Spiritual Distress Experienced by Cancer Patients
-Develop a Spiritual Care for Cancer Patients
Ya-Lie Ku, RN, Penn State MSN, UIC PhD candidate, Lecturer of Fooyin University
Abstract
Cancer is the leading number one cause of mortality in Taiwan. A literature review indicates that the majority of cancer patients explore the spiritual needs. However,nursesfrequently neglectthepatients’spiritualstatus.Theproblem is that nurses are unfamiliar with assessing and diagnosing spiritual problems, as well as providing spiritual care for cancer patients. This study aims to develop a framework of spiritual care for cancer patients and established defining
characteristics, related factors, nursing interventions of spiritual distress for cancer patients, and criteria for predicting the outcomes of spiritual distress for cancer patients. A qualitative study design and purposive sampling procedure was used. Cancer patients were interviewed by using semi-open questions following Wlotersdorff(1994) framework to describe their experiences of
themselves, others, and their gods during the illness. This study was approved by a medical center in southern Taiwan and conducted from February to April, 2003. Based on the categories of study findings, the investigator developed 27 defining characteristics, 13 related factors, 20 nursing interventions, and 18 outcomes criteria of spiritual distress for cancer patients. Based on the findings, the spiritual distress of cancer patients has defined as a cancer patient has the experiences of negative psychological states, contradictory relationship with health care professionals, God, traditional values, religion, and difficulties to deal with death issues. Besides, the investigator developed a framework of spiritual care for cancer patients and four scales on which defining characteristics, related factors, nursing interventions, and criteria for outcomes of spiritual distress for cancer patients. An upcoming study will evaluate the reliability and validity of these scales for future application to cancer patients. The hope is places on cancer patients who will live meaningfully by strengthening their spiritual care.
Background
Cancer is the leading cause of mortality in Taiwan and the journey along the path
from discovering one’sillnessto facing death isvery difficultforcancerpatients.
Therefore, concern for the spirituality of cancer patients is crucial, with the aim of
giving their lives meaning during nursing. A literature review discloses that most
cancer patients desire spiritual help through the course of their illness. Hu et al1
identified that 62% of 21 cancer patients wish for spiritual care. Spiritual care is
perceived as one main expected type of desirable care among 73 family members of
Japanese cancer patients2.
Nevertheless, nurses who are frequently busy performing routine tasks, often
neglect the spiritual care of cancer patients. American Cancer Society3has reported
that 69% of 74 cancer patients received unsatisfactory ‘incomplete’spiritual support.
Only 33% of 20 French nurses have considered the spiritual needs of 27 cancer
patients4. Moreover, Highfield5found that 52% of 40 nurses evaluate the spiritual
status of cancer patients incorrectly. More than fifty percent of 166 Finland nurses
were less or not willing to provide spiritual support for cancer patients because of
their insufficient skills for spiritual care6. Byrne7observed that nurses need guidance
in administering spiritual care. The central problem is that nurses are unfamiliar with
patients, since no comprehensive framework of spiritual care for cancer patients was
developed, as well as no scales were established on which defining characteristics,
related factors, nursing interventions, and criteria for outcomes of spiritual distress for
cancer patients.
Aim
This qualitative study examines the experiences of spiritual suffering of cancer
patients, developing a framework of spiritual care for cancer patients and four
measurement scales: defining characteristics, related factors, nursing interventions,
and criteria for forecasting the outcomes of spiritual distress for cancer patients.
Literature Review
The literature review covers three areas: definition of spirituality, theories of
spirituality, and nursing interventions related to spiritual care.
Definition of Spirituality
Mao8 and Liu9 defined spirituality as individuals searching for purpose and
meaning in their lives and interpreting life-value and meaning triumphing over the
self. Chao10 combined thesuggestionsofvariousauthors’to definespirituality as
individuals thinking about the meaning of their existence, including their own inner
that can allow individuals to live comfortably and happily. Byrne’s7 defined
spirituality as the search for meaning and Barnum12 has defined spirituality as
searching and expressing their connection to a greater and meaningful context.
However, although definitions of spirituality were so plentiful, the topic of spiritual
distress is not as popular as spirituality. According to NANDA13, spiritual distress is
the experience of the inability to integrate the meaning and purpose of life by self,
others, art, music, literature, nature, or the connection with God.
Theories of Spirituality
Three theories of spirituality are introduced below. Carson14 conceived of
spiritual dimensions for nursing practice as a circle, with individual spirituality being
the inner area of the circle, influencing willpower, emotion, wisdom, and other values
in the area further from the center of the circle, which in turn affect physiology, the
outermost part of the circle. Hoshiko15 proposed a theory of spirituality being based
on six life relations, namely life-goals, interaction with self and others, environment,
past experiences, and future orientation. Wlotersdorff16 designed a framework that
views individual spiritual well being the ability to maintain peaceful relations among
Spiritual Care of Nursing Interventions
Nursing interventions concerned with spiritual care were devised by following
the Wlotersdorff’s16framework involving the relationship of the self with self, with
others, and with God.
1. Relations with self
Carr and Morris17, Newshan18, and Yang19proposed self- exploration, acceptance,
and valued as important elements for strengthening spirituality. Life-reviewing
nursing interventions9、11、20involving active listening4through story telling, using
metaphor or black humor can enliven the inner world of patients21、22. Additionally,
meditation and imagination while listening to music can enrich patients’spirituality20、
23
. Moreover, therapy such as writing or painting, reading Chinese literature or poems,
gardening, and using alternative therapies can aid patients in searching for answers to
their questions, maintain their faith, allowing them to discover inner peace7、20、22、24.
2. Relations with others
Yang19postulated that relations between nurses and patients might affect
patients’spirituality and thus suggested company, communication, warmth, empathy,
and careful relations as the significant nursing interventions for ensuring spiritual
care17、18、25、26. Besides nurses, family members with traditional cultural values also
meeting the cultural expectations and needs of patients in terminal care28.
Relations with God
Patients’spirituality can beenhanced by participating in religious activities, such
as a Bible study, Buddhist recitation, and prayer9、11、20、29. One important study sampled
500 open-heart surgery patients who prayed and compared them with a control group
of 500 non-praying open-heart surgery patients. The prayer group went home 11%
sooner and experienced 12% fewer post-operative complications30. Taylor31examined
the feasibility of incorporating prayer in nursing practice, while suggesting areas for
assessing and supporting patients in prayer. Nurses can also refer patients to Buddhist
masters, pastors, or priests who can design spiritual activities for patients, by
cooperating with their spiritual partners or health professionals17、18.
Methods
Study Design
This qualitative study developed a framework of spiritual care for cancer patients
and established four scales, including defining characteristics, related factors, nursing
interventions, and criteria for estimating the outcomes of spiritual distress for cancer
patients.
Sample
half a year, clear consciousness, stable vital signs, age of over 20 years old,
proficiency in Mandarin or Taiwanese, and willingness to participate in this study.
Procedure
This study was approved by a southern Taiwanese medical center, and data were
gathered in chemotherapy clinics weekly from February to April, 2003. A guide for
interviewing was developed by three investigators based on Wlotersdorff’s16
framework. The patients were interviewed with semi-open questions and asked to
describe experiences of themselves, others, and gods during their illness.
Data Analysis
Three scales were established following the instructions of Waltz, Strickland, and
Lenz28.First,contentanalysiswasbased on Wlotersdorff’s16framework of the
patients’relations with themselves, with others, and with gods as three units of
analysis. Second, under each unit, the investigator developed a scheme for an explicit
classification of the content and coding and scoring instruction. Third, formal data
analysis was conducted as the inter-rater reliability of coding skills between two
researchers approached .80. Data collection and analysis were discontinued, since 20
interviews produced more than sufficient data for analysis.
Findings
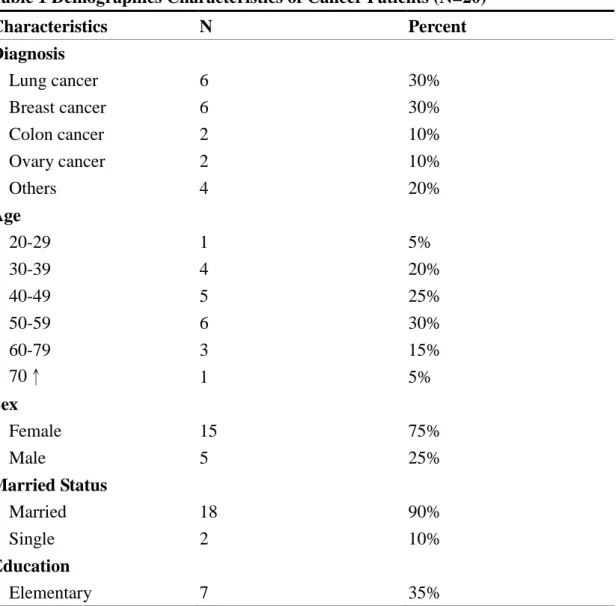
diagnosed with lung cancer (30%), breast cancer (30%), colon cancer (10%), ovary
cancer (10%), and others, respectively (5%). The subject ages ranged from 28 to 74
years with the majority 30-59 (75%). The sample was 75% female; 90% married;
65% educated to at least high school level; 80% economically stable; 35% Buddhist,
25% atheist, 20% Taoist, 10% Christian, and others, respectively (5%). Except for one,
all cancer patients were taken cared for by their family members. The demographics
of 20 cancer patients are presented in Table 1.
Table 1 Demographics Characteristics of Cancer Patients (N=20)
Characteristics N Percent Diagnosis Lung cancer Breast cancer Colon cancer Ovary cancer Others Age 20-29 30-39 40-49 50-59 60-79 70↑ Sex Female Male Married Status Married Single Education Elementary 6 6 2 2 4 1 4 5 6 3 1 15 5 18 2 7 30% 30% 10% 10% 20% 5% 20% 25% 30% 15% 5% 75% 25% 90% 10% 35%
Vocational school High school College Incomes High Middle Low Religion Buddhist Taoist Christian Catholics Yi guan dao Atheist Caregivers Parents Couples Children Friends Self Nurse aids 7 3 3 4 8 4 7 4 2 1 1 5 3(15%) 9(45%) 2(10%) 1(5%) 4(20%) 1(5%) 35% 15% 15% 20% 60% 20% 35% 20% 10% 5% 5% 25% 15% 45% 10% 5% 20% 5%
The investigation identified several categories for describing spiritual
experiences, in three main areas: (1) In relations with self-two subcategories were
labeled as emotion and thoughts. For emotion, shock, denial, resentment, regret,
worry, fear, suffering, sorrow, loneliness, and numbness were identified. For thoughts,
fatalism, pessimism, and resignation were found. (2) In relations with others-distrust,
disobedience, dissatisfaction, and non-forgiveness were found. (3) In relations with
god-negative relationships with god involved disrespect toward god and the feeling
and death. Examples of these included the feeling ofbeing unprotected from one’s
ancestors, feeling sinfulness, insecurity, inability to discuss death, worry about the
death process, the ritual of death, and the destination of the spirit after death. Based on
those categories, the investigator developed defining characteristics of spiritual
distress for cancer patients as shown in Table 2.
Table2 Defining Characteristics of Spiritual Distress for Cancer Patients
Unit Relations with
self
Relations with others
Relations with God
Categories Emotion shock denial resentment regret worry fear suffering sorrow loneliness numbness Thoughts fatalism pessimism resignation distrust disobedience dissatisfaction non-forgiveness God
disrespect toward god feeling that god is powerless
Traditional Values
being unprotected from one’sancestors
Religion
sinfulness insecurity
being governed by religious beliefs
Death
inability to discuss death worry about death process worry about the ritual of death
worry about the destination of the spirit after death
Except for defining characteristics, factors related to spiritual distress for cancer
patients were also identified. (1) Negative relationships with self included negative
involved miscommunication, irresponsibility, lack of empathy, and lack of caring
from health care professionals. (3) Negative relationship with god included
unawareness of god and broken relationship with god, and for traditional values and
religions, transmigration, inability to perform religious rituals, lack of religious
decoration, loss of status and involvement in religious institutions were identified.
Based on those categories, the investigator developed factors related to spiritual
distress for cancer patients as shown in Table 3.
Table 3 Factors related to Spiritual Distress for Cancer Patients
Unit Relations
with self
Relations with others
Relations with God
Categories negative past
experiences physical suffering miscommunication irresponsibility lack of empathy lack of caring God unawareness of god
broken relationship with god
Traditional Values
transmigration
Religion
inability to perform religious rituals lacking of religious decoration loss of status in religious institutions lack of involvement in religious institutions
To help cancer patients compensate for defining characteristics as well as factors
related to spiritual distress, nursing interventions based on research findings and
literature were created with reference to four themes: rebuilding life values, rebuilding
building courage to face death. Based on each theme, the nursing goals of caring for
spiritual distress for cancer patients were designed and five nursing interventions
under each goal were also established. Four themes and nursing interventions to
alleviate spiritual distress of cancer patients are presented in Table 4.
Table4 Nursing Interventions to Alleviate Spiritual Distress of Cancer Patients
Themes rebuilding life
values rebuilding value placed in relationships with others improving the relationship with god building courage to face death
Interventions 1. lead life
review with funny stories by humor 2. listen and accept patients’ exploration 3. draw to express inner world 4. read inspired articles 5. grow a vital plant 1. accompany with 2. therapy touch
3. share with same experiencing
4. discuss the daily life with family
5. arrange leisure activities with family 1. spiritual ministers visited 2. read spiritual articles 3. broadcast spiritual music 4. offer spiritual gifts 5. contact with spiritual friends 1. talk lost and grief emotion 2. express thoughts of life and death 3. assist unfinished will 4. discuss the death rite 5. write the last statement Additionally, three outcome criteria were established. (1) Positive relations with
self were exemplified by personal sore point, emotional stability, feeling of
contentment, loving self, self worth, optimism, and feeling that life is meaningful. (2)
Positive relations with others included forgiveness of others, trust of health
care, attendance of social activities, getting along with others, and caring for others. (3)
In good relations with god: attendance of religious activities, getting along with
religious representatives and religious partners, releasing feelings of sinfulness,
obtaining security, rebuilding a good relationship with god, and understanding the
destination of the spirit after death were listed. Outcomes criteria of spiritual distress
for cancer patients are presented in Table 5.
Table5 Outcome Criteria of Spiritual Distress for Cancer Patients
Unit Positive relations with
Self
Positive relations with Others
A good relations with God
Categories personal sore point
exemplified emotional stability feeling of contentment loving self self worth optimism
feeling that life is meaningful
forgive others
trust health professionals
accept care and obey the instructions of health professionals
attend social activities
get along with others
care others
attend religious activities
get along with religious representatives and religious partners
release sinful feelings
obtain security
rebuild a good
relationships with god
understand destination of the spirit after death
Discussion and Conclusion
Following Wlotersdorff’s16framework which included thepatients’relationships
with themselves, with others, and with gods, this study has asserted that negative past
influencecancerpatients’spirituality in termsofnegativeemotions and thoughts.
Additionally, miscommunication between cancer patients and health care
professionals, as well as irresponsibility, lack of empathy, and caring from health care
professionalsmay influencepatients’spirituality in termsoftrustof and obedience to
health care professionals. Alternatively, the patients may not be satisfied with the
health care and even cannot forgive how health care professionals have treated them.
Moreover,cancerpatients’spiritual distress may originate in disrespect for God,
or feeling God is powerless because they are unaware of God or have a broken
relationship with Him. Some patients may feel themselves unprotected from ancestors
because of traditional transmigration beliefs, while others have feelings of sinfulness,
insecurity, or being governed by religious beliefs since they cannot wear religious
decoration or perform religious activities, or have lost involvement and status in
religious institutions. Finally, cancer patients have difficulties discussing death and
worry about the process and ritual of death, as well as being anxious about where their
spirits are going to after death.
In conclusion, this study has defined spiritual distress for cancer patients as
meaning that a cancer patient experiences negative psychological states, contradictory
relationships with health care professionals, God, traditional values, religion, and has
the literature, which emphasized individual spirituality in searching for existing
values and meaning. Additionally, Carson14stated an individual’s emotion and
physiology would be influenced by his spirituality. However, spiritual distress for
cancer patients in this study was interpreted as psychological states affected by
physical responses and social experiences. The definition in this study is similar to
Hoshiko’s15and Wlotersdorff’s16
that spirituality is based on interaction with self,
others, and past experiences as well as maintaining a peaceful relationship among the
self, others, and God.
Except for the definition, the other categories were identified primarily to include
relationships with health care professionals; however, the literature has emphasized
individual spirituality in terms of relationships with family members or friends.
Cancer patientscaregreatly abouthealth careprofessionals’responsibility,empathy,
and caring. This care influences their communication, trust, satisfaction, and
compliance with those professionals. In addition, the god categories for cancer
patients were identified as the process of knowing and maintaining a relationship with
God, and the possibility of attending religious activities. Compared with previous
literature, the significantly different results of this study include the awareness that
traditional values like transmigration and death issues have been identified as
Overall, based on the research findings, the investigator developed a framework
of spiritual distress care for cancer patients (Figure 1). For future areas of research,
Narayanasamy32and Skoberne26considered spiritual care to be an essential
component integral to patient care. Parish patients regarded their nurses as useful,
meaningful, and effective professionals because the nurses integrated spirituality with
health in their nursing interventions33. To assist developing spiritual care in clinical
units, based on the framework, the investigator designed four scales to measure
defining characteristics, related factors, nursing interventions, and criteria for
outcomes of spiritual distress for cancer patients undergoing chemotherapy. A further
study will evaluate the reliability and validity of these scales for application to cancer
patients. Hopefully cancer patients can live happily and meaningfully by
strengthening their spiritual care; and in turn, they can perceive nurses as useful,
meaningful, and effective professionals for their spiritual care.
Acknowledgement
The author thanks the Nursing Department of Kaohsiung Chang Gung Memorial
Hospital for approving and supporting this study. Ywi Chi Kan and Tsay-Yi Au are
appreciated for their advices of data analysis. Special thanks are given to the 20
cancer patients of Chemotherapy room where the study subjects were recruited, under
References
1. Hu, W. Y., Chiu, T.Y., Bhikkhu, H.M., Chen, C.Y., & Chen, Y.C. (1999). Spiritual Needs of Terminal Cancer Patients from the Viewpoint of Medical Professionals. China Journal of Family Medicine, 3(1): 8-19.
2. Ogasawara, C., Kume, Y., & Andou, M. (2003). Family satisfaction with perception of and barriers to terminal care in Japan. Oncology Nursing Forum, 30(5), 100-105.
3. American Cancer Society(1994). Cancer facts and figures. Atlanta, GA: American Cancer Society.
4. Kohler, C. (1999). Nursing diagnosisof“spiritualdistress”:anecessary revaluation. Recherche en Soins Infirmiers, 56, 12-72.
5. Highfield, M. F. (1992). Spiritual health of oncology patients: nurse and patient perspectives. Cancer Nursing, 15(1), 1-8.
6. Kuuppelomaki, M. (2002). Spiritual support for families of patients with cancer: a pilot study of nursing staff assessments. Cancer Nursing, 25(3), 209-218.
7. Byrne, M. (2002). Spirituality in palliative care: what language do we need? International Journal of Palliative Care, 8(2), 67-70.
8. Mao, H. C. (1997). Recognition of Spiritual Needs of the Patients. Formosan Journal of Medicine, 1(5), 653-656.
9. Liu, S. J. (1999). The Spiritual Care of the Elderly. Journal of Nursing, 46(4), 51-57.
10. Chao, C. S. (1998). Psychiatric Mental Health Nursing and Spiritual Care. Journal of Nursing, 45(1), 16-21.
11. Lin, S. (2000). Spiritual Care and Human Caring. Journal of Veteran Nursing, 17(2), 153-158.
12. Barnum, B. S. (2003). Spirituality in Nursing: from Traditional to New Age. New York: Springer Publishing Company.
13. Kao, C. H. (2003). NANDA Nursing Diagnosis: Definition & Classification 2003-2004. Taipei: Farseeing.
14. Carson, V. B. (1989). Spiritual Dimensions of Nursing Practice. Philadelphia: Saunders Company.
15. Hoshiko, B. R. (1993). Nursing Responses to Spirituality: Kent State University School of Nursing. In JA. Shelly (ed.). Teaching Spiritual Care. Wisconsin: Nursing Christian Fellowship.
16. Woltersdorff , N. (1994). For justice in shalom. In Bolton, WG, Kennedy, TD, & Verhey, A (eds.). From Christ to the World: Introductory readings in Christian ethics. Michigan: Wm. B, Eerdmans Publishing Co.
17. Carr, E. W., & Morris, T. (1996). Spirituality and patients with advanced cancer: a social work response. Journal of Psychosocial Oncology, 14(1), 71-81.
18. Newshan, G. (1998). Transcending the physical: spiritual aspects of pain in patients with HIV and/or cancer. Journal of Advanced Nursing, 28(6), 1236-1241.
19. Yang, K. P. (1998). Spiritual Care in Nursing Practice. Journal of Nursing, 45(3), 77-84.
20. Lin, G. C., & Chiou, Y. F. (1996). Spiritual care of terminal cancer patients. Nursing Images, 6(2), 49-56.
21. Lackey, N. R., Gates, M. F., & Brown, G..(2001). African American women’s experiences with the initial diagnosis, and treatment of breast cancer. Oncology Nursing Forum, 28(3), 519-527.
22. Leu, S. C. (2000). Art therapy and spiritual care. Taiwan Journal of Hospice Palliative Care, 5(2), 62-65.
23. Brown-Saltzman, K. (1997). Replenishing the spirit by meditative prayer and guided imagery. Seminars in Oncology Nursing, 13(4), 255-259.
24. Taylor, E. J. (2001). Spirituality, culture, and cancer care. Seminars in Oncology Nursing, 17(3), 197-205.
25. Sheu, L. A. (2000). My opinions of spiritual care. Taiwan Journal of Hospice Palliative Care, 5(2), 11-13.
26. Skoberne, M. (2002). Spirituality and spiritual health. Obzornik Zdravstvene Nege, 36(1), 23-31.
27. Burhansstipanov, L, & Hollow, W. (2001). Native American cultural aspects of oncology nursing care. Seminars in Oncology Nursing, 17(3), 206-219.
28. Waltz, C. F., Strickland, O. L., & Lenz, E. R. (1991). Measurement in Nursing Research. Philadelphia: F.A. Davis Company.
29. Musick, M. A., Koenig, H. G.., Hays, J. C., & Cohen, H. J. (1998). Religious activity and depression among community-dwelling elderly persons with cancer: the moderating effect of race. Psychological Sciences & Social Sciences, 53B(4), S218-227.
30. Brewes, R. (2002). The Scientific Side of Spirituality in Nursing. RN, 65(12), 10.
31. Taylor, E. J. (2003). Prayer’sclinicalissuesand implications.HolisticNursing Practice, 17(4), 179-188.
32. Narayanasamy, A. (2002). Spiritual coping mechanisms in chronically ill patients. British Journal of Nursing, 11(22), 1461-1462.
33. Wallace, D. C., Tuck, I., Boland, C. S., & Witucki, J. M. (2002). Client perceptions of parish nursing. Public Health Nursing, 19(2), 128-135.