Article type: Original
Article title: Outpatient Visits by Dentists: A Nationwide Cohort Study in Taiwan
Short running head: MORBIDITY OF TAIWANESE DENTISTS
Authors full names, affiliations and addresses: Chang-Ta CHIU1,
Shu-Min HUANG2, Yu-Wen LIN2, Ming-Chung KO3, Chung-Yi LI4,5
1. Department of Dentistry, Sin Lau Christian Hospital, #57, Sec. 1, Dongmen Rd., Tainan 701, TAIWAN.
2. Department of Public Health, College of Medicine, Fu-Jen Catholic University, #510 Chung-Cheng Road, Hsinchuang, New Taipei City 242, TAIWAN.
3. Department of Surgery, Taipei City Hospital, #145 Zheng Zhou Road, Taipei 103, TAIWAN
4. Department of Public Health, College of Medicine, National Cheng Kung University, #1 University Road, Tainan 701, TAIWAN.
5. Department of Public Health, College of Public Health, China Medical University, #91 Hsueh-Shih Road, Taichung 404, TAIWAN.
Ming-Chung KO and Chung-Yi LI contributed to this article equally.
Correspondence to: Ming-Chung Ko, MD, MSc
Department of Surgery, Taipei City Hospital 145 Zheng Zhou Rd., Taipei, Taiwan 103 e-mail: [email protected]
Abstract
We conducted a cohort study of 7,760 dentists in Taiwan between 2003 and 2007 to assess the risk of outpatient visit among dentists. Control groups included physicians and other health personnel. Over the 5-year study period, the dentist cohort made a total of 270,712
outpatient visits, representing an incidence rate of 7,038 visits /103 person-years. Compared to physicians, dentists experienced a
significantly reduced covariate adjusted rate ratio (ARR) for all-cause visits (ARR=0.59, 95% CI=0.58-0.59), as well as for nearly all other causes, except neoplasm (ARR=1.06, 95% CI=1.02-1.09). Compared to other health personnel, the dentists still experienced a significantly reduced ARR for all causes (ARR=0.70), but had a slightly but
significantly increased risk for endocrine/metabolic/immunity (ARR= 1.04, 95% CI=1.02-1.05) and mental (ARR=1.04, 95% CI=1.01-1.07) disorders. Although the dentists in Taiwan utilized lesser outpatient visits than did their medical colleagues, they tended to have slightly higher rates of outpatient visits for neoplasm, endocrine/metabolic/immunity disorders, and mental illnesses. Policy makers and hospital
administrators must not overlook dentists’ potentially unseen health problems. A mandatory periodical physical examination for dentists can seriously be considered.
Introduction
Like many other health care workers, dentists are in the forefront position of health care system and their health is critical to the quality of oral care received by patients. Compared to the general population, dentists were frequently found to experience lower rates of morbidity and mortality, mainly due to their relatively healthy lifestyle and better knowledge in disease prevention1-3). Despite that, the health of dentists should not be overlooked because it has been well recognized that various occupational and work environmental hazards could pose adverse effects to dentists,including musculoskeletal4-5) / connective tissue6) disorders, skin disease7), metabolic disorder8), infection9-11), gastroenterological disorder12), and cancer13,14). Sporadic reports also suggested increased risks of suicide in dentists because of stress,
burnout, depressive symptoms associated with dental practice15,16), and of miscarriage in female dentists due to occupational exposure to certain work related hazards such as acrylate compounds, mercury amalgam, solvents or disinfectants17).
Since the launch of the National Health Insurance (NHI) program in 1994, the health services industry in Taiwan has changed dramatically. The universal health insurance removed barriers to health care for those newly insured, enabling them more access to health care. By the end of
2004, more than 98% of the Taiwanese people were covered by the NHI program18). The annual medical statistics showed that the annual
prevalence rate of dental visit in Taiwan increased from 32.0% in 1999 to 42.7% in 200819).Due to increased demand in the health care
environment, the health care personnel have encountered heavy workload strain and psychosocial demand20). Taiwan’s dentists also seemed to experience higher workloads than their counterparts in Western nations. According to the 2009 World Health Organization Statistical Information System Report21), the US had the most adequate provision of dentists in the world in 2000-2007, with a figure of 16 dentists / 10,000 people, followed by Canada and Greek (both were 12 dentists / 10,000 people). In Asia, the dentist density was relatively low, with higher figures noted in Japan (7 dentists / 10,000 people) and Philippine (6 dentists / 10,000 people). The figure for Taiwan was 4.28 dentists /10,000 people21). Additionally, the annual prevalence rate (42.7% in 2008)19) of dental visit in Taiwanese was similar to those reported in some European nations areas including Ireland (40.90%), France (48.39%) and Belgium (49.69%), higher than the figures of Poland (23.76%), Spain (25.37%), and Italy (36.76%), but much lower than those reported in others including The Netherlands (65.73%), Germany (75.64%), Sweden (81.55%), Switzerland (73.73%), and Denmark (80.43%)22). Epidemiological evidence has shown that heavy
work load is associated not only with elevated risks of mental disorders but also with adverse effects from diseases of the circulatory system through triggering the release of catecholamine and increased blood pressure, both of which are known risk factors for cardiovascular diseases23).
Morbidity and mortality have been frequently investigated previously in Taiwan to associate various health care professionals including
physicians24), nurses25), and physicians of Chinese medicine26). Despite acknowledging the work related hazards in clinical settings and the increasing heavy workload among the dentists in Taiwan, there have been little information concerning the morbidity of Taiwanese dentist population. This study used the NHI claim data with a cohort study design to investigate this understudied issue, i.e., the risk of outpatient visit in the dentist population in Taiwan. Unlike
infection/chemical/physical hazards that usually target specific organs, the psychosocial hazards may cause the whole-body effect. Thus, in addition to certain illnesses previously reported to be associated with dental practice, this study was also design to systematically investigate the major disease categories in the dentist population of Taiwan.
Subjects and Methods
Sources of data
Data used in this study were retrieved from several claim files of the National Health Insurance Research Database (NHIRD) provided by the Bureau of National Health Insurance (BNHI), Department of Health and managed by the National Health Research Institutes (NHRI). The
universal NHI program has been implemented in Taiwan since March 1995. By the end of 1996, more than 96% of people in Taiwan were covered in the NHI program27) and the Bureau of NHI contracted with 97% of hospitals and 90% of clinics all over the nation27). The NHIRD has accumulated eight different registries and eight claims files reported from all contracted hospitals and clinics. Details of both registry and claims files are described elsewhere27). We used the registry for medical personnel (2002), the outpatient claims for 2003 to 2007, and an
updated registry for beneficiaries (2003-2007). To ensure the accuracy of the claim files, the BNHI performs expert reviews on a random sample of every 50–100 outpatient and inpatient claims quarterly and false report of diagnosis results in severe penalty from the BNHI28). The datasets used in this study can be inter-linked by the scrambled unique
individual’s personal identification number (PIN). The NHRI safeguards the privacy and confidentiality of all beneficiaries and transfers the
health insurance data to health researchers after ethical approval has been obtained. In this analysis, access of the NHIRD has been approved by both the NHRI and the Fu-Jen Catholic University Medical School Ethics Review Board (#C-9703).
Identifications of study subjects and data linkage
The registry of medical personnel covers information on
demographic characteristics and contract status with the NHI for various health professionals including dentists, physicians, physicians of Chinese medicine, pharmacists, nurses, medical laboratory technicians,
radiological technologists, speech-language therapists, physical and occupational therapists, and dieticians. Based on the registry of 2002, a total of 7,760 dentists were identified on the last day of 2002, and was used as the study cohort. At the same time, we identified two groups of medical workers as references for comparison. One group consisted of 23,211 physicians who also had contracts with the NHI. The other
reference group consisted of 56,788 health personnel other than dentists or physicians.
For each study subject, we linked her PIN to the outpatient visit claim data to retrieve information on outpatient visits between 2003 and 2007. A linkage was considered successful only when the outpatient visit occurring within the period of contract for these three study groups. In
total, the cohort of dentists encountered a total of 270,712 outpatient visit in the period of 2003-2007. The number of visits made by
physicians and the other health personnel was 1,143,136 and 2,814,509, respectively during the same period.
Statistical analysis
We used the person-year approach under the Poisson assumption to calculate the incidence rate of outpatient visit during the follow-up period. The incidence rate was calculated for all causes as well as for 14 major disease categories based on the International Classification of Disease 9th version, Clinical Modification (ICD-9-CM) codes. Through linkages to the beneficiary registry, we were able to identify the study subjects who terminated their enrollment in the NHI program for various reasons such as mortality and emigration between 2003 and 2007. Termination of the contract with the NHI program for dentists and the subjects from two control groups can also be noticed from the updated registry of medical personnel. The study subjects who were no longer insured in the NHI program were all considered censored in the
calculation of person-years being followed for each individual. The person-years observed for each individual was then calculated between January 1, 2003 and either December 31, 2007 (for those uncensored) or the date of censoring (for those censored). The total person-years
observed for dentists, physicians, and other health personnel were 38,463.8, 115,117, and 281,997.5, respectively.
To make comparisons of all-cause and cause-specific incidence rates between the dentist group and the two reference groups, we used the log-linear model with the natural logarithm of incidence rate as the dependent variable to fitted grouped data with simultaneously adjusting for age (5 categories), gender (2 categories), insurance premium (4 categories), place of practice (6 categories), contracted category of affiliation (4 types), and urbanization for the area of practice (3 categories) according to the National Statistics of Regional Standard Classification29). The log-linear model was fitted with standard Poisson distribution assumption and was used to assess the variation of
incidence rates of outpatient visit among the three study groups30). The ratio of two incidence rates adjusted for potential confounders (i.e., adjusted rate ratio, ARR) was calculated using the formula em, where m
is the regression coefficient. The ARR was used to estimate the covariate adjusted relative risk in this study. We adjusted geographic variables for presence of an urban-rural difference in accessibility to medical care in Taiwan31). Previous studies indicated that medical personnel with
different types of affiliations might experience different job demand and work load, and then might have different adverse health risks20).
confounding by affiliation. The analyses were performed with SAS v9.1.3 (SAS Institute, Cary, NC, USA), and the level of significance was set an -value of 0.05.
Results
The mean age (40.1±8.2 years) of dentists was older than that of other health personnel (38.0±8.8 years), but was similar to the mean age of physicians (40.5±8.8 years). Male dominance of the study sample was observed in the three study groups, with the greatest women to men ratio noted for physicians (89.0/11.0), followed by dentists
(83.2/16.8) and other health personnel (55.3/44.8). Physicians and other health personnel had the highest and lowest mean insurance premium, respectively, and dentists were in between. There were apparent
geographic distributions in practice for the three study group. More than a half of dentists (41.7%) practiced in Taipei city, capital of Taiwan, while the corresponding figures for other health personnel and physicians were somewhat lower at 28.8% and 37.3%, respectively. Compared with the other two groups, dentists were less likely to be employed at medical centers or hospitals. More than 80% of dentists worked at clinics. (Table 1)
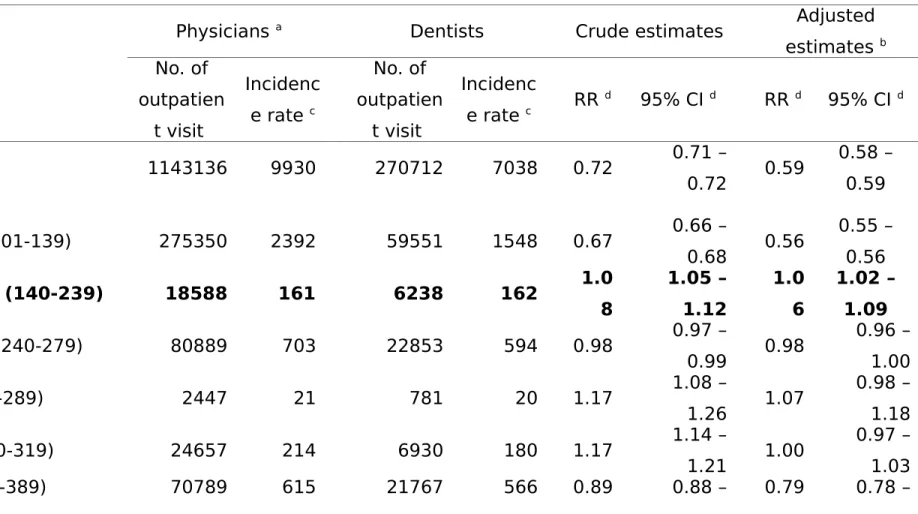
During the 5-year follow-up period, the incidence rate of outpatient visit for various causes was the lowest for the dentists (7,038 per 103 person-years), followed by the physicians (9,930 per 103 person-years), and other health personnel (9,981 per 103 person-years). The later two groups were very similar in rate of outpatient visit (Table 2). Table 2 also
compares the rates of all-cause and cause-specific rates of outpatient visit between dentists and physicians, and shows that dentists
experienced a significantly reduced ARR of not only all-cause outpatient visit (ARR=0.59, 95% CI 0.58, 0.59), but also visits for illnesses related to infection (ARR=0.56), nerve ( ARR= 0.79), circulation (ARR=0.85), respiratory tract (ARR=0.49), digestive system (ARR=0.52),
genitourinary system (ARR=0.89), skin (ARR=0.86), musculosketal system (ARR=0.62), and injury (ARR=0.69). On the other hand, dentists had a modestly but significantly higher rate of outpatient visit for
neoplasm (ARR=1.06, 95% CI 1.02, 1.09).
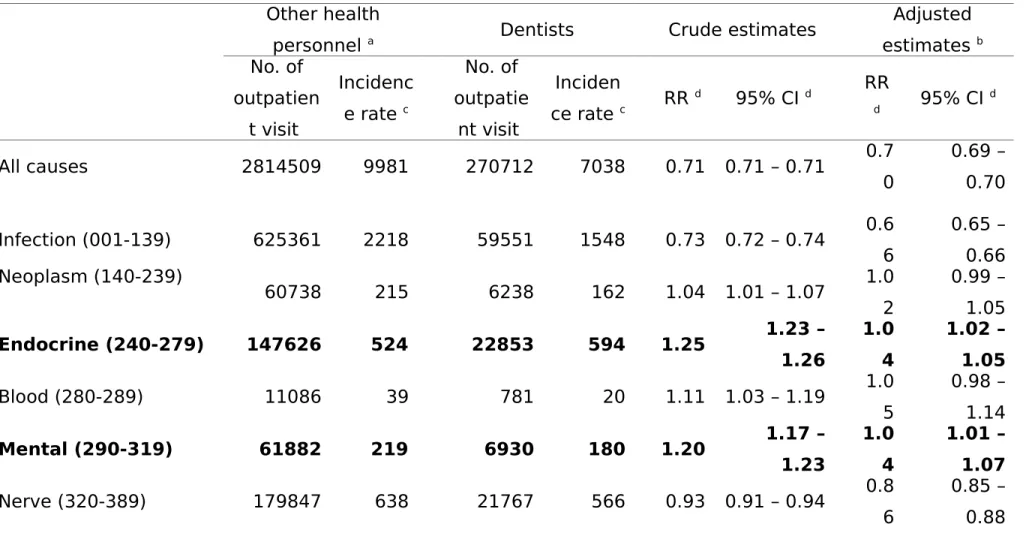
Table 3 shows significantly reduced ARRs for all-cause outpatient visit (0.70, 95% CI 0.69, 0.70) and for various causes including infection (ARR=0.66), nerve disease (ARR=0.86), circulatory illness (ARR=0.90), respiratory illness (ARR=0.61), digestive illness (ARR=0.62),
genitourinary disorder (ARR=0.85), skin disease (ARR=0.79), musculosketal disorder (ARR=0.65) and injury (ARR=0.72) among dentists, as compared to other health personnel. On the other hand, dentists were noted to experience slightly, but significantly, increased ARRs for endocrine/metabolic/immunity (ARR=1.04, 95% CI 1.02, 1.05) and mental (ARR=1.04, 95% CI 1.01, 1.07) disorders.
Discussion
This study is believed to be the first health report with all dentists who have a contract with a nationwide NHI program in Taiwan. Taiwan’s dentists had an annual average of 7.04 outpatient visits per person between 2003 and 2007, which was much lower than the figures for physicians (9.93 visits) and for other health personnel (9.98 visits). Also with NHI claims, Chen et al. reported that Taiwanese people had an average of 13.4 outpatient visits per person in 200632), indicating that dentists in Taiwan had a very low utilization rate of outpatient visit. Respiratory diseases were the most prevalent cause of outpatient visit for dentists. Other common causes included infection,
endocrine/metabolic/immunity disorders, and nervous disease. Despite a lower incidence of all-cause outpatient visits, the dentists did suffer more frequently than control groups from neoplasm,
endocrine/metabolic/immunity disease, and mental illness.
The dentists in Taiwan suffered less frequently than physicians from overall and many cause-specific outpatient visits, except neoplasm. Additionally, dentists were also at obviously lesser risks of outpatient visit for all causes and most specific causes, as compared to other health personnel, but were at greater risks of mental disorders and
noted in dentists was unlikely to be entirely attributed by dentists’ reluctance to seek appropriate health cares or by their self-treating behaviors, since we included physicians and other health personnel as control groups, who also tend to be reluctant to adopt the role of a
patient and concern about confidentiality, which could also impede their access to appropriate health cares and lead to their self-treating33). Our findings may have reflected that dentists are more likely than their
medical colleagues to exercise healthy behaviors. It could also be due to lesser exposure to occupational hazards involved in dentists’ duties. Although dentists had an obvious reduced rate of overall outpatient visit, they suffered from frequent visits for neoplasm, mental disorders, and endocrine/metabolic/immunity diseases by a magnitude of 4%-6%, which however should not be overlooked.
Rix and Lynge34) performed a 17-year cohort analysis of the Danish Occupational Mortality Register, noting that the overall cancer incidence was elevated in dental practitioners. Male dental practitioners also had significantly higher risks of melanomas of the skin. The breast cancer risk was elevated among female salaried dentists as well. A Japanese study reported that with the general Tokyo residents as a reference population, the standardized mortality ratios for dentists were
significantly higher for esophageal and colon cancers35). In addition, several studies also reported an increased risk for skin cancer, especially
melanoma, in dentists2, 36, 37). In a recent meta-analysis, Simning and Wijngaarden reported an estimated relative risk of 2.4 (95% CI 1.6, 3.7) for melanoma in male dentists, and to a lesser magnitude for female dentists (relative risk=2.0, 95% CI 1.1, 3.9) 14). Although some of the previous reports argued that the elevated risks experienced by dentists may be related to social status level2, 36, 37) or lifestyle (e.g., behavior related to sunlight exposure)22), the review by Simning and
Wijngaarden14) still suggested that certain hazards in the workplace may account for such findings. Our study employed physicians and other health personnel as reference groups, whose social status level and lifestyle are similar to dentists, which may have largely, even not
entirely, excluded the potential confounding posed by social status level and lifestyle.
The review by Alaujan and Alzahem38) indicated that dentists are faced every day with many stressors; as a result, they are subject to many symptoms of stress that must be identified and managed in the early stages before serious physical and psychological consequences develop. A recent survey of British dentists revealed that the most common factors contributing to stress at work were patient demands (75%), practice management/staff issues (56%), fear of
complaints/litigation (54%) and non-clinical paperwork (54%)39). A national survey of dentists registered with the Lithuanian Dental
Association indicated that fatigue (94.7%) and back pain (91.0%) were the most prevalent physical complaints reported40). Of the 256 Mexican dentists, chronic high stress levels were found in 35 (13.7%) of the dentists, medium level stress in 184 (71.8%), and a low level of chronic stress in 37 (14.5%)15). In a prospective study, Ahola and Hakanen16) investigated whether burnout may mediate the association between job strain and depressive symptoms in a national sample of Finnish dentists. The results showed that there was a reciprocal relationship between burnout and depressive symptoms, and job strain predisposed to depression through burnout. In comparison, job strain predisposes to burnout directly and via depression. Given a relatively high work load in Taiwan’s dentist population, the above findings from various previous studies might explain, at least to some extent, the slightly higher prevalence of outpatient visit for mental illnesses in Taiwan’s dentists.
In addition to mental illnesses, dentists were also noted to
experience a slightly increased risk of endocrine/metabolic/immunity disorders, which are probably the most highly lifestyle-related symptoms investigated in this study. A recent British survey showed that more than half (53%) of dentists were relatively inactive during the day but 57% took some form of physical exercise at least 3-4 times per week. Nearly a half (49%) of respondents felt that their level of physical activity was probably inadequate, and was very likely or somewhat likely to cause
them health problems37). A local study conducted in Taiwan on a sample of hospital employees reported that although the prevalence of
metabolic syndrome may be lower in hospital employees than in the general population, the prevalence of metabolic syndrome can still be as high as 10.3% (21.8% males, 7.0% females) among hospital employees, and suggested more efficient health-promotion programs administered to hospital employees to further reduce the metabolic syndrome41). Due to lack of information regarding the work shift and work-related lifestyles of dentists and other health personnel in Taiwan, we were unable to make more specific interpretations of our findings.
Most of the published studies suggesting lower risks of mortality or morbidity among dentists than in the general population are subject to methodological limitations owing to a higher socioeconomic status and healthier lifestyle of dentists. Our current study employed physicians and other health personnel as reference controls may have largely removed such confounding, and balanced the potential problems of self-treating commonly seen in health care workers. Moreover, we further adjusted a number of factors in the multivariate regression model, including age, sex, type of affiliation, and several socio-demographic factors to remove potential confounding. As such, our findings may have better reflected the hazards more directly related to dental work.
work-related lifestyles, and possible occupation related hazards for dentists, we were unable to make specific interpretations regarding what factors that truly caused increased outpatient visit for certain disease among dentists in Taiwan. Additionally, we didn’t have complete information on a study subject’s history of employment, which also limited the causal inference between dental profession and incidence of outpatient visit.
There is a potential for disease misclassification in claim data. Although the BNHI performed regular check-up for the accuracy of reimbursement, the codes of disease diagnoses in the NHI claims have not been systematically examined. However, the potential disease misclassification is likely to proportionally apply in the three study groups, resulting in a non-differential type of disease misclassification, which will bias, if any, the study findings toward the null, and should not be a valid argument for the increased ARR observed in this study. In conclusion, with such a large dentist cohort and multiple control groups, we noted that the dentists in Taiwan were indeed at greater rates of endocrine/metabolic/immunity disease, mental illness, and neoplasm, which needs more investigations. Future studies of dentists’ health would also benefit from the assessment of specific occupational exposures rather than relying on job title alone. Besides, whether the findings found in this study were specific to Taiwanese dentists or can be
applicable to dentists of other nations also deserved further
investigations. Policy makers and hospital administrators must not overlook dentists’ potentially unseen health problems. A mandatory periodical physical examination for dentists can seriously be considered.
Acknowledgements
This study was supported by grants from National Scientific Council (NSC98-2314-B-227-001-MY2). The interpretation and conclusions contained herein do not represent those of BNHI, Department of Health or NHRI.
References
1) Zwemer JD, Williams JE (1987) Dentist health status and risks. J AM Coll Dent 54, 7-12.
2) Andersen A, Barlow L, Engeland A, Kjærheim K, Lynge E, Pukkala E (1999) Work-related cancer in the Nordic Countries. Scand J Work Environ Health 25 suppl 2,1-116.
3) Smning A, Wijngaarden E (2007) Literature review of cancer
mortality and incidence among dentists. Occup Environ Med 64:432-8.
4) Leggat PA, Smith DR (2006) Musculoskeletal disorders self-reported by dentists in Queensland, Australia. Aust Dent J 51,324-7.
5) Kierklo A, Kobus A, Jaworska M, Botuliński B (2011) Work-related musculoskeletal disorders among dentists - a questionnaire survey. Ann Agric Environ Med 18, 79-84.
6) Ding H, Solovieva S, Vehmas T, Takala EP, Leino-Arjas P (2010) Hand osteoarthritis and pinch grip strength among middle-aged female dentists and teachers. Scand J Rheumatol 39, 84-7.
7) Kurpiewska J, Liwkowicz J, Benczek K, Padlewska K (2011) A survey of work-related skin diseases in different occupations in Poland. Int J Occup Saf Ergon 17, 207-14.
8) Palacios-Rodríguez RG, Paulín-Villalpando P, López-Carmona JM, Valerio-Acosta Mdel M, Cabrera-Gaytán DA (2010) Metabolic syndrome in health care personnel from a primary care unit. Rev Med Inst Mex Seguro Soc 48, 297-302. Spanish.
9) Neguţ EA, Bălteanu M, Ionescu G, Băncescu A, Iliescu A, Skaug N (2007) Control of blood-transmitted infections in dentistry. Roum Arch Microbiol Immunol 66, 26-36.
HCV infection in Japanese dental care workers. Int J Mol Med 21, 791-9.
11) Azodo CC, Ehigiator O, Ojo MA (2010) Occupational risks and hepatitis B vaccination status of dental auxiliaries in Nigeria. Med Princ Pract 19, 364-6.
12) Loster BW, Czesnikiewicz-Guzik M, Bielanski W, Karczewska E, Loster JE, Kalukin J, Guzik TJ, Majewski S, Konturek SJ (2009) Prevalence and characterization of Helicobacter pylori (H. pylori) infection and
colonization in dentists. J Physiol Pharmacol 60, 13-8.
13) Tanaka H, Nishio N, Tokunaga R, Tsukuma H (2004) Liver cancer risk in Japanese male dentists: a long-term retrospective cohort study. J Occup Health 46, 398-402.
14) Simning A, van Wijngaarden E (2007) Literature review of cancer mortality and incidence among dentists. Occup Environ Med 64, 432-8.
15) Pozos Radillo BE, Tórrez López TM, Aguilera Velasco Mde L, Acosta Fernández M, González Perez GJ (2008) Stress-associated factors in Mexican dentists. Braz Oral Res 22, 223-8.
16) Ahola K, Hakanen J (2007) Job strain, burnout, and depressive
symptoms: a prospective study among dentists. J Affect Disord 104, 103-10.
17) Lindbohm ML, Ylöstalo P, Sallmén M, Henriks-Eckerman ML,
Nurminen T, Forss H, Taskinen H (2007) Occupational exposure in dentistry and miscarriage. Occup Environ Med 64, 127-33.
18) Department of Health, Division of Health Statistics (2005) Trend of health statistics in Taiwan. Department of Health, Executive Yuan, Taiwan.
19) Department of Health. Annual report of medical statistics. http://www.doh.gov.tw/CHT2006/DM/DM2_2_p02.aspx?
Accessed January 16, 2012.
20) Lin YW, Chang YW, Tsai CC (2004) Job strain and health-related quality of life of hospital employees: case of a medical canter in Taichung. Taiwan J Public Health 23, 108-20.
21) World Health Organization (2009) Health workforce, infrastructure, essential medicines. 95-105, WHO Press, Switzerland.
22) Listl S, Moran V, Maurer J, Faggion CM Jr (2012) Dental service utilization by Europeans aged 50 plus. Community Dent Orl Epidemiol 40, 164-74.
23) Karasek RA, Theorell T (1990) Health work stress, productivity and the reconstruction of working life. Basic Books, New York.
24) Lin CM, Yang CH, Sung FC, Li CY (2008) Risks of hospitalization among physicians in Taiwan. Health Serv Res 43, 675-92.
25) Huang IC, Yang CH, Sung FC, Chen HF, Li CY (2009) Risks of
ambulatory cares among female nursing staffs in Taiwan. J Clin Nurs 18, 1207-16.
26) Liu SH, Li TH, Lin YL, Shiao YJ, Wu SC, Li CY, Sung FC, Yang CY, Wu TN (2009) Morbidity and disease risk among the Chinese medicine physicians in Taiwan. Tohoku J Exp Med 219, 207-14.
27) Department of Health, Division of Health Statistics (2003) Trend of health statistics in Taiwan. Department of Health, Executive Yuan, Taiwan.
28) Bureau of National Health Insurance. NHI Statistics.
http://www.nhi.gov.tw/information/bulletin_file/421_0890036465-19.doc, Accessed October 1, 2010.
29) Directorate-General of Budget (1993) National statistics of regional standard classification data. Taipei, Taiwan. Directorate-General Budget, Accounting and Statistics, Executive Yuan.
30) Holford TR (1983) The estimation of age, period and cohort effects
31) Tan HF, Tseng HF, Chang CK, Lin W, Hsiao SH (2005) Accessibility assessment of the health care improvement program in rural Taiwan. J Rural Health 21, 372-7.
32) Chen TJ, Chou LF, Hwang SJ (2006) Patterns of ambulatory care
utilization in Taiwan. BMC Health Serv Res 6, 54-61.
33) Thompson WT, Cupples ME, Sibbett CH, Skan DI, Bradley T (2001) Challenge of culture, conscience, and contract to general
practitioners’ care of their own health: qualitative study. Br Med J 323, 728-31.
34) Rix BA, Lynge E (1996) Cancer incidence in Danish health care workers. Scand J Soc Med 24, 114-20.
35) Shimpo H, Yokoyama E, Tsurumaki K (1998) Causes of death and life expectancies among dentists. Int Dent J 48, 563-70.
36) Firth HM, Cooke KR, Herbison GP (1996) Male cancer incidence by occupation: New Zealand, 1972-1984. Int J Epidemiol 25,14-20. 37) Eriksson M, Hardell L, Malker H, Weiner J (1998) Increased cancer
incidence in physicians, dentists, and health care workers. Oncol Rep 5, 1413-8.
38) Alaujan AH, Alzahem AM (2004) Stress among dentists. Gen Dent 52, 428-32.
39) Kay EJ, Lowe JC (2005) A survey of stress levels, self-perceived health and health-related behaviours of UK dental practitioners in 2005. Br Dent J 204, E19-E28.
40) Puriene A, Aleksejuniene J, Petrauskiene J, Balciuniene I, Janulyte V (2008) Self-reported occupational health issues among Lithuanian dentists. Ind Health 46, 369-74.
41) Ho HH, Tsai TY, Lin CL, Wu SY, Li CY (2011) Prevalence and
associated factors for metabolic syndrome in Taiwanese hospital employees. Asia Pac J Public Health 23, 307-14.
Table 1. Characteristics of the study subjects.
Dentists Physicians Other health personnel a No. of study subjects 7760 23211 56788 Person-years observed 38463.8 115117.9 281997.5 n % n % n % Age (year) <=29 718 9.3 10796 19.0 2180 9.4 30-39 3269 42.1 23840 42.0 9647 41.6 40-49 2732 35.2 15664 27.6 7553 32.5 50-59 917 11.8 5473 9.6 3130 13.5 >=60 124 1.6 1015 1.8 701 3.0 SD x 40.1±8.2 40.5±8.8 38.0±8.8 Gender Men 6455 83.2 31364 55.3 20665 89.0 Women 1305 16.8 25403 44.8 2541 11.0 Insurance premium (NTD b) <40,100 1162 15.0 17194 30.3 1733 7.5 40,100-< 55,400 1397 18.0 17278 30.4 4672 20.1 55,400-< 87,600 2722 35.1 9955 17.5 5932 25.6 ≧87,600 2479 32.0 12361 21.8 10874 46.9 SD x 60845.0±23679. 5 67730.2±22240. 3 50909.0±24541. 5 Place of practice Taipei 3232 41.7 16368 28.8 8658 37.3 North 871 11.2 8384 14.8 3126 13.5 Central 1555 20.0 11260 19.8 4170 18.0 South 804 10.4 10589 18.7 2874 12.4 Kao-Pin 1168 15.1 8460 14.9 3744 16.1 East 130 1.7 1727 3.0 639 2.8
Type of affiliation Medical center 709 9.1 12360 21.8 7772 33.5 Regional hospital 497 6.4 10698 18.8 5333 23.0 Local hospital 284 3.7 11374 20.0 3572 15.4 Clinics 6270 80.8 22356 39.4 6534 28.2 Urbanization Metropolitans 4634 59.7 30231 53.2 13974 60.2 Satellite cities 2002 25.8 13777 24.3 5256 22.6 Rural areas 1124 14.5 12780 22.5 3981 17.2 a Including physicians of Chinese medicine, pharmacists, nurses,
medical laboratory technicians, radiological technologists, speech-language therapists, physical and occupational therapists, and dieticians.
b NTD=New Taiwan Dollars, 32 NTD 1 USD; insurance premium was determined according to individual's monthly income.
Table 2. Comparisons of rates of all-cause and cause-specific outpatient visit between dentists and physicians, 2003-2007.
Physicians a Dentists Crude estimates Adjusted estimates b No. of outpatien t visit Incidenc e rate c No. of outpatien t visit Incidenc e rate c RR d 95% CI d RR d 95% CI d All causes 1143136 9930 270712 7038 0.72 0.71 – 0.72 0.59 0.58 – 0.59 Infection (001-139) 275350 2392 59551 1548 0.67 0.66 – 0.68 0.56 0.55 – 0.56 Neoplasm (140-239) 18588 161 6238 162 1.0 8 1.05 – 1.12 1.0 6 1.02 – 1.09 Endocrine (240-279) 80889 703 22853 594 0.98 0.97 – 0.99 0.98 0.96 – 1.00 Blood (280-289) 2447 21 781 20 1.17 1.08 – 1.26 1.07 0.98 – 1.18 Mental (290-319) 24657 214 6930 180 1.17 1.14 – 1.21 1.00 0.97 – 1.03 Nerve (320-389) 70789 615 21767 566 0.89 0.88 – 0.79 0.78 –
0.91 0.81 Circulation (390-459) 66006 573 15835 412 0.89 0.87 – 0.90 0.85 0.83 – 0.86 Respiratory (460-519) 300849 2613 64377 1674 0.66 0.65 – 0.66 0.49 0.49 – 0.50 Digestive (520-579) 85036 739 16772 436 0.66 0.65 – 0.68 0.52 0.51 – 0.53 Genitourinary (580-629) 25255 219 9784 254 1.00 0.98 – 1.03 0.89 0.87 – 0.92 Pregnancy (630-676) 2468 21 1090 28 0.99 0.92 – 1.06 0.91 0.84 – 1.00 Skin (680-709) 51761 450 13229 344 0.81 0.80 – 0.83 0.68 0.67 – 0.70 Musculoskeletal (710-739) 63241 549 13445 350 0.70 0.68 – 0.71 0.62 0.61 – 0.63 Injury (E800-999) 29020 252 6914 180 0.77 0.75 – 0.79 0.69 0.67 – 0.71 a Reference group.
b Adjustment for age, sex, insurance premium, place of practice, type of affiliation, and urbanization.
Table 3. Comparisons of rates of all-cause and cause-specific outpatient visit between dentists and other health personnel, 2003-2007.
Other health
personnel a Dentists Crude estimates
Adjusted estimates b No. of outpatien t visit Incidenc e rate c No. of outpatie nt visit Inciden ce rate c RR d 95% CI d RR d 95% CI d All causes 2814509 9981 270712 7038 0.71 0.71 – 0.71 0.7 0 0.69 – 0.70 Infection (001-139) 625361 2218 59551 1548 0.73 0.72 – 0.74 0.6 6 0.65 – 0.66 Neoplasm (140-239) 60738 215 6238 162 1.04 1.01 – 1.07 1.0 2 0.99 – 1.05 Endocrine (240-279) 147626 524 22853 594 1.25 1.23 – 1.26 1.0 4 1.02 – 1.05 Blood (280-289) 11086 39 781 20 1.11 1.03 – 1.19 1.0 5 0.98 – 1.14 Mental (290-319) 61882 219 6930 180 1.20 1.17 – 1.23 1.0 4 1.01 – 1.07 Nerve (320-389) 179847 638 21767 566 0.93 0.91 – 0.94 0.8 0.85 –
Circulation (390-459) 114411 406 15835 412 1.10 1.08 – 1.11 0.9 0 0.89 – 0.92 Respiratory (460-519) 689280 2444 64377 1674 0.71 0.71 – 0.72 0.6 1 0.60 – 0.61 Digestive (520-579) 184625 655 16772 436 0.78 0.77 – 0.79 0.6 2 0.61 – 0.63 Genitourinary (580-629) 163935 581 9784 254 0.73 0.71 – 0.74 0.8 5 0.83 – 0.87 Pregnancy (630-676) 23799 84 1090 28 1.01 0.95 – 1.07 1.0 6 1.00 – 1.13 Skin (680-709) 148034 525 13229 344 0.81 0.80 – 0.83 0.7 9 0.77 – 0.80 Musculoskeletal (710-739) 157396 558 13445 350 0.76 0.75 – 0.78 0.6 5 0.64 – 0.66 Injury (E800-999) 77977 277 6914 180 0.81 0.79 – 0.83 0.7 2 0.70 – 0.74 a Reference group.
b Adjustment for age, sex, insurance premium, place of practice, type of affiliation, and urbanization.
c Per 1,000 person-years.