j o u r n a l h o m e p a g e : w w w . i n t l . e l s e v i e r h e a l t h . c o m / j o u r n a l s / i j m i
Mobile information and communication in the
hospital outpatient service
Wen-Yuan Jen
a, Chia-Chen Chao
b, Ming-Chien Hung
c, Yu-Chuan Li
d,∗, Y.P. Chi
e aDepartment of Information Management, Overseas Chinese Institute of Technology,Taichung, Taiwan, No. 100, Chiao-Kwang Road, Taichung 407, Taiwan, ROC
bDepartment of Management Information System, Ph.D. Program, National ChenChi University, No. 64, Sec. 2, Zhi-nan Rd., Wenshan, Taipei, Taiwan, ROC
cDepartment of E-Business, WuFeng Institute of Technology, No. 117, Sec. 2, Chian-Kuo Rd., Ming-Hsiung , Chia-yi, Taiwan, ROC
dGraduate Institute of Medical Informatics and Department of Medical Management, Taipei Medical University, Taipei, Taiwan, No. 250, Wu Hsing St., Taipei, Taiwan, ROC
eDepartment of Information Management, National ChenChi University, No. 64, Sec. 2, Zhi-nan Road, Wenshan, Taipei, Taiwan, ROC
a r t i c l e
i n f o
Article history:Received 13 October 2005 Received in revised form 7 March 2006
Accepted 11 April 2006
Keywords: Mobile technology Mobile outpatient service Healthcare providers
a b s t r a c t
Objectives: Most healthcare providers provide mobile service for their medical staff; however, few healthcare providers provide mobile service as part of their outpatient service. The mobile outpatient service system (MOSS) focuses on illness treatment, illness prevention and patient relation management for outpatient service users. Initiated in a local hospital in Taiwan, the MOSS pilot project was developed to improve outpatient service quality and pursue higher patient safety.
Method: This study focuses on the development of the MOSS. The workflow, architecture and target users of the MOSS are delineated. In addition, there were two surveys conducted as part of this study. After a focus group of medical staff identified areas in which outpatient services might be improved by the MOSS, the first survey was administered to outpatients to confirm the focus group’s intuitions. The second administration of the survey explored outpatient satisfaction after they used the MOSS service.
Results: With regard to outpatient attitudes, about 93% of participants agreed that the mobile outpatient service improved outpatient service quality. In the area of outpatient satisfaction, about 89% of participants indicated they were satisfied with the mobile outpatient service. Discussion/conclusion: Supported by our study finding, we propose that more diverse mobile outpatient services can be provided in the future.
© 2006 Published by Elsevier Ireland Ltd.
1.
Introduction
Healthcare services can be differentiated as either inpatient or outpatient. Outpatient healthcare is a vital component of the healthcare system and represents one of the strongest growth
∗Corresponding author. Tel.: +886 2 29307930x8866; fax: +886 2 29334823.
E-mail addresses:denise@ocit.edu.tw(W.-Y. Jen),vic@wanfang.gov.tw(C.-C. Chao),chemy@mail.wfu.edu.tw(M.-C. Hung), jack@tmu.edu.tw(Y.-C. Li),ypchi@mis.nccu.edu.tw(Y.P. Chi).
areas in the healthcare industry. Two-thirds of Taiwan’s total national health insurance (NHI) expenditure is spent on outpa-tient services; hence, managing outpaoutpa-tient services is of great importance[1]. Outpatient service plays a major role in health-care delivery in Taiwan.
1386-5056/$ – see front matter © 2006 Published by Elsevier Ireland Ltd. doi:10.1016/j.ijmedinf.2006.04.008
In its report of “Crossing the Quality Chasm: A New Health System for the 21st Century”, the Institute of Medicine (IOM) emphasizes the importance of patient safety[2]. Cur-rently, in the realm of patient safety, most hospitals focus on devices, procedures, professionals and healthcare delivery systems to pursue patient safety[3]. However, there is room to apply advanced information technology (IT) to further pur-sue patient safety. Information technology has the potential to transform the delivery of care by streamlining processes, making procedures more accurate and efficient and reducing the risk of human error[4]. Retrospective studies have pointed out that most mobile technology contributed to medical care [3,5–8], as the mobile services and devices were designed based on hospital staff requirements. Yet, there are few cases of applying mobile services to enhance patient safety in terms of outpatient services. Therefore, this research seeks to develop an integrated system which especially applies mobile technol-ogy to patient safety as well as outpatient service.
Owing to technological advances in diagnostics, medi-cation and procedure, most healthcare needs are neces-sarily handled on an outpatient basis [2]. Physicians and nurses are highly mobile in their hospital routine, moving fre-quently between outpatient clinics, therapeutic departments and operating theatres. Based on the physician’s and nurse’s workflow and mobility requirements, healthcare providers have adopted mobile technology to provide manifold medi-cal information and improved communication channels. Cur-rently, mobile information and communication systems play an important role in clinical routine. Mobile service has greatly improved communication [9], patient data entry[10], med-ical decision-making [5] and healthcare [11]. However, few healthcare providers employ mobile technology in their out-patient services. Outout-patient services still have much room for improvement. For example, outpatients often wait for a long time at doctors’ offices before receiving treatment; there is no
reminder service for outpatient appointments; hospitals are unable to notify a large number of outpatients about lectures, give healthcare reminders or offer birthday greetings.
The population and the ratio of users’ to use cellular phone numbers in Taiwan was 1:1.04 [12]. The high utilization of mobile communication is increasing dramatically each year. Most people are accustomed to communicating by cellular phone daily. The center of Patient Safety Informatics (PSI) in Wan Fang (W.F.) Hospital implemented the mobile outpatient service system (MOSS) to deliver manifold information to out-patients who owned cellular phone sets. The MOSS was also designed to send warning messages (e.g., abnormal laboratory test results) to physicians and administrators as well, thus, enabling the system to not only deliver high quality outpa-tient service but also to enhance paoutpa-tient safety.
2.
Study aims
The illness treatment, illness prevention and patient relations management aspects of outpatient services still have room for improvement. W.F. Hospital implemented the MOSS to improve the outpatient service quality and it was the first hos-pital to provide mobile outpatient service in Taiwan. Hence, this study focuses on that institution’s development of the MOSS.
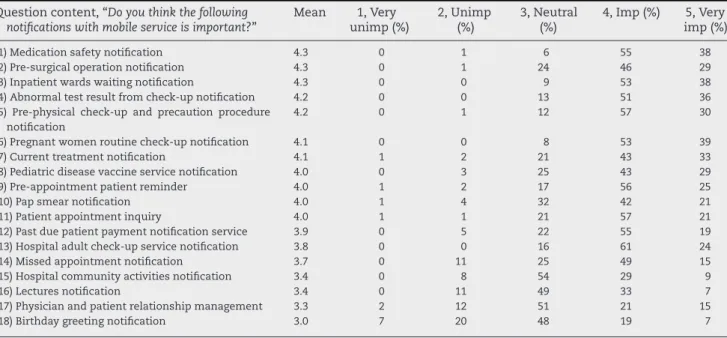
The MOSS project consists of medical staff (administrators and physicians) and technologists; they suggested 18 func-tions of mobile outpatient services (Table 1). Before imple-menting the MOSS, this project investigated outpatient atti-tudes toward the proposed mobile outpatient services. After a 6-month experiment period, the project surveyed MOSS user satisfaction. In this study, we present the results mainly for outpatients from W.F. Hospital and we sought to answer the following questions:
Table 1 – The questions of questionnaire ranked by means Question content, “Do you think the following
notifications with mobile service is important?”
Mean 1, Very unimp (%) 2, Unimp (%) 3, Neutral (%) 4, Imp (%) 5, Very imp (%)
(1) Medication safety notification 4.3 0 1 6 55 38
(2) Pre-surgical operation notification 4.3 0 1 24 46 29
(3) Inpatient wards waiting notification 4.3 0 0 9 53 38
(4) Abnormal test result from check-up notification 4.2 0 0 13 51 36
(5) Pre-physical check-up and precaution procedure notification
4.2 0 1 12 57 30
(6) Pregnant women routine check-up notification 4.1 0 0 8 53 39
(7) Current treatment notification 4.1 1 2 21 43 33
(8) Pediatric disease vaccine service notification 4.0 0 3 25 43 29
(9) Pre-appointment patient reminder 4.0 1 2 17 56 25
(10) Pap smear notification 4.0 1 4 32 42 21
(11) Patient appointment inquiry 4.0 1 1 21 57 21
(12) Past due patient payment notification service 3.9 0 5 22 55 19
(13) Hospital adult check-up service notification 3.8 0 0 16 61 24
(14) Missed appointment notification 3.7 0 11 25 49 15
(15) Hospital community activities notification 3.4 0 8 54 29 9
(16) Lectures notification 3.4 0 11 49 33 7
(17) Physician and patient relationship management 3.3 2 12 51 21 15
(18) Birthday greeting notification 3.0 7 20 48 19 7
Imp, important service; Unimp, unimportant service. The means are on a scale of 1–5. Smaller values of mobile service indicated a lower importance of outpatient service, while larger values indicated a greater importance of outpatient service. Sample size: 102.
• The introduction of the MOSS system: what is the workflow of the MOSS? What is the architecture? Who are the service targets?
• Outpatient attitudes: what were the outpatient’s attitudes before adopting the mobile outpatient service?
• Outpatient satisfaction: were the outpatient satisfied after receiving the MOSS service?
The followed sections are organized as follows: The intro-duction of the MOSS is described in Section3. The analytical methodology is briefly described in Section4. The results are presented in Section5and this study ends with the conclu-sions and a discussion.
3.
MOSS
3.1. Mobile technology applied in medical care
Mobile technology has aroused considerable interest among service providers, users, vendors and content developers. For medical care providers, significant mobile advances have been made in devices, applications and networking infrastructure. For example, home care[11], ER service[3], user interface ser-vice[8], medical knowledge access[6], mobile patient informa-tion[5,7,8], mobile healthcare computing devices[13,14]and security services[15]have gradually been adopted by health-care providers. More and more mobile tools and services have been developed.
To date, no hospital is actively providing mobile service for outpatients in Taiwan. Observing the current workflow of outpatient services, we considered the weaknesses of outpa-tient service that could be improved by mobile technology. This study portrays the practices outpatients, physicians and administrators:
(1) Outpatients, they often spend much waiting at inpatient ward counters to get into an inpatient ward. In addi-tion, check-up and preventative services, patient relations management and patient safety service, all were difficult to provide with limited resources.
(2) Physicians, notification of emergent events such as adverse drug effects, patient falls, needle sticks, unknown fevers and others, sometimes reach the assigned physicians after hours.
(3) Administrators, they often move about in the hospital and they need to timely information to manage the hospital more efficiently.
3.2. The description of MOSS
The workflow, architecture and target users of the MOSS are as follows:
3.2.1. The workflow of the MOSS
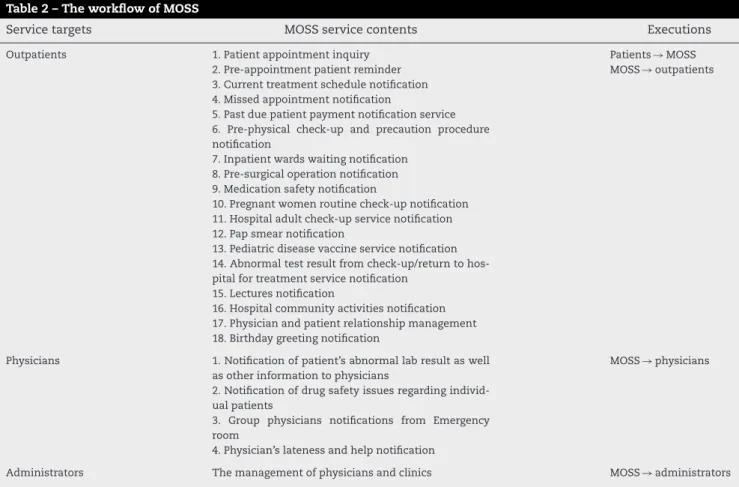
Table 2lists the service targets, service contents and execution of the MOSS. The MOSS was designed to contribute to illness
Table 2 – The workflow of MOSS
Service targets MOSS service contents Executions
Outpatients 1. Patient appointment inquiry Patients→ MOSS
2. Pre-appointment patient reminder MOSS→ outpatients 3. Current treatment schedule notification
4. Missed appointment notification
5. Past due patient payment notification service 6. Pre-physical check-up and precaution procedure notification
7. Inpatient wards waiting notification 8. Pre-surgical operation notification 9. Medication safety notification
10. Pregnant women routine check-up notification 11. Hospital adult check-up service notification 12. Pap smear notification
13. Pediatric disease vaccine service notification 14. Abnormal test result from check-up/return to hos-pital for treatment service notification
15. Lectures notification
16. Hospital community activities notification 17. Physician and patient relationship management 18. Birthday greeting notification
Physicians 1. Notification of patient’s abnormal lab result as well as other information to physicians
MOSS→ physicians 2. Notification of drug safety issues regarding
individ-ual patients
3. Group physicians notifications from Emergency room
4. Physician’s lateness and help notification
treatment, illness prevention and patient relations manage-ment. The MOSS was an integrated system that served outpa-tients, physicians and hospital administrators. The MOSS not only provided messages through mobile cellular phones and Internet e-mails, but also provided voice notification for aging patients who were not familiar with the operation of cellular phone short messages. In the following section, the workflow of the MOSS was delineated from the aspect of patients, physi-cians and administrators, respectively.
The outpatient services content of the MOSS can be explained briefly as follows:
(1) Outpatient appointment service. The MOSS provided an auto-matic inquiry function to reduce waiting time. Patients were allowed to check on the status of current outpa-tient receiving. The service automatically sent short, voice phone messages and Internet mails to outpatients. The purpose was to inform the outpatient service status and how many patients were in line ahead of his/her appoint-ment number. Related services are listed inTable 1. (2) Check-up and precaution service. Some services were
designed to remind the outpatient of precautions and pro-cedures to follow before receiving physical check-ups or surgery.
(3) Patient safety service. These services provided safety warn-ings and reminders which were related to patient safety issues.
(4) Patient relations management. The service improved enhanced patient relations management through the delivery of messages via mobile cellular phone, voice mail and Internet. Most messages communicated the physician’s concern about the patient’s health, birthday greetings and lectures for improving patient health. The physician’s service contents of the MOSS are explained as follows:
(1) ER notification: Use of this function mobilized a group of physicians to the emergency room, sending trauma patient pictures and data through the MOSS before the patient arrived at the emergency room.
(2) High risk reminder: This played the important role of deliv-ering critical radiology, pathology and other text reports to physicians.
(3) Adverse events notification: Through this function, physi-cians were notified of adverse drug events, patient falls, etc.
The administrator’s service content of the MOSS included: daily financial revenue information, outpatient visit and inpa-tient bed occupancy rate notifications, ER daily painpa-tient visits information, OPD new patient visit information, self-pay and insurance reimbursement financial information and adverse events notification information. MOSS sent the above infor-mation to administrators, facilitating efficient hospital man-agement.
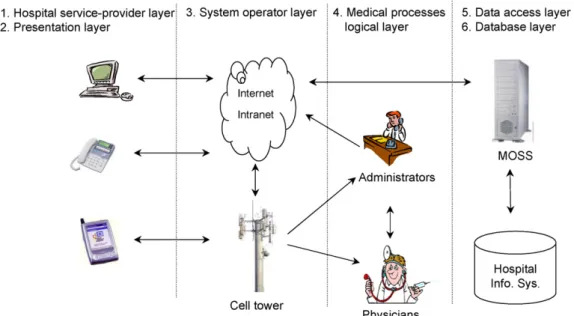
3.2.2. The architecture of the MOSS
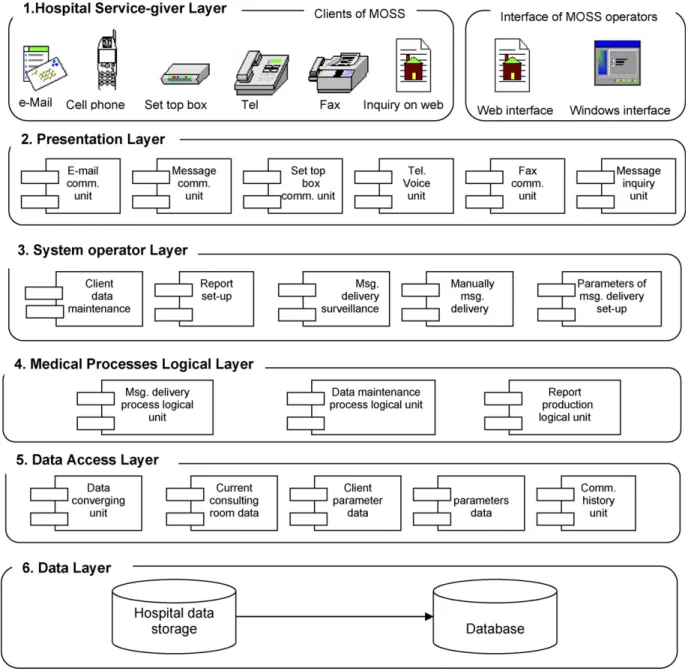
The MOSS was structured as follows. The MOSS offered a vari-ety of functions to deliver mobile services to dedicated medical processes and patients. Six subsystem layers including hospi-tal service-provider, presentation, system operators, medical processes logic, data access and database layers comprised the MOSS (Figs. 1 and 2).
(1) Hospital service-provider layer: This layer allowed for com-munication between administrators of hospitals, physi-cians and patients by means of e-mail, mobile messages, set top box, telephone, fax and Internet. The users of the MOSS were free to use mobile tools, capable of transmis-sion on the Internet.
(2) Presentation layer: Mobile tools dedicated to the MOSS allowed users to check messages from a visual menu. This
Fig. 2 – The layers of mobile MOSS architecture.
layer communicated with e-mail, mobile messages, set top box, telephone, fax and Internet. This not only pro-vided a visual menu for mobile tool users but also helped the operators of the MOSS deal with the maintenance of user menus, reports, monitoring message delivery, man-ual message delivery, parameters of the system and ser-vice requirements.
(3) System operator layer: This layer was an interface of commu-nication between the MOSS system and system operators. The interface provided for connection with workstations, Window NT platform and web pages in order to support all hospital medical information.
(4) Medical processes logic layer: All MOSS system logical functions were integrated in this layer, which was the core unit of mobile service including a processing log-ical unit, data maintenance unit and report-producing unit.
(5) Data access layer: This layer provided stability and effi-ciency in accessing data, helping the MOSS to manage the medical processes logical layer smoothly. It consisted of the following functions: data insertion, in-time refer-ral data, personal parameters, default parameters and a historical communication data function. All functions and parameters were executed in the application server with-out problems. In particular, MOSS reached highly accurate and consistent performance standards based on Microsoft COM+.
(6) Database layer: Any database utilizing the Microsoft .NET platform and ADO.NET was able to collaborate with MOSS system easily.
3.2.3. The target users of the MOSS
Fig. 3shows the service items in the MOSS (outpatient reser-vation, outpatient registration and abnormal test results
noti-Fig. 3 – The operating chart from outpatient service of MOSS.
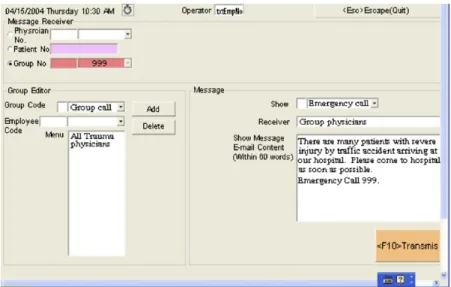
fications and greetings). System operators were able to set up functions for outpatients and physicians.Fig. 4shows the screen used to input short messages. The short message field allowed no more than 60 words. The system operator sent short messages to MOSS users by automatic or manual trans-mission.
InFig. 5, the MOSS sent the dedicated outpatient personal outpatient treatment data automatically (examples include pre-physical check-up or surgery precautionary procedure notification service and birthday greetings). In Fig. 6, the short message sent from the MOSS reminded physicians to pay attention to outpatient waiting time; meanwhile, a short
Fig. 4 – A short message being entered by a MOSS operator.
Fig. 6 – Samples of the MOSS for physicians and administrators.
MOSS reported to the administrator if the emergency room needed more physicians to treat outpatients.
4.
Study design
4.1. Procedures
To answer the questions outlined in Section2, there were two surveys conducted, one before and one after implementing the MOSS system.
4.1.1. Survey one
The project leaders considered that physicians and hospital administrators contact outpatients daily and that all of them understand the outpatients’ needs. Hence, the MOSS team members comprised 11 physicians and administrators. Based on the medical staffs’ experience and suggestions, the team designed various functions that focused on improving out-patient service. After completing the MOSS system design, the project team designed a questionnaire to measure out-patient attitudes toward adopting mobile outout-patient services. The purpose of survey one was to explore whether the MOSS met outpatients’ needs.
In January 2004, the MOSS project team designed the ques-tionnaire, which contained 19 questions regarding outpa-tient services. The first 18 questions asked participants which mobile services they thought would be important to improving
Fig. 7 – Responses of the participants to the 19th question of survey one questionnaire: “Do you think the mobile service will improve outpatient service quality?”.
outpatient service quality (Table 1). The 19th question asked the participants if they thought that mobile services would be important to improving outpatient service quality (Fig. 7). The questionnaire adopted a 5-point scale to measure the participants’ attitudes, 5 (very important/strongly agreed), 4 (important/agreed), 3 (neutral), 2 (unimportant/disagreed) and 1 (very unimportant/strongly disagreed). In addition, the par-ticipant’s education, sex, age and personal cellular phone were surveyed.
4.1.2. Survey two
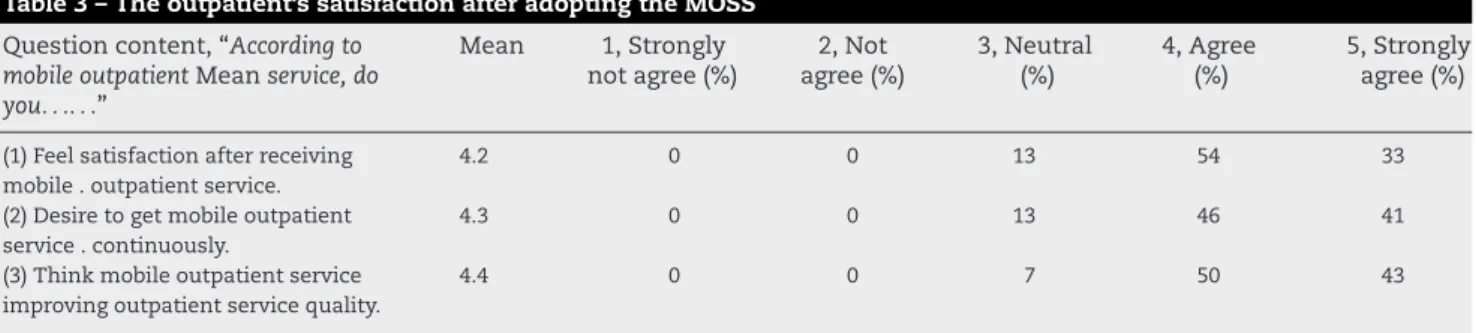
The second questionnaire was a telephone survey in which the MOSS users were asked three questions about their expe-rience using the MOSS service (Table 3). The survey adopted a 5-point scale to measure each participant’s satisfaction after using the MOSS service. Participants were asked to indicate whether they strongly agreed (5), agreed (4), were neutral about (3), disagreed (2) or strongly disagreed (1) with the survey state-ments.
4.2. Participants
In January 2004, before implementing the MOSS, 120 ques-tionnaires were distributed in survey one, which had an 85%
Table 3 – The outpatient’s satisfaction after adopting the MOSS Question content, “According to
mobile outpatient Mean service, do you. . .. . .” Mean 1, Strongly not agree (%) 2, Not agree (%) 3, Neutral (%) 4, Agree (%) 5, Strongly agree (%)
(1) Feel satisfaction after receiving mobile . outpatient service.
4.2 0 0 13 54 33
(2) Desire to get mobile outpatient service . continuously.
4.3 0 0 13 46 41
(3) Think mobile outpatient service improving outpatient service quality.
4.4 0 0 7 50 43
The means are on a scale of 1–5. Smaller values of agree indicated a lower satisfaction for mobile outpatient service, while larger values indicated a greater satisfaction for mobile outpatient service. Sample size: 198.
response rate. From the analysis of respondent characteris-tics, the majority of participants were female (65%) and 82% of participants’ educational background was beyond the high school level. Their average age was 39.2 years. Among the par-ticipants, 97% had cellular phones and over 82% of cellular phone users used the message and listened to voice message functions.
The PSI center employed the MOSS for 6 months from February to June in 2004. During the experiment period, the MOSS delivered approximately 10,300 service messages to 6700 patients from August 2004 to January 2005. In February 2005, survey two was conducted by telephone. A sample of 250 questionnaires were distributed and 198 questionnaires were completed. As the result, it had a 79% response rate. The majority of participants were female (58%), 67% of partic-ipants’ educational background was beyond the high school level and the average age was 48.6 years.
4.3. Course of the study
The primary target user group of the MOSS is outpatients. Based on the original outpatient service workflow, the PSI Center identified out the 19 kinds of mobile outpatient ser-vice content to prompt responses to outpatient serser-vice quality. Thus, we were able to elicit from the participating outpatients not only information regarding their needs, satisfaction with services and contribution of the MOSS to outpatient services and patient care, but also their implicit suggestions for future mobile outpatient service.
5.
Results
5.1. Survey one—outpatient’s attitudes
Table 1presents summary information ranked by means. The outpatient service means ranged from 4.3 (very important ser-vice being perceived) to 3.0 (neutral). In Table 1, we found that the means less than 4.0 were related to non-examination or non-medical outpatient services. In contrast, the means greater than 4.0 were related to examination or medical out-patient service. There were eleven types of service that were considered of significant importance.
According to the 19th question,Fig. 7shows diverse opin-ions on the potential value of the MOSS. The results showed that about 61% of participants “agreed” that the MOSS would improve outpatient services and 32% “strongly agree.” In sum, over 93% of participants agreed that the mobile outpatient ser-vice would improve outpatient serser-vice quality. Inspired by the results of survey one, the PSI Center was encouraged to imple-ment the MOSS.
5.2. Survey two—outpatient satisfaction
Table 3shows the agreement means ranging from 4.2 to 4.4, indicating that participants felt satisfied with mobile outpa-tient service, i.e., “Do you think mobile outpaoutpa-tient service will improve outpatient service quality?” This mean was the high-est among the three quhigh-estions. This might be attributed to the fact that MOSS users felt that with the mobile system
they could better manage their healthcare at no additional expense. In brief, this study concludes that the MOSS may have met the outpatients’ expectations.
6.
Discussions
The results of questionnaires imply that most outpatients care about the quality of outpatient services. Healthcare providers may consider offering more mobile medical care services for their patients. Improvements in the areas of timesavings, operational efficiency, missed appointment rate and overall outpatient service quality can be attributed to MOSS use. The main contribution of the MOSS may be as a stimulant to the growth of a new generation of mobile hardware and software with more outpatient service functions. We would like to pro-pose some suggestions for the future development of mobile outpatient systems:
6.1. Customized care for chronic patients
For chronic patients and their families, mobile services can be customized to meet these specific needs, such as provid-ing reminders or warnprovid-ings on dedicated dates. Additionally, adapting mobile service could look up chronic patient’s symp-toms from hospital databases. These foreseeable functions will facilitate improvement in patient safety without greatly increasing hospital operational costs.
6.2. Integrating clinical information systems into MOSS
The systematic integration of clinical information is a crit-ical component in most hospitals. It operates the clini-cian order entry, interactive clinical data repository sys-tems, multidiscipline documentation and point-of-care (POC). Applications might be integrated into a system that could be utilized for future development of mobile outpatient services.
6.3. Integration of mobile tools into hospital information systems
A synchronous integration of mobile tools and hospital infor-mation systems provide an interactive platform for patients and hospitals. Home care delivery and emergency medical service (EMS) could benefit from mobile services as well. Fol-lowing, we provide three possibilities. (1) Emergency medical services (EMS): first-aid personnel forward patients’ data to dedicated hospitals before they reach the emergency room. Hospital information departments might get the patient’s care records over XML-based systems in cases where the patient’s care records do not belong to a particular ded-icated hospital. (2) Citizen health system (CHS): we sug-gest that some chronic patients be equipped with mobile global positioning, system-enabled tools. This will assist these chronic patients when confronted with any sudden situations and allow EMS to know where the patients are. (3) Patient safety: IT ensures streamlined processes for patient safety and makes the processes more accurate and efficient. The
powerful functions of mobile service drastically reduce the risk of human error. EMS providers could access data from referral information systems, EMS databases and others; addi-tionally, patients could access data from hospital databases by following directions provided by a referral information system.
6.4. Developing a new generation of mobile hardware and software
Various tools for mobile information processes and commu-nication are commercially available at present. The ability of currently available personal digital assistants (PDA), display and text input devices (mostly pen-based) and mobile com-puters (pen-based notebook comcom-puters and laptops, virtual terminals, etc.) to communicate with and integrate into hospi-tal information systems can be expected in the near future. In other words, hospital mobile services coordinated with mobile tools dedicated for patients are diffusing and assimilating and this will encourage more patients to adopt mobile services from hospitals for more efficient, higher quality service.
7.
Conclusions
The conclusions of this study were based on outpatient ser-vice, physician patient care and administrator’s managerial perspectives.
Traditionally, the missed appointment rate of outpatients in W.F. Hospital was around 15–17%. Forgetting appointments and having to wait too long were main reasons for missed appointments. After the 6-month experiment period, the MOSS helped the missed appointment rate drop to around 5%. The MOSS not only improves outpatients’ missed appoint-ment rate, but also reminded outpatient to get regular physical check-ups.
After adopting the MOSS, severe abnormal test results reached the physicians effectively, saving from 72 to 30 h. Meanwhile, the utilization rate of adverse events notifications increased 500% because the medical staff were able to provide instant care after they received the adverse events notifica-tion. For physicians, the MOSS increased the patient safety. For managers, the MOSS provided managerial notifications and reports. Based on the MOSS reporting data, the administra-tors enhanced their response time in dealing with all crises and improved hospital management.
With fast and far-reaching changes, mobile technology plays the role of promoting patient safety in various fields of medical care and promotes patient service. In the future, we will expand the MOSS functions in outpatient services, which will play the role of a multi-functional healthcare agent to increase healthcare service quality in an era of mobile out-patient services.
Acknowledgements
The authors are most grateful to the PSI staff at Wan Fang Municipal Hospital for their active participation in this project. Thanks also to the reviewers for their valuable comments on this paper.
Summary points
What was known before the study
• Mobile technology can meet the dynamic workflow requirements of medical care providers in their clin-ical routine.
• Inability to foresee daily outpatient caseload leads to long waits for patients and affects the quality of care provided.
• At present, it is difficult to deliver various patient noti-fications and to manage patient relations.
What the study has added to our knowledge
• Employing cutting-edge technologies, mobile health-care service is able to provide various notifications to patients and (by providing real-time waiting line updates) to decrease waste of outpatient time. • Mobile healthcare service delivers important
informa-tion to patients, medical staff and healthcare admin-istrators more quickly than conventional telephone or paper systems, reducing risk to patients.
• In areas with high mobile communication use, health-care providers can utilize mobile technology to create and maintain systems for provider-patient communi-cation which promote closer provider-patient relations and increase patient safety.
r e f e r e n c e s
[1] S. Su, C.L. Shih, Managing a mixed-registration-type appointment system in outpatient clinics, Int. J. Med. Inf. 70 (1) (2003) 31–40.
[2] K.J. Klassen, T.R. Rohleder, Scheduling outpatient appointment in a dynamic environment, J. Opera Manage. 14 (1996) 83–101.
[3] V. Anantharaman, H.L. Swee, Hospital and emergency ambulance link: using IT to enhance emergency pre-hospital care, Int. J. Med. Inf. 61 (2–3) (2001) 147–161. [4] M. Bang, A. Larsson, E. Berglund, H. Eriksson, Distributed
user interfaces for clinical ubiquitous computing applications, Int. J. Med. Inf. 74 (7–8) (2005) 545–551. [5] D. Krause, F. Hartl, M. Theis, K.E. Stangl, A.T. Gerauer,
Mehlhorn, mobile decision support for transplantation patient data, Int. J. Med. Inf. 73 (5) (2004) 461–464.
[6] W. Michalowskia, S. Rubinb, R. Slowinskic, S. Wilkc, Mobile clinical support system for pediatric emergencies, Decision Support Syst. 36 (2003) 161–176.
[7] P.Y.K. Chau, P.J.H. Hu, Investigating healthcare professionals’ decisions to accept telemedicine technology: an empirical test of competing theories, Inf. Manage. 39 (4) (2002) 297–311.
[8] R. Andrade, A.V. Wangenheim1, M.K. Bortoluzzi, Wireless and PDA: a novel strategy to access DICOM-compliant medical data on mobile devices, Int. J. Med. Inf. 71 (23) (2003) 157–163.
[9] E.G. Poon, G.J. Kuperman, J. Fiskio, D.W. Bates, Real-time notification of laboratory data requested by users through
alphanumeric pagers, J. Am. Med. Inform. Assoc. 9 (3) (2002) 217–222.
[10] C.A. Williams, T. Templin, A.D. Mosley-Williams, Usability of a computer-assisted interview system for the unaided self-entry of patient data in an urban rheumatology clinic, J. Am. Med. Inform. Assoc. 11 (4) (2004) 249–259.
[11] N. Maglaveras, V. Koutkias, I. Chouvarda, D.G. Goulis, A. Avramides, D. Adamidis, G. Louridas, E.A. Balas, Home care delivery through the mobile telecommunications platform: the citizen health system (CHS) perspective, Int. J. Med. Inf. 68 (1–3) (2002) 99–111.
[12] FIND,http://www.find.org.tw, 2004/05/10.
[13] B. Lin, J.A. Vassar, Mobile healthcare computing devices for enterprise-wide patient data delivery, Int. J. Mobile Commun. 2 (4) (2004) 343–353.
[14] E. Ammenwerth, A. Buchauer, B. Bludau, R. Haux, Mobile information and communication tools in the hospital, Int. J. Med. Inf. 57 (1) (2000) 21–40.
[15] P. Jelekainen, GSM-PKI solution enabling secure mobile communications, Int. J. Med. Inform. 73 (3) (2004) 317– 320.