DOI 10.1378/chest.114.2.393 1998;114;393-397
Chest
Chun-Yuh Yang, Meng-Chiao Lin and Kuang-Chi Hwang
Environment in a Subtropical Area
Childhood Asthma and the Indoor
http://chestjournal.chestpubs.org/content/114/2/393
services can be found online on the World Wide Web at:
The online version of this article, along with updated information and
ISSN:0012-3692
)
http://chestjournal.chestpubs.org/site/misc/reprints.xhtml
(
prior written permission of the copyright holder.
this article or PDF may be reproduced or distributed without the Dundee Road, Northbrook, IL 60062. All rights reserved. No part of Copyright1998by the American College of Chest Physicians, 3300 Physicians. It has been published monthly since 1935.
is the official journal of the American College of Chest
Chest
at Kaohsiung Medical University Library on May 11, 2012
chestjournal.chestpubs.org
Childhood Asthma and the Indoor
Environment
in
a
Subtropical
Area'
Chun-Yuh
Yang,
PhD,
MPH;Meng-Chiao
Lin, MD, MPH; andKuang-Chi
Hwang,
MDStudy
objectives:
Theobjective
of thisstudy
is to examine therelationship
between indoor environmental factors andchildhoodasthmain asubtropical
area.Design:
A case-controlstudy
wasperformed
using participants
of aprevalence
survey thatincluded 165 schoolchildren withasthma and 165 age-and
gender-matched
controlsubjects.
Setting:
Thestudy
was confined to 4,164 schoolchildrenaged
6 to 12 yearsattending eight
primary
schoolsinKaohsiung
County
ruralmunicipalities
whoparticipated
inaprevalence
study
concerning
the healtheffects of the indoorenvironment.Participants:
Cases(n=165)
were defined as children with current asthma confirmedby
aphysician.
Controlsubjects
(n=165)were selected from thesame school and class and matchedfor age and
gender,
andthey
didnothaveaprevious
diagnosis
ofasthma,
history
ofphysician-confirmed
atopic
diseases,
persistent
wheezing,
cough,
orphlegm,
orreported
chestillness,
pneumonia,
orbronchitis.Measurementsand results: Information
regarding
the home environmentwasobtainedusing
astructuredwritten
questionnaire,
completed by
theparents of the children. Of the many indoor environmental factors includedin thisstudy, only
homedampness
showedan associationwithasthma
(odds ratio=2.65).
Conclusions:Weconclude that
dampness
inthehomeisanewpublic
healthissueinsubtropical
areas.(CHEST
1998;114:393-397)
Keywords: asthma;case-control
study;
dampness;
indoorenvironmentAbbreviations: CI=confidenceinterval; OR=oddsratio
4
sthma,
which is animportant
medicalproblem
^*-worldwide,
is the most common chronic diseaseamong
pediatric
patients.
It often leads tocostly
treatment,
disability,
and school absence.1-2 Theprevalence
of asthma indeveloping
countries has increasedinrecentyears.3
Theprevalence
of asthmain schoolchildren in
Taipei
increased from 1.3% in 1974to5.1%in 19854andto 10.8%in 1994(unpub¬
lished
data;
K.H.Hsieh;
NationalTaiwanUniversity
Hospital;
1994).
Asthma is also the most common
lung
diseaseassociatedwith indoorair
pollution.5
Mostpeople
insubtropical
areasspend
much oftheir lifeindoors,
and concern about the health effects of the indoor
environmenthas been
growing
in recentyears.6
The *Fromthe SchoolofPublicHealth,Kaohsiung
MedicalCollege,
Kaohsiung,
Taiwan, ROC.Supported
inpartby
agrantfrom the NationalScienceCouncil,ExecutiveYuan, Taiwan(NSC-84-2621-P-037-001).
ManuscriptreceivedOctober21,1997;revisionacceptedJanuary
8, 1998.
Correspondence to: Chun-Yuh Yang, MD, School of Public Health,
Kaohsiung
Medical College, 100 Shih-Chuan 1st RD,Kaohsiung, Taiwan 80708;email:chunyuh@cc.kmc.edu.tw
indoor environment in
developing
countries is sub¬jected
topollutants
from numerous sources.7 In1994,
we conducted alarge questionnaire-based
study
oftherespiratory
health effects of the indoorenvironment inthe ruralareasof
Kaohsiung
County,
which has a
subtropical
climate. This article focuses onthepossible
associationbetween indoorenviron¬mental factors and asthma among
participants
of thisprevalence
surveyofelementary
schoolchildren.Materials and Methods
Study
Areas andSurveyProceduresFourmunicipalitiesinKaohsiungwereselected for thepresent
study
basedontheurban-rural classificationinTaiwan.8Accord¬ing to this classification, each municipality was given a 1 to 8
urbanizationcategory7. Municipalitieswith the
highest
urbaniza¬ tionlevel,suchastheTaipeimetropolitanarea,wereassigned
tocategory 1,while
municipalities
withthelowest urbanization levelwere
assigned
to category 8. The fourmunicipalities
selectedwere
predominantly
rural andthey
wereassigned
tocategory8.The rural areas selected forthepresent
study
also hadnolocal sources of industrialairpollution.9These areaswerejudgedtothe healthof childrenintheseareas was
unlikely
tobe influencedby
regional
airpollution.
Webelieve that the levels andtypesofoutdoorair
pollution
wereessentially
similarinthestudiedareas. All16public
primaryschools within thestudy
areasagreed
toparticipate in the
study.
A randomsample
ofone halfoftheprimary schools was chosen. All school
buildings
are made ofconcreteandthe conditions inside the classroomsarealmostthe same.with no
particular
indoor airpollution
sources for thestudied schools. All children from the first
through
the sixthgrades
(children6to 12yearsofage)
intheeight
schoolswereenrolledinthis
study.
Sample
sizes inparticipatingschools varied from350to700pupils.
Aquestionnairethatevaluatedrespiratoryillnesses and symp¬
tomsofchildrenwas distributed tothechildren inthepartici¬
patingschools
by
theirteachersduring
theperiod
fromSeptem¬bertoNovember, 1994. Thequestionnairewas
completed
by
aparent or
guardian
most familiar with the child's health andreturnedtotheschool.Thequestionswereobtainedormodified from other
previously
usedquestionnaires,namely,
theAmericanThoracicSociety-DivisionofLungDiseaseRespiratorySymptom
Questionnaire,10 which was used in the Harvard Six Cities
Study,11
andthe questionnaireusedby
the Health andWelfareDepartmentinCanadafora
community-based
study
of children'shealth.12
Fromthe questionnaire, the
following
factorswere assessed:environmental exposures in the homes of a chemical nature,
including
presence ofahouseholdsmokerinthehome;exposure to gascooking appliances;
mosquitorepellant burning;
andincense
burning.
Otherenvironmentalfactorsofaphysical
naturesuch aswhetherthe housecontained anaircleaner,
dehumidi-fier,orairconditioner,and other
biologic
factorsincluding family
ownership
offurry
pets, carpeting,plants
inside thehome, and homedampness
werealsoassessed.Homedampness
wasdefinedaspresence ofanyoneof the
following:
visiblemold ormildewgrowth
onthe surfaces inside thehome, appearance ofstanding
waterwithin the home;water
damage;
orwaterleaks into thebuilding.
Study Subjects
The
subjects
for the presentcase-controlstudy
wereselected fromtheparticipantsoftheprevalence study.
Thequestionusedforcasedefinitionwas"Hasthe childeverhad asthma
diagnosed
by
adoctor?" Thecontrolsubjects,
selectedfromthesameschool and class and matchedonageandgender,
didnothaveapreviousdiagnosis
ofasthma,history
ofphysician-confirmed
atopic dis¬ eases,persistentwheezing, cough,
orphlegm,
orreported
chestillness,pneumonia, orbronchitis.
Itwasestimatedthat,ifthetrueoddsratio(OR)was2,inorder
to detect an association betweenindoor environmental factors
and asthma witha
specificity
of95% (a=0.05) and apower of 80% (B=0.2),asample
sizeof75casesandanequal
numberof controlsubjectswouldbeneeded.13Statistics
Allstatistical
analyses
wereperformed
usingstatistical software(Statistical
Analysis
System; SAS; Cary, NC). A conditionallogistic
regression model was used to calculate OR and 95% confidence intervals (CIs)adjusted
for other risk factors and forpotential confounding
factors.14 All statistical tests were twosided.
Covariables used to adjust the associations between indoor environmental factors and asthma included the
following:
age,gender,
highest
level of education achievedbyeitherparent,the child'sallergies,
eg,tofood, dust,orpollen,parental
asthma,andbreast
feeding.
Results
The
parents
of all 4,389 children enrolled in theeight
schoolsstudied receivedaquestionnaire;
4,213(96%)
questionnaires
were returned.Complete
in¬formationwas availableon
4,164
children. Theprev¬alence of asthma was 4%
(n=165)
and anequal
number of matched control
subjects
wereidentified.The
prevalence
is less than thatreported
by
aprevious
study
conducted inTaipei.4
Thisprevious
study,
however,
usedadifferentcasedefinition(they
definedcases as "achild who had hadat least three
recurrent,
paroxysmal
attacks ofwheezing
anddys¬
pneain the
past
12months")
andwas conductedinan urban area.
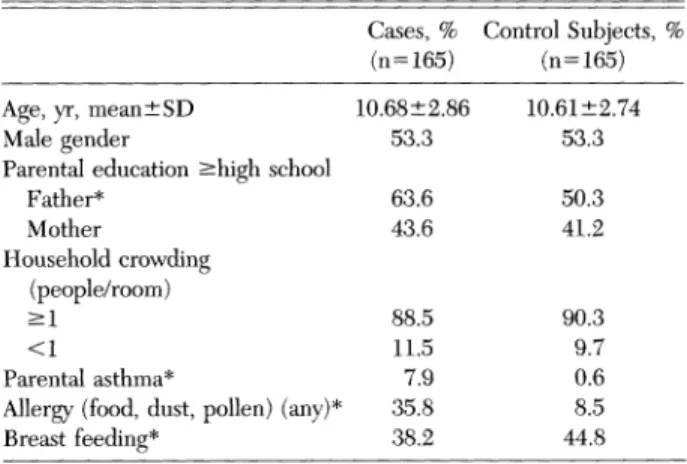
Table 1shows the distribution ofcasesand control
subjects by
selectedpersonal
characteristics. Therewere morecasesthancontrol
subjects
withallergies,
afamily
history
of asthma(parental
asthma),
andhigher
paternal
education. Control mothers breastfed their child more often than case mothers did.
Having
ahistory
ofpneumonia
ortonsillectomy
wasnot
reported by
any ofthe cases or controlsubjects
(not
shown in Table1).
Table 2 shows the indoor environmental charac¬ teristicsofthe
study subjects.
Therewere nonotabledifferences between the cases and control
subjects
with
regards
tohouseholdsmoking,
useofdehumid-ifiers,
useofanaircleaner,
useofanairconditioner,
owning
furry
pets,
useofcarpets,
mosquito
repellent
burning,
andhaving plants
inside the home. Homedampness
had apositive
andstatistically significant
associationwith asthma.
However,
anegative
associ¬ation was observed between asthma and incense
burning
andfrequency
ofgascooking.
AsshowninTable
3,
asthmawasonly
significantly
associated with home
dampness
(OR=2.65,
95%01=1.52,
4.62)
when conditionalmultiple
logistic
regression
was used to obtain estimates ofassocia-Table 1.Characteristics
of
theStudy Population
Cases, % ControlSubjects,(n=165) (n=165)
Age,yr,mean±SD
Malegender
Parental education^highschool Father* Mother Householdcrowding (people/room) >1 <1 Parentalasthma*
Allergy(food,dust,pollen)(any)"*
Breastfeeding* 10.68±2.86 53.3 63.6 43.6 88.5 11.5 7.9 35.8 38.2 10.61±2.74 53.3 50.3 41.2 90.3 9.7 0.6 8.5 44.8 *p<0.05. 394 ClinicalInvestigations
at Kaohsiung Medical University Library on May 11, 2012
chestjournal.chestpubs.org
Table 2.Crude ORand95% CI
of
Indoor EnvironmentalFactors and AsthmaFactors
Cases, Control
No. Subjects,No. OR(95% CI) Householdsmoking None Any Useofadehumidifier No Yes
Useofanaircleaner
No Yes
Useofanairconditioner
No Yes Furrypets No Yes Carpets No Yes
Mosquitorepellent burning No
Yes
Incenseburning* No
Yes
Plantsinside the home
No Yes Gascooking* <l/d >l/d Homedampness* No Yes 75 90 140 25 157 31 134 120 45 144 21 79 72 93 89 76 21 144 44 121 67 98 136 29 158 38 127 105 60 144 21 103 62 41 124 99 66 10 155 85 80 1.00 0.83(0.54-1.27) 1.00 0.83(0.46-1.51) 1.00 1.16(0.39-3.47) 1.00 1.32(0.76-2.29) 1.00 0.67(0.43-1.06) 1.00 1.00(0.52-1.92) 1.00 1.51(0.98-2.35) 1.00 0.42(0.25-0.68) 1.00 1.28(0.83-1.93) 1.00 0.48(0.24-0.96) 1.00 2.95(1.80-4.84) *p<0.05.
tions
adjusted
for other risk factors. ORs wereadjusted
for age, sex,parental
education,
parental
asthma,
physician-confirmed allergy
to food ordust,
etc, and breast
feeding.
Afteradjustment
for thesefactors,
gascooking
and incenseburning
were notsignificantly
associated with asthma.Discussion
The
present
case-controlstudy
indicated that re¬ported
homedampness
wastheonly
indoorenviron¬mental factor that is associated with asthma for
children
residing
inKaohsiung
rural areas. Thisfinding
is inagreement
with thefindings
of otherepidemiologic
studies.1523Determinationofthe presenceof home
dampness
in this
study
relies onself-reporting
and therefore wassubjective.
Ifdampness
iswidely
held to be a cause ofasthma,
an association basedentirely
onself-reported
information should be considered pronetoreporting
bias. This could bepossible
iftheparents
ofasthmaticchildrenreport
dampness
inthehome more
readily
than those whose children arenot asthmatic. This seems
unlikely,
however,
be¬ cause thepotential
role ofdampness
in thehome as arisk factor for asthma hasnotreceived muchpublic
attention in Taiwan.
Since determination of the presence of home
dampness
was basedentirely
onself-reporting,
thiscould result in misclassification of exposure and reduce the observed associations. However, several studies have
reported
thevalidity
ofself-reported
housing
conditions andindependent
objective
as¬sessments of
temperature,
humidity,
and moldgrowth.19'20'24-26
Inaddition,
thequestionnaire
didnotfocus
exclusively
ondampness
inthe home. Thequestions
related todampness
in the home andgrowth
of molds werewidely separated
inthe ques¬tionnaire and the
respondents generally
did notknow that
dampness
in the home and molds couldcause adverse health effects.
Therefore,
itwould bereasonable to believe that it is
unlikely
thatoverre-porting
orunderreporting
ofdamp housing
condi¬tions could have biased the
study
results.Though
differences inquestionnaire
design,
lan¬ guage,climate,
andhousing
conditions mayexist,theORs found inthe
present
study
are similar to thosereported
from other countries.1517'2022 The consis¬tency
of our results with those ofprevious
studiesmeets one of the criteria for an
epidemiologic
asso¬ciationto beconsidered causal.
Therefore,
the asso¬ciations between asthma and
dampness
inthe homeare
probably
causal,
although
doubtremainsbecauseofthe
subjective
nature of theself-reporting.
Fungi,
house dust mites, and cockroaches areknown tobe more
prevalent
indamp
homes than indry
homes,
and allare knowntoproduce
substancesthat may
trigger
allergic
reactions.27-35Taiwanis in asubtropical
climate,
andhigh
relativehumidity
(>80%)
occursthroughout
the year. House dustmites and
fungi
are themajor
allergens
in oursubtropical
area.36Aspergillus,
Penicillium,
andCla-dosporium
are thepredominant
genera, and theirTable
3.Adjusted
ORs (95% CIs)for
theAssociation RetweenIndoor EnvironmentalFactorsand Asthma*Variable CrudeOR AdjustedOR(95%CI)
Gascooking Incenseburning Home dampnessf 0.48 0.42 2.95 1.16(0.50-2.68) 1.53(0.90-2.58) 2.65(1.52-4.62)
*Adjustedfor age, sex, parentaleducation, parentalasthma, physi¬
cian-confirmedallergytofood, dust,orpollen, andbreastfeeding.
indoor levels are
higher
than levelsin otherparts
ofthe world.3738 A
previous
study
has demonstrated thevalidity
ofquestions
inregard
todampness
andmolds as indicators of indoor mold
growth,
and therespondent's
perception
of homedampness
hasbeen correlated with measured spore levels.20 In thepresent
study,
however,
the concentrationsoffungi,
house dust mites, and cockroaches were not deter¬mined.
Therefore,
there is no direct evidence toshow that this mechanism is
responsible
for theobserved associations between
dampness
of the home and asthma.The indoor environmental factors that have re¬
ceived the most attention in the
past
are environ¬mental tobacco smoke and
directly
orindirectly
measured
nitrogen dioxide,
whichmainly
comesfrom gas
cooking appliances. Although
manystudies have shown astatistically significant relationship
between
passive
smoking
and childhood asth¬ma,111839-45
ourstudy
did not. This inconsistentfinding
maybe duepartly
tothe fact thatwedidnot assess whether household smokersactually
smokedindoorsor
because,
indeveloping
countries, manyofthose who smoke
actually
smokeonly
a fewciga¬
rettes per
day.
Also we did not determine whichparent
smoked. This could beimportant
since ma¬ternal
smoking
indoorsmaybeagreater
riskfactortochildren.
Furthermore,
almost all the students in rural Taiwan walk to school. We think that theprobability
that the effects ofparental
smoking
inside the car with the childrenpresent
may haveaffected ourresults is
negligible.
We didnot findanassociation between gas cook¬
ing
andasthma. Thisresultis consistentwith severalother
reports
that also found that the use of gascooking appliances
was notsignificantly
associatedwith asthma.1141-44'46In
reality,
itwasnotpossible
tosee any
impact
of gasstove use onrespiratory
healthbecause
nearly
91% of the homes of thestudy
subjects
(87.3%
of thecasesand93.9%ofthecontrolsubjects)
used gas stoves for foodpreparation
morethan onetime per
day.
The
burning
of Chinese incense forworshipping
deities is adaily
routine for most Chinese. Thesmoke
produced by
thispractice
has been found tocontain
formaldehyde.47
Exposure
toindoor formal¬dehyde
may cause asthma48 or asthma-like symp¬toms.49 Incense
burning
was not shown to be asignificant
risk factorinthisstudy (adjusted
OR,
1.53[CI,
0.90 to2.58]).
Burning
mosquito
repellents
isa common sourceof indoorairpollution
insubtropical
rural areas. In this
study,
theprevalences
of mos¬quito
repellent burning
were 47.9% and 37.6% forthecases and the control
subjects,
respectively.
Thepotential
harmfulness ofproducts produced
by
burn¬ing mosquito
repellent
has beenacknowledged.50
Two studies conducted in
tropical
countries havefound that exposure to
mosquito
repellent
smokewasassociated withasthma.5152Inthis
study,
wedidnotfind anassociationbetweeneitherincenseburn¬
ing
smoke ormosquito
repellent
smoke exposureandasthma.
However,
theirpotential
forharm mer¬its further
study
insubtropical
areas.In
conclusion,
in thisstudy,
weinvestigated
therelationship
between several indoor environmental factors and childhood asthma. Of the many indoorenvironmental factors included in this
study,
only
home
dampness
was found to be associated withasthma. This
finding
supports
thehypothesis
ofanassociationbetween asthma and
reported
dampness
in thehome,
which has been observed in otherrecent
epidemiologic
studies. In view of thehigh
relative
humidity
insubtropical
areasand the resultsof the
present
study,
homedampness
shouldbecomea new
public
health issue for Taiwan'spopulation.
The
possible
adversehealth effects ofdamp
housing
deservefurtherstudy.
References
1 WeissKB, Gergen PJ,
Hodgson
TA. Aneconomicevaluation of asthmaintheUnitedStates. NEngl
JMed1992;326:826 2 Marion RJ, Creer TL,Reynolds
RVC. Direct and indirect costs associatedwithmanagementof childhoodasthma.AnnAllergy
1985;54:31-343 CooksonJB. Prevalenceratesof asthmain
developing
coun¬tries and theircomparisonwith tiiose inEuropeand North America. Chest1987;9L97S-103S
4 Hsieh KH, Shen JJ. Prevalence of childhood asthma in
Taipei, Taiwan, andotherAsianPacificcountries.JAsthma 1988;25:73-82
5 SametJ. Environmental controls and
lung
disease. Am RevRespirDis 1990; 142:915-39
6 Samet JM,
Marbury
MC,Spengler
JD. Health effects and sources of indoorairpollution:
part I. Am RevRespir Dis 1987; 136:1486-15087 ChenBH,HongCJ,
Pandey
MR,etal. Indoorairpollution
indeveloping
countries. World HealthStat Q1990;43:127-36 8 TzengGH,Wu TY.Characteristics of urbanizationlevels inTaiwandistricts.
Geograph
Res 1986; 12:287-3239 MinistryofEconomics, Taiwan(ROC). Censusofmanufac¬ turers.Taipei: MinistryofEconomics,Taiwan (ROC), 1989 10 Ferris BG.
Epidemiology
standardization project. Am RevRespirDis 1978; 118:36-47
11 WareJH,
Dockery
DW, SpiroA,etal. Passivesmoking,
gascooking,
andrespiratoryhealth ofchildrenliving
in sixcities. AmRevRespirDis 1984;129:366-7412 Stern B, Jones L, Raizenne ME, et al. Respiratory health
effects associated with ambient sulfates and ozone in two
rural Canadian communities. Environ Res 1989;49:20-39
13 SchlesselmanJJ. Casecontrolstudies:designconduct
analy¬
sis. NewYork: OxfordUniversityPress, 1982; 143-70
14 BreslowNE,DayNE.Statistical methodsincancerresearch
(vol 1): the
analysis
of case-control studies. Lyon: Interna¬tionalAgencyfor ResearchonCancer, 1980;248-79 15 Brunekreef B,
Dockery
DW, Speizer FE, et al. Homedampness
and respiratorymorbidity
in children. Am RevRespirDis 1989; 140:1363-67
396 ClinicalInvestigations
at Kaohsiung Medical University Library on May 11, 2012
chestjournal.chestpubs.org
16 BrunekreefB.Associationsbetweenquestionnairereportsof
home
dampness
and childhood respiratory symptoms. SciTotalEnviron 1992; 127:79-89
17 Dales RE,
Zwanenburg
H, Burnett R, et al. Respiratory health effects ofhomedampness
andmoldsamong Canadian children.AmJEpidemiol
1991; 134:196-20318 DekkerC,Dales R, BartlettS,etal. Childhood asthma and theindoorenvironment.Chest1991; 100:922-26
19 Platt SD, Martin CJ, Hunt SM, et al. Damp
housing,
moldgrowth,
andsymptomatichealthstate.BMJ1989;298:1673-78 20Waegemaekers
M,VanWageningenN,BrunekreefB, etal. Respiratorysymptomsindamp
homes: apilot
study.
Allergy
1989;44:192-9821
Jaakkola
JJK,Jaakkola
N, RuotssalainenR. Homedampness
and molds as determinants of respiratory symptoms and asthmainpre-school
children. J ExpoAnalEnvironEpide¬
miol1993;3(suppl
l):129-4222 Strachan DP, Sanders CH. Damp
housing
and childhood asthma: respiratory effects of indoor air temperature and relativehumidity.
JEpidemiol
Community Health 1989; 43:7-1423 Strachan DP. Damp
housing
andchildhoodasthma: valida¬ tionofreportingofsymptoms. BMJ1988;297:1223-26 24 Martin CJ, Platt SD, Hunt SM. Housing conditions andill-health. BMJ1987; 294:1125-27
25
Hyndman
SJ. Housingdampness
andhealthamongstBritishBengalis
inEastLondon. Soc Sci Med1990;30:131-41 26 Wickman M,Graveson S, Nordvall SL, etal. Indoor viabledust-bound
microfungi
inrelationtoresidential characteris¬tics,
living
habits, andsymptoms inatopic and control chil¬ dren.JAllergy
Clin Immunol1992; 87:752-5927
Korsgaard
J.Miteasthma andresidency.
AmRevRespirDis 1983; 128:231-3528
Blythe
ME. Someaspectsoftheecological study
of the house dustmites. BrJDis Chest1976; 70:3-3129 Smith JM. Clinical
findings
inchildren withallergy
tothe house dustmites. ActaAllergy
1970;25:37-4030 Burr ML, Mullins J, MerrettTG, et al. Indoor molds and
asthma.JRSocHealth 1988; 108:99-101
31 Gravesen S.Fungias a causeof
allergic
disease.Allergy
1979; 34:134-5432
Salvaggio
J,AukrustL. Moldinduced asthma.JAllergy
ClinImmunol 1981;68:327-46
33 KangB.
Study
oncockroach antigenasaprobable
causativeagent in bronchial asthma. J
Allergy
Clin Immunol 1976; 58:357-6534 Twarog FJ, Picone FJ, StrunkRS,et al. Immediate
hyper¬
sensitivitytocockroach:isolation and
purification
of themajorantigens.J
Allergy
ClinImmunol1977;59:154-6035 GelberLE,SeltzerLH,BouzoukisJK,etal.Sensitizationand exposuretoindoor
allergens
asrisk factors for asthma amongpatients presenting to
hospital.
Am Rev Respir Dis 1993; 147:573-7836 LiCS,WanGH,HsiehKH,etal.Seasonalvariationsofhouse dust mite
allergen
(Der p I) in thesubtropical
climate. JAllergy
Clin Immunol1994;94:131-3437 Li CS, Kuo YM.
Microbiological
indoorairquality
in sub¬tropical
areas. Environ Int1993; 19:233-3938 Kuo YM, Li CS. Seasonal
fungus prevalence
inside andoutside of domesticenvironments inthe
subtropical
climate.Atoms Environ1994;28:3125-30
39 Gortmaker SL, Walker DK,
Jacobs
FH, et al. Parentalsmoking
and the risk of childhood asthma. Am J PublicHealth1982;6:574-79
40 Somerville SM, Rona RJ, Chinn S. Passive
smoking
andrespiratoryconditionsinprimaryschoolchildren.J
Epidemiol
CommunityHealth 1988;42:105-1041 Ogston SA,
Florey
CV, Walker CHM. TheTayside
infantmorbidity
andmortality study:
effectonhealth ofusinggasfor
cooking.
BMJ 1985;290:957-6042 Weitzman M, Gortmaker S, Walker DK, et al. Maternal
smoking
andchildhoodasthma. Pediatrics 1990;85:505-11 43Dodge
R.Theeffects of indoorpollution
onArizonachildren.Arch EnvironHealth1982;37:151-55
44 MeliaRJW,
Florey
CV, Morris RW,etal. Childhoodrespi¬ratory illness and the home environment: II. Association betweenrespiratoryillness andnitrogen dioxide,temperature
andrelative
humidity.
IntJEpidemiol
1982; 11:164-69 45 EhrlichR,KattanM,GodboldJ,etal. Childhoodasthmaandpassive
smoking:
urinarycotinineas abiomarker of exposure.AmRevRespirDis 1992; 145:594-99
46 Schenker MB, Samet JM, Speizer FE. Risk factors for
childhoodrespiratorydisease: the effect of host factors and
home environmental exposures. Am Rev Respir Dis 1983; 128:1038-43
47 Lin JM,WangLH. Gaseous
aliphatic aldehydes
inChineseincensesmoke. BullEnvironContamToxicol1994;53:374-81 48 WieslanderG, Noorback D,Bjornsson E,etal.Asthmaand
the indoor environment: the
significance
of emission offormaldehyde
and volatile organiccompounds
fromnewly
painted
indoor surfaces. Int Arch Occup Environ Health 1997;69:115-2449 NorbackD, Bjornsson E, Janson C, etal. Asthmatic symp¬
toms and volatile organic
compounds, formaldehyde,
andcarbon dioxide in
dwellings.
Occup Environ Med 1995; 52:388-9550 World HealthOrganization. Safeuse of
pesticides.
Geneva: World Health Organization, 1985;21-4651 AziziBHO, HenryRL.The effectsof indoorenvironmental factors on respiratory illness in primary school children in
KualaLumpur.IntJ
Epidemiol
1991;20:144-5052 AziziBHO, ZulkifliHI, Kasim MS. Indoorair
pollution
andasthma in
hospitalized
children in atropical
environment.DOI 10.1378/chest.114.2.393 1998;114; 393-397
Chest
Chun-Yuh Yang, Meng-Chiao Lin and Kuang-Chi Hwang
Childhood Asthma and the Indoor Environment in a Subtropical Area
May 11, 2012 This information is current as of
http://chestjournal.chestpubs.org/content/114/2/393
Updated Information and services can be found at:
Updated Information & Services
http://chestjournal.chestpubs.org/content/114/2/393#related-urls
This article has been cited by 4 HighWire-hosted articles:
Cited Bys
http://www.chestpubs.org/site/misc/reprints.xhtml
found online at:
Information about reproducing this article in parts (figures, tables) or in its entirety can be
Permissions & Licensing
http://www.chestpubs.org/site/misc/reprints.xhtml
Information about ordering reprints can be found online:
Reprints
"Services" link to the right of the online article.
Receive free e-mail alerts when new articles cite this article. To sign up, select the
Citation Alerts
PowerPoint slide format. See any online figure for directions.
articles can be downloaded for teaching purposes in
CHEST
Figures that appear in
Images in PowerPoint format
at Kaohsiung Medical University Library on May 11, 2012
chestjournal.chestpubs.org