Dens evaginatus
333 Kaohsiung J Med Sci July 2005 • Vol 21 • No 7
F
ACIAL
C
ELLULITIS
A
RISING
FROM
D
ENS
E
VAGINATUS
:
A C
ASE
R
EPORT
Chun-Ming Chen, Kun-Tsung Lee,1 Fu-Hsiung Chuang,2 Yi-Yuh Hong,1 Hsiu-Chuan Chen,1 Kun-Rong Hsu,1 Yi-Min Wu,1 and Huey-Er Lee3
Departments of Oral and Maxillofacial Surgery, 1Family Dentistry, 2Conservative Dentistry, and 3Prosthodontics, Kaohsiung Medical University, Kaohsiung, Taiwan.
Dens evaginatus is a developmental anomaly that produces a tubercle on the occlusal surface of a tooth. It is found most frequently in the mandibular premolars. The occlusal tubercle easily causes occlusal interferences. Attrition or fracture of the tubercle can lead to pulpitis, pulp necrosis, periapical pathosis, and periapical infection. This case report illustrates the treatment of facial cellulitis arising from dens evaginatus with open apex. Calcium hydroxide was used for the apexification procedure. One year after canal obturation, radiography revealed no apical pathosis and the apical seal was evident.
Key Words: facial cellulitis, dens evaginatus (Kaohsiung J Med Sci 2005;21:333–6)
Received: December 9, 2004 Accepted: April 12, 2005 Address correspondence and reprint requests to: Dr. Kun-Tsung Lee, Department of Family Dentistry, Kaohsiung Medical University, 100 Shih-Chuan 1st Road, Kaohsiung 807, Taiwan.
E-mail: [email protected]
© 2005 Elsevier. All rights reserved.
Dens evaginatus is a rare dental anomaly involving an extra cusp or tubercle that protrudes from the occlusal surface of the affected tooth. It occurs in the mandible more frequently than in the maxilla and is most commonly seen in premolars, but may occur in molars, canines, and incisors [1]. The prevalence of dens evaginatus ranges from 1.1% to 4.3% of people, with a higher incidence among Asians [2–4]. Lin and Roan found an overall prevalence of 3.52% in the southern region of Taiwan [5].
Dens evaginatus is easily worn or fractured, resulting in pulp exposure, pulp infection, loss of vitality, and infection of facial structures. A history of pulp necrosis in a noncarious tooth and unusual root formation support the presence of dens evaginatus. Endodontic management of the pulpless permanent tooth with a wide-open blunderbuss apex has long presented a challenge to dentistry. This condition necessitates endodontic procedures, such as apexification with subsequent obturation in teeth with immature apices, or removal of the tooth [6]. Calcium hydroxide has long been recognized for its antibacterial effects and is the material
of choice for apical barrier formation and healing [7]. If a tooth with incomplete root formation is found to be nonvital at the time of diagnosis, calcium hydroxide can be used to provide apical closure. This article presents a case of facial cellulitis arising from dens evaginatus with open apex and apexification treatment using calcium hydroxide.
C
ASEP
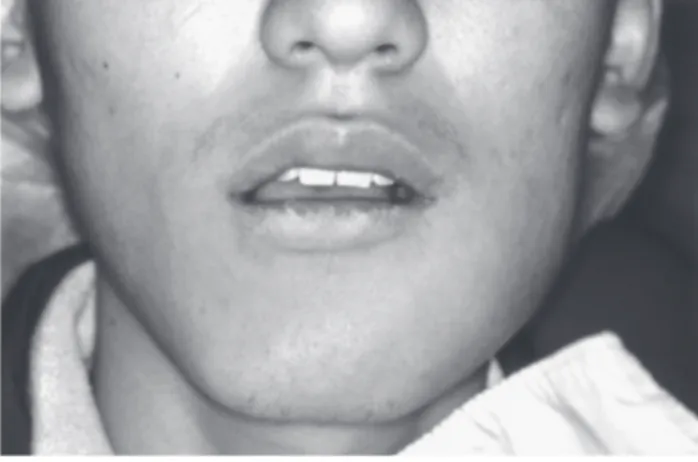
RESENTATIONA 20-year-old man was referred to our department with the chief complaint of painful swelling over the left side of his face. He had developed this symptom following a left mandibular second premolar toothache 3 days earlier. Extraoral examination revealed a firm, warm, and diffused swelling affecting the left facial region with buccal and masticatory space involvement (Figure 1). Intraoral exam-ination showed a worn tubercle on the occlusal surface of the left mandibular second premolar and an otherwise normal crown (Figure 2). The tooth was extremely tender to percussion and its buccal sulcus presented a diffuse firm swelling. An open apex and radiolucency in the periapical area were found on radiography (Figure 3). A diagnosis of facial cellulitis arising from dens evaginatus was made. On intraoral and radiographic examinations, the remaining seven premolars showed complete root formation without
Kaohsiung J Med Sci July 2005 • Vol 21 • No 7 C.M. Chen, K.T. Lee, F.H. Chuang, et al
334
formation, so the canal was obturated with gutta-percha and the cavity was restored with composite resin. One year after canal obturation, radiography showed improved apical healing (Figure 4).
D
ISCUSSIONDens evaginatus is an uncommon dental anomaly in which an extra cusp or tubercle protrudes from the occlusal surface of posterior teeth or the lingual surface of anterior teeth. The tubercle of dens evaginatus is frequently susceptible to
Figure 1. The left buccal and masticatory spaces are involved and have painful swelling.
Figure 2. The left mandibular second premolar shows a worn tubercle on the occlusal surface between the buccal and lingual cusps. The buccal sulcus presents a diffuse firm swelling.
Figure 3. Radiography reveals incomplete root formation with an open apex and radiolucency in the periapical area.
dens evaginatus involvement. Tracing the patient’s history revealed that a sinus tract had persisted over the buccal gingival area of the left mandibular second premolar for several years; his medical history was noncontributory.
On the same day, the pulp chamber was opened without anesthesia and purulent pus discharged from the pulp chamber. Through gentle debridement and saline irrigation, the pulp chamber was open-drained through the occlusal surface of the dens evaginatus, and a systemic antibiotic was delivered. Four days later, the pain and swelling had subsided, and no more pus was being discharged from the pulp chamber. The canal was thoroughly cleaned and a thick paste of calcium hydroxide was applied every 4 weeks to induce apical closure. The calcium hydroxide was changed a total of seven times. Seven months later, radiography showed evidence of apical closure as a result of hard-tissue
Figure 4. One year after canal obturation, radiography shows a well-defined lamina dura and no radiolucent apical lesion.
Dens evaginatus
335 Kaohsiung J Med Sci July 2005 • Vol 21 • No 7
fractures and pulp complications. The reported incidence of pulp-involved teeth ranges from 14.1% to 40.2% [2,3,5]. Lin and Roan reported that 89.3% of dens evaginatus are worn, 19.6% with nonvital pulp response [6]. In the case of early pulp exposure or infection of the pulp by bacterial access through immature dentinal tubules, the sequel is pulp necrosis.
Emphasis should be placed on early detection of this anomaly and on proper prophylactic treatment. Many treatment options for dens evaginatus have been reported in the literature [4,6–8], and these have changed over time. Treatments include grinding the cusp to encourage second-ary dentin formation, reducing the risk of attrition or fracture of the tubercle by elimination of opposing occlusal interferences, protection of the tubercle with pit and fissure sealant (or by composite resin reshaping), and removal of the tubercle followed by direct or indirect pulp capping and partial pulpotomies [6]. Treatments for pulp involve-ment include conventional endodontic therapy, calcium hydroxide technique for apexification, surgical root canal therapy, or extraction of the tooth [6].
Endodontic treatment can be complicated further by incomplete root formation with an open apex. An apexi-genesis procedure treats an open apex with vital pulp, while an apexification procedure treats an open apex with nonvital pulp. Kaiser first reported the use of calcium hydroxide for apexification in the pulpless tooth in 1964 [9]. Calcium hydroxide is considered to fulfill many of the properties of an ideal root canal dressing due to its moderate antibacterial action, its ability to induce hard tissue formation and to cause intracanal occlusion, and its tissue-dissolving capability [7]. Since 1964, calcium hydroxide alone or in combination with other drugs has become the most widely accepted material to promote apexification. This case presents a dens evaginatus with incomplete root formation. In order to perform root canal therapy, the root needs to be completely formed. Calcium hydroxide is used to medicate and initiate apex closure in order to complete the tooth development.
The usual time required for apexification is 6–24 months [7,10]. There are four successful clinical results of apexification procedures: continued closure of the canal and apex to a normal configuration; apex closure, although the canal retains a blunderbuss configuration; no radiographic change, but a thin osteoid-like barrier providing definite closure; and radiographic evidence of an apical barrier [7]. In our case, formation of a thin osteoid-like apical barrier was shown by radiography after 7 months. Facial cellulitis arising from dens evaginatus with an open apex is uncommon. The result of this case report showed adequate infection control and successful apexification by calcium hydroxide.
R
EFERENCES1. Geist JR. Dens evaginatus. Case report and review of the literature. Oral Surg Oral Med Oral Pathol 1989;67:628–31. 2. Merrill RG. Occlusal anomalous tubercles on premolars of
Alaskan Eskimos and Indians. Oral Surg Oral Med Oral Pathol 1964;17:484–96.
3. Yong SL. Prophylactic treatment of dens evaginatus. ASDC J
Dent Child 1974;41:289–92.
4. Uyeno DS, Lugo A. Dens evaginatus: a review. ASDC J Dent
Child 1996;63:328–32.
5. Lin LC, Roan RT. Incidence of dens evaginatus investigated from three junior middle schools at Kaohsiung City. Formosan
Sci 1980;34:113–21.
6. Huang TJ, Roan RT. Clinical study of dens evaginatus cases with pulpal involvement. Kaohsiung J Med Sci 1997;13: 440–7.
7. Weine FS. Alternatives to routine endodontic treatment. In: Weine FS, ed. Endodontic Therapy, 3rd
edition. St Louis: Mosby, 1982:561–92.
8. Gaynor WN. Dens evaginatus—how does it present and how should it be managed? N Z Dent J 2002;98:104–7.
9. Kaiser HJ. Management of wide open canals with calcium hydroxide. Read before the American Association of Endodontists, Washington DC, 1964.
10. Camp JH. Pedodontic endodontic treatment. In: Cohen S, Burns RC, eds. Pathways of the Pulp, 8th
edition. St. Louis: Mosby, 1991:682–719.
Kaohsiung J Med Sci July 2005 • Vol 21 • No 7 C.M. Chen, K.T. Lee, F.H. Chuang, et al