children were obtained from their medical chart. All the experimen-tal procedures were performed in a quiet room, with the temperature controlled between 21–26°C. Beverages rich in caffeine content and vigorous exercise were prohibited within 2 h before testing. Study subjects were asked to stand still for 10 min in resting state, followed by an exercise with a fixed rhythm on a stair-stepper (JK-355c; JKexer, Taipei, Taiwan) for 10 min in active state. The ECG was continuously monitored throughout the test and the last
5-min recordings of steady ECG in each section were obtained for HRV analysis.
Statistical analysis
Statistical analysis was performed using the Statistical Package for the Social Sciences for Windows, version 12.0 (SPSS, Chicago, IL, USA). Data were expressed as mean ±standard deviation (SD). Student’s t test was performed to determine the differences between diabetes and control group, and between resting and active state. The relationship among physical activity level, HbA1c, and disease duration was examined by Pearson correlation analysis. Stepwise regression analysis was performed to assess the combined influence of physical activity level, HbA1c, and disease duration on HRV. One way ANOVA was used to examine differences of HRV among groups with various physical activity levels. Post hoc analysis was done by Scheffe’s test and a p value <0.05 was considered statistically significant.
Results
There were 93 type 1 diabetic children in the diabetes group and 107 healthy children in the control group. No
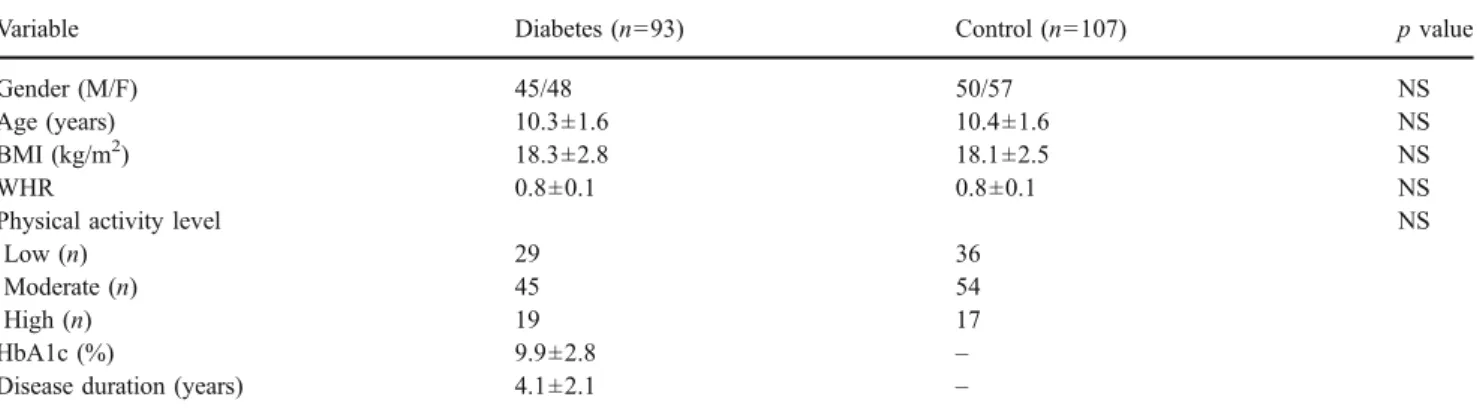
significant difference was found regarding gender (male/ female, 45/48 vs 50/57), age (10.3±1.6 vs 10.4±1.6 years), BMI (18.3±2.8 vs 18.1±2.5 kg/m2), or WHR (0.8±0.1 vs 0.8±0.1). The mean HbA1c and disease duration for the diabetes group were 9.9% ± 2.8% and 4.1 ± 2.1 years, respectively (Table1).
In resting state, there were significantly lower LnLF (6.0± 0.7 vs 6.3±0.6 ms2), LnHF (4.9±0.9 vs 5.2±0.9 ms2), and LnTP (6.7±0.4 vs 7.1±0.6 ms2) in the diabetes group compared to the control group. However, no significant difference of LnLF/HF (1.1±0.7 vs 1.2±0.7) was observed. In active state, there was no significant difference of HRV between the diabetes group and the control group in terms of LnLF (4.0±0.9 vs 4.1±0.8 ms2), LnHF (2.2±1.1 vs 2.3± 1.1 ms2), LnLF/HF (1.7±0.5 vs 1.7±0.7), and LnTP (5.0± 0.8 vs 5.0±0.7 ms2; Table2).
While proceeding from resting state to active state, healthy control subjects revealed significant decreases of LnLF (6.3±0.6 vs 4.1±0.8 ms2), LnHF (5.2±0.9 vs 2.3± 1.1 ms2), and LnTP (7.1±0.6 vs 5.0±0.7 ms2). Similar significant decreases of HRV were also observed in type 1 diabetic children as regard to LnLF (6.0±0.7 vs 4.0± 0.9 ms2), LnHF (4.9±0.9 vs 2.2±1.1 ms2), and LnTP (6.7± 0.4 vs 5.0±0.8 ms2). The difference of LnLF/HF between resting state and active state in both study groups, however,
Table 1 Demographic data of type 1 diabetic children and healthy control subjects
Variable Diabetes (n=93) Control (n=107) p value
Gender (M/F) 45/48 50/57 NS
Age (years) 10.3±1.6 10.4±1.6 NS
BMI (kg/m2) 18.3±2.8 18.1±2.5 NS
WHR 0.8±0.1 0.8±0.1 NS
Physical activity level NS
Low (n) 29 36
Moderate (n) 45 54
High (n) 19 17
HbA1c (%) 9.9±2.8 –
Disease duration (years) 4.1±2.1 –
Data are given as mean±SD or n.
NS Not significant, BMI body mass index, WHR waist/hip ratio.
Table 2 Heart rate variability in type 1 diabetic children and healthy control subjects in resting and active states
Variable Diabetes (n=93) Control (n=107)
Resting Active Resting Active
LnLF (ms2) 6.0±0.7*,** 4.0±0.9 6.3±0.6** 4.1±0.8
LnHF (ms2) 4.9±0.9*,** 2.2±1.1 5.2±0.9** 2.3±1.1
LnLF/HF 1.1±0.7 1.7±0.5 1.2±0.7 1.7±0.7
LnTP (ms2) 6.7±0.4*,** 5.0±0.8 7.1±0.6** 5.0±0.7
Data are given as mean±SD. *p<0.05 vs control in same state. **p<0.05 vs same group in active state.
was not significant (1.1±0.7 vs 1.7±0.5 for diabetes group and 1.2±0.7 vs 1.7±0.7 for control group; Table2).
The difference of HRV between diabetes group and control group in resting state was further studied by dividing them into subgroups according to their physical activity level as low (n=29 for diabetes group and n=36 for control group), moderate (n=45 for diabetes group and n= 54 for control group), and high activity (n=19 for diabetes group and n=17 for control group). The demographic data was not significantly different among all subgroups (Data not shown). Subjects in diabetes group with low, moderate and high activity had similar HbA1c (10.5±3.0, 9.5±2.6, and 9.7±2.6%, respectively) and compatible disease dura-tion (4.3±1.7, 4.0±2.4, and 4.2±2.0 years, respectively). In resting state, the increases of physical activity level in both diabetes group and control group were associated with a trend of increase in terms of LnLF, LnHF, and LnTP (Fig. 1). Although a decreasing trend in LnLF/HF was observed, it was not statistically significant. Significantly lower LnLF, LnHF, and LnTP were observed in type 1 diabetes with low activity compared to those in type 1 diabetes with moderate to high activity and in all control subgroups. No significant difference of LnLF, LnHF, and LnTP was noted between diabetes groups with moderate to high activity and all control subgroups, except that healthy children with high activity had higher LnHF than that of healthy children with low activity (5.7±0.8 vs 4.8±0.8 ms2), and higher LnTP than that of type 1 diabetes with moderate activity (7.3±0.7 vs 6.8±0.2 ms2). The differences of LnLF/HF among all the subgroups of type 1 diabetes and healthy control subjects were not significant. In contrast to the significant lower HRV in type 1 diabetes with low activity in resting state, no significant difference of any HRV parameters could be demonstrated in active state among subjects with different physical activity both in diabetes group and control group.
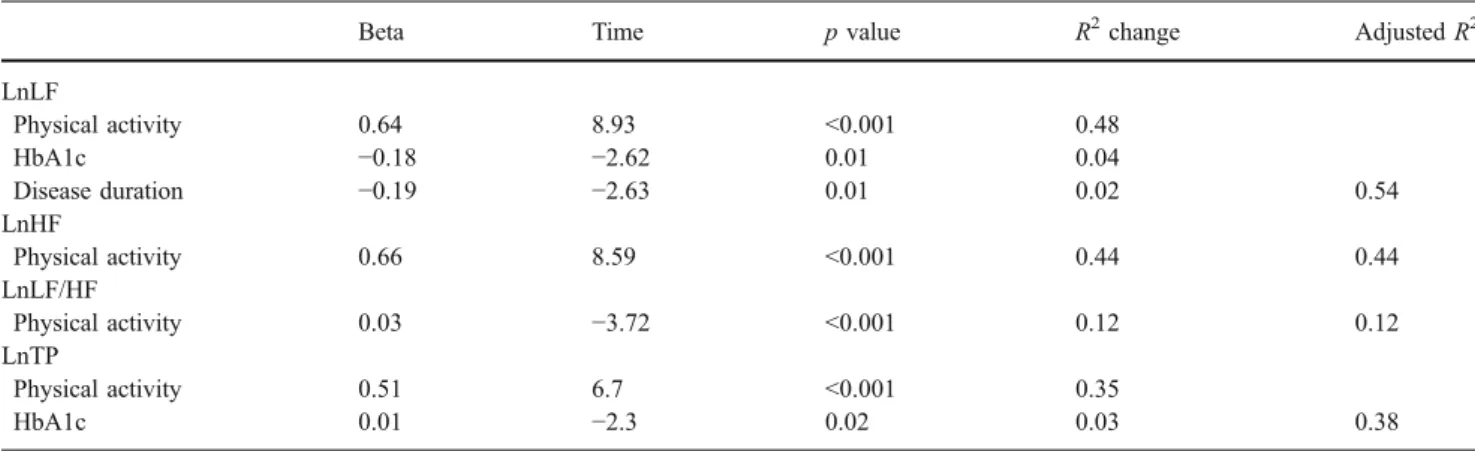
A stepwise regression analysis with HRV parameters as the dependent variables and with physical activity, HbA1c and disease duration as independent variables revealed that all of them were predictors of HRV (Table 3). Physical activity was the largest contributor, which predicted 12 to 54% of the variance of HRV parameters. There was a significant correlation between physical activity and HbA1c (r =−0.21, p<0.05). The correlations between disease duration and physical activity (r=−0.06, p=0.59) or HbA1c (r=0.14, p=0.17), however, were not significant.
Fig. 1 Heart rate variability in type 1 diabetic children and healthy control subjects in resting state plotted against the physical activity level (a LnLF, b LnHF, c LnLF/HF., d LnTP). Asterisk denotes p<0.05 vs type 1 diabetes with low activity. Single dagger denotes p < 0.05 vs. control group with low activity. Double dagger denotes p<0.05 vs. dia-betes group with moderate activityDiscussion
Our data showed that, type 1 diabetic children had lower LnLF, LnHF, LnTP, and similar LnLF/HF compared to those of healthy children in resting state. This finding implied that cardiovascular autonomic function was ad-versely affected by diabetes. It was also noted that the impaired autonomic nervous activities seemed to consist mainly in parasympathetic component. These findings were consistent with previous report by Colhoun et al. who analyzed 160 type 1 diabetic adults and found that all frequency components were decreased except LF/HF when compared to the general population [7]. A similar result was also reported by Kardelen et al. who demonstrated a significant reduction in parasympathetic activities in type 1 diabetic children [12].
Several previous studies have shown that acute physical activities may result in a reduced HRV as a consequence of vagal withdrawal [13,35]. Their findings are consistent with our results that healthy subjects had decreased LnLF, LnHF, and LnTP when proceeding from resting state to active state. Similar decrease was also observed in our study group with diabetes. However, the lower HRV in diabetic children than that of healthy subjects in resting state was no more significant in active state. This finding may imply a modulation effect of physical activity on autonomic nervous function. It was also possible that the predominant sympa-thetic nervous activity in the active state might not be adversely affected by diabetes in our subjects, as manifested by the comparable LnLF/HF between the two study groups. The pathogenesis of CAN in diabetes remains poorly understood. Chronic hyperglycemia, vascular insufficiency, and autoimmune mechanisms had been suggested as the plausible causes of neural damage [9,19,30]. The influence of physical activity level on autonomic nervous function in type 1 diabetes, however, has never been reported. Our data suggested that higher physical activity level was associated with higher HRV in children with type 1 diabetes, thus it is
reasonable to recommend physical activity for type 1 diabetes to benefit their autonomic nervous function. We also disclosed that the decreased HRV presented only in diabetic children with a low level of physical activity but not in those with moderate to high levels of physical activity. This finding implied that CAN in type 1 diabetes could be delayed or prevented by intensifying the physical activity.
The protective effects of physical activity on the auto-nomic nervous function might come from a better control of glycemia in diabetic children. Our results showed a signif-icantly negative correlation between physical activity and HbA1c, suggesting a beneficial effect on glycemic control from physical activity. It was demonstrated that hyperglyce-mia could damage nervous system by hyperosmolarity, increased oxidative stress, reduced nitric oxide synthesis, or vascular dysfunction [34]. Accordingly, the higher HbA1c level in diabetic children with low physical activity, although not statistically significant, predisposed them to the threat of hyperglycemia and subsequent autonomic neuropathy. Physical activity might have direct effects on autonomic function, as was reported by Monahan et al. that aerobic exercise increased the cardiovagal baroreflex sensi-tivity in healthy subjects, which resulted in a higher parasympathetic tone and thus higher HRV [16]. Physical exercise may also help decrease body weight to benefit their autonomic nervous function. However, we did not find any difference of body weight among the subgroups of all the study subjects.
Regular physical activity and exercise program in children with type 1 diabetes have long been recommended. However, the potential risk of vigorous activity still raised our concern. Type 1 diabetes may have too little insulin in their circulation due to inadequate therapy. Consequently, increasing level of glucose may become exacerbated during vigorous activity and even precipitate ketoacidosis. Con-versely, exogenous insulin administration will attenuate the mobilization of glucose that is induced by physical activity, and thus ensue hypoglycemia. Furthermore, the
cardiovas-Table 3 Predictors for heart rate variability
Beta Time p value R2change Adjusted R2
LnLF Physical activity 0.64 8.93 <0.001 0.48 HbA1c −0.18 −2.62 0.01 0.04 Disease duration −0.19 −2.63 0.01 0.02 0.54 LnHF Physical activity 0.66 8.59 <0.001 0.44 0.44 LnLF/HF Physical activity 0.03 −3.72 <0.001 0.12 0.12 LnTP Physical activity 0.51 6.7 <0.001 0.35 HbA1c 0.01 −2.3 0.02 0.03 0.38
cular function of diabetic children may have been impaired, and thus vigorous exercise may increase the risks of cardiovascular morbidity and mortality [21]. The adequate intensity of physical activity needs further study before the clinical guideline can be made.
In conclusion, efforts should be made for children with type 1 diabetes toward early prevention of CAN and slowing down its progression. We demonstrated that the decreased HRV in type 1 diabetes was associated with low but not moderate to high physical activities. Children with type 1 diabetes should be encouraged to engage in regular physical activity with more intensity, but avoid vigorous activity to prevent the possible risk exacerbated by their metabolic disturbance.
Acknowledgements We would like to extend sincere appreciation to the children who participated in the study. In addition, we are thankful to Mackay Memorial Hospital (94MMH-TMU-04) who funded this study.
References
1. Akinci A, Celiker A, Baykal E, Tezic T (1993) Heart rate variability in diabetic children, sensitivity of the time-and frequency-domain methods. Pediatr Cardiol 14:140–146 2. Akselrod S, Gordon D, Ubel FA, Shannon DC, Berger AC, Cohen
RJ (1981) Power spectrum analysis of heart rate fluctuation: a quantitative probe of beat-to-beat cardiovascular control. Science 213:220–222
3. Alberti KG, Zimmet PZ (1998) Definition, diagnosis and classification of diabetes mellitus and its complications. Part 1. Diagnosis and classification of diabetes mellitus. provisional report of a WHO consultation. Diabet Med 15:539–553 4. American Diabetes Association (2006) Standards of medical care
in diabetes—2006. Diabetes Care 29:S4–S42
5. Bellavere F, Balzani I, De Masi G, Carraro M, Carenza P, Cobelli C, Thomasseth K (1992) Power spectral analysis if heart-rate variation improves assessment of diabetic cardiac autonomic neuropathy. Diabetes Care 41:633–640
6. Chessa M, Butera G, Lanza GA, Bossone E, Delogu A, Rosa GD, Marietti G, Rosti L, Carminati M (2002) Role of heart rate variability in the early diagnosis of diabetic autonomic neuropathy in children. Herz 27:785–790
7. Colhoun HM, Francis DP, Rubens MB, Underwood SR, Fuller JH (2001) The association of heart-rate variability with cardiovascu-lar risk factors and coronary artery calcification: a study in type 1 diabetic patients and the general population. Diabetes Care 24:1108–1114.
8. Crocker PR, Bailey DA, Faulkner RA, Kowalski KC, McGrath R (1997) Measuring general level of physical activity: preliminary evidence for the Physical Activity Questionnaire for older children. Med Sci Sports Exer 29:1344–1349
9. Ewing DJ, Boland O, Neilson JM, Cho CG, Clarke BF (1991) Autonomic neuropathy, QT interval lengthening, and unexpected deaths in male diabetic patients. Diabetologia 34:182–185 10. Ewing DJ, Campbell IW, Clarke BF (1980) The nature history of
diabetic autonomic neuropathy. Q J Med 49:95–108
11. Ewing DJ, Campbell IW, Clarke BF (1981) Heart rate variability in diabetes mellitus. Lancet 1:183–186
12. Kardelen F, Akcurin G, Ertug H, Akcurin S, Bircan I (2006) Heart rate variability and circadian variations in type 1 diabetes mellitus. Pediatr Diabetes 7:45–50
13. Macor F, Fagard R, Amery A (1996) Power spectral-analysis of RR interval and blood- pressure short-term variability at rest and during dynamic exercise: comparison between cyclists and controls. Int J Sports Med 17:175–181
14. Mandigout S, Melin A, Fauchier L, N’Guyen LD, Courteix D, Obert P (2002) Physical training increases heart rate variability in healthy prepubertal children. Eur J Clin Investig 32:479–487 15. Melanson EL (2000) Resting heart rate variability in men
varying in habitual physical activity. Med Sci Sports Exerc 32: 1894–1901
16. Monahan KD, Dinenno FA, Tanaka H, Clevenger CM, DeSouza CA, Seals DR (2000) Regular aerobic exercise modulates age-associated declines in cardiovagal baroreflex sensitivity in healthy men. J Physiol 529:263–271
17. Nagai N, Hamada T, Kimura T, Moritani T (2004) Moderate physical exercise increases cardiac autonomic nervous system activity in children with low heart rate variability. Childs Nerv Syst 20:209–214
18. O’Brien IA, McFafffen JP, Corrall RJM (1991) The influence of autonomic neuropathy on mortality insulin-dependent diabetes. Q J Med 79:495–502
19. Ram Z, Sadeh M, Walden R, Adar R (1991) Vascular insufficien-cy quantitatively aggravates diabetic neuropathy. Arch Neurol 48:1239–1242
20. Rennie KL, Hemingway H, Kumari M, Brunner E, Malik M, Marmot M (2003) Effects of moderate and vigorous physical activity on heart rate variability in a British study of civil servants. Am J Epidemiol 158:135–143
21. Salvatoni A, Cardani R, Biasoli R, Salmaso M, De Paoli A, Nespoli L (2005) Physical activity and diabetes. Acta Biomed Ateneo Parmense 76:85–88
22. Sigal RJ, Kenny GP, Wasserman DH, Castaneda-Sceppa C, White RD (2006) Physical activity/exercise and type 2 diabetes: a consensus statement from the American Diabetes Association. Diabetes Care 29:1433–1438
23. Sochett E, Daneman D (1999) Early diabetes related complica-tions in children and adolescents with type 1 diabetes: implica-tions for screening and intervention. Endocrinol Metab Clin N Am 28:865–882
24. Stella P, Ellis D, Maser RE, Orchard TJ (2000) Cardiovascular autonomic neuropathy (expiration and inspiration ratio) in type 1 diabetes. Incidence and predictors. J Diabetes Its Complicat 14:1–6 25. Sztajzel J (2004) Heart rate variability: a noninvasive electrocar-diographic method to measure the autonomic nervous system. Swiss Med Wkly 134:514–522
26. Takase B, Kitamura H, Noritake M, Nagase T, Kurita, Ohsuza F (2002) Assessment of diabetic autonomic neuropathy using twenty-four-hour spectral analysis of heart rate variability: a comparison with the findings of the Ewing battery. Jpn Heart J 43:127–135
27. Task Force of the European Society of Cardiology and the North American Society of Pacing and Electrophysiology (1996) Heart rate variability: standards of measurement, physiological interpre-tation and clinical use. Circulation 93:1043–1065
28. The Expert Committee on the Diagnosis and Classification of Diabetes Mellitus (2003) Follow-up report on the diagnosis of diabetes mellitus. Diabetes Care 26:3160–3167
29. Vanelli M, Corchia M, Iovane B, Bernardini A, Mele A, Chiari G (2006) Self-monitoring adherence to physical activity in children and adolescents with type 1 diabetes. Acta Biomed Ateneo Parmense 77(Suppl 1):47–50
30. Vinik AI, Maser RE, Mitchell BD, Freeman R (2003) Diabetic autonomic neuropathy. Diabetes Care 26:1553–1579
31. Walsh MG, Zgibor J, Borch-Johnsen K, Orchard TJ; DiaMond Investigators (2004) A multinational comparison of complications assessment in type 1 diabetes: the DiaMond substudy of complications (DiaComp) level 2. Diabetes Care 27:1610–1617 32. Weston PJ, James MA, Panerai RB, McNally PG, Potter JF,
Thurston H (1998) Evidence of defective cardiovascular regulation in insulin-dependent diabetic patients without clini-cal autonomic dysfunction. Diabetes Res Clin Pract 42:141– 148
33. Wheeler SG, Ahroni JH, Boyko EJ (2002) Prospective study of autonomic neuropathy as a predictor of mortality in patients with diabetes. Diabetes Res Clin Pract 58:131–138
34. Yabe-Nishimura C (1998) Aldose reductase in glucose toxicity: a potential target for the prevention of diabetic complications. Pharmacol Rev 50:21–33
35. Yoshiharu Y, Hughson RL, Peterson JC (1991) Autonomic control of heart rate during exercise studied by heart rate variability spectral analysis. J Appl Physiol 71:1136–1142