Radiation dose evaluation of dental cone beam computed tomography using an anthropomorphic adult head phantom
Jay Wua,*, Cheng-Ting Shihb, Chang-hung Hoc, Yan-Lin Liud, Yuan-Jen Change, Max Min Chaoc, and Jui-Ting Hsuf
a Department of Biomedical Imaging and Radiological Science, China Medical University, No.91, Hsueh-Shih Road, Taichung City 40202, Taiwan, R.O.C.
b Department of Biomedical Engineering and Environmental Sciences, National Tsing-Hua University, 101, Sec. 2, Kuang-Fu Rd., Hsinchu City 30013, Taiwan, R.O.C.
c Department of Medical Imaging and Radiological Science, Central Taiwan University of Science and Technology, No.666, Buzih Road, Beitun District, Taichung City 40601, Taiwan, R.O.C.
d Institute of Nucelar Engineering and Science, National Tsing-Hua University, 101, Sec. 2, Kuang-Fu Rd., Hsinchu City 30013, Taiwan, R.O.C.
e Department of Management Information Systems, Central Taiwan University of Science and Technology, No.666, Buzih Road, Beitun District, Taichung City 40601, Taiwan, R.O.C.
f School of Dentistry, China Medical University, No.91, Hsueh-Shih Road, Taichung City 40202, Taiwan, R.O.C.
Corresponding author:
Jay Wu, PhD, Associate Professor
Department of Biomedical Imaging and Radiological Science, China Medical University, No.91, Hsueh-Shih Road, Taichung City 40202, Taiwan, R.O.C.
Tel: (886)-4-22053366#7809 Fax: (886)-4-22053366
Abstract
Dental cone beam computed tomography (CBCT) provides high-resolution tomographic images and has been gradually used in clinical practice. Thus, it is important to examine the amount of radiation dose resulting from dental CBCT examinations. In this study, we developed an in-house anthropomorphic adult head phantom to evaluate the level of effective dose. The anthropomorphic phantom was made of acrylic and filled with plaster to replace the bony tissue. The contour of the head was extracted from a set of adult computed tomography (CT) images. Different combinations of the scanning parameters of CBCT were applied. Thermoluminescent dosimeters (TLDs) were used to measure the absorbed doses at 19 locations in the head and neck regions. The effective doses measured using the proposed phantom at 65, 75, and 85 kVp in the D-mode were 72.23, 100.31, and 134.29 µSv, respectively. In the I-mode, the effective doses were 108.24, 190.99, and 246.48 µSv, respectively. The maximum percent error between the doses measured by the proposed phantom and the Rando phantom was l4.90%. Therefore, the proposed anthropomorphic adult head phantom is applicable for assessing the radiation dose resulting from clinical dental CBCT.
Keywords: dental cone beam computed tomography (CBCT), anthropomorphic phantom, thermoluminescent dosimeters (TLD)
1. Introduction
Dental cone beam computed tomography (CBCT) can rapidly provide high-resolution cross-sectional images for clinical diagnoses. By using surface and volume rendering, the three-dimensional (3D) structures of the bones and soft tissues in the oral cavity, such as the maxilla and mandible, can be reconstructed (Kuszyk et al., 1996; Cavalcanti et al., 2004; Scarfe et al., 2006). Visualizing these structures by using 2D and 3D images helps dental practitioners accurately and safely perform dental therapies such as orthodontic therapy (Scarfe et al., 2006; Silva et al., 2008), implantation (Ruivo et al., 2009; King et al., 2012), and dentition reconstruction (Qiu et al., 2012; Barone et al., 2013). In addition, dental CBCT images with a large field of view (FOV) are used to diagnose lesions around the oral and sinus cavity {Januario, 2008 #25} (Simon et al., 2006) and guide the reconstruction or reshaping of facial bones (Meng et al., 2012). Because of these applications, dental CBCT has become a vital diagnostic tool in clinical practice. Consequently, it is essential to evaluate the radiation dose of dental CBCT.
Several measurement tools, such as the dose area product (DAP) meter (Poppe et al., 2007; Lofthag-Hansen et al., 2008; Han et al., 2012), metal-oxide semiconductor field-effect transistor (MOSFET) (Koivisto et al., 2012), and Farmer-type ion chamber (Yu et al., 2010; Batista et al., 2012), have been used to evaluate the dose of dental CBCT. In addition, thermoluminescent dosimeters (TLDs) coupled with an anthropomorphic phantom are an effective tool for measuring dental CBCT radiation doses (Ludlow et al., 2006; Roberts et al., 2009; Qu et al., 2012). TLDs are inserted in the phantom at different locations corresponding to specific organs. The effective dose is calculated based on the TLD readout by applying the conversion factor and the tissue weighting factors. At present, the Alderson Rando anthropomorphic phantom made in accordance with the ICRU-44 standards (ICRU, 1989) is commonly applied in clinical dose evaluations (Ludlow and Ivanovic, 2008). The phantom is shaped to a human torso and sectioned into slabs. Its composition simulates human muscle, bone, air cavities, and other tissues. The tissue-equivalence of the Rando phantom for the beam quality of diagnostic x-rays has been proven (Tsiklakis et al., 2005).
In this study, we proposed a home-made anthropomorphic adult head phantom. The phantom was built by stacking polymethylmethacrylate (PMMA) slabs that were segmented based on actual CT images of the
head and neck of a patient. Dental restorative materials were used to fill the bone sites to mimic the bony structures. The proposed phantom was used to measure the x-rays emitted from the CBCT scanner. After comparing our measurements with those of the Rando phantom, we could determine the applicable of the proposed head phantom for evaluating the effective dose during dental CBCT scanning.
2. Materials and Methods
2.1 Self-made anthropomorphic phantom
The anthropomorphic phantom built in this study was based on a set of CT images of a 78 years old male patient (170 cm and 68 kg). Two thresholds of -250 HU and 200 HU were applied on these images to segment the contours of the head, air cavity, and bony structures. These contours were then used to guide the laser cutting machine to cut the PMMA slabs automatically. To simulate the bone in our phantom, the plaster-water mixture with a volume ratio of 2:1 was filled into the bony compartments in each PMMA slab. After 4 hours of solidification of the mixture in the ambient condition, the PMMA slabs were stacked up and fixed by two PMMA rods across the slabs.
2.2 Dental CBCT scanner
A commercially available dental CBCT scanner (AZ3000, Asahi Roentgen, Japan) was used. It was calibrated for geometric alignment, center of rotation, image resolution, and image uniformity before the
study. Four exposure protocols are available in this scanner, including panoramic, temporomandibular joint
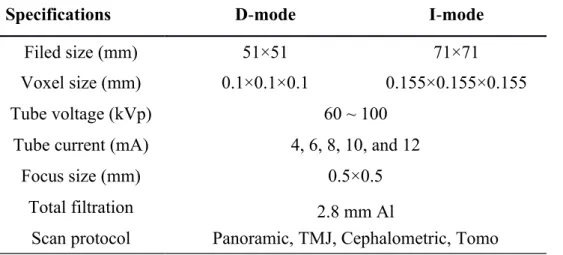
(TMJ), cephalometric and tomo scans, and two FOVs can be set including the dental mode (D-mode) and the child mode (I-mode). Table 1 shows the specifications of the dental CBCT. Here, we used the tomo scan protocol, which can be at 65, 75, and 85 kVp and D/I mode, to evaluate the radiation doses of the proposed phantom and Rando phantom. The tube current (mA) and the scan time (sec) of the scanning protocol were set to 6 mA and 17 s, respectively.
2.3 Dose measurements
TLD chips (TLD-100, LiF: Mg, Ti), having a minimum detection limit of 0.3 mGy and linear dose response between 0.3 and 32 mGy (Bauk et al., 2011), were used to measure the absorbed dose. First, the TLDs were put into a thin PMMA disk and then irradiated against an ion chamber by using 85 kVp and 102
mAs. The field size was 20 × 20 cm2 to cover the entire disk. The TLDs were read out after 24 hours post-irradiation by the RA’94 TLD reader-analyzer (Microlab, Poland). Any TLD with a dose-response variation greater than 5% was excluded from further usage and analysis. The thermoluminescent (TL) signal of the TLD chip was divided by the mean TL signal, and the results were used as calibration factors.
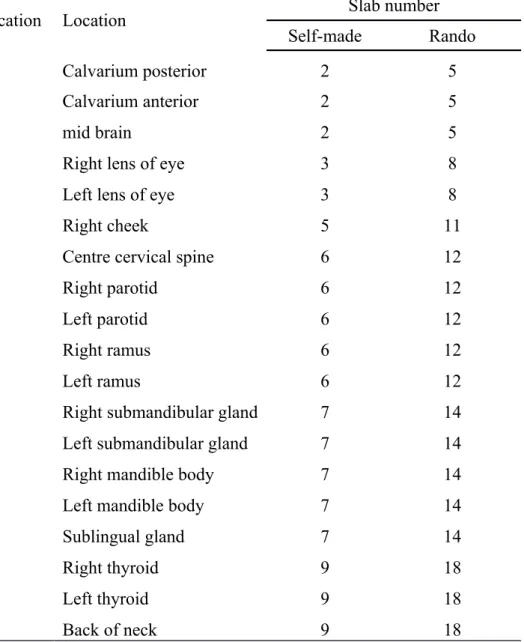
A total amount of 57 TLDs were selected. 19 locations in the anthropomorphic phantom were chosen and listed in Table 2; several small holes were drilled accordingly in the phantom and three TLD chips were inserted in each location. The measurement was repeated three times at each location using the tomo scan protocol with both FOVs and three kVps. The effective doses of the proposed phantom and the Rando phantom were evaluated.
2.4 Calculating the effective dose of radiation
The readouts of TLDs were converted to the equivalent dose by using the dose response curve (Fig. 1) with r2 value of 0.993 and the radiation weighting factor (wR = 1). Furthermore, the effective dose (E) (Roberts et al., 2009) was calculated as follows:
T T T
E
W H (1)where T indicates the organ or tissue of interest. WT denotes the tissue weighting factor for the organ or tissue T. HT is the tissue equivalent dose averaged over the TLD measurements. In this study, the tissue weighting factors were taken from the ICRP Report 103 (ICRP, 2007; Theodorakou et al., 2012).
3. Results
Fig. 2 shows the front view of the proposed anthropomorphic phantom and the Rando phantom. The self-made phantom consists of 19 slabs each with 1-cm thickness, while the head and neck of the Rando phantom is covered by 9 slabs each with 2.5-cm thickness. Because of the slightly small dimension of the proposed phantom, four additional shoulder slabs were added to maintain the height of both phantoms.
The mean TLD dose of each location ranged from 0.38 mGy for the D-mode scan of Rando phantom with 65 kVp to 24.60 mGy for the I-mode scan of the proposed phantom with 85 kVp. These dose values are
higher than the detection limit of the TLD chips (Bauk et al., 2011) and in the linear range of the dose response curve. The coefficient of variance (CV%) of the mean TLD dose at each location was calculated. For the two operating modes and three tube voltages, the CV% for the Rando phantom ranged from 2.79% to 5.55%, and the CV% for the proposed phantom ranged from 2.05% to 4.49%.
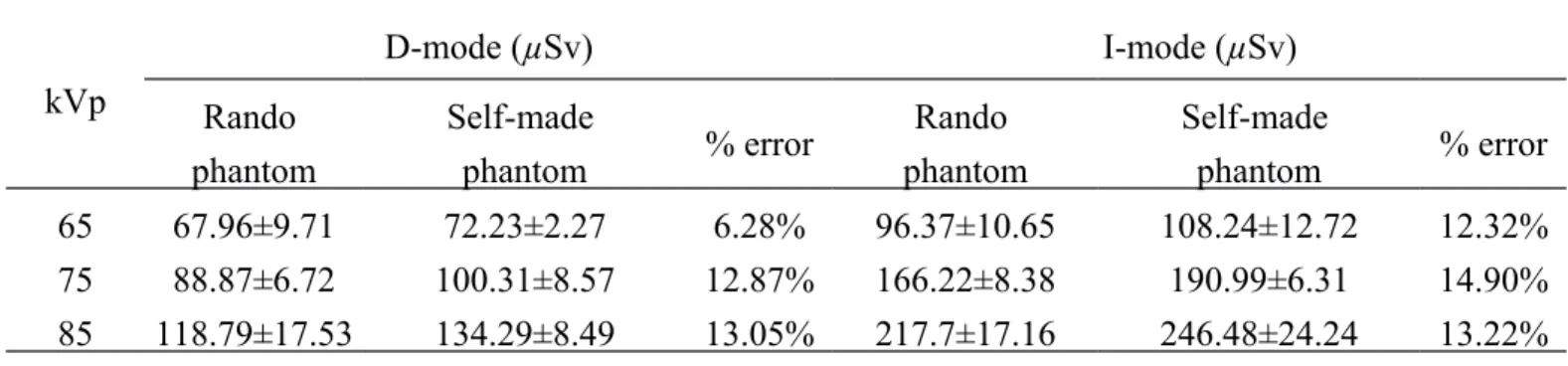
The effective doses measured using both phantoms and the percent errors between them are listed in Table 3. The minimum percent error between two phantoms was 6.28% at the D-mode with tube voltage of 65 kVp. As the tube voltage and FOV increased, the percent errors between phantoms also increased. The maximum percent errors for the D-mode and I-mode were 13.05% at 85 kVp and 14.90% at 75 kVp, respectively. There was a large difference of the measured effective doses between modes. At 65 kVp, the effective doses under the I-mode were approximately 45% higher than the doses under the D-mode. When the tube voltage increased to 75 and 85 kVp, the effective doses increased 83% ~ 90% between the D-mode and the I-mode. This is mainly because the I-mode has larger field size than the D-mode. The TLDs thus receive more radiation dose from primary and scattered x-ray beams.
4. Discussion
The Rando anthropomorphic phantom is the most commonly used model in clinical radiation dose evaluation. However, it is costly and is not affordable to the dental clinics. In this study, we built an anthropomorphic adult head phantom to evaluate the x-ray doses emitted from the dental CBCT. In the proposed phantom, PMMA slabs were used to shape the outer contour of the head and neck and to simulate soft tissue, while plaster was used to simulate the bony structures. The major advantage of the self-made head phantom is the low price. The total costs including the material costs and production costs are about $ 500 that is far lower than the price of the Rando phantom.
Plaster is a common bone substitution material to fill bone defects (Peltier, 1957; Hadjipavlou et al., 2001). It can be molded into different shapes and is easy to prepare and operate in clinical practice. In the proposed phantom, the plaster-water mixture with a volume ratio of 2:1 was used to mimic the bony structures. The mixing ratio is critical. Increasing the proportion of water makes the mixture hard to solidify,
whereas increasing the amount of plaster results in easy fragmentation. In addition, the mixing ratio changes the effective atomic number (Z) and electron density (ρe). The plaster-water mixture for the proposed phantom has an effective Z of 14.2 and electron density of 3.07×1023, which is comparable to the cortical bone (Z=13.23 and ρe=3.09×1023) (ICRU, 1989). The influence of the elementary composition and mixing ratio of the bone substitution material on the absorbed dose needs to be further investigated.
The percent errors between the effective doses measured using the Rando phantom and the proposed phantom were less than 15% for all tomographic scanning protocols. The inconsistency can be attributed to two factors. First, the soft tissue and bone in the proposed phantom are mimicked using PMMA and plaster. The attenuation characteristics of these materials may differ from the materials used in the Rando phantom, causing potential differences in photon attenuation and energy absorption. Second, the proposed phantom was segmented according to a single patient. The shape and weight are significantly different from the Rando phantom. The proposed phantom has a total weight of 3.85 kg which is relatively lighter than the head and neck portion of the Rando phantom (5.05 kg). Consequently, the absorbed doses of radiation measured using the proposed phantom are higher than those measured using the Rando phantom. These findings are consistent with the results investigated by Perisinakis (Perisinakis et al., 2013).
Another possible reason causing the high effective dose of the proposed phantom is because of the head size. The radiation field covers the lower part of the eyes and the upper part of the thyroid. In the proposed head phantom, the scattered radiation has a greater chance to enter these critical organs due to their shorter distances to the oral region than the distances in the Rando phantom. Therefore, the effective doses measured using the proposed phantom are higher than those measured using the Rando phantom. Despite these differences, the proposed head phantom is comparable to the Rando phantom in terms of radiation protection, especially for dose measurement of Asians.
The effective doses measured in this study were slightly higher than those of other studies. This may be because the CBCT machine, tube voltage, and x-ray filtration used in dose measurement are different. In the previous studies, tube voltages higher than 100 kVp (Roberts et al., 2009; Loubele et al., 2009) were usually
used. The x-ray photons are easy to penetrate the phantom without interaction with the TLDs compared to the x-ray of 65 to 85 kVp used in this study. In the future, we will gather a set of CT images corresponding to the average weight and height of Taiwanese (Wu et al., 2008). The corresponding physical phantoms can be built to server as the standard reference man and woman to improve the accuracy of dose evaluation in radiation protection for clinical practice.
5. Conclusion
In this study, we proposed a self-made anthropomorphic adult head phantom to evaluate the radiation doses emitted from the dental CBCT. The effective doses measured using the proposed phantom were comparable to those measured using the Rando phantom. The proposed phantom can be built quickly and easily with lower price than the standard Rando phantom. These advantages facilitate the construction of the realistic phantoms, such as the nationally averaged reference man, which can be used in clinical practice to improve the accuracy of radiation dose evaluation.
Acknowledgment
The authors would like to thank China Medical University of Taiwan for financially supporting this research under Contract no. CMU102-S-22.
References
Batista, W.O., Navarro, M.V., Maia, A.F., 2012. Effective doses in panoramic images from conventional and CBCT equipment. Radiat. Prot. Dosimetry. 151, 67–75.
Barone, S., Paoli, A., Razionale, A.V., 2013. Computer-aided modelling of three-dimensional maxillofacial tissues through multi-modal imaging. Proc. Inst. Mech. Eng. 227, 89–104.
Batista, W.O., Navarro, M.V., Maia, A.F., 2012. Effective doses in panoramic images from conventional and CBCT equipment. Radiat. Prot. Dosimetry. 151, 67–75.
Bauk, S., Alam, M. S., Alzoubi, A. S., 2011. Precision of low-dose response of LiF: Mg, Ti dosimeters exposed to 80 kVp x-rays. Journal of Physical Science. 22, 125-130.
Cavalcanti, M.G., Rocha, S.S., Vannier, M.W., 2004. Craniofacial measurements based on 3D-CT volume rendering: implications for clinical applications. Dentomaxillofac. Radiol. 33, 170–176.
Hadjipavlou, A. G., Simmons, J. W., Tzermiadianos, M. N., Katonis, P. G., Simmons, D. J., 2001. Plaster of Paris as bone substitute in spinal surgery. Eur. Spine J. 10, S189–S196.
Han, S., Lee, B., Shin, G., Choi, J., Kim, J., Park, C., Park, H., Lee, K., Kim, Y., 2012. Dose area product measurement for diagnostic reference levels and analysis of patient dose in dental radiography. Radiat. Prot. Dosimetry. 150, 523–531.
ICRP, 2007. Recommendations of the international commission on radiological protection. ICRP Publication 103. International Commission on Radiological Protection. Ann. ICRP, 37. Elsevier. ICRU, 1989. Tissue substitutes in radiation dosimetry and measurement. ICRU Report 44. International
Commission on Radiation Units and Measurements, Bethesda, Maryland.
King, R.M., Chueh, J.Y., van der Bom, I.M., Silva, C.F., Carniato, S.L., Spilberg, G., Wakhloo, A.K., Gounis, M.J., 2012. The effect of intracranial stent implantation on the curvature of the
cerebrovasculature. AJNR Am. J. Neuroradiol. 33, 1657–1662.
Koivisto, J., Kiljunen, T., Tapiovaara, M., Wolff, J., Kortesniemi, M., 2012. Assessment of radiation exposure in dental cone-beam computerized tomography with the use of metal-oxide semiconductor field-effect transistor (MOSFET) dosimeters and monte carlo simulations. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 114, 393–400.
Kuszyk, B.S., Heath, D.G., Bliss, D.F., Fishman, E.K., 1996. Skeletal 3-D CT: advantages of volume rendering over surface rendering. Skeletal Radiol. 25, 207–214.
Lofthag-Hansen, S., Thilander-Klang, A., Ekestubbe, A., Helmrot, E., Grondahl, K., 2008. Calculating effective dose on a cone beam computed tomography device: 3D Accuitomo and 3D Accuitomo FPD. Dentomaxillofac. Radiol. 37, 72–79.
Loubele, M., Bogaerts, R., Van Dijck, E., Pauwels, R., Vanheusden, S., Suetens, P., Marchale, G.,
Sanderinkf, G., Jacobs, R., 2009. Comparison between effective radiation dose of CBCT and MSCT scanners for dentomaxillofacial applications. Eur. J. Radiol. 71, 461–468.
Ludlow, J. B., Davies-Ludlow, L.E., Brooks, S.L., Howerton, W.B., 2006. Dosimetry of 3 CBCT devices for oral and maxillofacial radiology: CB Mercuray, NewTom 3G and i-CAT. Dentomaxillofac. Radiol. 35, 219–226.
Ludlow, J. B., Ivanovic, M., 2008. Comparative dosimetry of dental CBCT devices and 64-Slice CT for oral and maxillofacial radiology. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 106, 106–114.
Meng, Q., Chen, S., Long, X., Cheng, Y., Deng, M., Cai, H., 2012. The clinical and radiographic
characteristics of condylar osteochondroma. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 114, e66–74.
Peltier, L.F., Bickel, E.Y., Lillo, R., Thein, M.S., 1957. The use of plaster of Paris to fill defects in bone. Ann. Surg. 146, 61–69.
Perisinakis, K., Seimenis, I., Tzedakis, A., Papadakis, A. E., Damilakis, J., 2013. The effect of head size/shape, miscentering, and bowtie filter on peak patient tissue doses from modern brain perfusion 256-slice CT: How can we minimize the risk for deterministic effects?. Med. Phys. 40, 011911. Poppe, B., Looe, H.K., Pfaffenberger, A., Chofor, N., Eenboom, F., Sering, M., Ruhmann, A., Poplawski,
A., Willborn, K., 2007. Dose-area product measurements in panoramic dental radiology. Radiat. Prot. Dosimetry. 123, 131–134.
Qiu, L., Haruyama, N., Suzuki, S., Yamada, D., Obayashi, N., Kurabayashi, T., Moriyama, K., 2012. Accuracy of orthodontic miniscrew implantation guided by stereolithographic surgical stent based on cone-beam CT-derived 3D images. Angle Orthod. 82, 284–293.
Qu, X., Li, G., Zhang, Z., Ma, X., 2012. Thyroid shields for radiation dose reduction during cone beam computed tomography scanning for different oral and maxillofacial regions. Eur. J. Radiol. 81, e376– 380.
Roberts, J. A., Drage, N.A., Davies, J., Thomas, D.W., 2009. Effective dose from cone beam CT examinations in dentistry. Br. J. Radiol. 82, 35–40.
Ruivo, J., Mermuys, K., Bacher, K., Kuhweide, R., Offeciers, E., Casselman, J.W., 2009. Cone beam computed tomography, a low-dose imaging technique in the postoperative assessment of cochlear implantation. Otol. Neurotol. 30, 299–303.
Scarfe, W.C., Farman, A.G., Sukovic, P., 2006. Clinical applications of cone-beam computed tomography in dental practice. J. Can. Dent. Assoc. 72, 75–80.
Silva, M.A., Wolf, U., Heinicke, F., Bumann, A., Visser, H., Hirsch, E., 2008. Cone-beam computed tomography for routine orthodontic treatment planning: a radiation dose evaluation. Am. J. Orthod. Dentofacial Orthop. 133, 640 e1–5.
Simon, J.H., Enciso, R., Malfaz, J.M., Roges, R., Bailey–Perry, M., Patel, A., 2006. Differential diagnosis of large periapical lesions using cone-beam computed tomography measurements and biopsy. J. Endod.
32, 833–837.
Theodorakou, C., Walker, A., Horner, K., Pauwels, R., Bogaerts, R., Jacobs, R., 2012. Estimation of paediatric organ and effective doses from dental cone beam CT using anthropomorphic phantoms. Br. J. Radiol. 85, 153–160.
Tsiklakis, K., Donta, C., Gavala, S., Karayianni, K., Kamenopoulou, V., Hourdakis, C.J., 2005. Dose reduction in maxillofacial imaging using low dose cone beam CT. Eur. J. Radiol. 56, 413–417. Yu, L., Vrieze, T.J., Bruesewitz, M.R., Kofler, J.M., DeLone, D.R., Pallanch, J.F., Lindell, E.P.,
McCollough, C.H., 2010. Dose and image quality evaluation of a dedicated cone-beam CT system for high-contrast neurologic applications. AJR Am. J. Roentgenol. 194, W193–201.
Wu, J., Hung, S.Y., Shih, C.T., 2008. Organ mass estimation of Taiwanese adults using magnetic resonance images. In: Proceedings of the 6th International Conference on Isotopes. Seoul, Korea. pp. 350.
List of Figures
Fig. 1. The dose response curve of TLD.
Fig. 2. A front view of (a) the self-made anthropomorphic adult head phantom and (b) the Rando phantom. The white fillings in the proposed phantom are the plaster-water mixture to replace the bony structure. The black regions around the nose and eyes are the air cavities.
Table 1 Specifications of the dental cone-beam computed tomography operated in two scanning modes.
Specifications D-mode I-mode
Filed size (mm) 51×51 71×71
Voxel size (mm) 0.1×0.1×0.1 0.155×0.155×0.155
Tube voltage (kVp) 60 ~ 100
Tube current (mA) 4, 6, 8, 10, and 12
Focus size (mm) 0.5×0.5
Total filtration 2.8 mm Al
Table 2 Locations of TLDs in the self-made adult head phantom and the Rando phantom.
Location Location Slab number
Self-made Rando
1 Calvarium posterior 2 5
2 Calvarium anterior 2 5
3 mid brain 2 5
4 Right lens of eye 3 8
5 Left lens of eye 3 8
6 Right cheek 5 11
7 Centre cervical spine 6 12
8 Right parotid 6 12
9 Left parotid 6 12
10 Right ramus 6 12
11 Left ramus 6 12
12 Right submandibular gland 7 14
13 Left submandibular gland 7 14
14 Right mandible body 7 14
15 Left mandible body 7 14
16 Sublingual gland 7 14
17 Right thyroid 9 18
18 Left thyroid 9 18
Table 3 Effective doses measured using the self-made anthropomorphic adult head phantom and the Rando phantom. The standard deviations and percent errors are listed as well.
kVp D-mode (µSv) I-mode (µSv) Rando phantom Self-made phantom % error Rando phantom Self-made phantom % error 65 67.96±9.71 72.23±2.27 6.28% 96.37±10.65 108.24±12.72 12.32% 75 88.87±6.72 100.31±8.57 12.87% 166.22±8.38 190.99±6.31 14.90% 85 118.79±17.53 134.29±8.49 13.05% 217.7±17.16 246.48±24.24 13.22%