【附錄4】
Developing a Measuring Scale for Students’ Mobile Learning
of Health Technology Literacy in Technological Colleges
CHIN-MOU CHENG
College of Humanities and Management,
Fooyin University
151, Chinhsueh Rd., Ta-liao, Kaohsiung,
TAIWAN
so003@mail.fy.edu.tw, littlecheng@gmail.com
Abstract: -
This study intended to develop a scale to examine the current situation of students’ literacy abouthealth technology, testing a model for students’ health in technological colleges to construct the contents of health technology literacy by using several theories. To achieve this goal, the following methods were applied: literature review, Delphi survey, professional interview and sampling questionnaire survey. Through the structure equation modeling (SEM) with two-order confirmatory factor analysis, validity and reliability analysis, the model was tested with good fit, and the contents were certainly a second-order factor of health technology literacy, including first-order factors, that is, cognition, innovation propensity, health belief and knowledge sharing. And then, by using a survey method with cluster and stratified random sampling from 16 technological colleges in Taiwan, 3,600 questionnaires were sent out, and 3,012 effective questionnaires were returned; the survey reached 83.67% of return-ratio. The results indicated that the students’ literacy content of health technology consisted of cognition, innovation propensity, belief and knowledge sharing, according to the theories of planning behavior, social cognition, innovative diffusion, technology acceptance and health belief. The model of students’ literacy contents of health technology was tested with good fit via the structural equation modeling (SEM), and it revealed, via SEM test, that a scale could be developed with high validity and reliability to examine the current situation of students’ literacy about health technology. Finally, conclusions and suggestions were advanced as references for the curriculum teaching and research in universities and industries in order to benefit the teachers and practitioners in mobile learning.
Key Words: health technology, validity and reliability, technological colleges, knowledge sharing, theory of planning behavior
1 Introduction
Technology and health are important issues in the 21st century of knowledge economy. Nowadays, the students receiving high level education in modern technological surroundings seem to rely on and utilize technology more than those of the previous age. However, in the technological surroundings, college students of the present age should take into consideration how technology makes an impact on their health [29]. Technology is like a two-edged sword. On the one hand, it can improve health, prolong life expectancy, elevate life quality, and help with the transfer of knowledge and technique. Nevertheless, on the other hand, overuse or misuse of technology will more often than not lead to technology addiction. For example, in the Internet or mobile learning addiction of adolescents or students; pathological or problematic Internet use [6] [9]. In
exercise, smoking, alcohol drinking, illegal drug use, psychological health problems, and bad habits of inadequate eating and drinking [13]. College students, in virtual reality of technology, have been physically and psychologically affected by their interaction with computers [4]. Lacking health technology literacy as well as a good understanding of the dual effect of technology on health, the college students of today have insistently pursued innovative products of technology without noticing their negative influences on body and mind.
In order to survive the inter-school competition, the colleges have made every effort to develop their own features to cultivate the students’ innovative capability in mobile learning with the hope that the students can attain holistic health, and the schools can be continuously run. Then mobile learning is the exciting art of using mobile technologies to enhance the learning experiences. In the century of innovation
362 capability. However, those who engage in the study of competitive health technology literacy are few. In addition, in spite of the diversity of the studies on health belief, research for health technology literacy is still pioneering. In this way, the health technology literacy of students can be improved, and then a milestone of education can be created. In viewing the social issues happening on college campus in recent years, it is found that the number of depression cases and self-harming cases has been rising. Judging from this, the study of their health technology literacy seems to emerge as an urgent necessity.
In addition, health technology literacy serves as a basic cognition of health technology which the college students should be equipped with. And it is also a supposedly accepted belief during their educational process. Furthermore, an inadequate use of the Internet technology tends to lead to addiction. And they would not brace themselves for the difficulties confronted in academic learning, which would make them tired of their regular academic learning [31]. And it should be noted that this would make a negative impact on their physical and psychological health. In recent twenty years, bountiful are the academic papers on health technology interpreted by the behavior theories of social psychology such as planning behavior, social cognition, diffusion of innovation, technology acceptance, and health belief. This study is expected to employ these theories to build up a scale to assess the health technology literacy of students.
This study focuses on the study of the contents of health technology literacy. Furthermore, the model of health technology literacy will be constructed, and the measuring scale of health technology literacy will be well developed in order to get a good grasp of the current state of students’ health technology literacy.
2 Literature review
2.1 Related studies on health technology
literacy
The adoption of innovative technology can make a positive impact on health care [10]. Health technology has the function of medical treatment and health preservation; it is the technology that can enhance man’s health and prevent illnesses. Technological literacy is defined as man’s capability of using, managing, understanding, and evaluating technology (see http://www.iteaconnect.org/). And technology literacy refers to practical affairs focusing on technology and literacy in courses; it is practical affairs uniting technological information and literacy [14]. The literacy is actually related to computers, humanism, and social sciences. The medical and
nursing staff serving in the field of health care, for example, need information literacy and computer technology in order to effectively engage in education research [8], and thus their computer knowledge and skills in the health care profession can be improved [27]. It is the basic capability and literacy of health care for professionals to effectively use information technology in mobile learning. Even the health technology literacy is the basic cognition capability needed for college students, as well.
Health technology is related to innovation, and the innovative style develops new software beneficial to health [10]. Moreover, the provision of health care can improve technology innovation, enhancing health status. The related health technology studies aim to provide students with a correct cognition of health technology, so it’s vitally important to evaluate the learners’ level of meta-cognition [32]. The nutrition classes based on the Internet can supply college students with nutrition information, helping them to show healthy behaviors in taking meals.
The literacy of computer multi-media helps students to learn knowledge management [18]. By using health information, nursing students can search for evidence in sharing health knowledge [5]. With the assistance of multi-media information of offering caring systems, we can understand the meaning of health technology knowledge transfer or sharing.
It’s vitally important for youngsters to seek normative health beliefs of body caring, especially when they lose health for smoking or depression [22], or drinking alcohol [25]. Moreover, the health beliefs of college students are associated with spiritual involvement and personality dimensions [21].
According to the aforesaid comments on the related studies, it seems that health technology literacy, to some extent, covered innovation, cognition, knowledge transfer, and belief.
2.2 Prominent models used to explain the
related health technology usage
Some prominent models that can be used to explain the related health technology usage, such as theory of planned behavior (TPB), technology acceptance model (TAM), diffusion of Innovation theory (DIT), social cognitive theory (SCT), and health belief model (HBM) [17] which are main references for a discussion of the contents of the health technology literacy.
The factors that directly or indirectly influence knowledge sharing are subjective norm, attitude intention, and perceived behavioral control [26]. TPB has made a study of relations among belief, attitude, intention, behavior, perceived behavior control, control propensity, and TPB [1]. TPB has been
widely applied to medical behavior, life-long learning, sports health, and information system.
SCT holds that an individual can learn others’ behavior via observation and imitation [23]. If we use SCT to explain giving up smoking, it can be found that this behavior is accompanied by the change of cognition determining factors, such as attitude, social influence, self-efficacy, and preferred health state.
According to TAM, belief can influence attitude, which can influence behavioral intention, which in turn has a positive impact on practical usage. This model is widely used to explain or predict the influencing factors of information technology usage. When using technology, perception of the easiness in using new technology will influence its utility [28].
The related DIT influencing factors include innovation, organization, mission, individuals, and surrounding features.
Health belief is mainly composed of perceived susceptibility, perceived severity, perceived benefits, and perceived barriers. HBM can revise the structure of teaching in order to improve health behaviors like giving up smoking [15]. It can also be applied to the study of SARS [30], and to develop a more suitable model to examine the acceptability of health careers under the condition of the mobile learning [33].
2.3 Related factors of the contents of
health technology literacy and interrelation
According to some studies, students’ perception of the use of computer technology is helpful for their learning experiences and professional career [19]. The innovative multi-media system of health technology can be applied to schools’ learning environments in order to improve health. In addition, the technology of information and broadcasting can easily be applied to social environments to create fresh life-long learning model, to stimulate students’ high level thinking in producing innovation [2]. According to some experiments and studies, students can use computers to relax themselves and soothe their own uncomfortable feelings [7].
The health caring industry gradually becomes a knowledge-based social entity connected with medical units and consumers in order to share knowledge [3]. It researches knowledge sharing in virtual communities from an e-business perspective [16]. In terms of subjective norm, an individual’s behavior is affected not only by his motivation but by his accessible groups and the important persons in his or her eyes. A physician’s subjective norm affects his knowledge sharing [26]. By using innovating diffusion, and planned behavior theory, we can figure
Cognition, innovation propensity and medical innovation technology are positive factors for long life, and psychological health [20]. Concerning beliefs and knowledge sharing, if perceiving the seriousness of illness infection, we can prevent the illness, thus benefiting our health. Health knowledge, via knowledge creation, acquirement, and discussion, is passed to others for sharing and mutual construction [11]. As a whole, caring knowledge and practical affairs should be connected. Based on this, theories and knowledge can be transferred to clinical affairs [12]. HBM can serve to reduce the threat and to remove execution barriers in order to interpret, and predict the mechanism of how people adopt preventive health behaviors.
3 Method
3.1 Sampling survey
In sampling investigation, cluster and stratified random sampling is adopted, and 16 schools are sampled from 78 technological colleges in the 2007 academic year throughout Taiwan. We intend to have a comprehensive understanding of college students’ cognition of health technology literacy contents. Totally speaking, 3,600 questionnaires were sent out, and 3,012 effective questionnaires were returned; the survey reached as high as 83.67% of return-ratio. After that, these data were input into computers for statistic analyses. Of all these effective measuring scales, in terms of gender, males accounted for 1320 (43.8%), while females, 1692(56.2%). And in terms of school systems, four-year tech accounted for 1754(58.2%); two-year tech, 342(11.4%); five-year junior colleges, 631(20.9%); extension education departments, 285(9.4%).
3.2 Measurement tool
It took one year to develop and design the research tools. First, the interview outline was written out by surveying relevant literature. And then, after interviewing ten experts, we completed a draft measuring scale of health technology literacy of college students. To standardize the process of designing the measuring scale, the pre-test measuring scale was validated by the experts from the perspectives of effectiveness, item analysis, reliability analysis and factor analysis. Furthermore, the 127 items of the pre-test were shortened into 106 ones by 16 experts, scholars, physicians respectively belonging to the fields of technological education, medical and nursing care, and educational psychology, and were transformed into a formal measuring scale. From Feb. 22, 2006 to May, 20, the
364 The formal measuring scale was completed, and 106 items, 115 items, and 98 items respectively in the previous questionnaires were changed, through revision, into 94 items, and then finally 92 items. The scale can be divided into four areas: 28 items in health technology cognition; 31 items in innovation propensity of health technology; 15 items in health technology belief; and 18 items in knowledge sharing of health technology. To keep most students from expressing neutral opinions and to balance the positive opinions and negative ones, the measuring scale used the Likert 6-point measuring rule.
4 Results
4.1 Factor analysis
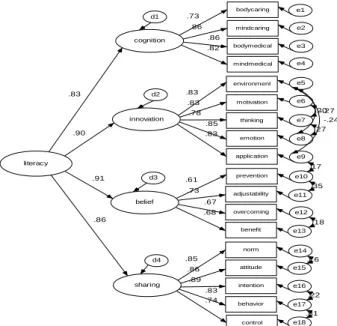
Principal components factor analysis with factor extraction and maximum likelihood rotation can discriminate effectiveness, and may be determined. Minimum eigen value is 1; the minimum factor burden amount of each index item is 0.4; simplifying the factor structure; excluding factors of the single items. Those whose structure α shortcut figure is higher than 0.7 are chosen for use. And all question items whose related scores in the whole measuring scale are lower than 0.4 are excluded. This can support the discrimination effectiveness of the measuring scale. The factor analysis uniting all layers is engaged in, and all items are included in order to develop the research structure. We employed the confirmatory factor analysis to evaluate the validity and reliability of the measuring scale. The route model of testing validity was shown in Figure 1.
literacy cognition innovation belief sharing bodymedical mindmedical environment motivation thinking emotion application prevention mindcaring bodycaring adjustability overcoming benefit norm attitude intention behavior control .91 .90 .83 .86 .86 .89 .73 .86 .86 .82 .83 .78 .85 .83 .83 .68 .67 .73 .61 .85 .83 .74 e1 e2 e3 e4 e5 e6 e7 e8 e9 e10 e11 e12 e13 e14 e15 e16 e17 e18 d1 d2 d3 d4 .31 .16 .35 .18 .27 .17 -.27 .20 .22 -.24
Figure 1 Two-order confirmatory factor analyses According to Figure 1, this study presupposed that the contents of the health technology literacy (second-order factor) of colleges are composed of
cognition, innovation propensity, belief, and knowledge sharing (first-order factor). And cognition included four sub-dimensions (observation variables) -technological body health care, mind health care, body medical treatment, and mind medical treatment. Innovation propensity included five sub-dimensions (observation variables) -innovative surroundings, innovation motivation, innovative thinking, and innovation application. Belief was inclusive of perception prevention, perception adjustability, perception overcoming, and perception effectiveness. And knowledge sharing included five sub- dimensions (observation variables) -behavior norm, sharing attitude, sharing intention, sharing behavior, perception behavior control.
The margin variance of which standard variables are positive ranges from 0.19 to 0.90, both of which fall below 0.95, which shows that the standard margin is not so significant. As a result, this is not against estimation norms so that the fitness of the model can be tested. In terms of individual variants of the model, by observing the standardized loadings amount which observatory variables reflect on factors, it can be found that all of the standardized coefficients reach a rather high level. This shows that the hypotheses of the model are rather consistent with the observed data. Thus the four variables of the first- order factors can account for eighteen observatory variables, while the second-order health technology literacy can explain four first-order factors.
Concerning the test of the validity of the model, as a whole, in terms of statistics, it is found that owing to the too big size of the sample (3012), the Chi-square coefficient is 15.435 > 3. After the revision of the model, Chi-square turns out to be 1.447< 3, p=.004>.001, which shows that there is no significant difference between hypothesis models and observatory variables, and that, the model is acceptable. RMSEA is 0.012, showing that the fitness is fine. And P figure test is <0.05; ECVI= 0.097, smaller than ECVI of the independence model. GFI=0.995, bigger than the acknowledgement value 0.90; AGFI=0.991, also bigger than 0.90, showing that this can be acceptable to the model. NFI = 0.997,NNFI=0.998, CFI=0.999, IFI=0.999, RFI =0.995; all of these figures are higher than 0.90, showing that the model fits. In addition, PNFI= 0.573, bigger than the acknowledgement value 0.5; PGFI = 0.512, bigger than the acknowledgement value, 0.5. AIC = 293.332, smaller than the AIC figure of the independent model. And RMR = 0.108, while Standardized RMR = 0.039<0.05, showing that based on the smallness of deviation, the fitness is
fine. According the above statistics, since absolute fitness, incremental fitness, parsimony fitness all reach an acceptable standard, we can see that the construction validity of the measuring scale, through two order factor examinations, can pass the test about statistics. Meanwhile, the intrinsic quality of the model, the loading amount of each factor within the indexes of basic fitness can reach a certain standard, showing that the intrinsic quality of the model is fine.
The measuring scale consists of 92 items, which can be divided into four subscales. The relation coefficients between each item and the subscale from .466 to .773 as well as related loading from .497 to .810 are analyzed by using Extraction Principal Component Analysis.
4.2 Reliability analysis
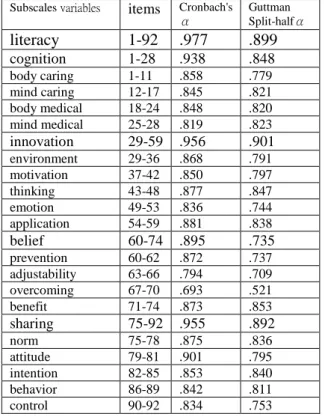
Cronbach’s α is used to evaluate the intrinsic consistence among the indicator factors within the structure, showing the reliability of the measuring scale. See Table 1.
Table 1 Subscales Cronbach's α Guttman Split-half α coefficient
Subscales variables items Cronbach's α Guttman Split-halfα literacy 1-92 .977 .899 cognition 1-28 .938 .848 body caring 1-11 .858 .779 mind caring 12-17 .845 .821 body medical 18-24 .848 .820 mind medical 25-28 .819 .823 innovation 29-59 .956 .901 environment 29-36 .868 .791 motivation 37-42 .850 .797 thinking 43-48 .877 .847 emotion 49-53 .836 .744 application 54-59 .881 .838 belief 60-74 .895 .735 prevention 60-62 .872 .737 adjustability 63-66 .794 .709 overcoming 67-70 .693 .521 benefit 71-74 .873 .853 sharing 75-92 .955 .892 norm 75-78 .875 .836 attitude 79-81 .901 .795 intention 82-85 .853 .840 behavior 86-89 .842 .811 control 90-92 .834 .753
In terms of Cronbach's α coefficient, all sub measuring scales exceed .90, while the sub measuring scale of health technology belief approximately reaches .90. The measuring scale, as a whole, reaches as high as .977. In addition, in terms of Guttman Split-half α, the perception overcoming of health technology belief is not as good as expected, while all other coefficients exceed .70. This shows
the theories well applied to health technology surroundings are mainly TPB, SCT, TAM, IDT, and HBM. Based on these theories, the contents of health technology literacy are established.
5 Conclusion and Suggestion
The development of the research tool took one year. It was a tedious work. So it was suggested that we can use some already available tests or measuring scales such as college students’ body and mind questionnaire, to function as a research tool. For this is both time saving and academically approved. The teaching model of health technology literacy can adopt the embedded teaching approach combined with mobile learning. This can improve the students’ health [10]. In fact, the contents of health technology literacy can be further interpreted and then divided into four special topic papers. For example, the study of the cognition of the health technology literacy of technological college students or something else. This can make the study more sophisticated than ever before. And then the result can be presented in international journals or academic conferences.In addition, we can put an eye on the current state of the health technology literacy of college students across the strait. Through means of consulting with experts, sampling investigation, and interviews, we can conduct cross strait academic research. This may enhance the competitiveness, and be more concerned about the physical and psychological growth of the students in these two areas. Brushing aside the enmity, we can enhance the interests and harmonious development of the body and mind of the students on both sides of the strait, and encourage students to participate in an equitable online operation through curriculum articulation [24] or embedded teaching of health technology literacy in mobile learning environment and constructing a bridge between the technological colleges and industries for teachers and practitioners.
Acknowledgements
This is part of a larger study on knowledge sharing of health technology and learning that has been financially supported by the National Science Council of Taiwan (NSC 96-2516-S-242-002).
References
[1]Ajzen, I. (2002). Perceived behavioral control, self-efficacy, locus of control, and the theory of planned behavior. Journal of Applied Social Psychology, 32, 665-683.
366 classrooms. Computers &Education, 39, 395-414 [3]Bose, R. (2003). Knowledge management-
enabled health care management systems: capabilities, infrastructure, and decision-support. Expert Systems with Applications. 24, 59-71. [4]Burdea, G. C., Coiffet, P. (2003), Virtual Reality
Technology (2nd edition), John Wiley & Sons, Inc., Hoboken, New Jersey.
[5]Cader, R. (2006). In search of evidence: A small scale study exploring how student nurses accessed information for a health needs assignment. Nurse Education Today. 26, 403-408 [6]Caplan, S. E. (2002), Problematic Internet use and psychosocial well-being: development of a theory- based-cognitive-behavioral measurement instrument,
Computers in Human Behavior, 18, 553-575.
[7]Carlbring, P., Bjornstjerna, E., Bergstrom, A., Waara, J., Andersson, G. (2007). Applied relaxation: an experimental analogue study of therapist vs. computer administration. Computers in Human Behavior. 23, 2-10.
[8]Colea, I. J., & Kelsey, A. (2004). Computer and information literacy in post-qualifying education, Nurse Education in Practice, 4, 190-199.
[9]Davis, R. A. (2001), A cognitive-behavioral model of pathological Internet use, Computers and Human Behavior, 17, 187-195.
[10]Garrett, B. M.; Jackson, C.(2006). A mobile clinical e-portfolio for nursing and medical students, using wireless personal digital assistants (PDAs). Nurse
Education in Practice. 6, 6, 339-346.
[11]Hakkinen, P.; Jarvela, S. (2006). Sharing and constructing perspectives in web-based conferencing.
Computers & Education. 47. 433–447.
[12]Henderson, S. (2002). Factors impacting on nurses’ transference of theoretical knowledge of holistic care into clinical practice. Nurse Education in Practice. 2, 244-250.
[13]Kim, Young-H. (2001). Korean Adolescents’ Health Risk Behaviors and Their Relationships with the Selected Psychological Constructs, Journal of adolescent Health, 29, 298-306. [14]Kimber, K., Pillay, H., Richards, C.(2007). Techno
literacy and learning: An analysis of the quality of knowledge in electronic representations of understanding. Computers & Education. 48. 59-79. [15]Kinzie, M. B. (2005) Instructional design
strategies for health behavior change. Patient Education and Counseling, 56, 3–15
[16]Koh, J., Kim, Y.-G. (2004). Knowledge sharing in virtual communities: an e-business perspective, Expert Systems with Applications, 26, 155-166. [17]Kukafka, R.; Johnson, S. ; Linfante, A.; Allegrante,
J. (2003). Grounding a new information technology implementation framework in behavioral science: a systematic analysis of the literature on IT use,
Journal of Biomedical Informatics, 36(3), 218-227. [18]Logan, J. R., & Price, S. L. (2004). Computer science education for medical informaticians, International
Journal of Medical Informatics, 73, 139-144.
[19]Lowerison, G., Sclater, J., Schmid, R., Abrami, C. (2006). Student perceived effectiveness of computer technology use in post-secondary classrooms. Computers & Education. 47, 465-489. [20]MacGregor (2003) Psychology, meaning and the
challenges of longevity. Futures, 35, 575-588.
[21]Maltby, J.; Day, L.(2001).Spiritual involvement
and belief: the relationship between spirituality and Eysenck’s personality dimensions. Personality and
Individual Differences. 30(2), 187-192
[22]Marcell, A. V. (2005). Adolescents' health beliefs are critical in their intentions to seek physician care.
Preventive Medicine. 41(1), 118-125.
[23]Marks, A. D.G. (2008). Assessing individual differences in adolescents’ preference for rational and experiential cognition. Personality and Individual Differences. 44, 1, 42-52.
[24]Mastersa, K., Oberprielerb, G. (2004). Encouraging equitable online participation through curriculum articulation, Computers & Education, 42, 319–332. [25]Olds, R. S.; Thombs, D. L. (2005). Relations
between normative beliefs and initiation intentions toward cigarette, alcohol and marijuana. Journal of
Adolescent Health. 37, 1, 75.
[26]Ryu, S., Ho, S. H., Han, I. (2003). Knowledge sharing behavior of physicians in hospitals, Expert Systems with Applications, 25, 113–122. [27]Saranto, K., Hovenga, E. J.S. (2004). Information
literacy—what it is about ? Literature review Of the concept and the context, International Journal of
Medical Informatics, 73, 503-513.
[28]Sharafi, P., Hedman, L., Montgomery, H. (2006).
Using information technology: engagement Modes, flow experience, and personality orientations.
Computers in Human Behavior. 22. 899-916. [29]Steinemann, A. (2000). Rethinking human health
impact assessment, Environmental Impact Assessment Review, 20, 627–645
[30]Wong, Chi-Yan & Tang, So-Kum (2005),
Practice of habitual and volitional health behaviors to prevent severe acute respiratory syndrome among Chinese adolescents in Hong Kong, Journal
of Adolescent Health, Vol: 36, Issue: 3, 193-200. [31]Yang, Hui-Jen, Farn, C. K. (2005). An
investigation the factors affecting MIS student burnout in technical-vocational college. Computers in Human Behavior. 21, 917-932. [32]Yeh, Siou-Wen; Lo, Jia-Jiunn (2005). Assessing
meta-cognitive knowledge in web-based computer-assisted language learning: a neural network approach, Computers and Education, 44, 97-113. [33]Yi, M.Y., Jackson, J. , Park, J. , Probst, J. C.(2006).
Understanding information technology acceptance by individual professionals: Toward an integrative view. Information & Management. 43. 350-363.